
Treatment of the Paretic Hand with a Robotic Glove Combined with Physiotherapy in a Patient Suffering from Traumatic Tetraparesis: A Case Report
 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Information
- Normal range of motion (ROM)
- Sufficient static and dynamic trunk control
- A slight increase in tone of the lower limbs, in particular of the knee flexors and extensors, hip adductors, and bilateral tibiotarsal plantiflexors
- Residual motor skills absent in the lower limbs, left triceps, wrist flexors, and hand muscles
- Presence of proximal motor quotas at the level of the pronators and wrist extensors (MRC 4-5/5) and a hint of contraction of the right triceps (MRC: 1/5).
2.2. Clinical Findings
2.3. Intervention
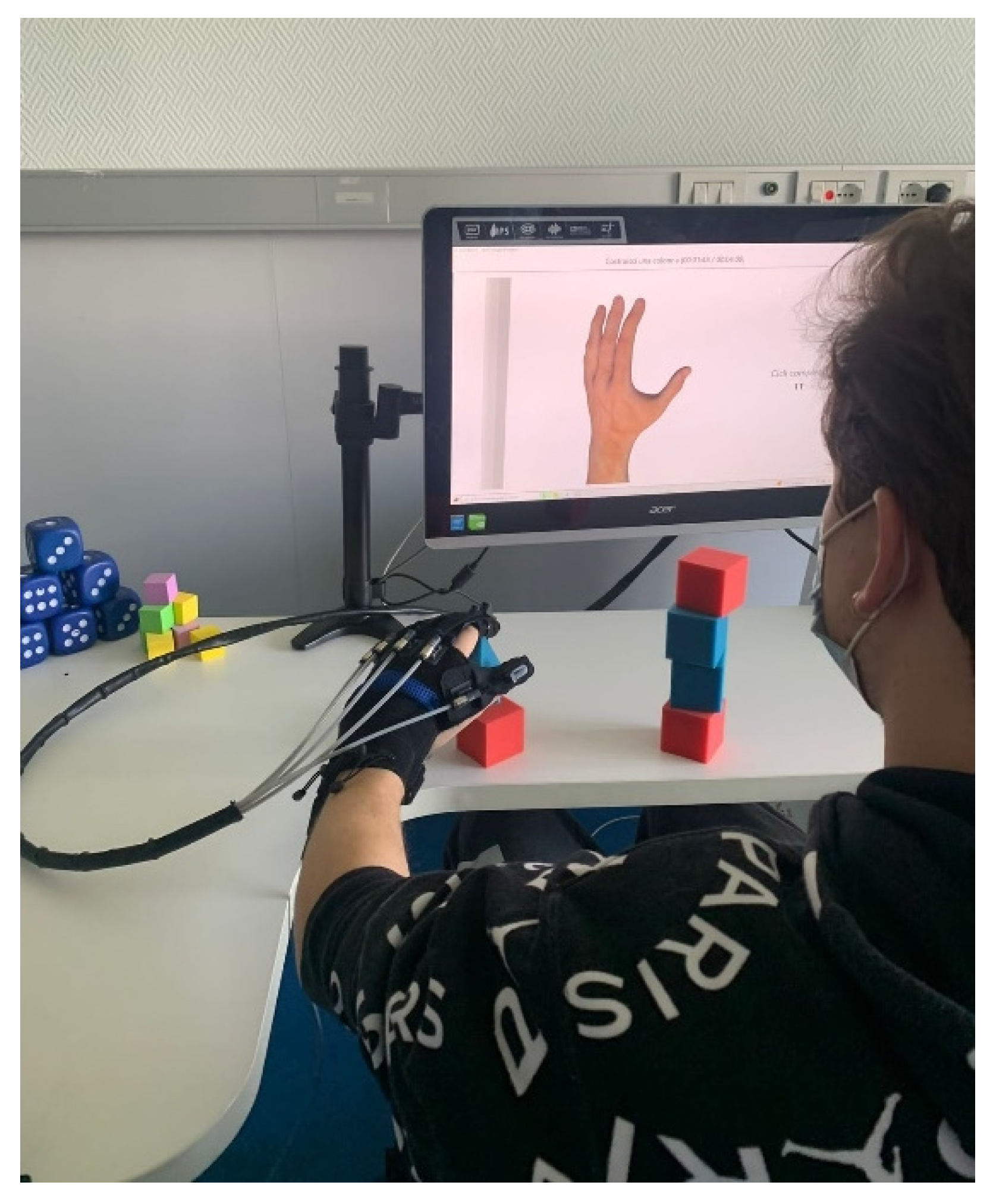
2.3.1. Robotic Therapy
- Passive mobilization exercises (the movements are carried out entirely by the device);
- Active-assisted exercises with graphic interface (the patient trains in flexion extension of the fingers thanks to motivating games; the motors support and integrate the patient’s voluntary movements only to the extent necessary) or with real objects (the patient trains fine grip);
- Interactive games (the patient can improve dexterity).
2.3.2. Conservative Treatment
- Muscle stretching of the tendons of the finger flexors and wrist flexors. This exercise was proposed with the aim of decreasing the tendon retractions, which caused a limitation of the movement in extension to the last degrees of the 4th and 5th fingers.
- Muscle strengthening exercises in the flexion movement of the fingers and grip (flexion and hold for 5 s, 10 repetitions for at least 2 sets). To improve the strength and resistance of the fingers, an instrument was used that was able to provide each finger with resistance in the flexion movement (closing of the hand) at the same time, through five independent springs. In this way, the activation was sought not only of the extrinsic muscles of the hand, but also of the intrinsic ones.
- Muscle strengthening exercises in the wrist extension movement (15 repetitions for at least two sets). This exercise aimed at strengthening pure extension, trying to avoid compensatory movements—such as radial deviation, forearm supination, or shoulder flexion and abduction. It was performed against a resistance given by an elastic band, which limited its radial deviation, leaving the extension movement free.
- Rhythmic stabilization exercise of the wrist (20 s for at least two series). In this exercise, the patient was asked to maintain a neutral wrist position while holding an object. The therapist created destabilizations through small pushes in all directions, which the patient had to counteract.
- Facilitation of muscle recruitment of the wrist flexors (at least 10 repetitions). The therapist provided the patient with sensory-motor facilitation stimuli, with the aim of improving the activation and muscle recruitment of the forearm and wrist muscles in the flexion movement.
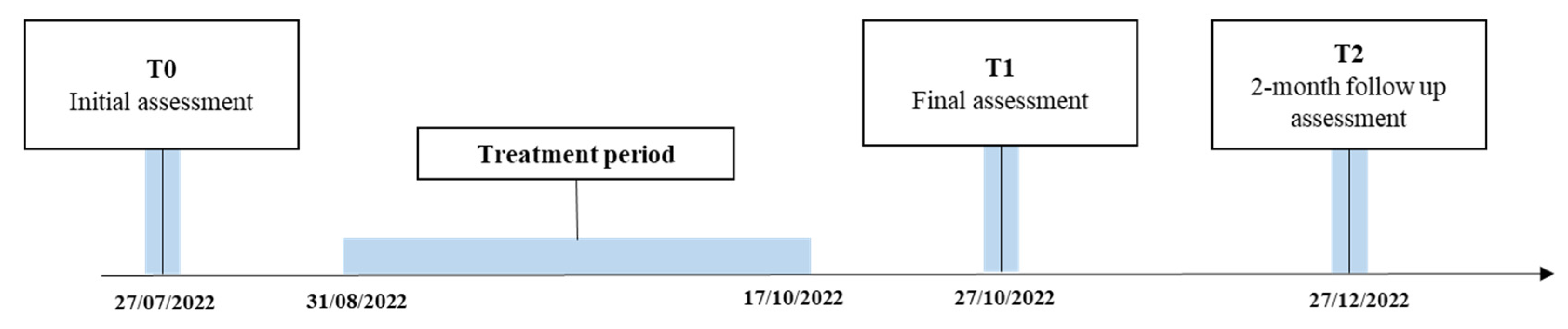
2.4. Outcome Measurement
- Fugl Meyer Assessment for Upper Limb (FMA/UE). This scale is one of the core measures to be used in the evaluation of patients with central nervous system (CNS) pathologies, such as stroke and SCI, as it evaluates the residual functionality of the affected limb(s). A higher score represents a greater functionality of the limb. The scale is comprised of five domains with 155 items in total:
- Motor functioning (0–66 points)
- Sensory functioning (0–12 points)—Evaluates light touch on two surfaces of the arm and position sense for shoulder, elbow, wrist and thumb joints;
- Joint range of motion of shoulder, elbow, forearm, wrist, and fingers (0–24 points);
- Joint pain (0–24).
- Disability of the Arm, Shoulder and Hand (DASH). This is a self-administered questionnaire that investigates the disability caused by the patient’s upper limb disorders in carrying out the ADLs. It consists of a total of 38 questions, divided into a main module (30 questions), which investigates hand functionality in ADLs and in recreational activities, the patient’s perception of disability in work and social activities, the presence of symptoms and difficulties related to limb and two optional modules, one question concerning working (four questions), and one question concerning sports/recreational activities (four questions). The score is expressed as a percentage from 0 to 100, where increasing the percentage will correspond to a greater disability.
- Nine Hole Peg Test (9HPT). This test is considered the gold standard for measuring manual dexterity in patients with upper limb disability. The test is performed by picking up the nine pegs, one at a time, with one hand, and inserting them into the nine holes provided. The test must be carried out as quickly as possible, since the measure used for the evaluation is precisely the time taken by the patient to complete the task.
- Range of Motion (ROM). Passive range of motion of the shoulder, elbow, wrist, and hand was measured using a goniometer. The measurements are expressed in degrees to evaluate all the movements of the upper limb joints.
- Medical Research Council (MRC). Upper limb muscle strength was measured with the MRC scale. In this assessment, the patient performs a movement, and the therapist offers an opposing resistance to it. A score is given from 0 (no contraction) to 5 (normal strength, movement against maximum resistance).
2.5. Force Assessment System Based on Virtual Reality Games
3. Results
Force Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wyndaele, M.; Wyndaele, J.J. Incidence, Prevalence and Epidemiology of Spinal Cord Injury: What Learns a Worldwide Literature Survey? Spinal. Cord 2006, 44, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Kirshblum, S.; Snider, B.; Rupp, R.; Read, M.S. Updates of the International Standards for Neurologic Classification of Spinal Cord Injury: 2015 and 2019. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 319–330. [Google Scholar] [CrossRef] [PubMed]
- Ding, W.; Hu, S.; Wang, P.; Kang, H.; Peng, R.; Dong, Y.; Li, F. Spinal Cord Injury: The Global Incidence, Prevalence, and Disability From the Global Burden of Disease Study 2019. Spine (Phila Pa 1976) 2022, 47, 1532–1540. [Google Scholar] [CrossRef]
- Baricich, A.; Amico, A.P.; Zampolini, M.; Gimigliano, F.; Cisari, C.; Fiore, P. People with Spinal Cord Injury in Italy. Am. J. Phys. Med. Rehabil. 2017, 96, S80–S82. [Google Scholar] [CrossRef]
- Morone, G.; de Sire, A.; Martino Cinnera, A.; Paci, M.; Perrero, L.; Invernizzi, M.; Lippi, L.; Agostini, M.; Aprile, I.; Casanova, E.; et al. Upper Limb Robotic Rehabilitation for Patients with Cervical Spinal Cord Injury: A Comprehensive Review. Brain Sci. 2021, 11, 1630. [Google Scholar] [CrossRef] [PubMed]
- de Miguel-Rubio, A.; Dolores Rubio, M.; Alba-Rueda, A.; Salazar, A.; Moral-Munoz, J.A.; Lucena-Anton, D. Virtual Reality Systems for Upper Limb Motor Function Recovery in Patients With Spinal Cord Injury: Systematic Review and Meta-Analysis. JMIR Mhealth Uhealth 2020, 8, e22537. [Google Scholar] [CrossRef]
- Sullivan, K.J.; Cen, S.Y. Model of Disablement and Recovery: Knowledge Translation in Rehabilitation Research and Practice. Phys. Ther. 2011, 91, 1892–1904. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Battistuzzo, C.R.; Zoghi, M.; Galea, M.P. Effects of Training on Upper Limb Function after Cervical Spinal Cord Injury: A Systematic Review. Clin. Rehabil. 2015, 29, 3–13. [Google Scholar] [CrossRef]
- Ozelie, R.; Gassaway, J.; Buchman, E.; Thimmaiah, D.; Heisler, L.; Cantoni, K.; Foy, T.; Hsieh, C.H.; Smout, R.J.; Kreider, S.E.D.; et al. Relationship of Occupational Therapy Inpatient Rehabilitation Interventions and Patient Characteristics to Outcomes Following Spinal Cord Injury: The SCIRehab Project. J. Spinal. Cord Med. 2012, 35, 527–546. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Lee, B.S.; Lee, H.J.; Kim, H.R.; Cho, D.Y.; Lim, J.E.; Kim, J.J.; Kim, H.Y.; Han, Z.A. Clinical Efficacy of Upper Limb Robotic Therapy in People with Tetraplegia: A Pilot Randomized Controlled Trial. Spinal. Cord 2019, 57, 49–57. [Google Scholar] [CrossRef]
- Mekki, M.; Delgado, A.D.; Fry, A.; Putrino, D.; Huang, V. Robotic Rehabilitation and Spinal Cord Injury: A Narrative Review. Neurotherapeutics 2018, 15, 604–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Casadio, M.; Pressman, A.; Acosta, S.; Danzinger, Z.; Fishbach, A.; Mussa-Ivaldi, F.A.; Muir, K.; Tseng, H.; Chen, D. Body Machine Interface: Remapping Motor Skills after Spinal Cord Injury. IEEE Int. Conf. Rehabil. Robot 2011, 2011. [Google Scholar] [CrossRef]
- Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; de los Reyes-Guzmán, A.; Aznar, M.A.; Alcubilla, C.; Pérez-Nombela, S.; del Ama-Espinosa, A.; Polonio-López, B.; Gil-Agudo, Á. Upper Limb Rehabilitation after Spinal Cord Injury: A Treatment Based on a Data Glove and an Immersive Virtual Reality Environment. Disabil. Rehabil. Assist. Technol. 2016, 11, 462–467. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.J.; Lee, J.K.; Lee, S.M. Effects of Robot-Assisted Therapy on Upper Extremity Function and Activities of Daily Living in Hemiplegic Patients: A Single-Blinded, Randomized, Controlled Trial. Technol. Health Care 2018, 26, 659–666. [Google Scholar] [CrossRef]
- Vanoglio, F.; Bernocchi, P.; Mulè, C.; Garofali, F.; Mora, C.; Taveggia, G.; Scalvini, S.; Luisa, A. Feasibility and Efficacy of a Robotic Device for Hand Rehabilitation in Hemiplegic Stroke Patients: A Randomized Pilot Controlled Study. Clin. Rehabil. 2017, 31, 351–360. [Google Scholar] [CrossRef] [PubMed]
- Miccinilli, S.; Bravi, M.; Foti, C.; Morrone, M.; Maselli, M.; Santacaterina, F.; Scotto Di Luzio, F.; Zollo, L.; Sterzi, S.; Bressi, F. Robotic Hand Treatment of Patients Affected by Chronic Stroke: A Monocentric Longitudinal Pilot Study. J. Biol. Regul. Homeost. Agents 2020, 34, 79–86, Technology in Medicine. [Google Scholar]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D. The CARE Guidelines: Consensus-Based Clinical Case Reporting Guideline Development. Glob. Adv. Health Med. 2013, 2, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SINFONIA—Gloreha. Available online: https://www.gloreha.com/sinfonia/ (accessed on 24 January 2023).
- Lapresa, M.; Lauretti, C.; Luzio, F.S.d.; Bressi, F.; Santacaterina, F.; Bravi, M.; Guglielmelli, E.; Zollo, L.; Cordella, F. Development and Validation of a System for the Assessment and Recovery of Grip Force Control. Bioengineering 2023, 10, 63. [Google Scholar] [CrossRef]
- Bressi, F.; Santacaterina, F.; Cricenti, L.; Campagnola, B.; Nasto, F.; Assenza, C.; Morelli, D.; Cordella, F.; Lapresa, M.; Zollo, L.; et al. Robotic-Assisted Hand Therapy with Gloreha Sinfonia for the Improvement of Hand Function after Pediatric Stroke: A Case Report. Appl. Sci. 2022, 12, 4206. [Google Scholar] [CrossRef]
- Kurillo, G.; Zupan, A.; Bajd, T. Force Tracking System for the Assessment of Grip Force Control in Patients with Neuromuscular Diseases. Clin. Biomech. 2004, 19, 1014–1021. [Google Scholar] [CrossRef]
- McKight, P.E.; Najab, J. Kruskal-Wallis Test. In The Corsini Encyclopedia of Psychology; Wiley: New York, NY, USA, 2010. [Google Scholar] [CrossRef]
- Armstrong, R.A. When to Use the Bonferroni Correction. Ophthalmic Physiol. Opt. 2014, 34, 502–508. [Google Scholar] [CrossRef] [PubMed]
- Cappello, L.; Meyer, J.T.; Galloway, K.C.; Peisner, J.D.; Granberry, R.; Wagner, D.A.; Engelhardt, S.; Paganoni, S.; Walsh, C.J. Assisting Hand Function after Spinal Cord Injury with a Fabric-Based Soft Robotic Glove. J. Neuroeng. Rehabil. 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Francisco, G.E.; Yozbatiran, N.; Berliner, J.; O’Malley, M.K.; Pehlivan, A.U.; Kadivar, Z.; Fitle, K.; Boake, C. Robot-Assisted Training of Arm and Hand Movement Shows Functional Improvements for Incomplete Cervical Spinal Cord Injury. Am. J. Phys. Med. Rehabil. 2017, 96, S171–S177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kousaka, H.; Mizoguchi, H.; Yoshikawa, M.; Tanaka, H.; Matsumoto, Y. Role Analysis of Dominant and Non-Dominant Hand in Daily Life. In Proceedings of the 2013 IEEE International Conference on Systems, Man, and Cybernetics, Manchester, UK, 13–16 October 2013; pp. 3972–3977. [Google Scholar] [CrossRef]
- Osuagwu, B.A.C.; Timms, S.; Peachment, R.; Dowie, S.; Thrussell, H.; Cross, S.; Shirley, R.; Segura-Fragoso, A.; Taylor, J. Home-Based Rehabilitation Using a Soft Robotic Hand Glove Device Leads to Improvement in Hand Function in People with Chronic Spinal Cord Injury: A Pilot Study. J. Neuroeng. Rehabil. 2020, 17, 1–15. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Exercise | Description | Aim of the Exercise |
|---|---|---|
| Dice in the box | To grab the dice and place them inside a box, and vice versa, take as well as to take them out of the box and place them on the table. | To seek the activation and recruitment of the whole limb, starting from the shoulder, elbow, and finally the hand. |
| Build a pyramid | To grab the dice and place them in order to build a pyramid on the table. Once the exercise was completed, the dice had to be returned to their starting point. | To improve the recruitment of the whole limb and the grip of the object. |
| Build a column | To grab the dice and place them in order to build a column on the table. Once the exercise was completed, the dice had to be returned to their starting point | To improve reaching, precision, and movement control, especially in the release phase. |
| Pick the flower | Take the flower on the screen, holding it and drop it into a box | To improve the functional grip of the 1st, 2nd, and 3rd finger. Therefore, to work on the fine grip of small objects, a small die was used (volume of 8 cm3). |
| Assessment | T0 | T1 | T2 | |
|---|---|---|---|---|
| FM-UE | ||||
| RIGHT SIDE | Motor functioning Sensory functioning Joint ROM Joint Pain | 58 12 23 24 | 59 12 24 24 | 60 12 24 24 |
| LEFT SIDE | Motor functioning Sensory functioning Joint ROM Joint Pain | 58 12 23 24 | 59 12 24 24 | 60 12 24 24 |
| NHPT | Right Side Left Side | 61 s 56 s | 58 s 48 s | 39.4 s 60.5 s |
| DASH | 34% | 33% | 34% |
| District | ROM Left (°) | ROM Right (°) | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Shoulder | ||||||
| Flexion | 180 | 180 | 180 | 180 | 180 | 180 |
| Extension | 60 | 60 | 60 | 60 | 60 | 60 |
| Abduction | 180 | 180 | 135 | 180 | 180 | 135 |
| Horizontal adduction | 45 | 45 | 45 | 45 | 45 | 45 |
| Horizontal abduction | 135 | 135 | 135 | 135 | 135 | 135 |
| Internal rotation | 70 | 70 | 70 | 70 | 70 | 70 |
| External rotation | 90 | 90 | 90 | 90 | 90 | 90 |
| Elbow-Forearm | ||||||
| Flexion | 150 | 150 | 150 | 150 | 150 | 150 |
| Extension | 0 | 0 | 0 | 0 | 0 | 0 |
| Supination | 80 | 80 | 80 | 80 | 80 | 80 |
| Pronation | 80 | 80 | 80 | 80 | 80 | 80 |
| Wrist | ||||||
| Flexion | 70 | 70 | 70 | 70 | 70 | 70 |
| Extension | 70 | 70 | 70 | 70 | 70 | 70 |
| Ulnar Deviation | 30 | 20 | 30 | 30 | 30 | 30 |
| Radial Deviation | 20 | 20 | 20 | 20 | 20 | 20 |
| Hand | ||||||
| MCP Flexion | 90 | 90 | 90 | 90 | 90 | 90 |
| MCP Extension | 20 | 20 | 20 | 20 | 20 | 20 |
| IFP Flexion | 90 | 90 | 90 | 90 | 90 | 90 |
| IFP Extension | 10 | 0 | 20 | 10 | 0 | 20 |
| District | Left | Right | ||||
|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | |
| Shoulder | ||||||
| Flexion | 5 | 5 | 5 | 5 | 5 | 5 |
| Extension | 5 | 5 | 5 | 5 | 5 | 5 |
| Abduction | 5 | 5 | 5 | 5 | 5 | 5 |
| Adduction | 5 | 5 | 5 | 5 | 5 | 5 |
| Horizontal adduction | 5 | 5 | 5 | 5 | 5 | 5 |
| Horizontal abduction | 5 | 5 | 5 | 5 | 5 | 5 |
| Internal rotation | 5 | 5 | 5 | 5 | 5 | 5 |
| External rotation | 5 | 5 | 5 | 5 | 5 | 5 |
| Elbow-Forearm | ||||||
| Flexion | 5 | 5 | 5 | 5 | 5 | 5 |
| Extension | 4 | 4 | 4 | 4 | 4 | 3 |
| Supination | 5 | 5 | 5 | 5 | 5 | 5 |
| Pronation | 5 | 5 | 5 | 5 | 5 | 5 |
| Wrist | ||||||
| Flexion | 5 | 5 | 5 | 5 | 5 | 5 |
| Extension | 1 | 3 | 3 | 1 | 3 | 3 |
| Hand | ||||||
| MCP Flexion | 2 | 3 | 3 | 2 | 3 | 3 |
| MCP Extension | 0 | 1 | 1 | 0 | 1 | 1 |
| Finger abduction | 0 | 0 | 0 | 0 | 0 | 0 |
| IFP Flexion | 1 | 1 | 1 | 1 | 1 | 1 |
| IFP Extension | 0 | 0 | 0 | 0 | 0 | 0 |
| Thumb opposition | 0 | 0 | 0 | 0 | 0 | 0 |
| Thumb extension | 0 | 0 | 0 | 0 | 0 | 0 |
| Hand | T0 | T1 | T2 |
|---|---|---|---|
| Right Hand | 0.66 N | 1.37 N | 1.70 N |
| Left Hand | 0.81 N | 1.34 N | 1.67 N |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bressi, F.; Cricenti, L.; Bravi, M.; Pannunzio, F.; Cordella, F.; Lapresa, M.; Miccinilli, S.; Santacaterina, F.; Zollo, L.; Sterzi, S.; et al. Treatment of the Paretic Hand with a Robotic Glove Combined with Physiotherapy in a Patient Suffering from Traumatic Tetraparesis: A Case Report. Sensors 2023, 23, 3484. https://doi.org/10.3390/s23073484
Bressi F, Cricenti L, Bravi M, Pannunzio F, Cordella F, Lapresa M, Miccinilli S, Santacaterina F, Zollo L, Sterzi S, et al. Treatment of the Paretic Hand with a Robotic Glove Combined with Physiotherapy in a Patient Suffering from Traumatic Tetraparesis: A Case Report. Sensors. 2023; 23(7):3484. https://doi.org/10.3390/s23073484
Chicago/Turabian StyleBressi, Federica, Laura Cricenti, Marco Bravi, Fabiana Pannunzio, Francesca Cordella, Martina Lapresa, Sandra Miccinilli, Fabio Santacaterina, Loredana Zollo, Silvia Sterzi, and et al. 2023. "Treatment of the Paretic Hand with a Robotic Glove Combined with Physiotherapy in a Patient Suffering from Traumatic Tetraparesis: A Case Report" Sensors 23, no. 7: 3484. https://doi.org/10.3390/s23073484