
Gait Variability to Phenotype Common Orthopedic Gait Impairments Using Wearable Sensors
by
 , , , , and
, , , , and
Junichi Kushioka
1,†,
Ruopeng Sun
1,2,*,†,
Wei Zhang
3,
Amir Muaremi
4,
Heike Leutheuser
5 ,
,
Charles A. Odonkor
6 and
and
Matthew Smuck
1,2 1
Department of Orthopaedic Surgery, Stanford University, Stanford, CA 94305, USA
2
Division of Physical Medicine and Rehabilitation, Stanford University, Stanford, CA 94305, USA
3
Laboratory of Movement Analysis and Measurement, Ecole Polytechnique Fédérale de Lausanne (EPFL), 1015 Lausanne, Switzerland
4
Novartis Institutes for BioMedical Research, 4056 Basel, Switzerland
5
Machine Learning and Data Analytics Lab (MaD Lab), Department Artificial Intelligence in Biomedical Engineering (AIBE), Friedrich-Alexander-Universität Erlangen-Nürnberg (FAU), 91052 Erlangen, Germany
6
Department of Orthopedics and Rehabilitation, Division of Physiatry, Yale School of Medicine, New Haven, CT 06510, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Sensors 2022, 22(23), 9301; https://doi.org/10.3390/s22239301
Submission received: 4 November 2022
/
Revised: 25 November 2022
/
Accepted: 28 November 2022
/
Published: 29 November 2022
(This article belongs to the Special Issue Advances in Sensor Technologies for Wearable Applications)
Abstract
:Mobility impairments are a common symptom of age-related degenerative diseases. Gait features can discriminate those with mobility disorders from healthy individuals, yet phenotyping specific pathologies remains challenging. This study aims to identify if gait parameters derived from two foot-mounted inertial measurement units (IMU) during the 6 min walk test (6MWT) can phenotype mobility impairment from different pathologies (Lumbar spinal stenosis (LSS)—neurogenic diseases, and knee osteoarthritis (KOA)—structural joint disease). Bilateral foot-mounted IMU data during the 6MWT were collected from patients with LSS and KOA and matched healthy controls (N = 30, 10 for each group). Eleven gait parameters representing four domains (pace, rhythm, asymmetry, variability) were derived for each minute of the 6MWT. In the entire 6MWT, gait parameters in all four domains distinguished between controls and both disease groups; however, the disease groups demonstrated no statistical differences, with a trend toward higher stride length variability in the LSS group (p = 0.057). Additional minute-by-minute comparisons identified stride length variability as a statistically significant marker between disease groups during the middle portion of 6WMT (3rd min: p ≤ 0.05; 4th min: p = 0.06). These findings demonstrate that gait variability measures are a potential biomarker to phenotype mobility impairment from different pathologies. Increased gait variability indicates loss of gait rhythmicity, a common feature in neurologic impairment of locomotor control, thus reflecting the underlying mechanism for the gait impairment in LSS. Findings from this work also identify the middle portion of the 6MWT as a potential window to detect subtle gait differences between individuals with different origins of gait impairment.
1. Introduction
Mobility limitations are increasing with the aging of modern society [1,2]. Among those suffering from mobility impairment, lumbar spinal stenosis (LSS) and knee osteoarthritis (KOA) are two of the most common causes worldwide [3,4,5], creating a substantial and increasing burden on society and the economy [6,7,8]. LSS has a neurogenic disease mechanism characterized by claudication, described as pain and/or numbness in the lower back and extremities that worsens with walking distance [9]. Alternatively, KOA has a structural joint disease mechanism characterized by knee pain from the initiation of walking [10], often associated with a “gelling phenomenon” or a feeling of joint stiffness that gradually mitigates with continuous movement [11]. Since the pathophysiology and symptomatology of LSS differ from KOA, the manifestations of their respective gait disturbances may also differ. Our previous analysis of walking tests, including the 6 min walk test (6MWT), identified significant differences between these two disorders and the healthy controls [12]. However, a challenge remains to further phenotype and distinguish between these two common causes of mobility impairment using gait measures.
Numerous parameters are used to characterize gait disturbances [13,14,15]. These gait parameters can be classified into four domains: rhythm, pace, asymmetry, and variability [16,17]. The rhythm domain represents measures of absolute timing. The pace domain relates to walking speed and length measures in the sagittal plane. The asymmetry domain links to differences between the right and left lower limb parameters, and the variability domain reflects fluctuations in spatiotemporal characteristics between steps. These gait parameters are often reported as mean values during the entire period of the test, however, recent work showed that the temporal change in gait performance over a period of time may reveal additional subtle gait alterations that may be fatigue-induced and/or disease-specific [18,19].
Traditionally, gait analysis has been conducted in well-equipped labs using 3D motion capture techniques, requiring the use of costly equipment and specialized facilities. Newer technologies (including inertial measurement units (IMU), smartphones, low-cost video/depth cameras, pressure sensors, ambient sensors, etc.), provide alternatives that can efficiently capture and analyze movement data in various settings [20]. Among these technologies, wearable IMUs are most commonly used as the most portable and flexible option to measure mobility [21], allowing physicians, physical therapists, and researchers to analyze gait in research laboratories, clinics, and in a patient’s home or community. IMU sensors contain small 3D accelerometers (linear acceleration), gyroscopes (angular velocity), and/or magnetometers (magnetic field) that can be used collectively to quantify movement through various time- and frequency-domain parameters [20]. By securely attaching wearable IMU sensors to various body segments, different kinematic and biomechanical parameters can be obtained with similar validity and reliability to conventional lab-based systems [22,23]. Gait features derived from wearable sensors have demonstrated potential clinical utility in neurological diseases by distinguishing disease populations from healthy controls and stratifying disease severity [16,18]. However, such clinical utility has yet to be demonstrated in orthopedic research.
This study aims to analyze data from foot-mounted IMUs worn by patients with LSS and KOA during the 6MWT to investigate gait characteristics in each of the four gait domains (rhythm, pace, asymmetry, and variability). Specifically, our primary goal is to extract gait features by each minute of the walking test to compare LSS and KOA and determine whether time series data reveals phenotypic differences between the two disease groups.
2. Materials and Methods
2.1. Participants
A total of 30 participants were enrolled in the study, with 10 in each of the 3 groups: LSS, KOA, and matched healthy controls (HC). The full study inclusion/exclusion criteria are detailed in a previous paper summarizing the overall results from multiple walking tests [12]. The study was HIPAA compliant and approved by the ethical committee for Human Subjects Research at Stanford University. Each participant provided written informed consent and completed the 36-Item Short-Form health survey (SF-36) [24].
2.2. Gait Analysis
Each participant underwent a series of gait assessments, including the 40 m fast-paced walk test [25], the self-paced walk test [26], and the 6MWT [25]. In this study, we focus on the 6MWT for its ability to assess endurance and change in gait parameters over time [25,27,28]. A minute-by-minute analysis of the 6MWT provides a unique opportunity to evaluate dynamic changes that occur during walking and investigate time series differences between the two disease groups [18,19].
During the entire 6MWT, participants wore two Shimmer 3 IMU sensors (Shimmer Sensing, Dublin, Ireland) on the dorsal surface of both feet. We used previously validated algorithms to extract spatial–temporal gait parameters that reflect steady-state walking (after excluding all turning episodes) [21]. For details on gait parameter extraction, please see Supplementary File S6. Eleven gait parameters were extracted representing the four different gait domains as described in previous research [16,17], including the rhythm domain (cadence, double support duration, and swing phase duration), the pace domain (stride length and speed), the asymmetry domain (asymmetry index for stride length and swing duration), and the variability domain (coefficient of variation for double support duration, swing duration, stride length, and gait cycle duration). Detailed descriptions of the extracted parameters are listed in Table 1. Among the extracted parameters, the asymmetry index was calculated using the difference ratio of the parameters derived from each limb [21]. A greater asymmetry index indicates a higher gait asymmetry [21]. In contrast, the coefficient of variation (CV) is a measure of variability, which refers to the ratio between the standard deviation and the mean of each parameter, expressed as a percentage [29]. A higher gait variability (more outstanding CV) indicates a worsening gait consistency [30]. To avoid redundancy, we did not present parameters that demonstrated similar results within the same domain. This approach for gait analysis was used previously in multiple studies [18,30,31,32,33,34]. The extracted gait parameters were further divided into 1 min segments to analyze minute-by-minute changes over the entire 6MWT.
All participants identified the side with more/most pain. However, since our preliminary analysis revealed no significant differences between limbs for all extract gait parameters, we reported averaged data for both limbs in this work. For data comparisons between limbs, please refer to Supplementary Files S3–S5.
2.3. Statistical Methods
All derived gait parameters were checked for normal distribution using the Shapiro–Wilk test. Gait variables that were not normally distributed (variability and asymmetry domain measures) were log-transformed. Differences in parameters among the three groups from the entire 6MWT were analyzed by a one-way ANOVA test followed by Tukey’s test. Next, differences in parameters among three groups in each minute of the 6MWT were analyzed by two-way ANOVA with group and minute as factors. In addition, differences in parameters between the LSS and KOA groups were analyzed for each minute of the 6MWT using the Student T-test. A p-value < 0.05 was defined as statistically significant. All sensor data processing and gait feature extractions were performed using customized MATLAB (MathWorks, Inc., Natick, MA, USA) programs, and data visualization and statistical analyses were performed using customized Python programs.
3. Results
3.1. Participants’ Characteristics
Participants’ demographic characteristics are presented in Supplementary File S1. The average age of all study participants was 65 years, with a range of 46–86 and an average BMI of 30.3. Additional details on the participants’ demographic and clinical characteristics were provided in the previous summary paper [12].
3.2. Analysis of the Entire 6MWT
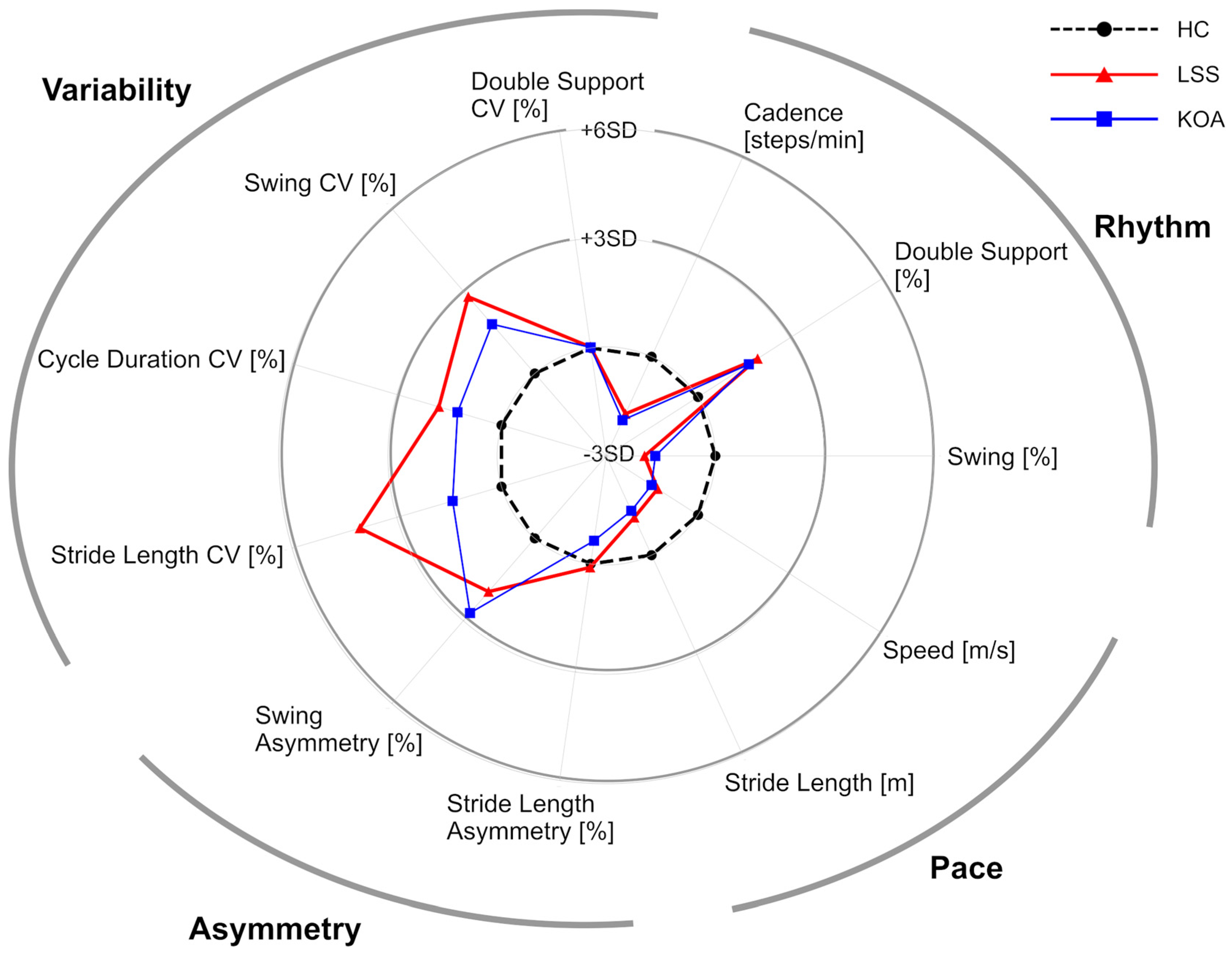
Figure 1 and Table 2 summarize the gait parameters extracted from the analysis of the entire 6MWT. In the rhythm domain, LSS and KOA groups showed a significantly lower cadence and swing ratio and a significantly higher double support ratio than the HC group (HC-LSS: p < 0.05, HC-KOA: p < 0.05), indicating decreased gait rhythm. In the pace domain, LSS and KOA showed significantly lower speed than HC (HC-LSS: p < 0.05, HC-KOA: p < 0.05). While both disease groups showed lower stride length, the difference between LSS and HC did not reach statistical significance (HC-LSS: p = 0.057, HC-KOA: p < 0.05). In the asymmetry domain, all three groups showed similar stride length asymmetry, while both LSS and KOA showed significantly higher swing asymmetry relative to HC (HC-LSS: p < 0.05, HC-KOA: p < 0.05). Finally, in the variability domain, both LSS and KOA showed significantly higher CV of cycle duration, and swing (HC-LSS: p < 0.05, HC-KOA: p < 0.05), indicating an increase in gait variance compared to HC. LSS showed a significantly higher stride length CV than HC (p < 0.05), while KOA’s stride length CV was similar to HC (p = 0.47). Although there were no significant differences between the LSS group and the KOA group for any parameter, stride length variability demonstrated a strong trend toward a difference between the two disease groups (stride length CV; LSS 4.7 ± 0.8, KOA 4.0 ± 0.8, p = 0.057) with greater variability in the LSS group.
3.3. Minute-by-Minute Analysis of the 6MWT
Next, we performed a minute-by-minute analysis to further assess changes over time during the 6MWT. Firstly, we conducted a two-way ANOVA (three groups by 6 min) and, as expected, observed that HC had significantly different gait parameters (lower double support ratio, swing asymmetry, stride length CV, cycle duration CV, swing CV, and higher cadence, swing ratio, speed, stride length) compared to the disease groups for every minute of the 6MWT (p < 0.05). Only stride length asymmetry and double support CV failed to show a difference between HC and the disease groups. On a minute-by-minute basis, we observed no significant temporal change within any group.
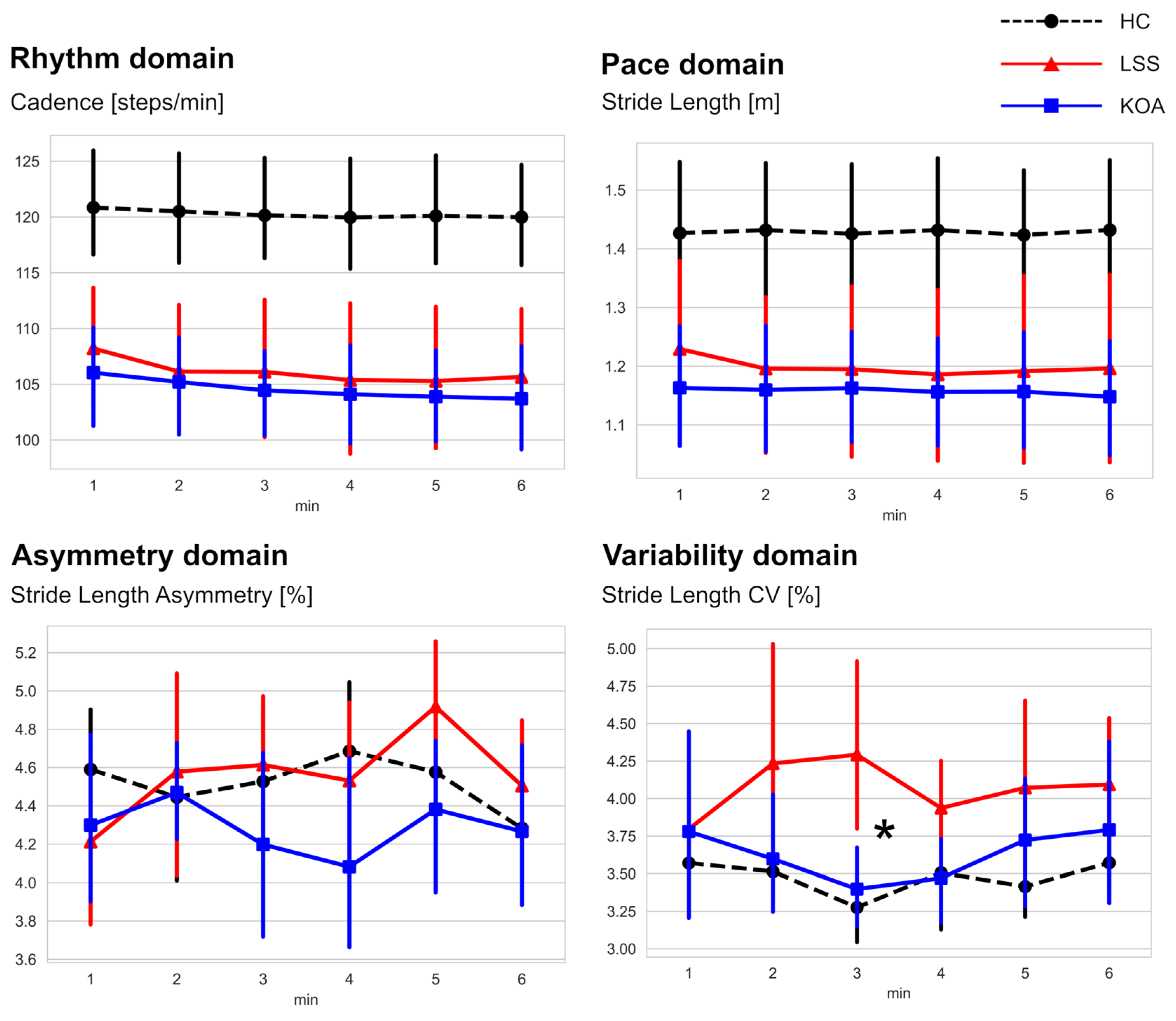
We performed additional comparisons to evaluate the two disease groups further. Representative graphs for each domain are shown in Figure 2, and other graphs are shown in Supplementary File S2. Focusing solely on the observed difference between the LSS and KOA groups, a significant between-group difference appeared in the middle portion of the 6MWT for stride length variability. Specifically, during the 3rd minute of the 6MWT, the stride length CV of the LSS group was significantly higher than that of the KOA group (4.29 ± 0.94 in the LSS group, 3.40 ± 0.45 in the KOA group, p < 0.05). In addition, the LSS group showed a trend toward higher stride length variability during the 4th minute of the 6MWT (3.94 ± 0.54 in the LSS group, 3.47 ± 0.50 in the KOA group, p = 0.06). This increased stride length variability in LSS indicates a worsening of gait rhythmicity.
4. Discussion
In this study, we derive gait parameters from foot-mounted IMU sensors worn during the 6MWT by people with LSS and KOA, compared to each other and HC for the entire 6MWT and during each minute. We characterize the findings based on four gait domains (rhythm, pace, asymmetry, and variability). When the entire 6MWT is considered, multiple gait parameters in all four domains distinguish between HC and LSS or KOA, while no statistical differences are observed between the two disease groups. Yet, the LSS group did show a trend toward higher stride length variability compared to the KOA group (p = 0.057). Further minute-by-minute analysis comparing gait characteristics between LSS and KOA revealed that LSS individuals displayed significantly greater stride length variability than KOA individuals during the middle portion of the walk test.
Stride length variability refers to the ratio between the standard deviation and the mean of the stride length, expressed as a percentage. Gait variability, stride-to-stride fluctuations during walking, is a potential biomarker for gait impairment and loss of gait rhythmicity [29,35,36]. An increase in variability indicates worsening gait consistency. Previous research demonstrates that maintaining gait consistency is a complex process dependent on diverse neurological structures from the cerebral cortex to the peripheral nerves and muscles [37]. Therefore, damage to any neuromuscular structure that governs locomotor control can influence gait variability [37]. Accordingly, many studies report altered gait variability (including increased CV of stride length) in various neurological disorders such as Alzheimer’s disease, amyotrophic lateral sclerosis, cerebellar ataxia, Huntington’s disease, multiple sclerosis, and Parkinson’s disease [38,39,40,41,42,43].
Similarly, LSS has a neurologic disease mechanism caused by the positional compression of the cauda equina or nerve roots, resulting in intermittent motor and/or sensory nerve dysfunction [9]. In agreement with our study findings, recent research [44] using a self-paced walking test with a chest-mounted IMU sensor also observed increased step length variability in LSS patients compared to the healthy controls. Previous research also suggested that gait irregularity can be attributed to neurogenic claudication and radicular pain, common clinical symptoms in LSS patients [44,45]. Previous research theorized that radicular pain, with its unpredictable ectopic discharge, may cause irregular walking and contribute to high gait variability [45]. Conversely, gait impairment in KOA originates from structural joint deformation that does not involve motor control mechanisms. This study’s minute-by-minute analysis for 6MWT revealed a significant difference between the LSS and KOA groups in the middle portion of the 6MWT for stride length variability. Therefore, findings from this work suggest that the stride length variability may be a potential sensitive mobility biomarker to distinguish between gait impairment from a neurological origin (LSS) and gait impairment from joint structural disease (KOA).
Findings from this work also highlighted that the middle portion of the 6MWT may be a potential window to detect subtle gait differences between individuals with different origins of gait impairment. In contrast, the first and last minutes of the 6MWT were not found to be informative for disease phenotyping. The middle portion of another long-duration gait test (400 m walking test, which is comparable with 6MWT for test duration) was recently reported to be more representative of an individual’s gait characteristics since it may provide better resolution for fatigue quantification as participants often increase gait speed during the initial and ending stages of the assessment [46,47,48]. However, previous research also demonstrated that the 6MWT could elicit a more significant fatigue effect in individuals with neurological gait impairments (multiple sclerosis) toward the end of the test [18]. Therefore, the most sensitive portion of a gait test for disease phenotyping may be disease-specific, and further investigation is needed.
There are several limitations to this study. The sample size is small, as is typical of an early investigation. More extensive studies are warranted to confirm our results. There were few minute-by-minute fluctuations during the 6MWT in any group, including healthy controls, suggesting that a six-minute walk may not provide sufficient time to detect the gait changes induced by LSS and KOA.
5. Conclusions
By examining gait parameters derived from foot-mounted IMU sensors worn during a 6MWT, we identified multiple parameters (in all four domains: rhythm, pace, asymmetry, and variability) that can distinguish between HC and patients with mobility limitations. Additional temporal analysis of the 6MWT on a minute-by-minute basis revealed a significantly higher stride length variability for LSS than KOA during the middle portion of the walk test. Gait variability may be a potential biomarker to distinguish gait impairment from neurological and structural joint diseases. The middle portion of the walk test may be a unique window to reveal the subtle differences observed between these conditions.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/s22239301/s1, Supplementary File S1: Participants’ demographic characteristics. Supplementary File S2: Changes in parameters from minute-to-minute analysis of 6MWT. Supplementary File S3: Radar plot illustrating the gait parameters extracted from analysis of the entire 6MWT (Data comparison between limbs). Supplementary File S4: The gait parameters extracted from analysis of the entire 6MWT (Data comparison between limbs). Supplementary File S5: Changes in parameters from minute-by-minute analysis of 6MWT (Data comparison between limbs). Supplementary File S6: Details on gait parameter extraction [21,49,50,51,52].
Author Contributions
Designed experiments: J.K., R.S., W.Z. and M.S., performed experiments: J.K., R.S., A.M., H.L. and W.Z., data analysis: J.K., R.S. and W.Z., writing and editing of manuscript: J.K., R.S., W.Z., A.M., H.L., C.A.O. and M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by departmental funding and unrestricted gift funding from the Stanford University Department of Orthopaedic Surgery.
Institutional Review Board Statement
The study was HIPAA compliant and approved by the ethical committee for Human Subjects Research at Stanford University.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data of this article are available from the authors on reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kannus, P.; Sievänen, H.; Palvanen, M.; Järvinen, T.; Parkkari, J. Prevention of falls and consequent injuries in elderly people. Lancet 2005, 366, 1885–1893. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Berg, K.; Chesworth, B.; Klar, N.; Speechley, M. Quantifying the magnitude of risk for balance impairment on falls in community-dwelling older adults: A systematic review and meta-analysis. J. Clin. Epidemiol. 2010, 63, 389–406. [Google Scholar] [CrossRef] [PubMed]
- Esser, S.; Bailey, A. Effects of Exercise and Physical Activity on Knee Osteoarthritis. Curr. Pain Headache Rep. 2011, 15, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Garstang, S.V.; Stitik, T.P. Osteoarthritis: Epidemiology, Risk Factors, and Pathophysiology. Am. J. Phys. Med. Rehabil. 2006, 85, S2–S11. [Google Scholar] [CrossRef]
- Ishimoto, Y.; Yoshimura, N.; Muraki, S.; Yamada, H.; Nagata, K.; Hashizume, H.; Takiguchi, N.; Minamide, A.; Oka, H.; Kawaguchi, H.; et al. Prevalence of symptomatic lumbar spinal stenosis and its association with physical performance in a population-based cohort in Japan: The Wakayama Spine Study. Osteoarthr. Cartil. 2012, 20, 1103–1108. [Google Scholar] [CrossRef] [Green Version]
- Cutler, D.M. Disability and the Future of Medicare. N. Engl. J. Med. 2003, 349, 1084–1085. [Google Scholar] [CrossRef]
- Lubitz, J.; Cai, L.; Kramarow, E.; Lentzner, H. Health, Life Expectancy, and Health Care Spending among the Elderly. N. Engl. J. Med. 2003, 349, 1048–1055. [Google Scholar] [CrossRef] [Green Version]
- Yelin, E. Cost of musculoskeletal diseases: Impact of work disability and functional decline. J. Rheumatol. Suppl. 2003, 68, 8–11. [Google Scholar]
- Katz, J.N.; Harris, M.B. Clinical practice. Lumbar spinal stenosis. N. Engl. J. Med. 2008, 358, 818–825. [Google Scholar] [CrossRef]
- Sharma, L. Osteoarthritis of the Knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef]
- Simon, L.S. Osteoarthritis: A review. Clin. Cornerstone 1999, 2, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Odonkor, C.; Kuwabara, A.; Tomkins-Lane, C.; Zhang, W.; Muaremi, A.; Leutheuser, H.; Sun, R.; Smuck, M. Gait features for discriminating between mobility-limiting musculoskeletal disorders: Lumbar spinal stenosis and knee osteoarthritis. Gait Posture 2020, 80, 96–100. [Google Scholar] [CrossRef]
- Rudisch, J.; Jöllenbeck, T.; Vogt, L.; Cordes, T.; Klotzbier, T.J.; Vogel, O.; Wollesen, B. Agreement and consistency of five different clinical gait analysis systems in the assessment of spatiotemporal gait parameters. Gait Posture 2021, 85, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Sagawa, Y.; Armand, S.; Lubbeke, A.; Hoffmeyer, P.; Fritschy, D.; Suva, D.; Turcot, K. Associations between gait and clinical parameters in patients with severe knee osteoarthritis: A multiple correspondence analysis. Clin. Biomech. 2013, 28, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Zeifang, F.; Schiltenwolf, M.; Abel, R.; Moradi, B. Gait analysis does not correlate with clinical and MR imaging parameters in patients with symptomatic lumbar spinal stenosis. BMC Musculoskelet. Disord. 2008, 9, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Din, S.; Galna, B.; Godfrey, A.; Bekkers, E.M.J.; Pelosin, E.; Nieuwhof, F.; Mirelman, A.; Hausdorff, J.M.; Rochester, L. Analysis of Free-Living Gait in Older Adults with and without Parkinson’s Disease and with and without a History of Falls: Identifying Generic and Disease-Specific Characteristics. J. Gerontol. Ser. A 2017, 74, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Gouelle, A.; Mégrot, F.; Presedo, A.; Husson, I.; Yelnik, A.; Penneçot, G.-F. The Gait Variability Index: A new way to quantify fluctuation magnitude of spatiotemporal parameters during gait. Gait Posture 2013, 38, 461–465. [Google Scholar] [CrossRef]
- Shema-Shiratzky, S.; Gazit, E.; Sun, R.; Regev, K.; Karni, A.; Sosnoff, J.J.; Herman, T.; Mirelman, A.; Hausdorff, J.M. Deterioration of specific aspects of gait during the instrumented 6-min walk test among people with multiple sclerosis. J. Neurol. 2019, 266, 3022–3030. [Google Scholar] [CrossRef]
- Burschka, J.M.; Keune, P.M.; Menge, U.; Oy, U.H.-V.; Oschmann, P.; Hoos, O. An exploration of impaired walking dynamics and fatigue in Multiple Sclerosis. BMC Neurol. 2012, 12, 161. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.; Sosnoff, J.J. Novel sensing technology in fall risk assessment in older adults: A systematic review. BMC Geriatr. 2018, 18, 14. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Smuck, M.; Legault, C.; Ith, M.A.; Muaremi, A.; Aminian, K. Gait Symmetry Assessment with a Low Back 3D Accelerometer in Post-Stroke Patients. Sensors 2018, 18, 3322. [Google Scholar] [CrossRef] [PubMed]
- Kobsar, D.; Charlton, J.M.; Tse, C.T.F.; Esculier, J.-F.; Graffos, A.; Krowchuk, N.M.; Thatcher, D.; Hunt, M.A. Validity and reliability of wearable inertial sensors in healthy adult walking: A systematic review and meta-analysis. J. Neuroeng. Rehabil. 2020, 17, 62. [Google Scholar] [CrossRef] [PubMed]
- Kobsar, D.; Masood, Z.; Khan, H.; Khalil, N.; Kiwan, M.Y.; Ridd, S.; Tobis, M. Wearable Inertial Sensors for Gait Analysis in Adults with Osteoarthritis-A Scoping Review. Sensors 2020, 20, 7143. [Google Scholar] [CrossRef] [PubMed]
- Ware, J.E.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Dobson, F.; Hinman, R.S.; Hall, M.; Marshall, C.J.; Sayer, T.; Anderson, C.; Newcomb, N.; Stratford, P.W.; Bennell, K.L. Reliability and measurement error of the Osteoarthritis Research Society International (OARSI) recommended performance-based tests of physical function in people with hip and knee osteoarthritis. Osteoarthr. Cartil. 2017, 25, 1792–1796. [Google Scholar] [CrossRef] [Green Version]
- Tomkins, C.C.; Battié, M.; Rogers, T.; Jiang, H.; Petersen, S. A Criterion Measure of Walking Capacity in Lumbar Spinal Stenosis and Its Comparison with a Treadmill Protocol. Spine 2009, 34, 2444–2449. [Google Scholar] [CrossRef]
- Stellmann, J.P.; Neuhaus, A.; Götze, N.; Briken, S.; Lederer, C.; Schimpl, M.; Heesen, C.; Daumer, M. Ecological Validity of Walking Capacity Tests in Multiple Sclerosis. PLoS ONE 2015, 10, e01238222. [Google Scholar] [CrossRef] [Green Version]
- Motl, R.W.; Pilutti, L.; Sandroff, B.M.; Dlugonski, D.; Sosnoff, J.J.; Pula, J.H. Accelerometry as a measure of walking behavior in multiple sclerosis. Acta Neurol. Scand. 2013, 127, 384–390. [Google Scholar] [CrossRef]
- Moon, Y.; Sung, J.; An, R.; Hernandez, M.E.; Sosnoff, J.J. Gait variability in people with neurological disorders: A systematic review and meta-analysis. Hum. Mov. Sci. 2016, 47, 197–208. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Rios, D.A.; Edelberg, H.K. Gait variability and fall risk in community-living older adults: A 1-year prospective study. Arch. Phys. Med. Rehabil. 2001, 82, 1050–1056. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Herman, T.; Weiss, A.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. Gait and balance in Parkinson’s disease subtypes: Objective measures and classification considerations. J. Neurol. 2014, 261, 2401–2410. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Brozgol, M.; Dorfman, M.; Herman, T.; Shema, S.; Giladi, N.; Hausdorff, J.M. Does the evaluation of gait quality during daily life provide insight into fall risk? A novel approach using 3-day accelerometer recordings. Neurorehabil. Neural. Repair. 2013, 27, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Weiss, A.; Herman, T.; Giladi, N.; Hausdorff, J.M. Objective assessment of fall risk in Parkinson’s disease using a body-fixed sensor worn for 3 days. PLoS ONE 2014, 9, e96675. [Google Scholar] [CrossRef] [Green Version]
- Brach, J.S.; Studenski, S.; Perera, S.; VanSwearingen, J.M.; Newman, A.B. Stance time and step width variability have unique contributing impairments in older persons. Gait Posture 2008, 27, 431–439. [Google Scholar] [CrossRef] [Green Version]
- Baltadjieva, R.; Giladi, N.; Gruendlinger, L.; Peretz, C.; Hausdorff, J.M. Marked alterations in the gait timing and rhythmicity of patients with de novo Parkinson’s disease. Eur. J. Neurosci. 2006, 24, 1815–1820. [Google Scholar] [CrossRef]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef]
- Wittwer, J.E.; Webster, K.E.; Hill, K. Reproducibility of gait variability measures in people with Alzheimer’s disease. Gait Posture 2013, 38, 507–510. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Lertratanakul, A.; Cudkowicz, M.E.; Peterson, A.L.; Kaliton, D.; Goldberger, A.L. Dynamic markers of altered gait rhythm in amyotrophic lateral sclerosis. J. Appl. Physiol. 2000, 88, 2045–2053. [Google Scholar] [CrossRef] [Green Version]
- Schniepp, R.; Wuehr, M.; Schlick, C.; Huth, S.; Pradhan, C.; Dieterich, M.; Brandt, T.; Jahn, K. Increased gait variability is associated with the history of falls in patients with cerebellar ataxia. J. Neurol. 2013, 261, 213–223. [Google Scholar] [CrossRef]
- Rao, A.K.; Muratori, L.; Louis, E.D.; Moskowitz, C.B.; Marder, K.S. Spectrum of gait impairments in presymptomatic and symptomatic Huntington’s disease. Mov. Disord. 2008, 23, 1100–1107. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Sandroff, B.M.; Motl, R.W. Quantifying gait abnormalities in persons with multiple sclerosis with minimal disability. Gait Posture 2012, 36, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Bello, O.; Sánchez, J.A.; Vazquez-Santos, C.; Fernandez-Del-Olmo, M. Spatiotemporal parameters of gait during treadmill and overground walking in Parkinson’s disease. J. Parkinsons Dis. 2014, 4, 33–36. [Google Scholar] [CrossRef] [Green Version]
- Natarajan, P.; Fonseka, R.D.; Sy, L.W.; Maharaj, M.M.; Mobbs, R.J. Analysing Gait Patterns in Degenerative Lumbar Spine Disease Using Inertial Wearable Sensors: An Observational Study. World Neurosurg. 2022, 163, e501–e515. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, N.C.; Christakis, D.G.; Tzagarakis, G.N.; Chlouverakis, G.I.; Kampanis, N.A.; Stergiopoulos, K.N.; Katonis, P.G. Gait variability measurements in lumbar spinal stenosis patients: Part A. Comparison with healthy subjects. Physiol. Meas. 2009, 30, 1171–1186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krumpoch, S.; Lindemann, U.; Becker, C.; Sieber, C.C.; Freiberger, E. Short distance analysis of the 400-meter walk test of mobility in community-dwelling older adults. Gait Posture 2021, 88, 60–65. [Google Scholar] [CrossRef]
- Glynn, N.W.; Qiao, Y.S.; Simonsick, E.M.; Schrack, J.A. Response to: Comment on: Fatigability: A Prognostic Indicator of Phenotypic Aging. J. Gerontol. Ser. A 2021, 76, e161–e162. [Google Scholar] [CrossRef]
- Qiao, Y.S.; Harezlak, J.; Moored, K.D.; Urbanek, J.K.; Boudreau, R.M.; Toto, P.E.; Hawkins, M.; Santanasto, A.J.; Schrack, J.A.; Simonsick, E.M.; et al. Development of a Novel Accelerometry-Based Performance Fatigability Measure for Older Adults. Med. Sci. Sports Exerc. 2022, 54, 1782–1793. [Google Scholar] [CrossRef]
- Mariani, B.; Rouhani, H.; Crevoisier, X.; Aminian, K. Quantitative estimation of foot-flat and stance phase of gait using foot-worn inertial sensors. Gait Posture 2013, 37, 229–234. [Google Scholar] [CrossRef]
- Mariani, B.; Hoskovec, C.; Rochat, S.; Büla, C.; Penders, J.; Aminian, K. 3D gait assessment in young and elderly subjects using foot-worn inertial sensors. J. Biomech. 2010, 43, 2999–3006. [Google Scholar] [CrossRef]
- Foxlin, E. Pedestrian tracking with shoe-mounted inertial sensors. IEEE Comput. Graph. Appl. 2005, 25, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Mariani, B.; Rochat, S.; Büla, C.J.; Aminian, K. Heel and toe clearance estimation for gait analysis using wireless inertial sensors. IEEE Trans. Biomed. Eng. 2012, 59, 3162–3168. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Radar plot illustrating the gait parameters extracted from the analysis of the entire 6MWT. The central black dots with connecting dashed lines represent HC data. This is compared to LSS (blue squares and lines) and KOA (red triangles and lines) with deviation along the axis radiating from the center of the plot representing the standard deviations (range; from −3 SD to +6 SD) from HC. (HC; healthy control, LSS; lumbar spinal stenosis, KOA; knee osteoarthritis, CV; coefficient of variation, SD; standard deviations).
Figure 1.
Radar plot illustrating the gait parameters extracted from the analysis of the entire 6MWT. The central black dots with connecting dashed lines represent HC data. This is compared to LSS (blue squares and lines) and KOA (red triangles and lines) with deviation along the axis radiating from the center of the plot representing the standard deviations (range; from −3 SD to +6 SD) from HC. (HC; healthy control, LSS; lumbar spinal stenosis, KOA; knee osteoarthritis, CV; coefficient of variation, SD; standard deviations).

Figure 2.
Changes in representative parameters from the minute-by-minute analysis of the 6MWT. The * identifies a significant difference between LSS and KOA (p < 0.05). (HC; healthy control, LSS; lumbar spinal stenosis, KOA; knee osteoarthritis, CV; coefficient of variation).
Figure 2.
Changes in representative parameters from the minute-by-minute analysis of the 6MWT. The * identifies a significant difference between LSS and KOA (p < 0.05). (HC; healthy control, LSS; lumbar spinal stenosis, KOA; knee osteoarthritis, CV; coefficient of variation).


{kind=link}
{kind=link}
Table 1.
Descriptions of the extracted spatiotemporal parameters.
| Domain | Parameter | Unit | Description |
|---|---|---|---|
| Rhythm | Cadence | steps/min | Number of steps per minute |
| Double support ratio | % | Percentage of the cycle where both feet are on the ground | |
| Swing Ratio | % | Percentage of the cycle during which the foot is in the air and does not touch the ground | |
| Pace | Stride Length | meter | Distance between two successive heel strides. |
| Speed | m/s | Forward stride speed of one cycle | |
| Asymmetry | Stride length asymmetry | % | Symmetry index of stride length |
| Swing asymmetry | % | Symmetry index of swing | |
| Variability | CV for double support | % | Coefficient of variation for double support |
| CV for swing | % | Coefficient of variation for swing | |
| CV for stride length | % | Coefficient of variation for stride length | |
| CV for cycle duration | % | Coefficient of variation for cycle duration |
CV: coefficient of variation.
Table 2.
Gait parameters extracted from the analysis of the entire 6MWT.
| p Value | |||||||
|---|---|---|---|---|---|---|---|
| Domain | Parameter | HC | LSS | KOA | HC-LSS | HC-KOA | LSS-KOA |
| Rhythm | Cadence (steps/min) | 120.3 (8.2) | 106.1 (10.2) | 104.6 (7.1) | 0.003 | 0.001 | 0.900 |
| Double Support (%) | 21.9 (4.0) | 29.7 (5.2) | 28.5 (5.9) | 0.005 | 0.019 | 0.861 | |
| Swing (%) | 39.1 (2.0) | 35.1 (2.6) | 35.7 (2.9) | 0.005 | 0.019 | 0.851 | |
| Pace | Speed (m/s) | 1.5 (0.3) | 1.1 (0.3) | 1.0 (0.2) | 0.010 | 0.003 | 0.878 |
| Stride Length (m) | 1.4 (0.2) | 1.2 (0.3) | 1.2 (0.2) | 0.057 | 0.022 | 0.900 | |
| Asymmetry | Stride Length Asymmetry (%) | 4.5 (0.4) | 4.6 (0.5) | 4.3 (0.5) | 0.900 | 0.416 | 0.340 |
| Swing Asymmetry (%) | 4.0 (2.1) | 8.1 (4.9) | 9.7 (6.8) | 0.043 | 0.010 | 0.797 | |
| Variability | Stride Length CV (%) | 3.6 (0.3) | 4.7 (0.8) | 4.0 (0.8) | 0.003 | 0.470 | 0.057 |
| Cycle Duration CV (%) | 1.9 (0.7) | 3.1 (0.9) | 2.8 (0.8) | 0.003 | 0.025 | 0.678 | |
| Swing CV (%) | 1.9 (0.5) | 3.1 (1.1) | 2.7 (0.7) | 0.003 | 0.025 | 0.628 | |
| Double Support CV (%) | 7.1 (2.9) | 7.2 (1.2) | 7.2 (2.8) | 0.898 | 0.900 | 0.900 | |
Significant p values (p < 0.05) are shown in bold. (HC; healthy control, LSS; lumbar spinal stenosis, KOA; knee osteoarthritis, CV; coefficient of variation).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kushioka, J.; Sun, R.; Zhang, W.; Muaremi, A.; Leutheuser, H.; Odonkor, C.A.; Smuck, M. Gait Variability to Phenotype Common Orthopedic Gait Impairments Using Wearable Sensors. Sensors 2022, 22, 9301. https://doi.org/10.3390/s22239301
AMA Style
Kushioka J, Sun R, Zhang W, Muaremi A, Leutheuser H, Odonkor CA, Smuck M. Gait Variability to Phenotype Common Orthopedic Gait Impairments Using Wearable Sensors. Sensors. 2022; 22(23):9301. https://doi.org/10.3390/s22239301
Chicago/Turabian StyleKushioka, Junichi, Ruopeng Sun, Wei Zhang, Amir Muaremi, Heike Leutheuser, Charles A. Odonkor, and Matthew Smuck. 2022. "Gait Variability to Phenotype Common Orthopedic Gait Impairments Using Wearable Sensors" Sensors 22, no. 23: 9301. https://doi.org/10.3390/s22239301
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.