
Assessment of Passive Upper Limb Stiffness and Its Function in Post-Stroke Individuals Wearing an Inertial Sensor during the Pendulum Test

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Clinical Assessments
2.3. Experimental Setup
2.4. Data Collection
2.5. Feature Extraction
2.6. Statistical Analysis
3. Results
3.1. Characteristics
3.2. Variables Related to the Scales
3.3. Variables Related to the Inertial Sensor and Pendulum Test
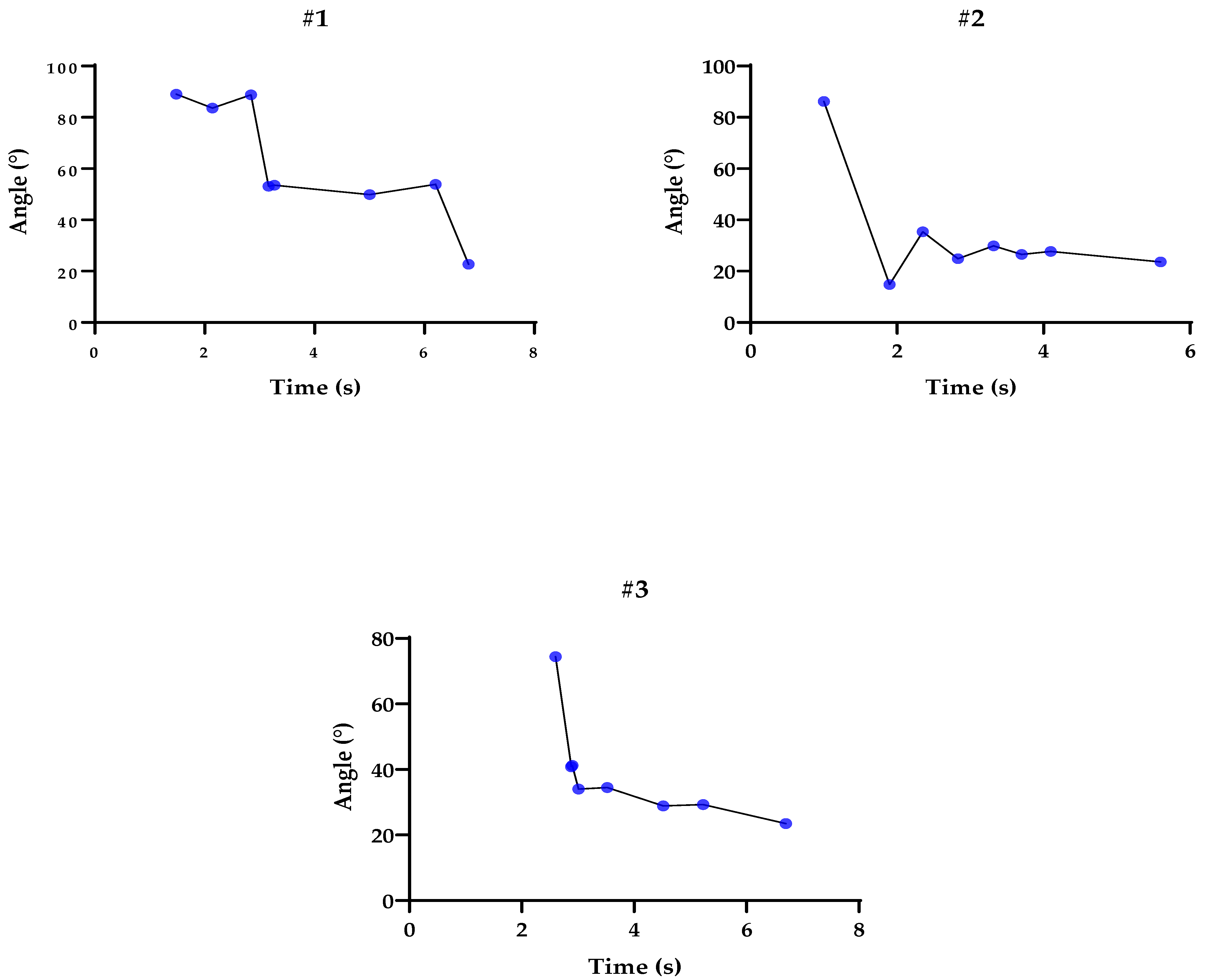
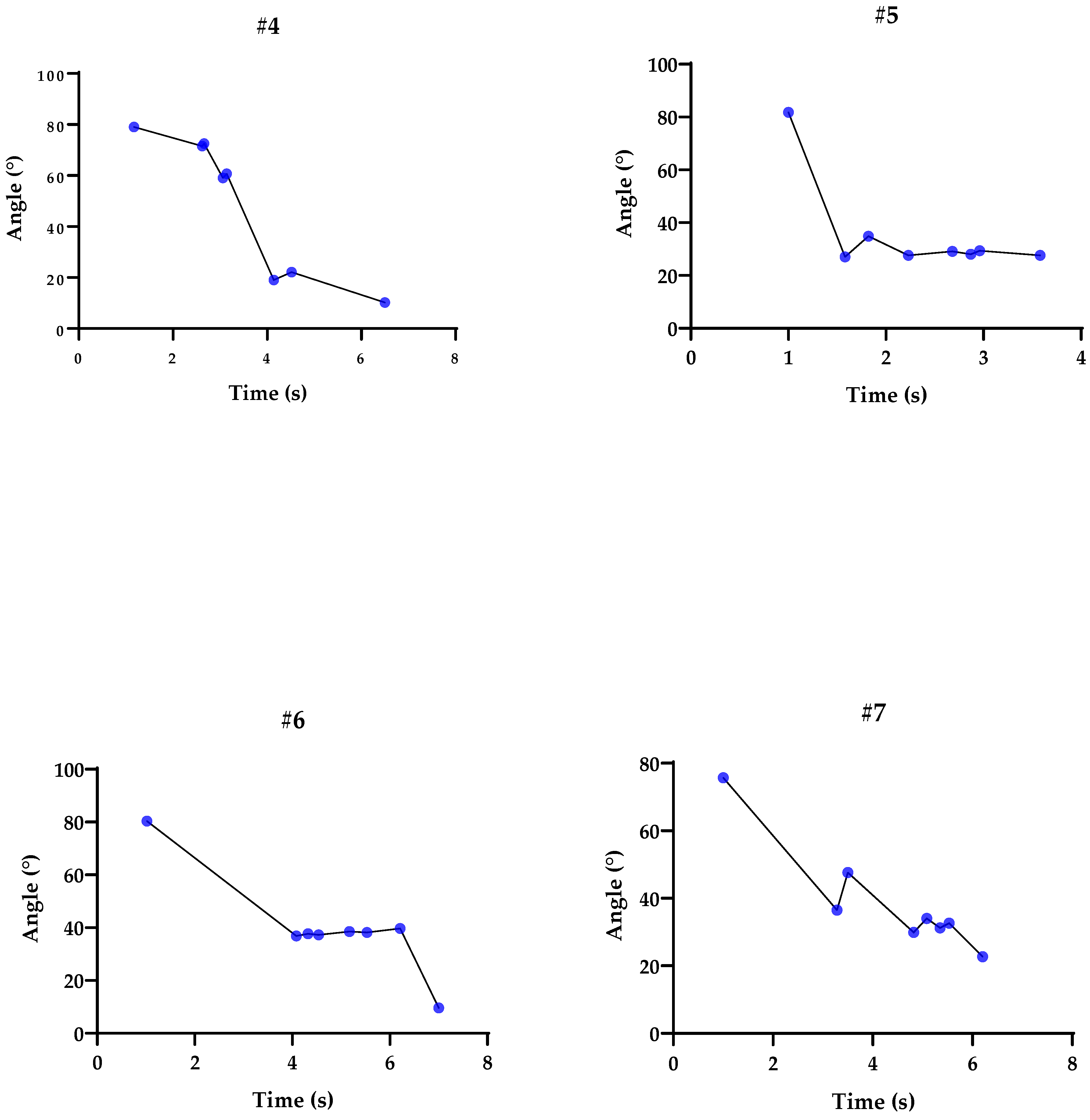
3.4. Graphs Related to Participants’ Tests during the Pendulum Test
3.5. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jones, T.A.; Allred, R.P.; Jefferson, S.C.; Kerr, A.L.; Woodie, D.A.; Cheng, S.-Y.; Adkins, D.L. Motor System Plasticity in Stroke Models: Intrinsically Use-Dependent, Unreliably Useful. Stroke 2013, 44, S104–S106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakayma, H.; Jørgensen, H.S.; Raaschou, H.O.; Olsen, T.S. Compensation in Recovery of Upper Extremity Function after Stroke: The Copenhagen Stroke Study. Arch. Phys. Med. Rehabil. 1994, 75, 852–857. [Google Scholar] [CrossRef] [PubMed]
- Cramer, S.C.; Wolf, S.L.; Adams, H.P.; Chen, D.; Dromerick, A.W.; Dunning, K.; Ellerbe, C.; Grande, A.; Janis, S.; Lansberg, M.G.; et al. Stroke Recovery and Rehabilitation Research. Stroke 2017, 48, 813–819. [Google Scholar] [CrossRef] [Green Version]
- Rabelo, M.; Nunes, G.S.; da Costa Amante, N.M.; de Noronha, M.; Fachin-Martins, E. Reliability of Muscle Strength Assessment in Chronic Post-Stroke Hemiparesis: A Systematic Review and Meta-Analysis. Top. Stroke Rehabil. 2016, 23, 26–35. [Google Scholar] [CrossRef]
- Wieters, F.; Weiss Lucas, C.; Gruhn, M.; Büschges, A.; Fink, G.R.; Aswendt, M. Introduction to Spasticity and Related Mouse Models. Exp. Neurol. 2021, 335, 113491. [Google Scholar] [CrossRef] [PubMed]
- Trompetto, C.; Marinelli, L.; Mori, L.; Pelosin, E.; Currà, A.; Molfetta, L.; Abbruzzese, G. Pathophysiology of Spasticity: Implications for Neurorehabilitation. BioMed Res. Int. 2014, 2014, 354906. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E. New Insights into the Pathophysiology of Post-Stroke Spasticity. Front. Hum. Neurosci. 2015, 9, 192. [Google Scholar] [CrossRef] [Green Version]
- Gürbüz, M.; Bilgin, S.; Albayrak, Y.; Kızılay, F.; Uysal, H. Biceps Femoris Late Latency Responses and the “Notching Sign” in Spasticity. J. Neuroeng. Rehabil. 2015, 12, 93. [Google Scholar] [CrossRef] [Green Version]
- Corbetta, D.; Sirtori, V.; Castellini, G.; Moja, L.; Gatti, R. Constraint-Induced Movement Therapy for Upper Extremities in People with Stroke. Cochrane Database Syst. Rev. 2015, 2015, CD004433. [Google Scholar] [CrossRef] [Green Version]
- Burton, E.; Farrier, K.; Lewin, G.; Pettigrew, S.; Hill, A.-M.; Airey, P.; Bainbridge, L.; Hill, K.D. Motivators and Barriers for Older People Participating in Resistance Training: A Systematic Review. J. Aging Phys. Act. 2017, 25, 311–324. [Google Scholar] [CrossRef] [Green Version]
- Fleuren, J.F.M.; Voerman, G.E.; Erren-Wolters, C.V.; Snoek, G.J.; Rietman, J.S.; Hermens, H.J.; Nene, A.V. Stop Using the Ashworth Scale for the Assessment of Spasticity. J. Neurol. Neurosurg. Psychiatry 2010, 81, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdollahi, M.; Kuber, P.M.; Shiraishi, M.; Soangra, R.; Rashedi, E. Kinematic Analysis of 360° Turning in Stroke Survivors Using Wearable Motion Sensors. Sensors 2022, 22, 385. [Google Scholar] [CrossRef] [PubMed]
- Stewart, J.C.; Cramer, S.C. Genetic Variation and Neuroplasticity: Role in Rehabilitation After Stroke. J. Neurol. Phys. Ther. 2017, 41, S17–S23. [Google Scholar] [CrossRef] [PubMed]
- Foroud, A.; Whishaw, I.Q. Reaching-to-Eat in Humans Post-Stroke: Fluctuating Components within a Constant Pattern. Behav. Neurosci. 2010, 124, 851–867. [Google Scholar] [CrossRef] [PubMed]
- Franklin, D.W.; Milner, T.E. Adaptive Control of Stiffness to Stabilize Hand Position with Large Loads. Exp. Brain Res. 2003, 152, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Ansari, N.N.; Naghdi, S.; Moammeri, H.; Jalaie, S. Ashworth Scales Are Unreliable for the Assessment of Muscle Spasticity. Physiother. Theory Pract. 2006, 22, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, D.M.; Liang, H.; Wu, J. Knee Joint Kinematics of the Pendulum Test in Children with and without Down Syndrome. Gait Posture 2020, 76, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Gracitelli, M.E.C.; Guglielmetti, C.L.B.; Botelho, C.A.S.; Malavolta, E.A.; Assunção, J.H.; Ferreira Neto, A.A. Surgical Treatment of Post-Traumatic Elbow Stiffness by Wide Posterior Approach. Rev. Bras. Ortop. 2020, 55, 570–578. [Google Scholar] [CrossRef]
- Hu, X.; Suresh, N.L.; Chardon, M.K.; Rymer, W.Z. Contributions of Motoneuron Hyperexcitability to Clinical Spasticity in Hemispheric Stroke Survivors. Clin. Neurophysiol. 2015, 126, 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Woytowicz, E.J.; Rietschel, J.C.; Goodman, R.N.; Conroy, S.S.; Sorkin, J.D.; Whitall, J.; McCombe Waller, S. Determining Levels of Upper Extremity Movement Impairment by Applying a Cluster Analysis to the Fugl-Meyer Assessment of the Upper Extremity in Chronic Stroke. Arch. Phys. Med. Rehabil. 2017, 98, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Saliba, V.A.; de Castro Magalhães, L.; de Morais Faria, C.D.C.; Laurentino, G.E.C.; Cassiano, J.G.; Teixeira-Salmela, L.F. Adaptação Transcultural e Análise Das Propriedades Psicométricas Da Versão Brasileira Do Instrumento Motor Activity Log. Rev. Panam. Salud Pública 2011, 30, 262–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Liu, T.-W.; Tse, M.M.Y.; Lai, C.K.Y.; Tsoh, J.; Ng, S.S.M. The Predictive Role of Hand Section of Fugl–Meyer Assessment and Motor Activity Log in Action Research Arm Test in People With Stroke. Front. Neurol. 2022, 13, 926130. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.S.; Seo, J.H.; Song, C.G. Portable Measurement System for the Objective Evaluation of the Spasticity of Hemiplegic Patients Based on the Tonic Stretch Reflex Threshold. Med. Eng. Phys. 2011, 33, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-W.; Ju, M.-S.; Wang, W.-C.; Lin, C.-C.K. Muscle Tone of Upper Limbs Evaluated by Quantitative Pendulum Test in Patients with Acute Cerebellar Stroke. Acta Neurol. Taiwan 2009, 18, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Valle, M.S.; Casabona, A.; Sgarlata, R.; Garozzo, R.; Vinci, M.; Cioni, M. The Pendulum Test as a Tool to Evaluate Passive Knee Stiffness and Viscosity of Patients with Rheumatoid Arthritis. BMC Musculoskelet. Disord. 2006, 7, 89. [Google Scholar] [CrossRef] [Green Version]
- Fee, J.W.; Miller, F. The Leg Drop Pendulum Test Performed under General Anesthesia in Spastic Cerebral Palsy. Dev. Med. Child Neurol. 2007, 46, 273–281. [Google Scholar] [CrossRef]
- Lin, C.C.K.; Ju, M.S.; Huang, H.W. Gender and Age Effects on Elbow Joint Stiffness in Healthy Subjects. Arch. Phys. Med. Rehabil. 2005, 86, 82–85. [Google Scholar] [CrossRef]
- Sokal, B.; Uswatte, G.; Barman, J.; Brewer, M.; Byrom, E.; Latten, J.; Joseph, J.; Serafim, C.; Ghaffari, T.; Sarkar, N. Network of Movement and Proximity Sensors for Monitoring Upper-Extremity Motor Activity after Stroke: Proof of Principle. Arch. Phys. Med. Rehabil. 2014, 95, 499–505. [Google Scholar] [CrossRef]
- Sterpi, I.; Caroli, A.; Meazza, E.; Maggioni, G.; Pistarini, C.; Colombo, R. Lower Limb Spasticity Assessment Using an Inertial Sensor: A Reliability Study. Physiol. Meas. 2013, 34, 1423–1434. [Google Scholar] [CrossRef]
- Lemmens, R.J.M.; Janssen-Potten, Y.J.M.; Timmermans, A.A.A.; Smeets, R.J.E.M.; Seelen, H.A.M. Recognizing Complex Upper Extremity Activities Using Body Worn Sensors. PLoS ONE 2015, 10, e0118642. [Google Scholar] [CrossRef] [Green Version]
- Rahimi, F.; Eyvazpour, R.; Salahshour, N.; Azghani, M.R. Objective Assessment of Spasticity by Pendulum Test: A Systematic Review on Methods of Implementation and Outcome Measures. Biomed. Eng. Online 2020, 19, 82. [Google Scholar] [CrossRef] [PubMed]
- Bhimani, R.; Anderson, L. Clinical Understanding of Spasticity: Implications for Practice. Rehabil. Res. Pract. 2014, 2014, 279175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altman, D.; Minozzo, F.C.; Rassier, D.E. Thixotropy and Rheopexy of Muscle Fibers Probed Using Sinusoidal Oscillations. PLoS ONE 2015, 10, e0121726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, K.S. Muscle Biophysics; Rassier, D.E., Ed.; Advances in Experimental Medicine and Biology; Springer: New York, NY, USA, 2010; Volume 682, ISBN 978-1-4419-6365-9. [Google Scholar]
- Lakie, M.; Vernooij, C.A.; Osborne, T.M.; Reynolds, R.F. The Resonant Component of Human Physiological Hand Tremor Is Altered by Slow Voluntary Movements. J. Physiol. 2012, 590, 2471–2483. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.J.; McCabe, J.P.; Holcomb, J.; Monkiewicz, M.; Gansen, J.; Pundik, S. Long-Dose Intensive Therapy Is Necessary for Strong, Clinically Significant, Upper Limb Functional Gains and Retained Gains in Severe/Moderate Chronic Stroke. Neurorehabil. Neural Repair 2019, 33, 523–537. [Google Scholar] [CrossRef] [Green Version]
- Pundik, S.; McCabe, J.; Skelly, M.; Tatsuoka, C.; Daly, J.J. Association of Spasticity and Motor Dysfunction in Chronic Stroke. Ann. Phys. Rehabil. Med. 2019, 62, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Mirbagheri, M.M.; Rymer, W.Z. Time-Course of Changes in Arm Impairment after Stroke: Variables Predicting Motor Recovery over 12 Months. Arch. Phys. Med. Rehabil. 2008, 89, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-W.; Ju, M.-S.; Lin, C.-C.K. Flexor and Extensor Muscle Tone Evaluated Using the Quantitative Pendulum Test in Stroke and Parkinsonian Patients. J. Clin. Neurosci. 2016, 27, 48–52. [Google Scholar] [CrossRef]
- Abe, M.O.; Yamada, N. Modulation of Elbow Joint Stiffness in a Vertical Plane during Cyclic Movement at Lower or Higher Frequencies than Natural Frequency. Exp. Brain Res. 2003, 153, 394–399. [Google Scholar] [CrossRef]
- Hou, J.; Sun, Y.; Sun, L.; Pan, B.; Huang, Z.; Wu, J.; Zhang, Z. A Pilot Study of Individual Muscle Force Prediction during Elbow Flexion and Extension in the Neurorehabilitation Field. Sensors 2016, 16, 2018. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | #1 | #2 | #3 | #4 | #5 | #6 | #7 |
|---|---|---|---|---|---|---|---|
| Sex | M | M | F | F | F | F | F |
| Age (years) | 54 | 45 | 49 | 60 | 72 | 43 | 40 |
| Height (m) | 168 | 177 | 167 | 160 | 140 | 153 | 159 |
| Weight (kg) | 70 | 72 | 54 | 57 | 64 | 54 | 73 |
| Time since stroke (months/days) | 12.6 | 6.4 | 7.2 | 12.4 | 5.4 | 12.6 | 6.3 |
| Stroke location (right/left) | L | R | L | L | L | R | L |
| Dominant side (right/left) | R | L | R | R | R | R | R |
| List of Parameters (Measures) | |
|---|---|
| E1 | First extension peak (◦/s) |
| F1 | First flexion peak (◦/s) |
| E1Amp | F1 − E1 (◦) |
| F1Amp | F1-initial angle (◦) |
| PA | Measure between the final angle and the initial angle (◦) |
| RI | F1 Amp/PA (◦)/relaxation index |
| ERI | E1 Amp/PA (◦)/extension relaxation index |
| D | Duration from the start angle to the end angle (◦) |
| ω | Natural frequency |
| B | Damping coefficient |
| K | Stiffness coefficient |
| ζ | Damping ratio |
| Scales | Subjects | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| #1 | #2 | #3 | #4 | #5 | #6 | #7 | Median | SD | |
| MAS | - | 2 | - | 2 | 2 | 1 | 1 | 2.0 | 0.54 |
| FM | 14 | 34 | 18 | 35 | 56 | 39 | 38 | 35 | 14.02 |
| Motor Activity Log—amount of limb use | 0.0 | 1.5 | 0.5 | 2.0 | 2.0 | 2.5 | 2.0 | 2 | 0.91 |
| Motor Activity Log—quality of use | 0.0 | 1.0 | 0.0 | 0.5 | 1.5 | 1.3 | 1.0 | 1.0 | 0.60 |
| Variable | Subjects | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| #1 | #2 | #3 | #4 | #5 | #6 | #7 | Median | SD | |
| Onset angle (°) | 89 | 86.2 | 74.4 | 79 | 81.8 | 80.4 | 75.7 | 80.40 | 5.28 |
| E1 amp | 172.6 | 101 | 115.2 | 150.5 | 108.8 | 117.3 | 112.2 | 115.20 | 26.05 |
| F1 amp | 0.2 | 50.8 | 33.2 | 6.5 | 46.9 | 42.7 | 28.1 | 33.20 | 19.72 |
| Plat Amp | 66.3 | 62.6 | 50.9 | 68.8 | 54.2 | 70.8 | 53 | 62.60 | 8.16 |
| RI | 0.003 | 0.812 | 0.652 | 0.094 | 0.865 | 0.60 | 0.53 | 0.60 | 0.33 |
| ERI | 2.60 | 1.61 | 2.26 | 2.18 | 2.00 | 1.65 | 2.11 | 2.12 | 0.34 |
| Natural frequency (rad/seg) | 6.15 | 6.75 | 1.45 | 14.27 | 9.6 | 13.65 | 11.62 | 9.66 | 4.59 |
| K (Nm/rad) | 0.355 | 0.448 | 0.013 | 1.78 | 0.61 | 1.10 | 0.79 | 0.67 | 0.58 |
| B (Nm.s.rad) | 0.029 | 0.025 | 0.003 | 0.047 | 0.024 | 0.025 | 0.030 | 0.03 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Lima, M.S.N.; dos Santos Couto Paz, C.C.; Ribeiro, T.G.; Fachin-Martins, E. Assessment of Passive Upper Limb Stiffness and Its Function in Post-Stroke Individuals Wearing an Inertial Sensor during the Pendulum Test. Sensors 2023, 23, 3487. https://doi.org/10.3390/s23073487
de Lima MSN, dos Santos Couto Paz CC, Ribeiro TG, Fachin-Martins E. Assessment of Passive Upper Limb Stiffness and Its Function in Post-Stroke Individuals Wearing an Inertial Sensor during the Pendulum Test. Sensors. 2023; 23(7):3487. https://doi.org/10.3390/s23073487
Chicago/Turabian Stylede Lima, Milene Soares Nogueira, Clarissa Cardoso dos Santos Couto Paz, Thais Gontijo Ribeiro, and Emerson Fachin-Martins. 2023. "Assessment of Passive Upper Limb Stiffness and Its Function in Post-Stroke Individuals Wearing an Inertial Sensor during the Pendulum Test" Sensors 23, no. 7: 3487. https://doi.org/10.3390/s23073487