1. Introduction
Diabetes is a chronic illness that affects 537 million adults around the world and this number is expected to rise to 783 million people by 2045 [
1]. People suffering from diabetes experience abnormal blood glucose levels (BGL), mainly owing to the absence or unregulated production of insulin. For example, in the case of type II diabetes, which accounts for 90% of the cases, the body does not produce enough insulin or is resistant to it, hence causing prolonged high levels of blood glucose [
2]. When left unmanaged and untreated, diabetes causes serious health problems and complications that can affect the eyes, heart, kidneys, and blood vessels. Diabetes may even have life-threatening consequences [
3], with 6.7 million people worldwide losing their lives to diabetes in 2021 [
4]. However, this chronic illness can be cured or delayed when it is in its pre-diabetic stage, and its complications prevented under the correct diet, improved lifestyle, and constant BGL monitoring, a subject of this study.
To minimize the complications and adverse health effects of diabetes, it is crucial for people with diabetes (PWD) to monitor their BGLs several times per day (4–10 times), typically before and after meals, and especially if they are under insulin treatment [
5]. Currently available out-of-clinic blood glucose monitoring (BGM) devices include invasive and minimally invasive ones. Invasive BGM involves pricking the finger to extract a small amount of capillary blood using a lancet (small needle). The blood is then collected on a strip which is inserted into a portable machine that measures and displays the BG level [
6]. This method is not only painful, but also carries the risk of infection, and does not provide a continuous means for BGM. In addition, it is unsuitable for a wide range of populations, the elderly for example, who might lack fine control of their hands and fingers or have poor eyesight which prevents them from performing all the required steps of the measurement [
7].
Minimally invasive devices, on the other hand, do provide a more continuous form of BGM. However, these devices typically involve the temporary implantation of a micro-needle that senses BGL from the interstitial fluid. The main problems with such devices include drifts and lags between the BGL from the interstitial fluid versus true BGL, in addition to the high running cost associated with an implanted needle that needs to be disposed of every few days [
8].
With the ever-growing number of PWD and the shortcomings of current BGM systems, there is an urgent need for readily wearable, non-invasive devices for continuous BGM. In recent years, several such non-invasive methods have been investigated; these either rest upon the sampling of bodily fluids, such as urine, tears, and sweat, or are based on shining a light of a certain wavelength through the skin [
9]. While each method has its advantages and disadvantages [
10], optical methods, especially those pertaining to near-infrared (NIR) spectroscopy, has attracted much interest. The NIR region of the electromagnetic spectrum lies between 700–2500 nm. It penetrates the skin in the mm range, depending on the wavelength [
11], and has been adopted for the development of continuous non-invasive BGM devices at various body locations [
12,
13,
14,
15,
16,
17,
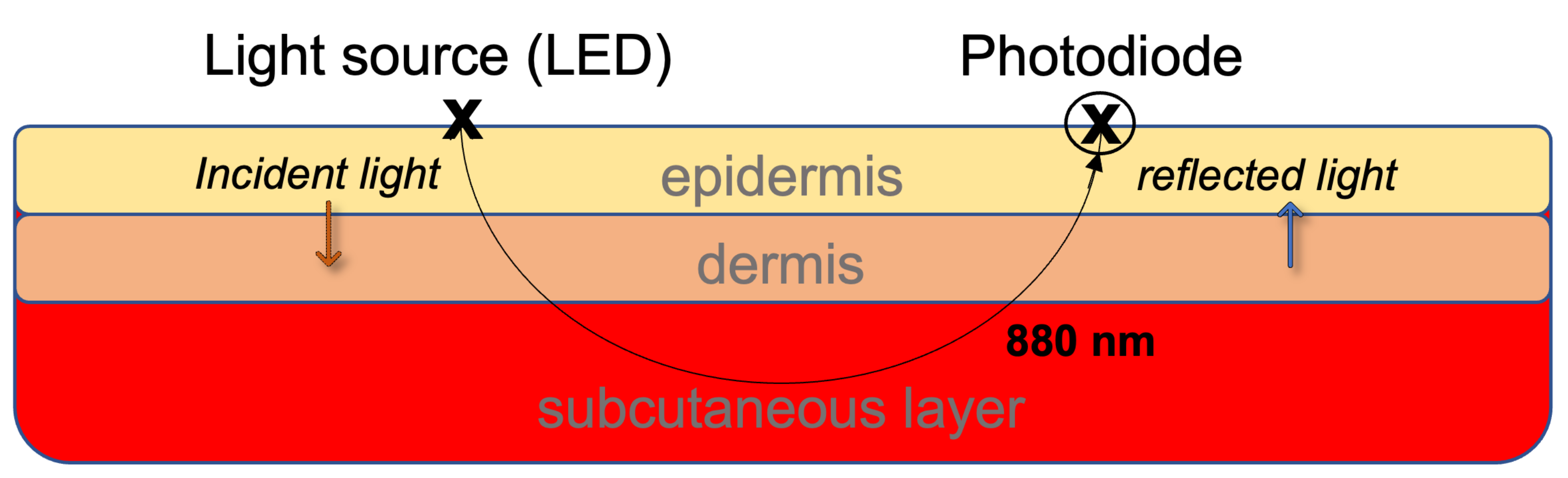
18]. These devices mainly derive the glucose level from features extracted from photoplethysmography (PPG) waveforms, which can be acquired from any part of the skin that has blood vessels [
19]—most commonly from the fingers, wrist, and earlobes. The PPG sensor used typically comprises light-emitting diodes (LED) of a certain wavelength(s) and a photodiode that receives the reflected light and is used to measure changes in blood volume in the tissue. It typically involves shining a light onto the skin and measuring the light intensity that is reflected back. This measurement is then used to calculate the amount of blood in the tissue and can provide information about heart rate, blood pressure, and other physiological parameters.
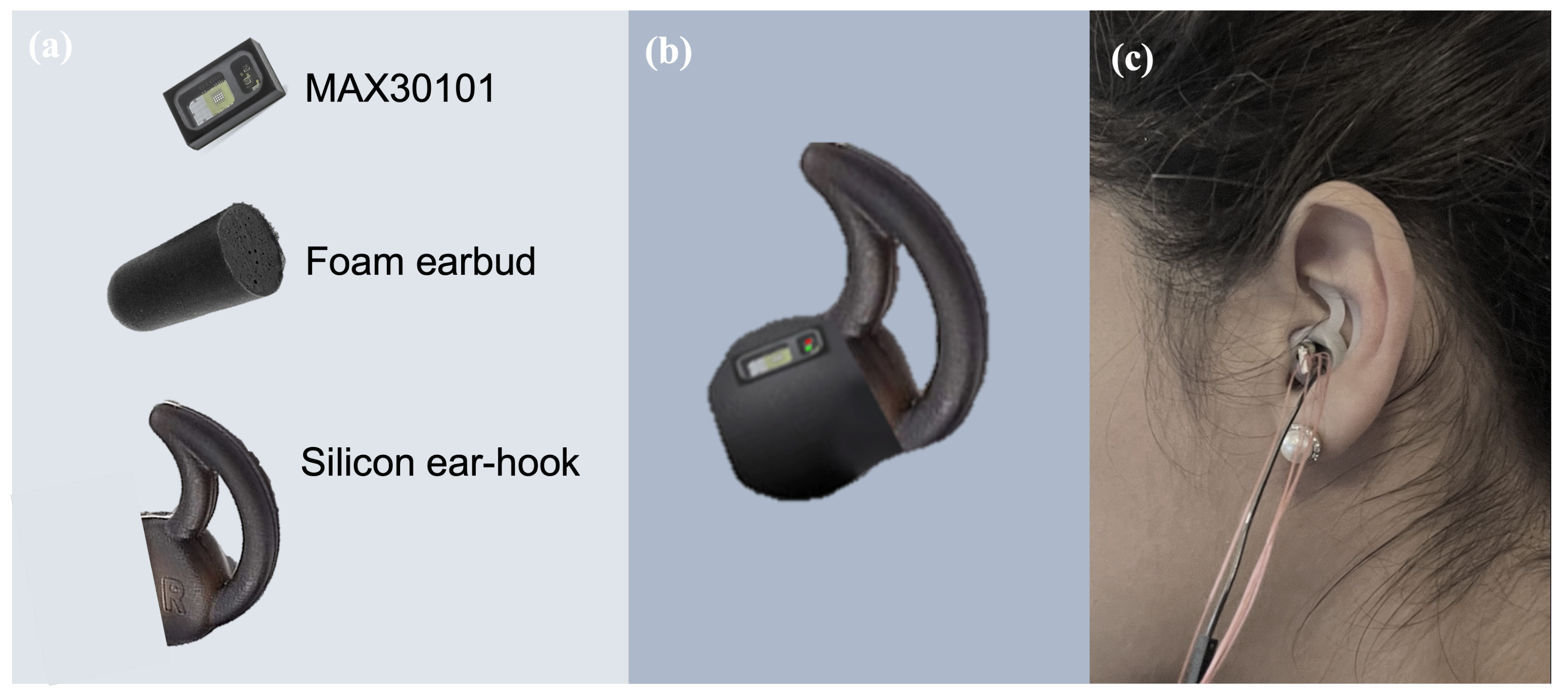
Recent advancements in wearable technology for vital signs monitoring have given rise to in-ear wearable devices, the so-called hearables [
20,
21]. Given the privileged position of the head on the human body, the ear provides a convenient and stable site for physiological measurement, while the ear canal also acts as an insulator of external electrical noise [
21]. Several studies have used the ear canal for general physiological sensing which includes electroencephalography (EEG) [
22,
23,
24], electrocardiography (ECG) [
25], and PPG [
26,
27,
28], and have reported promising results when compared to clinical devices.
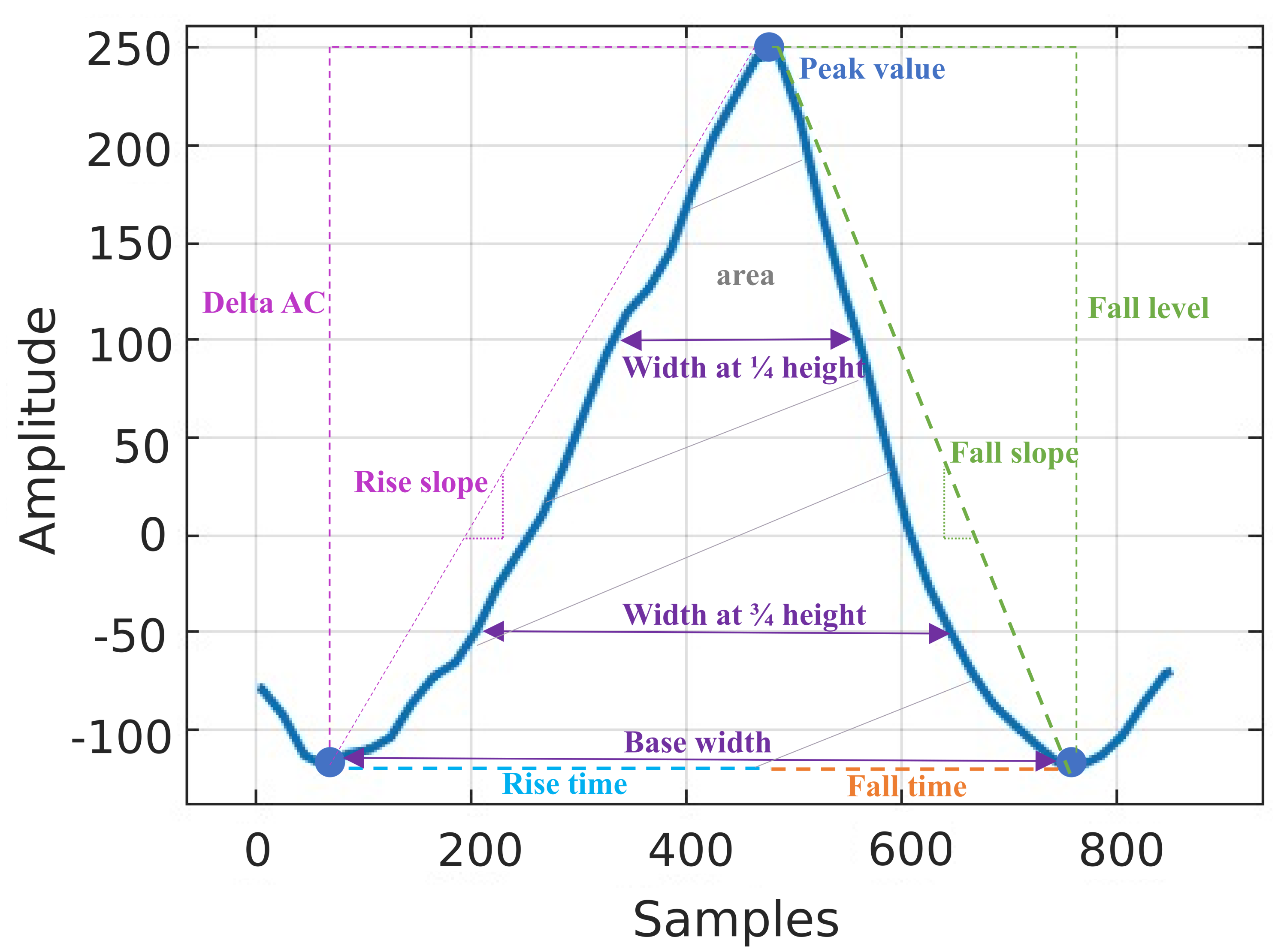
This work introduces the proof of concept for a continuously wearable in-ear non-invasive glucose monitoring system that uses a single NIR LED (880 nm) to acquire the PPG signal. For rigor, we considered a whole range of diabetic conditions—a non-diabetic control, pre-diabetic, type I, and type II diabetic subject with the considered BGL range varying from 63–345 mg/dL. The blood glucose levels were estimated based on 18 discriminating features, which were employed by machine learning algorithms to predict the BGL values from the corresponding PPG waveforms. The input variable selection (IVS) across all subjects indicates that the most discriminative features are related to the energy of the PPG cycle. As desired, all of the predicted BGLs fell in regions A and B of the Clarke error (CEG) plots—the regions with no adverse effects on clinical outcomes. To the best of our knowledge, the proposed system is the first to utilize the ear canal as a site of non-invasive blood glucose measurement through NIR spectroscopy and opens up avenues for unobtrusive 24/7 blood glucose monitoring in the community.
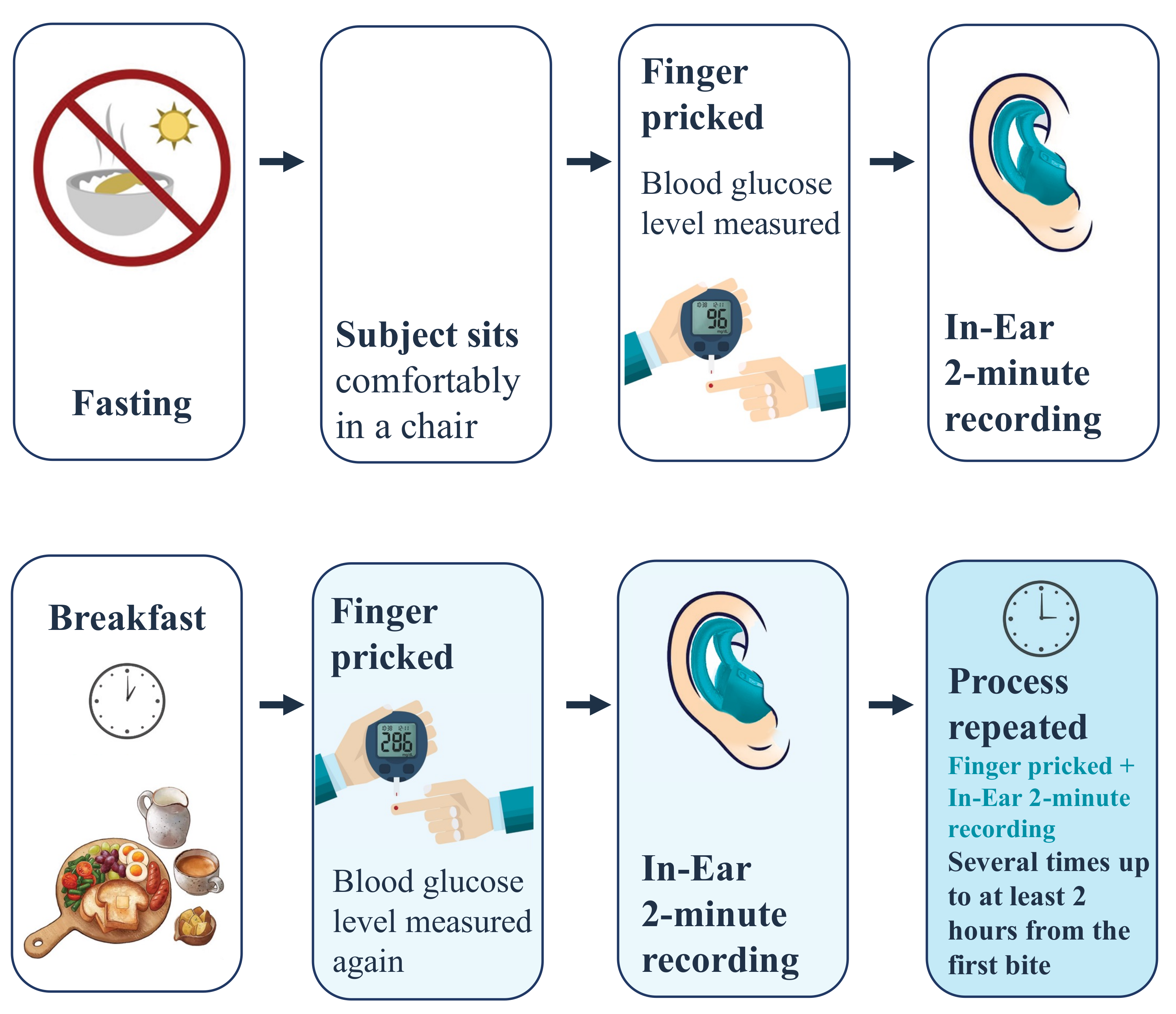
4. Results
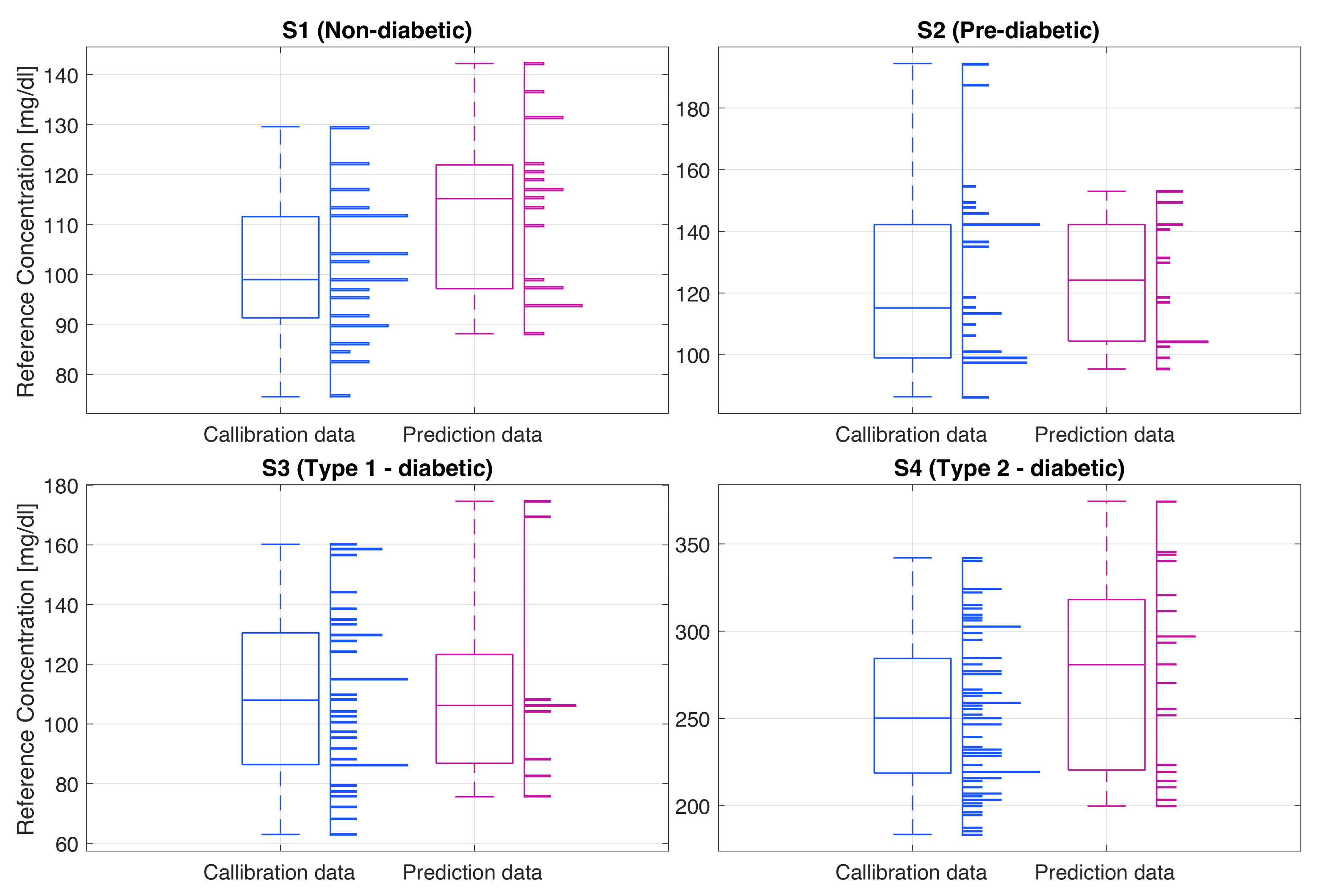
The gold standard glucose levels of the recorded subjects, shown in
Figure 8, were consistent with their health conditions. For the non-diabetic subject (S1) the glucose ranges were within the normal limits, typically 90 mg/dL while fasting, and with a maximum of 142 mg/dL typically half an hour after the meal, after which the BGL dropped back to around 90 mg/dL. Subject 2 (S2), a pre-diabetic, had a higher fasting glucose level of around 100 mg/dL and a maximum glucose value of 194 mg/dL. High BGL remained constant over a longer period of time, typically returning to the fasting level within about two hours from breakfast. The type I diabetic subject (S3) had hypoglycemic BGLs. This subject was using insulin to regulate the BGL, typically right before the meal, after an estimate of the number of carbohydrates in food. For this type of diabetes, as evident from the data, the glucose levels tend to be quite unpredictable; for example, they can be low both before and after the mean, or equally, they can be high both before and after the meal. The highest BGL can be seen in the type II diabetic subject (S4) where the fasting glucose was around 200 mg/dL and the maximum BGL after the meal was around 354 mg/dL. It is important to note that this subject does not inject any insulin, hence the constantly elevated BGL.
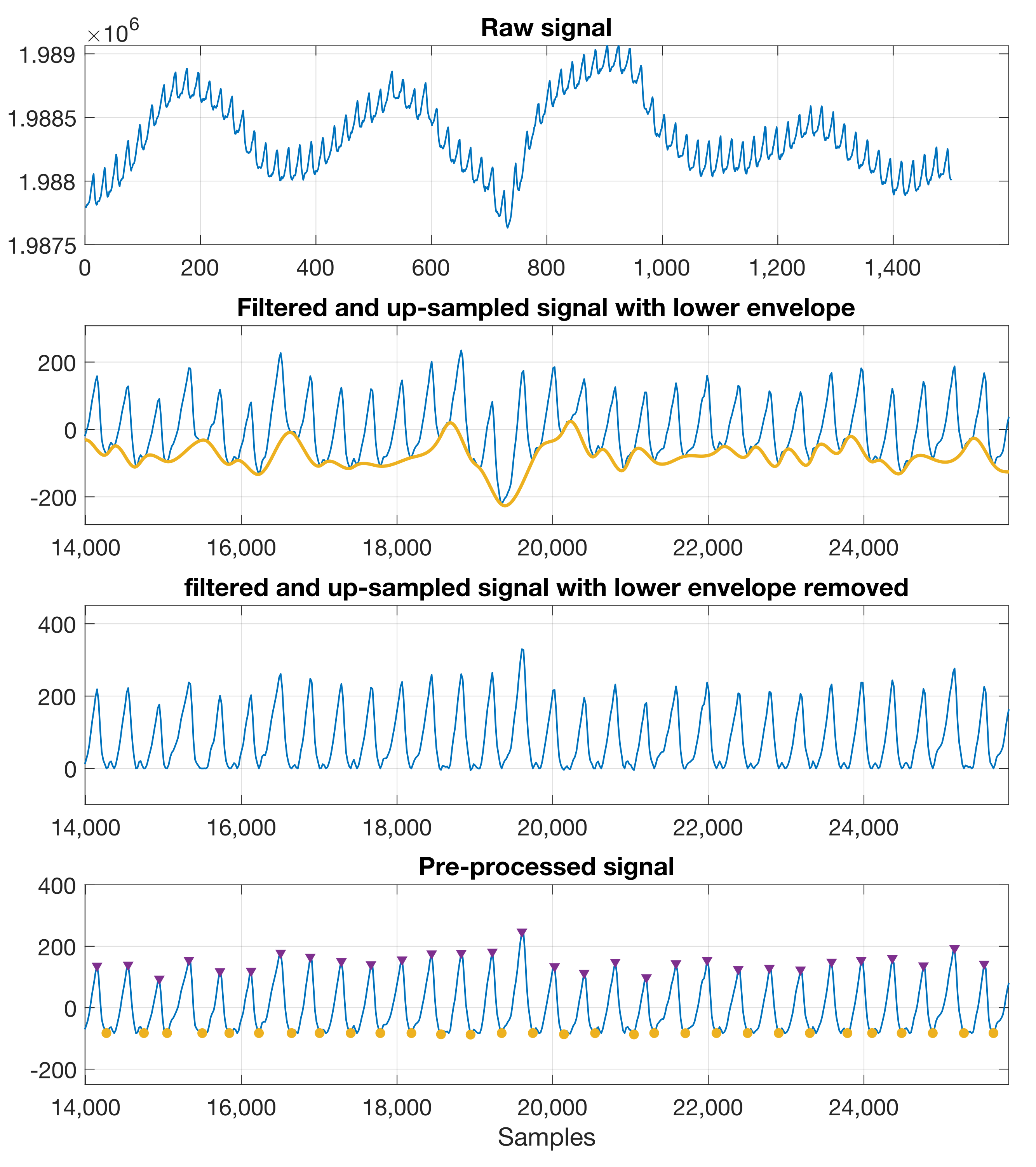
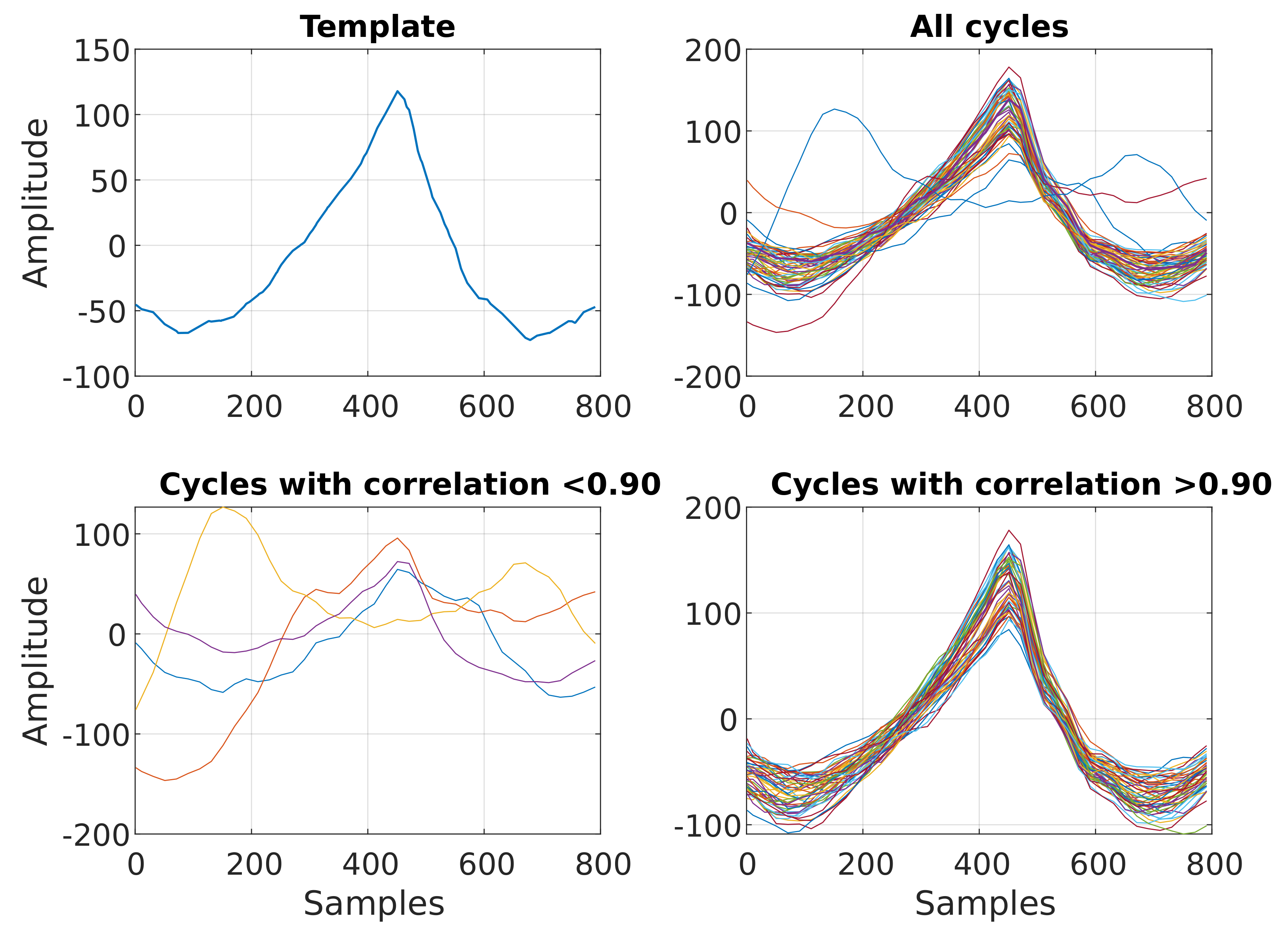
The PPG signals obtained from each subject using the in-ear PPG sensor showed clear systolic peaks, with an average of 80% of the cycles (no. of valid cycles in
Table 3) having a high correlation (r > 0.9) with the template cycle of the recording in hand, as shown in
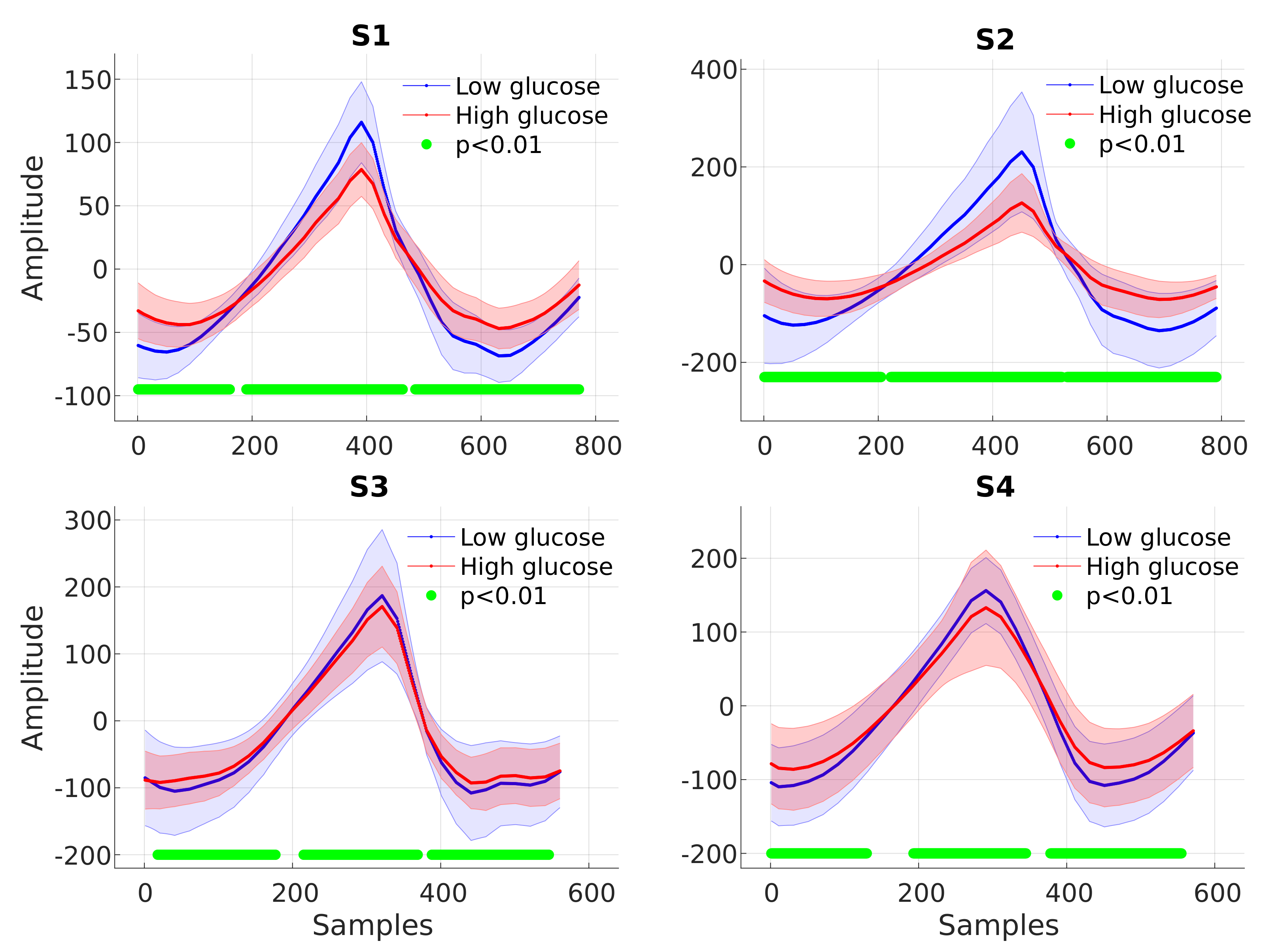
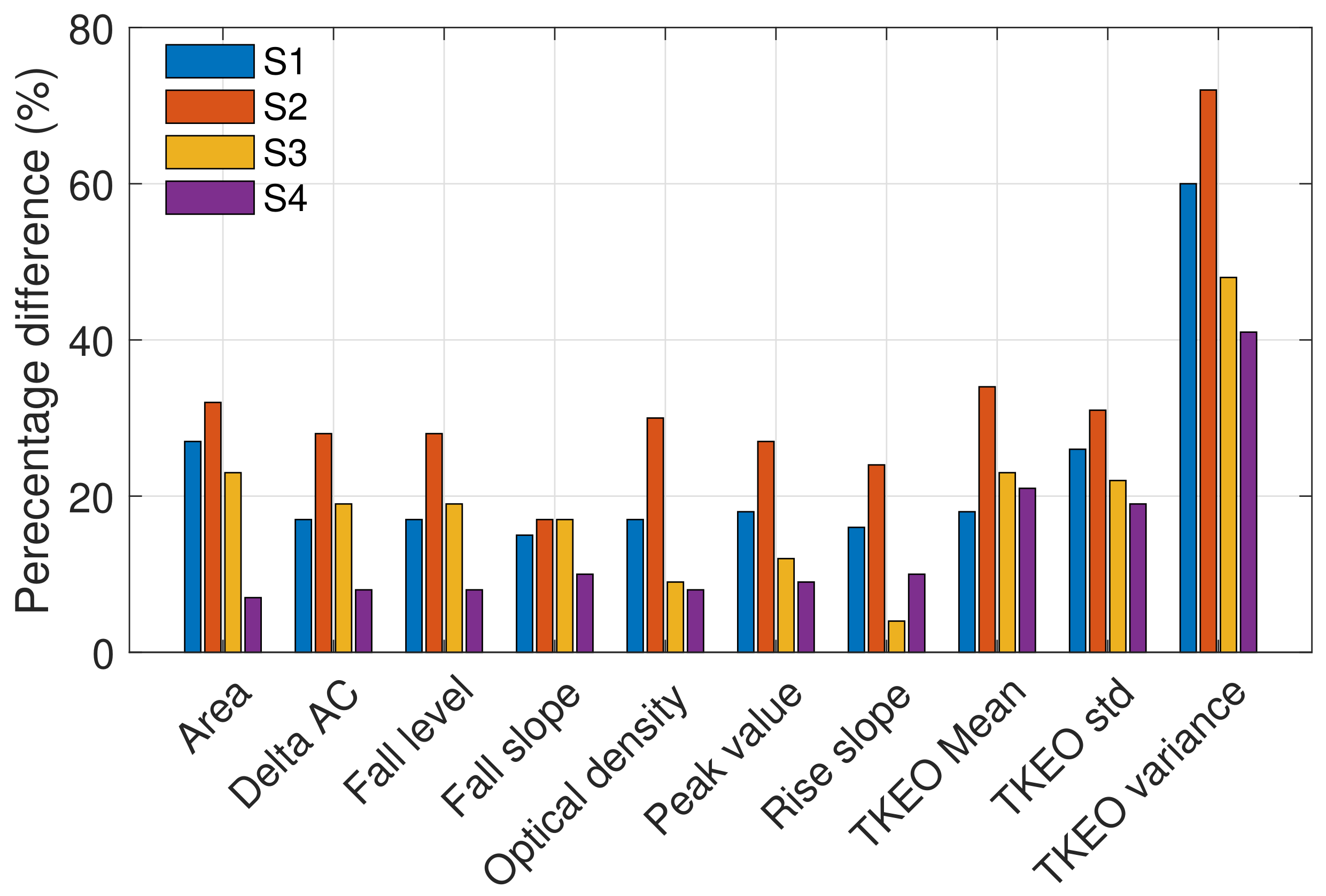
Figure 5. The highest number of discarded cycles was for subject S3; this is likely due to the subject moving their mouth, grinding their teeth, yawning, coughing, or due to sensor displacement. The clean cycles were split between the training and test sets, with the first seven days used to train the model and the last two days for testing. The ten most significant features which yielded statistically significant differences in high versus low blood glucose PPG cycles are presented in
Figure 9. Observe that the highest percentage differences are found for S1 and S2, while the lowest percentage difference can be observed in S4. Features calculated from the energy feature TKEO were constantly highly representative of BGLs in all subjects. The features extracted from training data were used to train different machine learning regression models. The best-performing models were ensemble regression trees; these models were optimized for each subject with hyperparameter ranges and validation results, as shown in
Table 4.
Figure 10 shows the CEG plot for each subject. Observe that, as desired, all the predicted BGL values reside within regions A and B of the CEG plots thus indicating no adverse effect on clinical decisions based on the proposed device. Moreover, on average 80% of the data for all subjects lie within region A of the CEG. The best prediction results, with around 90% of the predicted points in region A, were obtained for S1, followed by 83.3% for S2, while the lowest predicted points of 77% in region A were for S3 and S4, as shown in
Table 5. This is consistent with the fact that the lowest significant difference in high versus low BGL PPG cycles were observed for the untreated type II diabetes subject S4. Least-squares regression analysis indicated a significant positive correlation between the predicted and reference glucose concentrations in all subjects (
Table 6).
5. Discussion
The potential of the proposed method for continuous BGL monitoring is evidenced by 100% of the estimated BGL values falling within the clinically acceptable regions A and B of the CEG plots for all four subjects, as shown in
Figure 10. The estimated CEG values in Region A fall within 20% of the reference (correct) BGL value, which has no negative effect on the clinical decisions, while the values in Region B of CEG are more than 20% apart from the reference BGL value, but this has low to no impact on clinical outcome [
33] and does not lead to inappropriate treatment. This level of accuracy is particularly important for diagnosing hypoglycemia and hyperglycemia, where immediate intervention is required, as clinically wrong diagnosis may lead to the potentially fatal decision to inject insulin in patients with extremely low blood glucose levels. According to the tolerance range of the latest ISO standard (ISO: 15197:2015), the estimated blood glucose levels should be within ±15 mg/dL when the true value is <100 mg/dL, whereas values ≥100 mg/dL should be within ±20 mg/dL [
34]. Observe from
Figure 10 that the results for S1 and S2 meet these criteria with an average accuracy of 15 mg/dL (±9), while the estimated values for the type I diabetic S3 (accuracy: 19 ± 17 mg/dL) and type II diabetic S4 (35 ± 22 mg/dL) marginally fall outside the recommended range. This can be explained by the range of BGLs in this study being 2–3 times larger than those considered in the existing studies in the literature, with BGLs as high as 345.7 mg/dL for subject S4. For rigor, we also performed the analysis based on the median of PPG cycles, with the results very similar to those reported here which were obtained based on the means of PPG cycles.
Overall, the results obtained using the in-ear sensor are comparable to those obtained in previous studies for other PPG sites, as shown in
Table 7. In [
17] four different wavelengths were tested, with the best results obtained when all four wavelength measurements were used for estimating BGLs. The results in this work are consistent with the results in [
17] when considering data within their tested glucose range (70–152 mg/dL) and the case where they use only two LEDs (880 nm and 940 nm) rather than four. While the choice of an optimal NIR wavelength for BGL monitoring is a subject of our continuing research, it is important to note that other glucose absorption peaks do exist at higher wavelengths [
11,
30,
31], but some constituents of blood (e.g., water) also have absorption peaks at this range and would therefore mask the absorption by the glucose molecules.
In this work, the ear canal was used as a measurement site, owing to its unique and distinguishing advantages over body-worn sensing locations. These include:
Stable body/skin temperature, which in turn means that in-ear PPG measurements do not suffer from the adverse effects of vasoconstriction, the phenomenon of the constriction of blood vessels due to local body temperature changes, which in turn affects the amplitude of the PPG signal and thus may bias the estimated BG values [
35];
Constant pressure/tension between the skin and the sensor yields stable and robust measurements (minimal day-to-day variation in the recordings);
The relative position between the head and the body remains mainly constant in most daily activities, which allows for truly continuous and stable long-term PPG measurements;
The in-ear sensor is generic and its viscoelastic nature means that it fits all ears;
Affordability and scalability, with only one off-the-shelf PPG sensor and only one wavelength needed for clinically acceptable accuracy.













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}