

Real-Time Detection and 3D Localization of Coronary Atherosclerosis Using a Microwave Imaging Technique: A Simulation Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Imaging Method
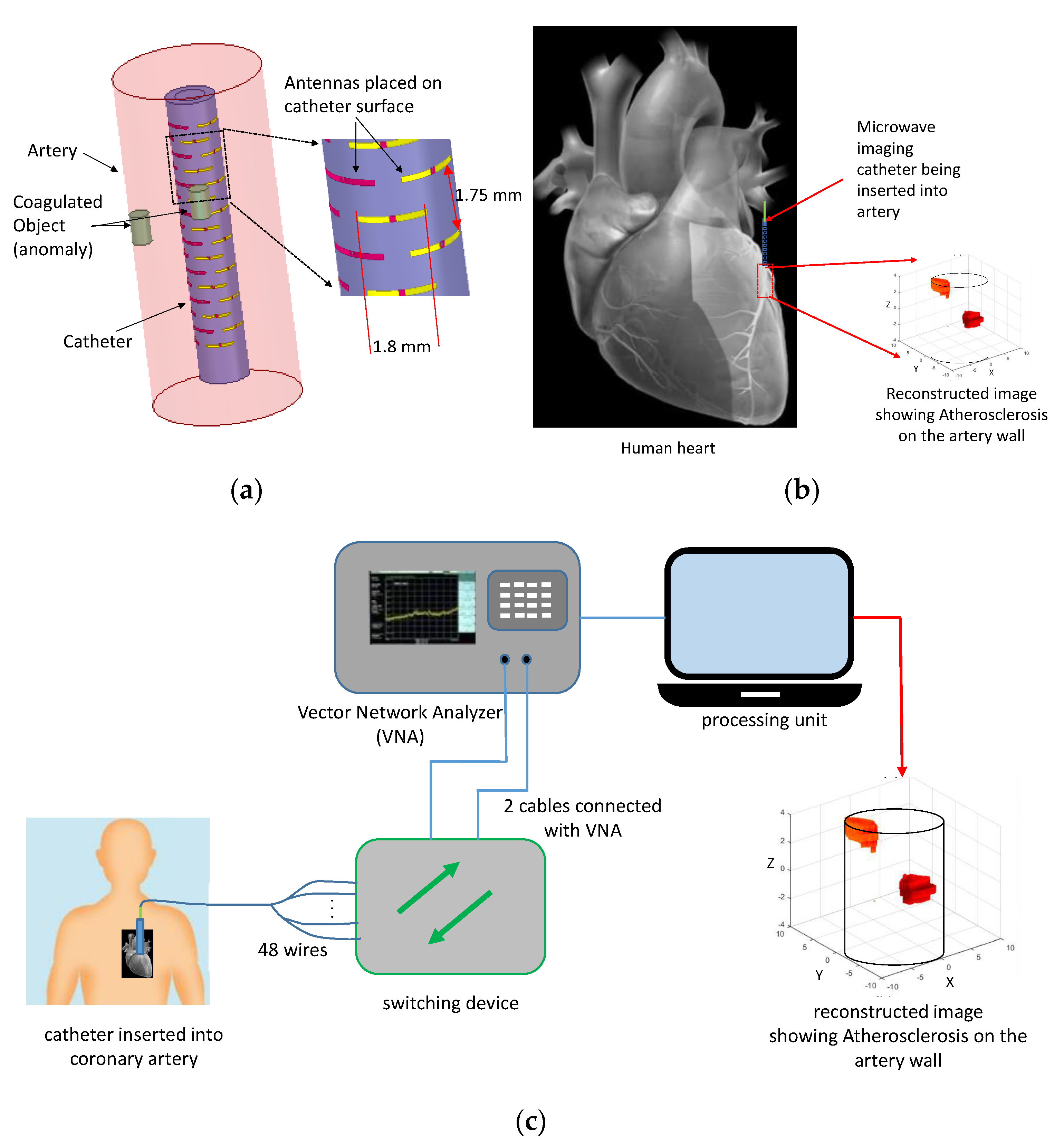
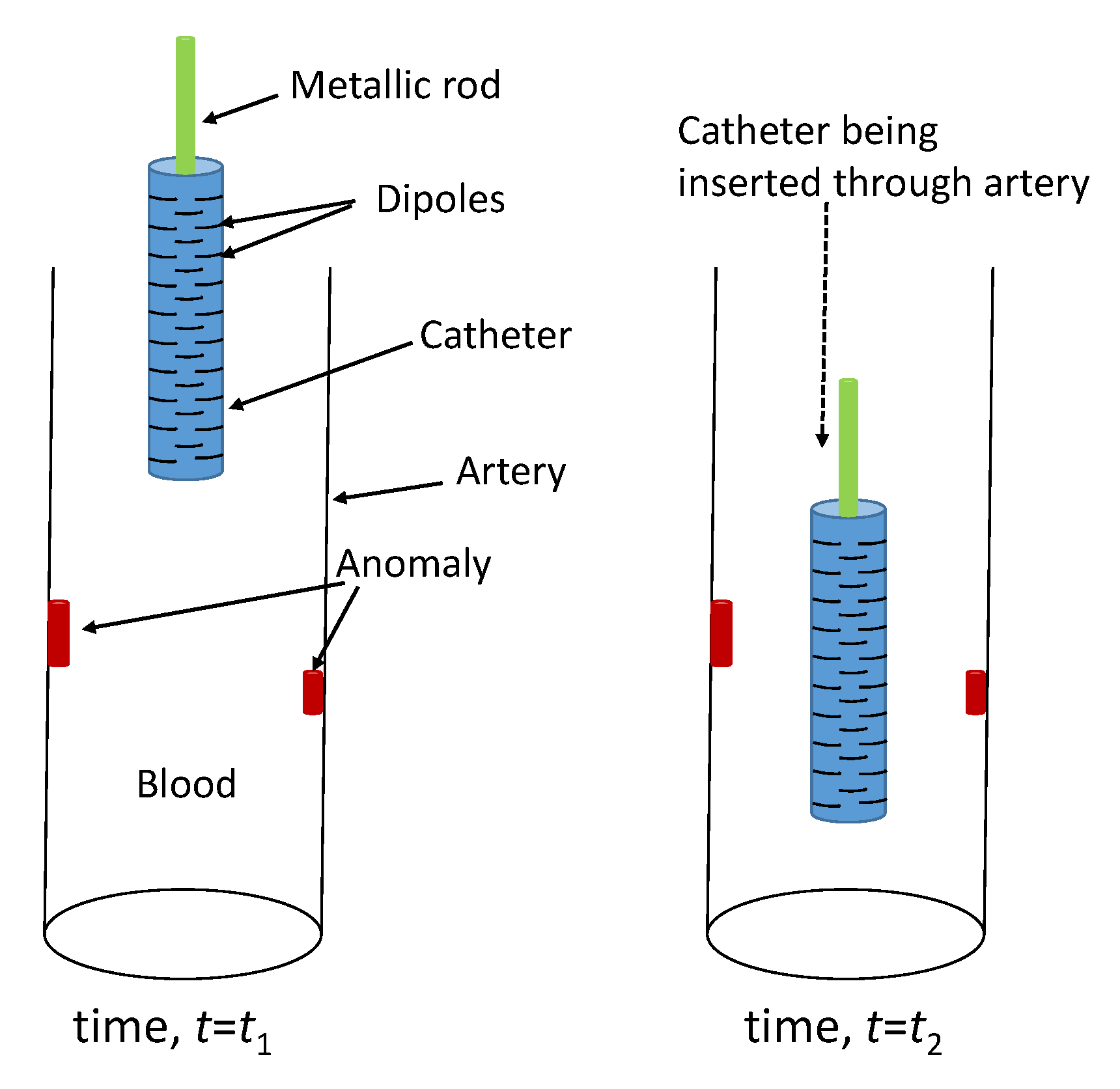
2.1. Catheter Design
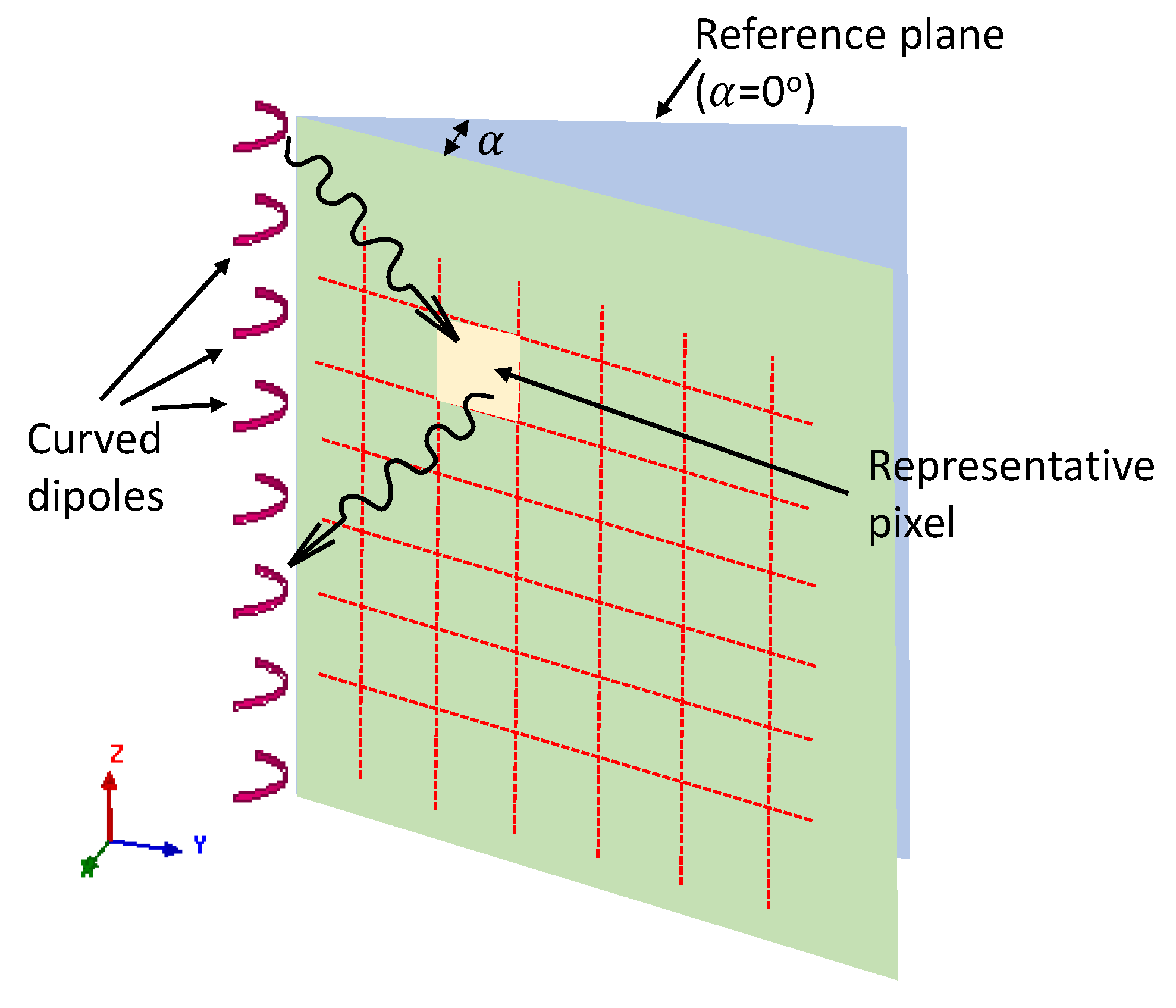
2.2. Imaging Process
3. Data Generation and Imaging Results
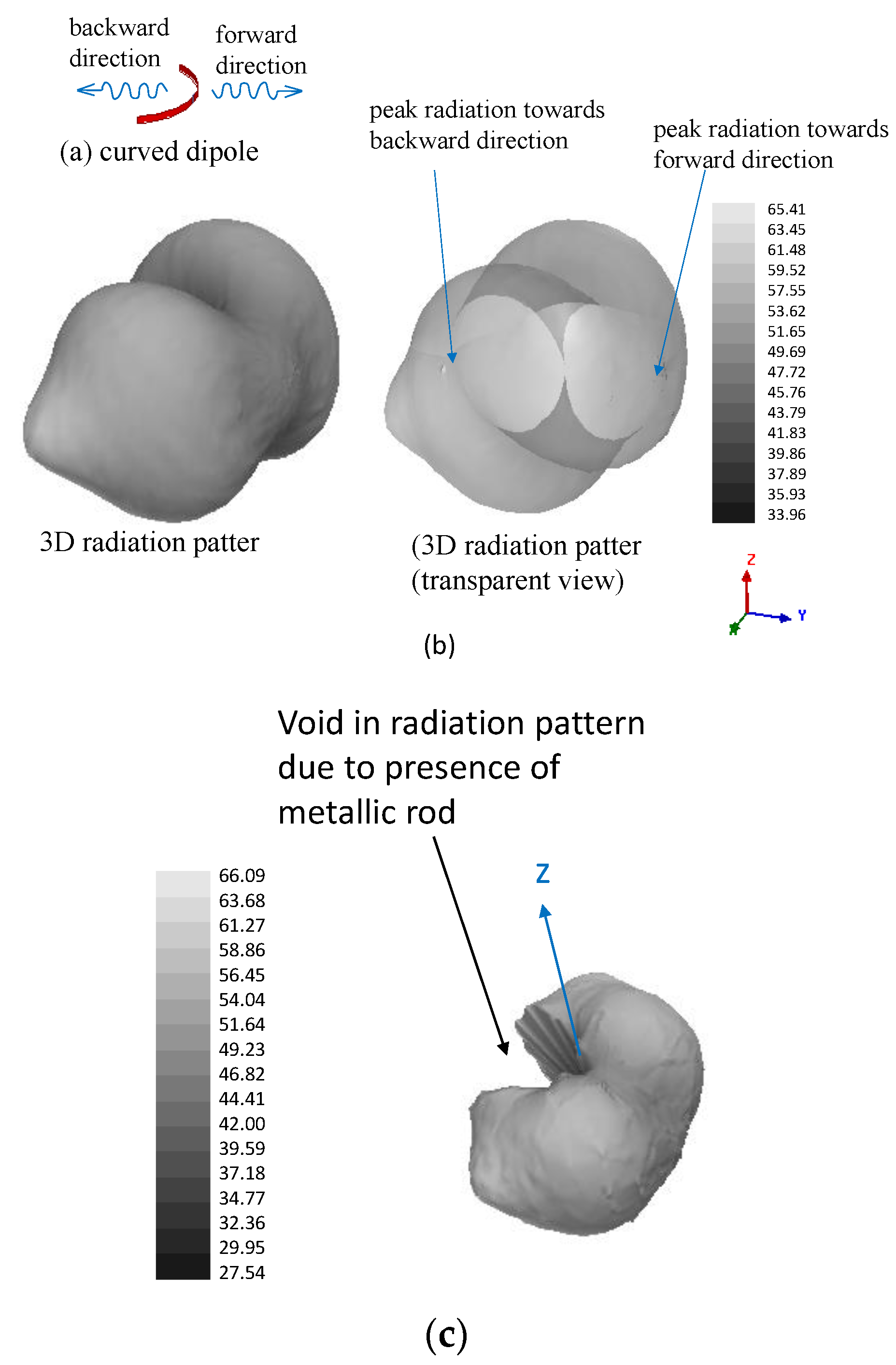
3.1. Justification of Using Metallic Rod in the Catheter (Resolving ‘Image Ambiguity’)
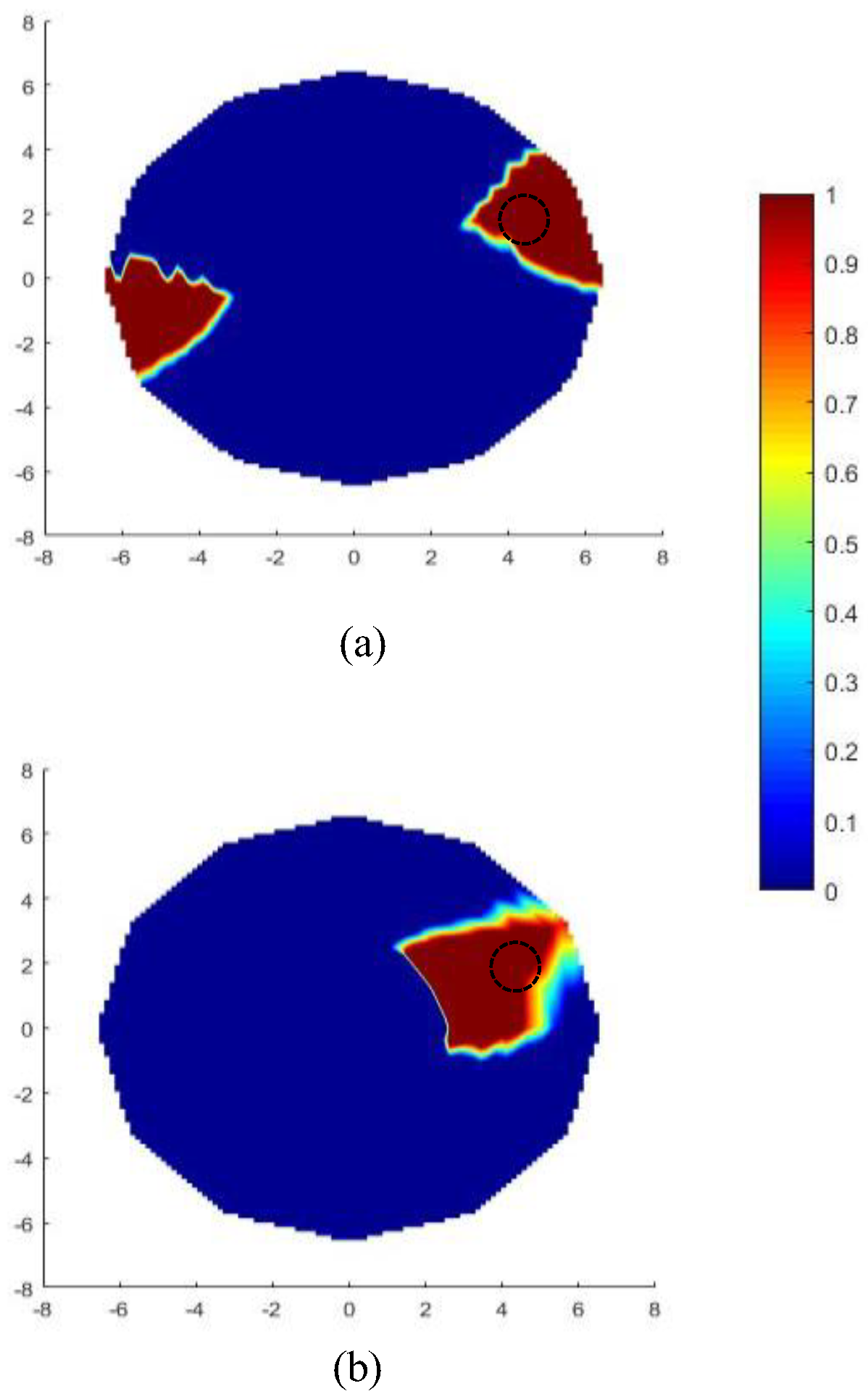
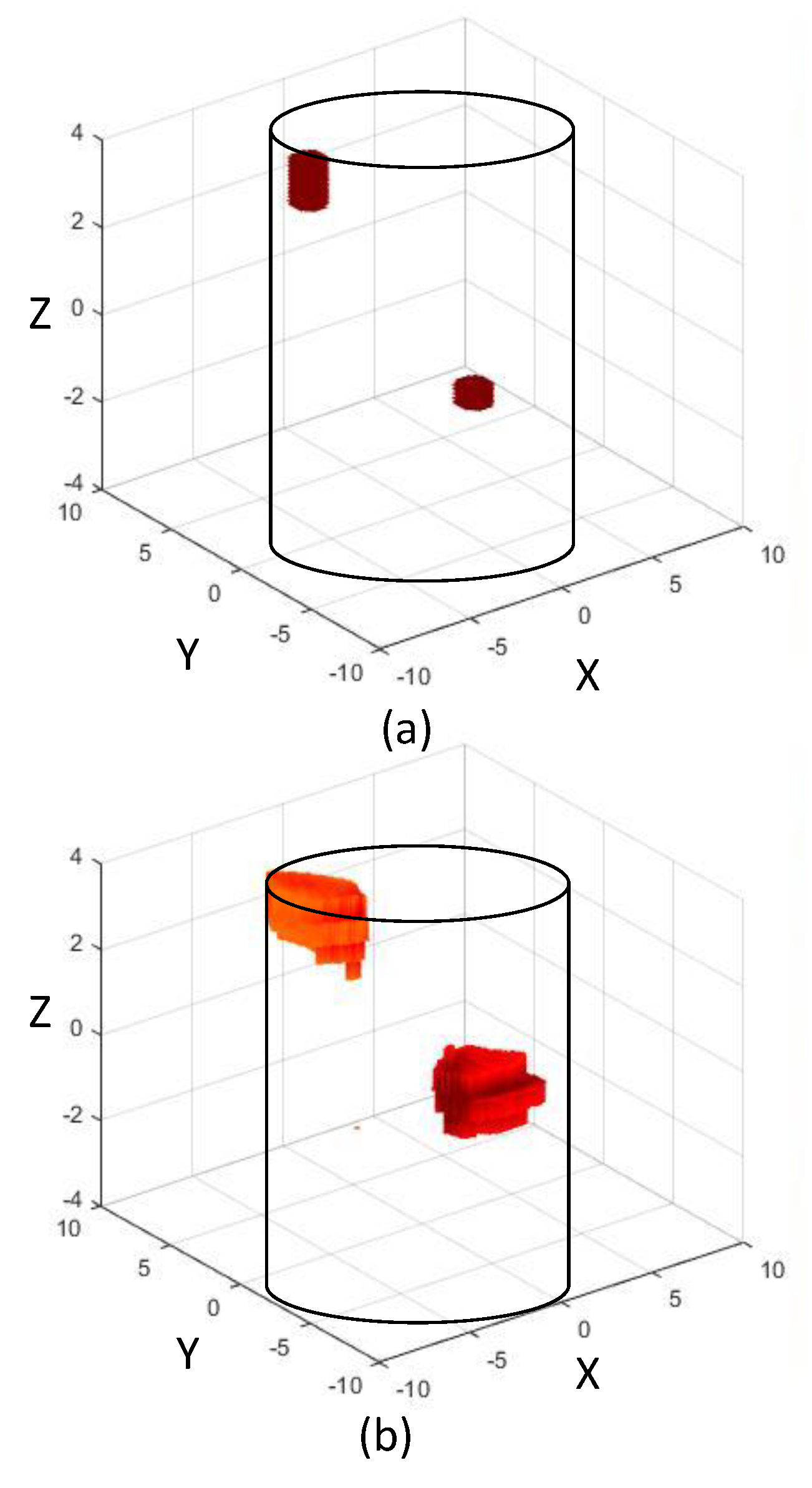
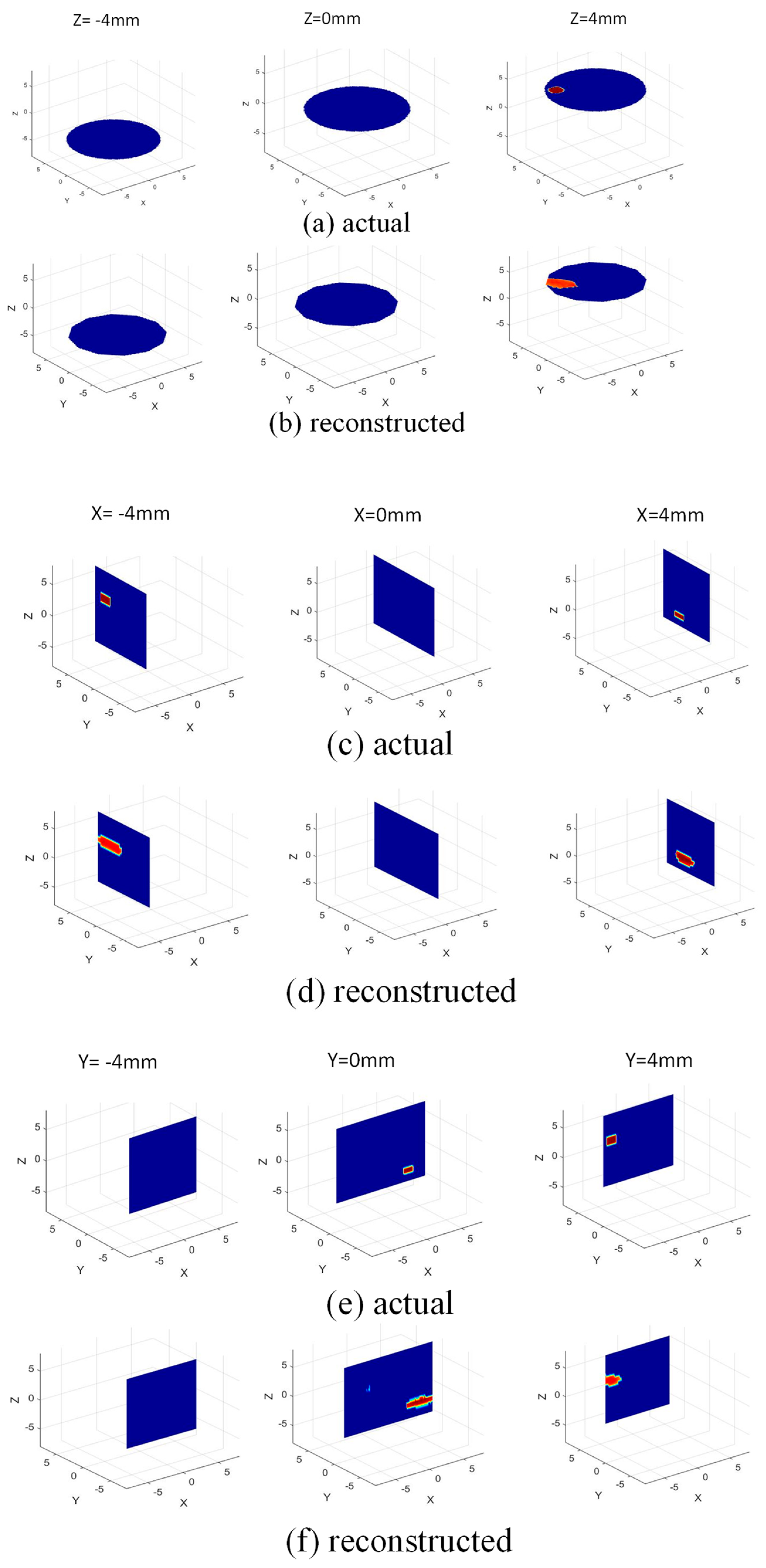
3.2. Imaging Scenario and Results
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, G.; Springelin, G.; Lovrak, M.; Mastik, F.; Iskander-Rizk, S.; Wang, T.; van Beusekom, H.M.M.; van der Steen, A.F.W.; Soest, G.V. Real-time volumetric lipid imaging in vivo by intravascular photoacoustics at 20 frames per second. Biomed. Opt. Exp. 2017, 8, 943–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourantas, C.V.; Jaffer, F.A.; Gijsen, F.J.; van Soest, G.; Madden, S.P.; Courtney, B.K.; Fard, A.M.; Tenekecioglu, E.; Zeng, Y.; Van Der Steen, A.F.; et al. Hybrid intravascular imaging: Recent advances, technical considerations, and current applications in the study of plaque pathophysiology. Eur. Heart J. 2016, 38, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Shuurman, A.S.; Vroegindewey, M.M.; Kardys, I.; Oemrawsingh, R.M.; Garcia-Garcia, H.M.; van Geuns, R.-J.; Regar, E.; Van Mieghem, N.M.; Ligthart, J.; Serruys, P.W.; et al. Prognostic Value of Intravascular Ultrasound in Patients with Coronary Artery Disease. Eur. Heart J. 2018, 72, 2003–2011. [Google Scholar]
- Hasan, M.S.M.; Faluk, M.; Patel, J.D.; Abdelmaseih, R.; Patel, J. Use of optical coherence tomography in coronary artery disease: Review article. Curr. Probl. Cardiol. 2020, 46, 100597. [Google Scholar] [CrossRef]
- Karlsson, S.; Anesäter, E.; Fransson, K.; Andell, P.; Persson, J.; Erlinge, D. Intracoronary near-infrared spectroscopy and the risk of future cardiovascular events. Open Heart 2019, 6, e000917. [Google Scholar] [CrossRef]
- Hui, J.; Cao, Y.; Zhang, Y.; Kole, A.; Wang, P.; Yu, G.; Eakins, G.; Sturek, M.; Chen, W.; Cheng, J.-X. Real-time intravascular photoacoustic-ultrasound imaging of lipid-laden plaque in human coronary artery at 16 frames per second. Sci. Rep. 2017, 7, 1417. [Google Scholar] [CrossRef] [Green Version]
- Bertrand, M.-J.; Abran, M.; Maafi, F.; Busseuil, D.; Merlet, N.; Mihalache-Avram, T.; Geoffroy, P.; Tardif, P.-L.; Abulrob, A.; Arbabi-Ghahroudi, M.; et al. In Vivo Near-Infrared Fluorescence Imaging of Atherosclerosis Using Local Delivery of Novel Targeted Molecular Probes. Sci. Rep. 2019, 9, 2670. [Google Scholar] [CrossRef] [Green Version]
- Lagarto, J.; Dyer, B.T.; Talbot, C.; Sikkel, M.B.; Peters, N.S.; French, P.M.W.; Lyon, A.R.; Dunsby, C. Application of time-resolved autofluorescence to label-free in vivo optical mapping of changes in tissue matrix and metabolism associated with myocardial infarction and heart failure. Biomed. Opt. Express 2015, 6, 324–346. [Google Scholar] [CrossRef] [Green Version]
- Islam, A.; Kiourti, A.; Volakis, J.L. A Novel Method to Mitigate Real–Imaginary Image Imbalance in Microwave Tomography. IEEE Trans. Biomed. Eng. 2019, 67, 1328–1337. [Google Scholar] [CrossRef]
- Islam, A.; Kiourti, A.; Volakis, J.L. A modified Gauss-Newton algorithm for fast microwave imaging using near-field probes. Microw. Opt. Technol. Lett. 2017, 59, 1394–1400. [Google Scholar] [CrossRef]
- Fear, E.; Li, X.; Hagness, S.; Stuchly, M. Confocal microwave imaging for breast cancer detection: Localization of tumors in three dimensions. IEEE Trans. Biomed. Eng. 2002, 49, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Davis, S.; Hagness, S.; van der Weide, D.; Van Veen, B. Microwave Imaging via Space–Time Beamforming: Experimental Investigation of Tumor Detection in Multilayer Breast Phantoms. IEEE Trans. Microw. Theory Technol. 2004, 52, 1856–1865. [Google Scholar] [CrossRef] [Green Version]
- Li, D.; Meaney, P.; Paulsen, K. Conformal microwave imaging for breast cancer detection. IEEE Trans. Microw. Theory Technol. 2003, 51, 1179–1186. [Google Scholar] [CrossRef] [Green Version]
- Paulsen, K.; Poplack, S.; Li, D.; Fanning, M.; Meaney, P. A clinical prototype for active microwave imaging of the breast. IEEE Trans. Microw. Theory Technol. 2000, 48, 1841–1853. [Google Scholar] [CrossRef]
- Rubaek, T.; Kim, O.S.; Meincke, P. Computational Validation of a 3-D Microwave Imaging System for Breast-Cancer Screening. IEEE Trans. Antennas Propag. 2009, 57, 2105–2115. [Google Scholar] [CrossRef] [Green Version]
- Gilmore, C.; Mojabi, P.; Zakaria, A.; Ostadrahimi, M.; Kaye, C.; Noghanian, S.; Shafai, L.; Pistorius, S.; LoVetri, J. A Wideband Microwave Tomography System With a Novel Frequency Selection Procedure. IEEE Trans. Biomed. Eng. 2009, 57, 894–904. [Google Scholar] [CrossRef] [PubMed]
- Ostadrahimi, M.; Zakaria, A.; LoVetri, J.; Shafai, L. A Near-Field Dual Polarized (TE–TM) Microwave Imaging System. IEEE Trans. Microw. Theory Technol. 2013, 61, 1376–1384. [Google Scholar] [CrossRef]
- Haynes, M.; Stang, J.; Moghaddam, M. Real-time Microwave Imaging of Differential Temperature for Thermal Therapy Monitoring. IEEE Trans. Biomed. Eng. 2014, 61, 1787–1797. [Google Scholar] [CrossRef] [Green Version]
- Pour Ebrahim, M.; Sarvi, M.; Yuce, M.R. A Doppler Radar System for Sensing Physiological Parameters in Walking and Standing Positions. Sensors 2017, 17, 485. [Google Scholar] [CrossRef] [Green Version]
- Chuma, E.L.; Lano, Y. A movement detection system using continuous-wave doppler radar sensor and convolutional neural network to detect cough and other gestures. IEEE Sens. J. 2021, 21, 2921–2927. [Google Scholar] [CrossRef]
- Tran, V.P.; Al-Jumaily, A.A.; Islam, S.M.S. Doppler Radar-Based Non-Contact Health Monitoring for Obstructive Sleep Apnea Diagnosis: A Comprehensive Review. Big Data Cogn. Comput. 2019, 3, 3. [Google Scholar] [CrossRef]
- IEEE Standard C95.1; IEEE Standard for Safety Levels with Respect to Human Exposure to Radiofrequency Electromagnetic Fields, 3 kHz to 300 GHz. Institute of Electrical and Electronics Engineers: Piscataway, NJ, USA, 1999.
- Federal Communications Commission. Evaluating Compliance with FCC Guidelines for Human Exposure to Radio Frequency Electromagnetic Fields, FCC OET Bulletin.65; Federal Communications Commission: Washington, DC, USA, 1997. [Google Scholar]
- Islam, M.A.; Volakis, J.L. Wearable microwave imaging sensor for deep tissue real-time monitoring using a new loss-compensated backpropagation technique. IEEE Sens. J. 2021, 21, 3324–3334. [Google Scholar]
- Gabriel, S.; Lau, R.W.; Gabriel, C. The dielectric properties of biological tissues—Part II: Measurement in the frequency range 10 Hz to 20 GHz. Phys. Med. Biol. 1996, 41, 2251–2269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabriel, S.; Lau, R.W.; Gabriel, C. The dielectric properties of biological tissues: III. Parametric models for the dielectric spectrum of tissues. Phys. Med. Biol. 1996, 41, 2271–2293. [Google Scholar] [CrossRef] [Green Version]
- Ghavami, N.; Tiberi, G.; Edwards, D.J.; Monorchio, A. UWB Microwave Imaging of Objects with Canonical Shape. IEEE Trans. Antennas Propag. 2011, 60, 231–239. [Google Scholar] [CrossRef]







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.A.; Volakis, J.L. Real-Time Detection and 3D Localization of Coronary Atherosclerosis Using a Microwave Imaging Technique: A Simulation Study. Sensors 2022, 22, 8822. https://doi.org/10.3390/s22228822
Islam MA, Volakis JL. Real-Time Detection and 3D Localization of Coronary Atherosclerosis Using a Microwave Imaging Technique: A Simulation Study. Sensors. 2022; 22(22):8822. https://doi.org/10.3390/s22228822
Chicago/Turabian StyleIslam, Md Asiful, and John L. Volakis. 2022. "Real-Time Detection and 3D Localization of Coronary Atherosclerosis Using a Microwave Imaging Technique: A Simulation Study" Sensors 22, no. 22: 8822. https://doi.org/10.3390/s22228822