
An Explainable Spatial-Temporal Graphical Convolutional Network to Score Freezing of Gait in Parkinsonian Patients
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials Furthermore, Methods
2.1. Behavioral Testing
2.1.1. Study Participants
2.1.2. Levodopa Challenge Paradigm
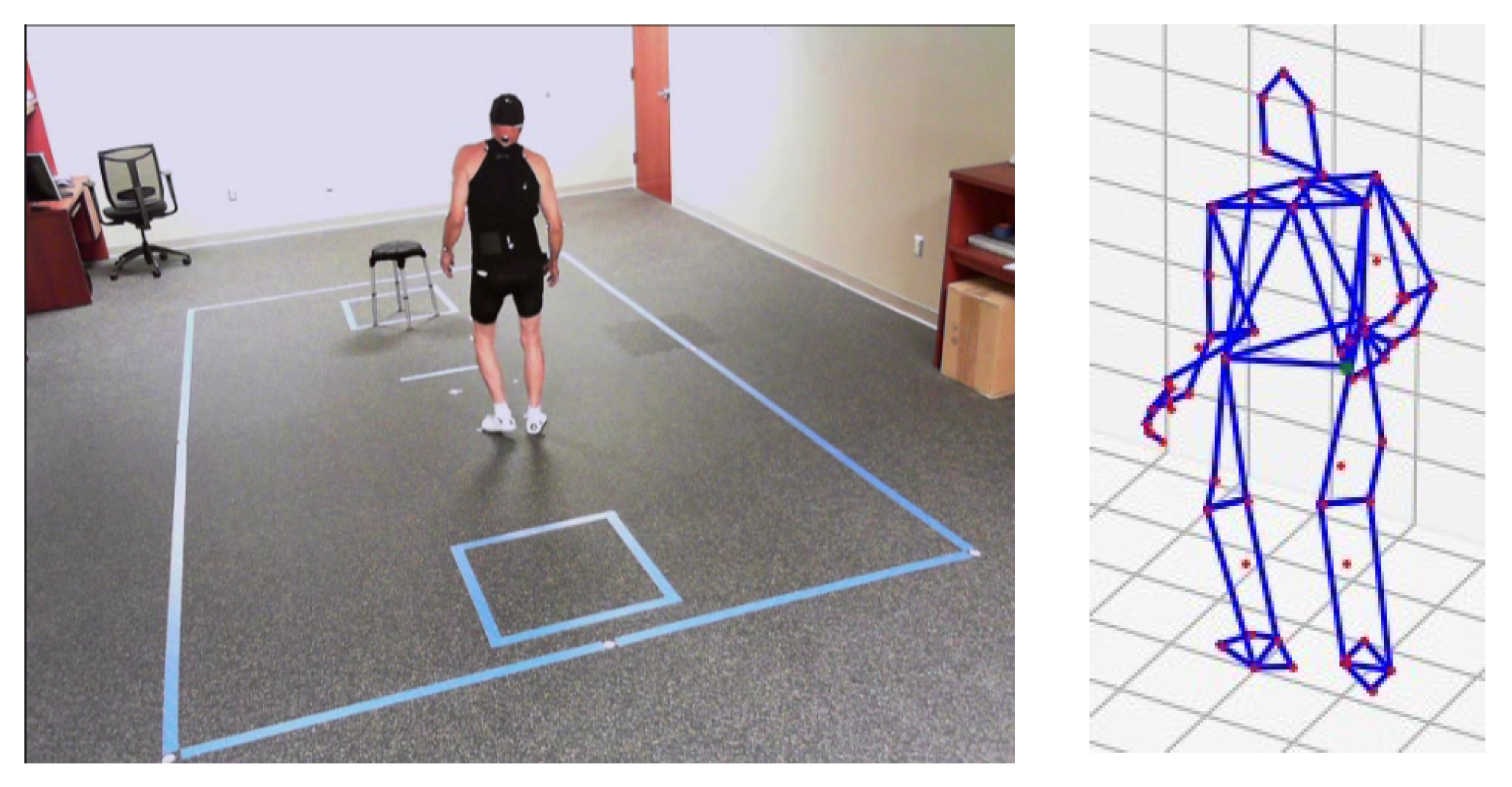
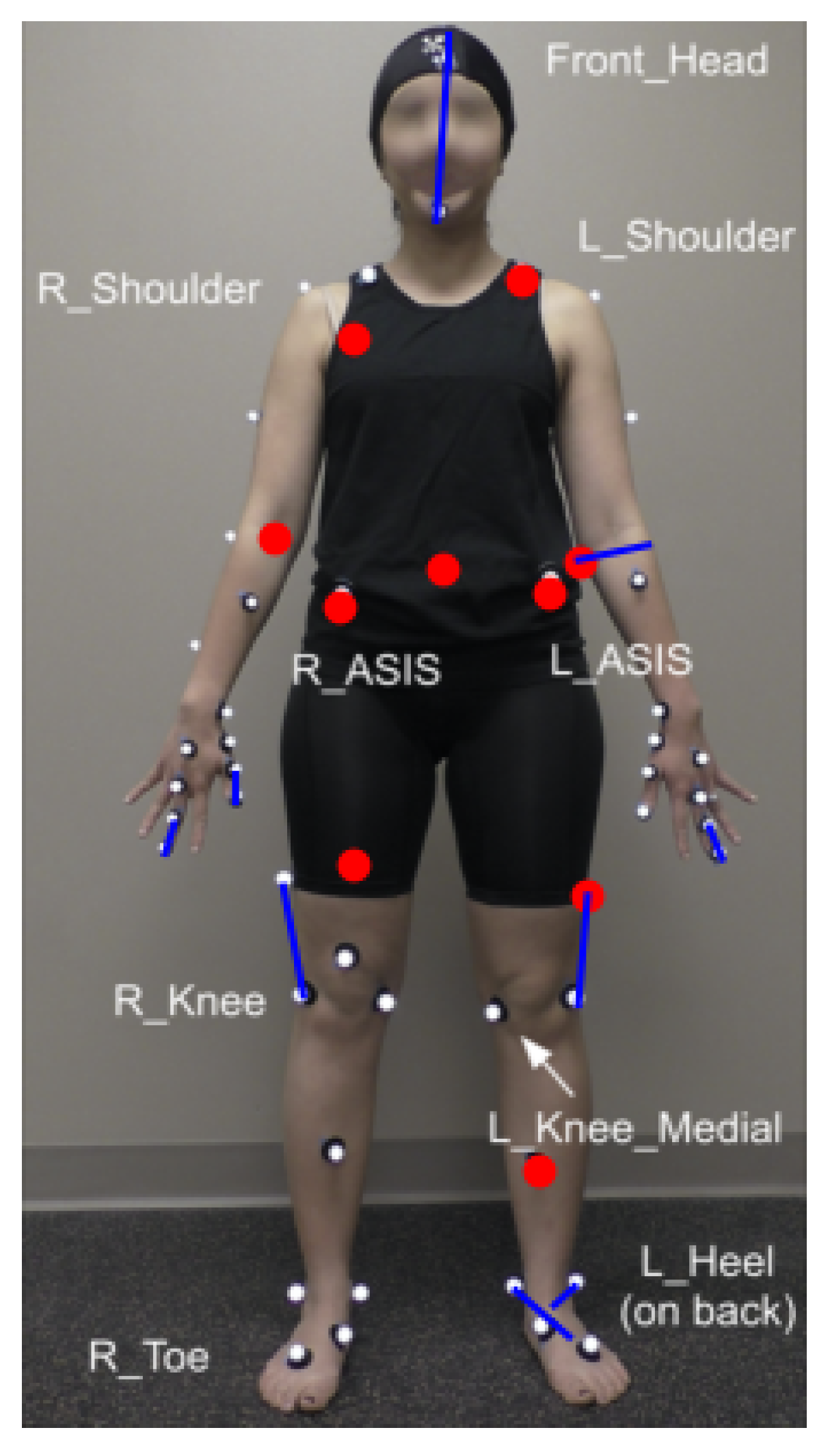
2.1.3. Motion Capture
2.2. Modeling
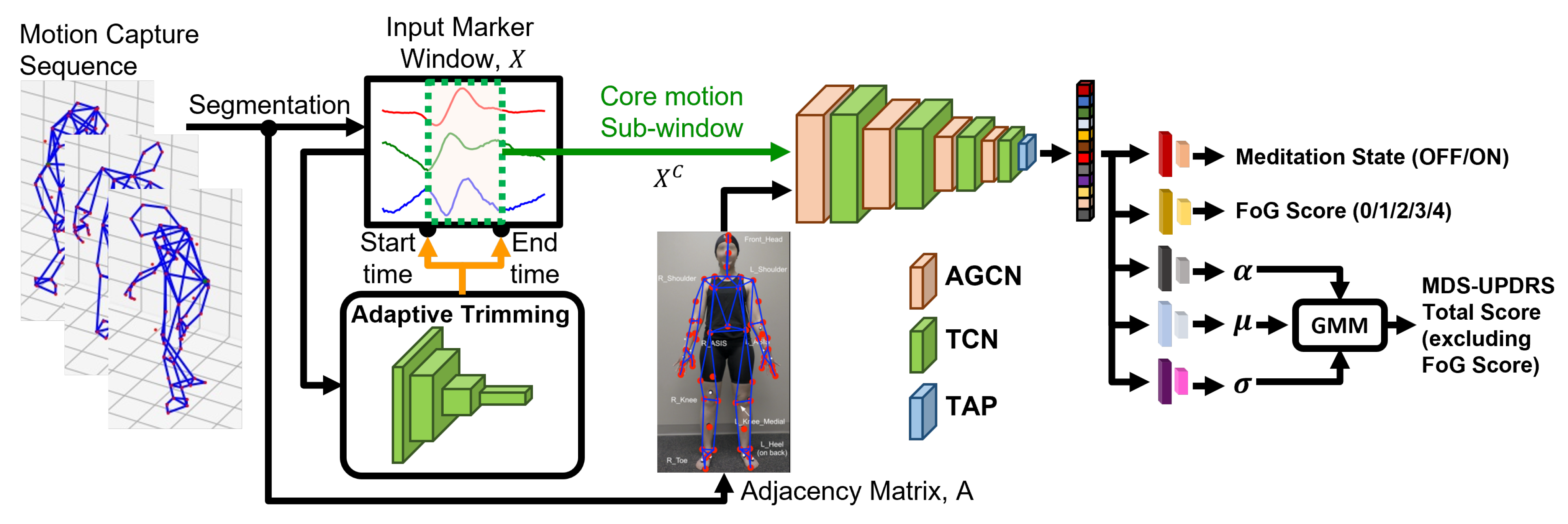
2.2.1. Model Overview
2.2.2. Trimming Core Motion Segment
2.2.3. Adaptive Graph Convolution
2.2.4. Multi-Task Prediction
3. Experiment Setting
3.1. Model Hyperparameter, Training and Evaluation
3.2. Performance Metrics
3.3. Comparison with Baseline Models
3.4. Comparison with Single-Task Prediction
3.5. Model Interpretability
3.6. Model Performance Furthermore, Potential Bias
4. Results
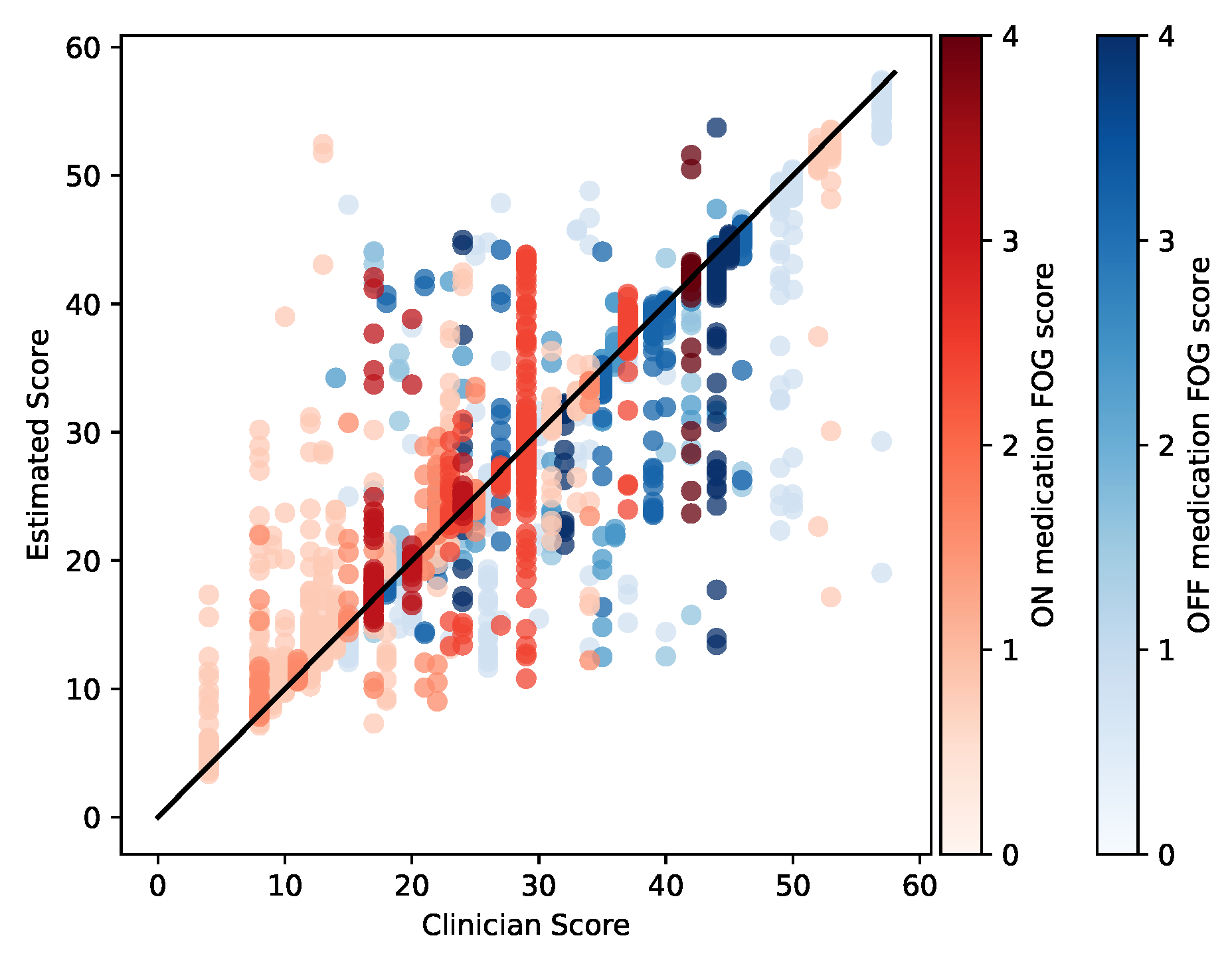
4.1. Overall Model Performance
4.2. Comparison to Baseline Models
4.3. Comparison to Single-Task Prediction
4.4. Model Interpretability
4.4.1. Most Relevant Joints and Limbs
4.4.2. Most Relevant Motion Segments
4.5. Classifier Performance Furthermore, Potential Bias
5. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Wilson Score Interval
References
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.; Sherer, T.; Okun, M.S.; Bloem, B.R. The emerging evidence of the Parkinson pandemic. J. Parkinson’s Dis. 2018, 8, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Lucas McKay, J.; Goldstein, F.C.; Sommerfeld, B.; Bernhard, D.; Perez Parra, S.; Factor, S.A. Freezing of Gait can persist after an acute levodopa challenge in Parkinson’s disease. NPJ Parkinson’s Dis. 2019, 5, 25. [Google Scholar] [CrossRef]
- Nonnekes, J.; Snijders, A.H.; Nutt, J.G.; Deuschl, G.; Giladi, N.; Bloem, B.R. Freezing of gait: A practical approach to management. Lancet Neurol. 2015, 14, 768–778. [Google Scholar] [CrossRef] [PubMed]
- Factor, S.A.; Jennings, D.L.; Molho, E.S.; Marek, K.L. The natural history of the syndrome of primary progressive freezing gait. Archiv. Neurol. 2002, 59, 1778–1783. [Google Scholar] [CrossRef] [PubMed]
- Haddad, Y.K.; Bergen, G.; Florence, C. Estimating the economic burden related to older adult falls by state. J. Public Health Manag. Pract. JPHMP 2019, 25, E17. [Google Scholar] [CrossRef] [PubMed]
- Florence, C.S.; Bergen, G.; Atherly, A.; Burns, E.; Stevens, J.; Drake, C. Medical costs of fatal and nonfatal falls in older adults. J. Am. Geriatr. Soc. 2018, 66, 693–698. [Google Scholar] [CrossRef]
- Pelicioni, P.H.; Menant, J.C.; Latt, M.D.; Lord, S.R. Falls in Parkinson’s disease subtypes: Risk factors, locations and circumstances. Int. J. Environ. Res. Public Health 2019, 16, 2216. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Hulzinga, F.; Nieuwboer, A.; Dijkstra, B.W.; Mancini, M.; Strouwen, C.; Bloem, B.R.; Ginis, P. The New Freezing of Gait Questionnaire: Unsuitable as an outcome in clinical trials? Mov. Disord. Clin. Pract. 2020, 7, 199–205. [Google Scholar] [CrossRef]
- Hatcher-Martin, J.; McKay, J.; Sommerfeld, B.; Howell, J.; Goldstein, F.; Hu, W.; Factor, S. Cerebrospinal fluid Aβ42 and fractalkine are associated with Parkinson’s disease with freezing of gait. medRxiv 2020, 1–12. [Google Scholar] [CrossRef]
- Forsaa, E.; Larsen, J.; Wentzel-Larsen, T.; Alves, G. A 12-year population-based study of freezing of gait in Parkinson’s disease. Park. Relat. Disord. 2015, 21, 254–258. [Google Scholar] [CrossRef]
- Zhang, Y.; Yan, W.; Yao, Y.; Bint Ahmed, J.; Tan, Y.; Gu, D. Prediction of freezing of gait in patients with Parkinson’s disease by identifying impaired gait patterns. IEEE Trans. Neural Syst. Rehab. Eng. 2020, 28, 591–600. [Google Scholar] [CrossRef]
- Yan, Y.; Liu, Y.; Li, C.; Wang, J.; Ma, L.; Xiong, J.; Zhao, X.; Wang, L. Topological Descriptors of Gait Nonlinear Dynamics toward Freezing-of-Gait Episodes Recognition in Parkinson’s Disease. IEEE Sens. J. 2022, 22, 4294–4304. [Google Scholar] [CrossRef]
- Silva de Lima, A.; Evers, L.J.; Hahn, T.; Bataille, L.; Hamilton, J.; Little, M.; Okuma, Y.; Bloem, B.; Faber, M. Freezing of gait and fall detection in Parkinson’s disease using wearable sensors: A systematic review. J. Neurol. 2017, 264, 1642–1654. [Google Scholar]
- Yungher, D.; Morris, T.; Dilda, V.; Shine, J.; Naismith, S.; Lewis, S.J.; Moore, S.T. Temporal characteristics of high-frequency lower-limb oscillation during freezing of gait in Parkinson’s disease. Parkinson’s Dis. 2014, 2014, 606427. [Google Scholar] [CrossRef]
- Rodríguez-Martín, D.; Samà, A.; Pérez-López, C.; Català, A.; Moreno Arostegui, J.M.; Cabestany, J.; Bayés, À.; Alcaine, S.; Mestre, B.; Prats, A.; et al. Home detection of freezing of gait using support vector machines through a single waist-worn triaxial accelerometer. PLoS ONE 2017, 12, e0171764. [Google Scholar] [CrossRef]
- Tahafchi, P.; Molina, R.; Roper, J.A.; Sowalsky, K.; Hass, C.J.; Gunduz, A.; Okun, M.S.; Judy, J.W. Freezing-of-Gait detection using temporal, spatial, and physiological features with a support-vector-machine classifier. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Republic of Korea, 11–15 July 2017; pp. 2867–2870. [Google Scholar]
- Reches, T.; Dagan, M.; Herman, T.; Gazit, E.; Gouskova, N.A.; Giladi, N.; Manor, B.; Hausdorff, J.M. Using wearable sensors and machine learning to automatically detect freezing of gait during a FOG-provoking test. Sensors 2020, 20, 4474. [Google Scholar]
- Ferrari, A.; Ginis, P.; Hardegger, M.; Casamassima, F.; Rocchi, L.; Chiari, L. A mobile Kalman-filter based solution for the real-time estimation of spatio-temporal gait parameters. IEEE Trans. Neural Syst. Rehab. Eng. 2015, 24, 764–773. [Google Scholar] [CrossRef]
- Diep, C.; O’Day, J.; Kehnemouyi, Y.; Burnett, G.; Bronte-Stewart, H. Gait Parameters Measured from Wearable Sensors Reliably Detect Freezing of Gait in a Stepping in Place Task. Sensors 2021, 21, 2661. [Google Scholar] [CrossRef]
- Mancini, M.; Shah, V.V.; Stuart, S.; Curtze, C.; Horak, F.B.; Safarpour, D.; Nutt, J.G. Measuring freezing of gait during daily-life: An open-source, wearable sensors approach. J. NeuroEng. Rehab. 2021, 18, 1. [Google Scholar] [CrossRef]
- Hatcher-Martin, J.M.; McKay, J.L.; Pybus, A.F.; Sommerfeld, B.; Howell, J.C.; Goldstein, F.C.; Wood, L.; Hu, W.T.; Factor, S.A. Cerebrospinal fluid biomarkers in Parkinson’s disease with freezing of gait: An exploratory analysis. NPJ Parkinsons Dis. 2021, 7, 105. [Google Scholar] [CrossRef]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatr. 1992, 55, 181–184. [Google Scholar] [CrossRef]
- Nocera, J.R.; Stegemöller, E.L.; Malaty, I.A.; Okun, M.S.; Marsiske, M.; Hass, C.J.; National Parkinson Foundation Quality Improvement Initiative Investigators. Using the Timed Up & Go test in a clinical setting to predict falling in Parkinson’s disease. Archiv. Phys. Med. Rehab. 2013, 94, 1300–1305. [Google Scholar]
- Shumway-Cook, A.; Baldwin, M.; Polissar, N.L.; Gruber, W. Predicting the probability for falls in community-dwelling older adults. Phys. Ther. 1997, 77, 812–819. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.; Wootten, M. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Yu, Y.; Samali, B.; Rashidi, M.; Mohammadi, M.; Nguyen, T.N.; Zhang, G. Vision-based concrete crack detection using a hybrid framework considering noise effect. J. Build. Eng. 2022, 61, 105246. [Google Scholar] [CrossRef]
- Soffer, S.; Ben-Cohen, A.; Shimon, O.; Amitai, M.M.; Greenspan, H.; Klang, E. Convolutional neural networks for radiologic images: A radiologist’s guide. Radiology 2019, 290, 590–606. [Google Scholar] [CrossRef]
- Ordóñez, F.J.; Roggen, D. Deep convolutional and lstm recurrent neural networks for multimodal wearable activity recognition. Sensors 2016, 16, 115. [Google Scholar] [CrossRef]
- Du, Y.; Wang, W.; Wang, L. Hierarchical recurrent neural network for skeleton based action recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1110–1118. [Google Scholar]
- Zhang, Y.; Tiňo, P.; Leonardis, A.; Tang, K. A survey on neural network interpretability. IEEE Trans. Emerg. Top. Comput. Intell. 2021, 5, 726–742. [Google Scholar] [CrossRef]
- Murahari, V.S.; Plötz, T. On attention models for human activity recognition. In Proceedings of the 2018 ACM International Symposium on Wearable Computers, Singapore, 8–12 October 2018; pp. 100–103. [Google Scholar]
- Shi, L.; Zhang, Y.; Cheng, J.; Lu, H. Two-stream adaptive graph convolutional networks for skeleton-based action recognition. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, Long Beach, CA, USA, 15–20 June 2019; pp. 12026–12035. [Google Scholar]
- Kwon, H.; Abowd, G.; Plötz, T. Complex Deep Neural Networks from Large Scale Virtual IMU Data for Effective Human Activity Recognition Using Wearables. Sensors 2021, 21, 8337. [Google Scholar] [CrossRef]
- Hammerla, N.Y.; Halloran, S.; Plötz, T. Deep, Convolutional, and Recurrent Models for Human Activity Recognition Using Wearables. In Proceedings of the IJCAI, New York, NY, USA, 9–15 July 2016. [Google Scholar]
- Bachlin, M.; Plotnik, M.; Roggen, D.; Maidan, I.; Hausdorff, J.M.; Giladi, N.; Troster, G. Wearable assistant for Parkinson’s disease patients with the freezing of gait symptom. IEEE Trans. Inf. Technol. Biomed. 2009, 14, 436–446. [Google Scholar] [CrossRef]
- Jaderberg, M.; Simonyan, K.; Zisserman, A.; Kavukcuoglu, K. Spatial transformer networks. Adv. Neural Inf. Process. Syst. 2015, 28. [Google Scholar] [CrossRef]
- Wang, X.; Girshick, R.; Gupta, A.; He, K. Non-local neural networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 7794–7803. [Google Scholar]
- Toth, C.; Rajput, M.; Rajput, A.H. Anomalies of asymmetry of clinical signs in parkinsonism. Mov. Disord. Off. J. Mov. Disord. Soc. 2004, 19, 151–157. [Google Scholar] [CrossRef]
- Djaldetti, R.; Ziv, I.; Melamed, E. The mystery of motor asymmetry in Parkinson’s disease. Lancet Neurol. 2006, 5, 796–802. [Google Scholar] [CrossRef]
- Lin, M.; Chen, Q.; Yan, S. Network in network. arXiv 2013, arXiv:1312.4400. [Google Scholar]
- Bishop, C.M. Mixture Density Networks; Aston University: Birmingham, UK, 1994. [Google Scholar]
- Nair, V.; Hinton, G.E. Rectified linear units improve restricted boltzmann machines. In Proceedings of the Icml, Haifa, Israel, 21–24 June 2010. [Google Scholar]
- Hammerla, N.Y.; Plötz, T. Let us (not) stick together: Pairwise similarity biases cross-validation in activity recognition. In Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Umeda, Osaka, Japan, 7–11 September 2015; pp. 1041–1051. [Google Scholar]
- Wilson, E.B. Probable inference, the law of succession, and statistical inference. J. Am. Stat. Assoc. 1927, 22, 209–212. [Google Scholar] [CrossRef]
- Naghavi, N.; Wade, E. Prediction of freezing of gait in Parkinson’s disease using statistical inference and lower–limb acceleration data. IEEE Trans. Neural Syst. Rehab. Eng. 2019, 27, 947–955. [Google Scholar] [CrossRef]
- Palmerini, L.; Rocchi, L.; Mazilu, S.; Gazit, E.; Hausdorff, J.M.; Chiari, L. Identification of characteristic motor patterns preceding freezing of gait in Parkinson’s disease using wearable sensors. Front. Neurol. 2017, 8, 394. [Google Scholar] [CrossRef]
- Moore, S.T.; MacDougall, H.G.; Ondo, W.G. Ambulatory monitoring of freezing of gait in Parkinson’s disease. J. Neurosci. Methods 2008, 167, 340–348. [Google Scholar] [CrossRef]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol.-Heart Circul. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed]
- Baby, M.S.; Saji, A.; Kumar, C.S. Parkinsons disease classification using wavelet transform based feature extraction of gait data. In Proceedings of the 2017 International Conference on Circuit, Power and Computing Technologies (ICCPCT), Kollam, India, 20–21 April 2017; pp. 1–6. [Google Scholar]
- Du, Y.; Fu, Y.; Wang, L. Skeleton based action recognition with convolutional neural network. In Proceedings of the 2015 3rd IAPR Asian Conference on Pattern Recognition (ACPR), Kuala Lumpur, Malaysia, 3–6 November 2015; pp. 579–583. [Google Scholar]
- Yan, S.; Xiong, Y.; Lin, D. Spatial temporal graph convolutional networks for skeleton-based action recognition. In Proceedings of the Thirty-Second AAAI Conference on Artificial Intelligence, New Orleans, LA, USA, 2–7 February 2018. [Google Scholar]
- Horváth, K.; Aschermann, Z.; Ács, P.; Deli, G.; Janszky, J.; Komoly, S.; Balázs, É.; Takács, K.; Karádi, K.; Kovács, N. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Park. Relat. Disord. 2015, 21, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Sama, A.; Martin, M.; Rodriguez-Martin, D.; Perez-Lopez, C.; Arostegui, J.M.M.; Cabestany, J.; Català, A.; Alcaine, S.; Mestre, B.; et al. Deep learning for freezing of gait detection in Parkinson’s disease patients in their homes using a waist-worn inertial measurement unit. Knowl.-Based Syst. 2018, 139, 119–131. [Google Scholar] [CrossRef]
- Khobkhun, F.; Hollands, M.; Tretriluxana, J.; Srivanitchapoom, P.; Richards, J.; Ajjimaporn, A. Benefits of task-specific movement program on en bloc turning in Parkinson’s disease: A randomized controlled trial. Physiother. Res. Int. 2022, 27, e1963. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.; Earhart, G.M. Effects of medication on turning deficits in individuals with Parkinson’s disease. J. Neurol. Phys. Ther. 2010, 34, 11–16. [Google Scholar] [CrossRef]
- Heremans, E.; Nackaerts, E.; Vervoort, G.; Vercruysse, S.; Broeder, S.; Strouwen, C.; Swinnen, S.P.; Nieuwboer, A. Amplitude manipulation evokes upper limb freezing during handwriting in patients with Parkinson’s disease with freezing of gait. PLoS ONE 2015, 10, e0142874. [Google Scholar] [CrossRef]
- Imai, H. Festination and freezing. Rinsho Shinkeigaku = Clin. Neurol. 1993, 33, 1307–1309. [Google Scholar]
- Dobson, F.; Morris, M.E.; Baker, R.; Graham, H.K. Gait classification in children with cerebral palsy: A systematic review. Gait Post. 2007, 25, 140–152. [Google Scholar] [CrossRef]
- Nunes, A.S.; Kozhemiako, N.; Stephen, C.D.; Schmahmann, J.D.; Khan, S.; Gupta, A.S. Automatic Classification and Severity Estimation of Ataxia From Finger Tapping Videos. Front. Neurol. 2022, 12, 2587. [Google Scholar] [CrossRef]
- Cheng, F.; Duan, Y.; Jiang, H.; Zeng, Y.; Chen, X.; Qin, L.; Zhao, L.; Yi, F.; Tang, Y.; Liu, C. Identifying and distinguishing of essential tremor and Parkinson’s disease with grouped stability analysis based on searchlight-based MVPA. BioMedical Eng. OnLine 2022, 21, 81. [Google Scholar] [CrossRef]
- GBD 2016 Parkinson’s Disease Collaborators. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [PubMed]
- Wallis, S. Binomial confidence intervals and contingency tests: Mathematical fundamentals and the evaluation of alternative methods. J. Quant. Linguist. 2013, 20, 178–208. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PD-FOG | PD-NoFOG | PP-FOG | |
|---|---|---|---|
| N | 35 | 17 | 5 |
| Age, y | |||
| Sex, M/F | 30/5 | 11/6 | 2/3 |
| Disease duration, y | |||
| LED, mg | |||
| MDS-UPDRS-III (OFF) | |||
| MDS-UPDRS-III (ON) | |||
| NFOG-Q |
| Medication | FOG Score | ||||
|---|---|---|---|---|---|
| State | 0 | 1 | 2 | 3 | 4 |
| OFF | 21 | 15 | 9 | 8 | 7 |
| ON | 38 | 11 | 7 | 3 | 1 |
| Medication State | FOG Score | MDS-UPDRS-III | Inference Time | |
|---|---|---|---|---|
| Model | (F1) | (F1) | (RMSE) | (Seconds) |
| SVM-L | - | |||
| RF-L | - | |||
| SVM-LR | - | |||
| RF-LR | - | |||
| TCN [52] | * | * | * | 0.0055 |
| GCN [53] | * | * | * | 0.0433 |
| AGCN [34] | * | * | * | 0.0435 |
| AT+AGCN | * | 0.0469 | ||
| AT+AGCN+GMM | * | 0.0471 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, H.; Clifford, G.D.; Genias, I.; Bernhard, D.; Esper, C.D.; Factor, S.A.; McKay, J.L. An Explainable Spatial-Temporal Graphical Convolutional Network to Score Freezing of Gait in Parkinsonian Patients. Sensors 2023, 23, 1766. https://doi.org/10.3390/s23041766
Kwon H, Clifford GD, Genias I, Bernhard D, Esper CD, Factor SA, McKay JL. An Explainable Spatial-Temporal Graphical Convolutional Network to Score Freezing of Gait in Parkinsonian Patients. Sensors. 2023; 23(4):1766. https://doi.org/10.3390/s23041766
Chicago/Turabian StyleKwon, Hyeokhyen, Gari D. Clifford, Imari Genias, Doug Bernhard, Christine D. Esper, Stewart A. Factor, and J. Lucas McKay. 2023. "An Explainable Spatial-Temporal Graphical Convolutional Network to Score Freezing of Gait in Parkinsonian Patients" Sensors 23, no. 4: 1766. https://doi.org/10.3390/s23041766