
Development and Evaluation of a Quantitative Fluorescent Lateral Flow Immunoassay for Cystatin-C, a Renal Dysfunction Biomarker



Abstract
:1. Introduction
2. Materials and Methods
2.1. Conjugation of the Alexa fluor 647-mAbs
2.2. Buffer Solutions
2.3. Fabrication of Cystatin-C Lateral Flow Immunoassay Membranes
2.4. Lateral Flow Assay Procedure
2.5. Determining the Limit of Blank (LoB) and Limit of Detection (LoD)
2.6. Recovery
2.7. Stability Test
2.8. ELISA
2.9. Statistical Analysis
3. Results and Discussion
3.1. Principle of the Quantitative Fluorescent Lateral Flow Immunoassay
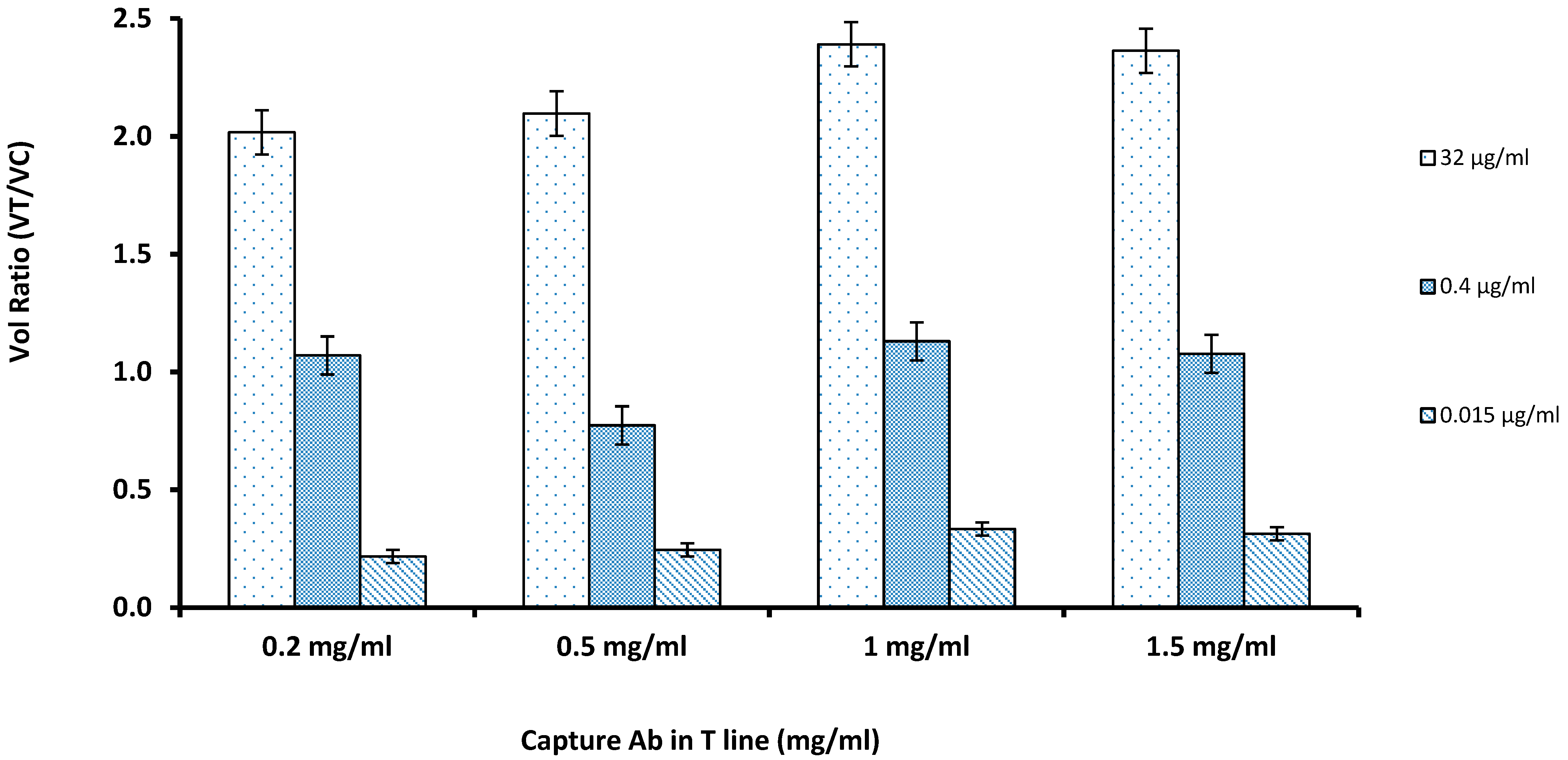
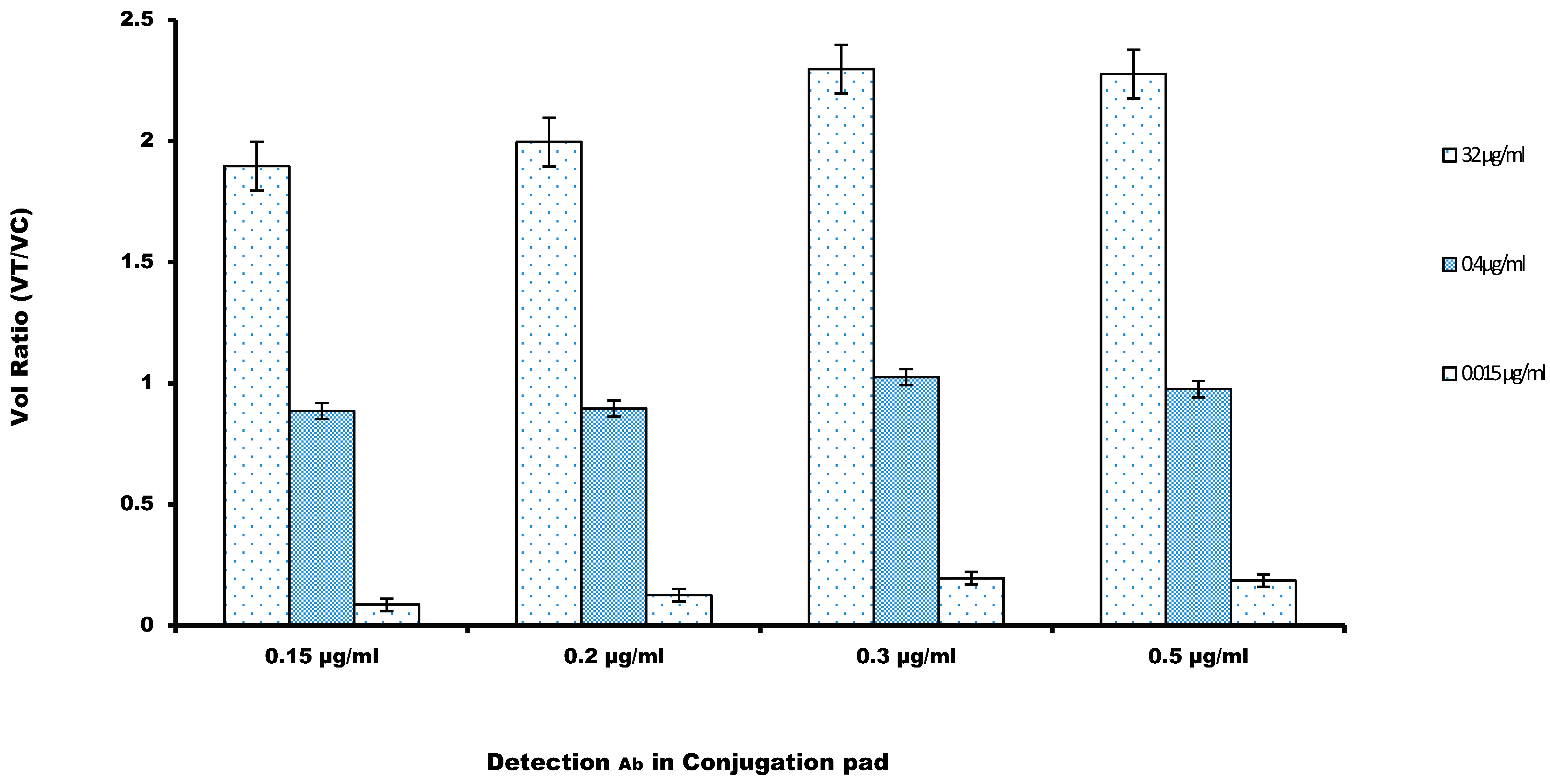
3.2. Optimization of the Parameters for the Lateral Flow Immunoassay
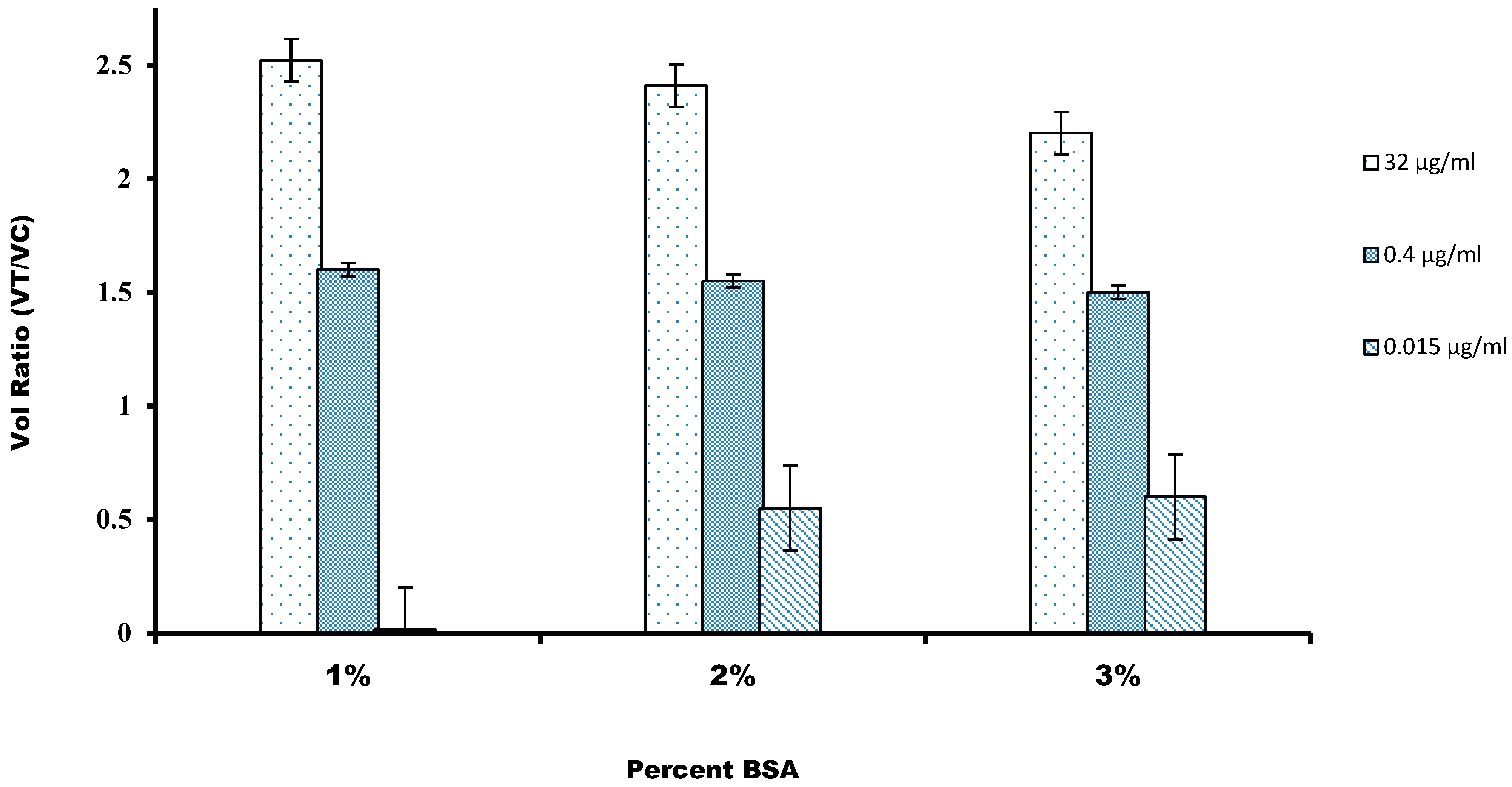
3.3. Effect of Nonspecific Interaction on Assay Quality
3.4. Analytical Validation and Functional Detection Limit
3.5. Precision
3.6. Recovery Study
3.7. Stability
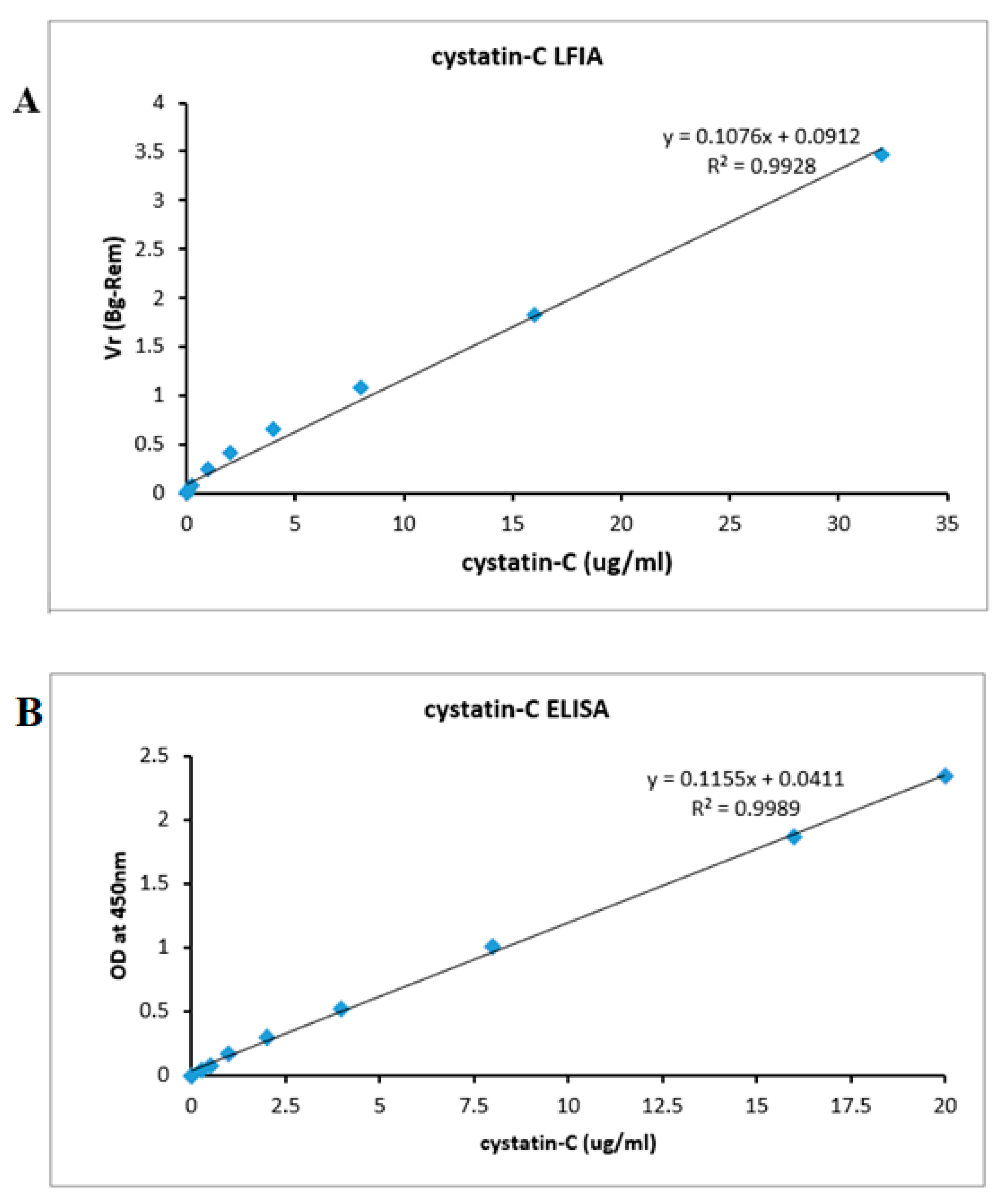
3.8. ELISA
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M. Global, regional, and national burden of chronic kidney disease, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef] [Green Version]
- Biljak, V.R.; Honović, L.; Matica, J.; Krešić, B.; Vojak, S.Š. The role of laboratory testing in detection and classification of chronic kidney disease: National recommendations. Biochem. Med. Biochem. Med. 2017, 27, 153–176. [Google Scholar] [CrossRef]
- Desai, D.; Kumar, A.; Bose, D.; Datta, M. Ultrasensitive sensor for detection of early stage chronic kidney disease in human. Biosens. Bioelectron. 2018, 105, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Ghaderian, S.B.; Beladi-Mousavi, S.S. The role of diabetes mellitus and hypertension in chronic kidney disease. J. Ren. Inj. Prev. 2014, 3, 109. [Google Scholar]
- Jung, K.; Jung, M. Cystatin-C: A promising marker of glomerular filtration rate to replace creatinine. Nephron 1995, 70, 370–371. [Google Scholar] [CrossRef] [PubMed]
- Shinde, A.; Shukla, A.; Juneja, M.; More, R. Comparison of Cystatin-C and creatinine for early detection of contrast induced nephropathy. Indian Heart J. 2015, 67, S123–S124. [Google Scholar] [CrossRef] [Green Version]
- Young, D.S.; Pestaner, L.; Gibberman, V. Effects of drugs on clinical laboratory tests. Clin. Chem. 1975, 21, 1D. [Google Scholar]
- Neild, G.H. Life expectancy with chronic kidney disease: An educational review. Pediatr. Nephrol. 2017, 32, 243–248. [Google Scholar] [CrossRef] [Green Version]
- Roos, J.F.; Doust, J.; Tett, S.E.; Kirkpatrick, C.M. Diagnostic accuracy of cystatin-C compared to serum creatinine for the estimation of renal dysfunction in adults and children—A meta-analysis. Clin. Biochem. 2007, 40, 383–391. [Google Scholar] [CrossRef]
- Dalton, R.N. Serum creatinine and glomerular filtration rate: Perception and reality. Clin. Chem. 2010, 56, 687. [Google Scholar] [CrossRef] [Green Version]
- Bargnoux, A.-S.; Cavalier, E.; Cristol, J.-P.; Simon, N.; Dupuy, A.-M.; Garrigue, V.; Badiou, S.; Delanaye, P.; Mourad, G. Cystatin C is a reliable marker for estimation of glomerular filtration rate in renal transplantation: Validation of a new turbidimetric assay using monospecific sheep antibodies. Clin. Chem. Lab. Med. (CCLM) 2011, 49, 265–270. [Google Scholar] [CrossRef] [Green Version]
- Dieterle, F.; Perentes, E.; Cordier, A.; Roth, D.R.; Verdes, P.; Grenet, O.; Pantano, S.; Moulin, P.; Wahl, D.; Mahl, A. Urinary clusterin, cystatin-C, β2-microglobulin and total protein as markers to detect drug-induced kidney injury. Nat. Biotechnol. 2010, 28, 463. [Google Scholar] [CrossRef] [PubMed]
- Chew, J.S.; Saleem, M.; Florkowski, C.M.; George, P.M. Cystatin-C–A paradigm of evidence based laboratory medicine. Clin. Biochem. Rev. 2008, 29, 47. [Google Scholar] [PubMed]
- Kyhse-Andersen, J.; Schmidt, C.; Nordin, G.; Andersson, B.; Nilsson-Ehle, P.; Lindström, V.; Grubb, A. Serum cystatin-C, determined by a rapid, automated particle-enhanced turbidimetric method, is a better marker than serum creatinine for glomerular filtration rate. Clin. Chem. 1994, 40, 1921–1926. [Google Scholar] [CrossRef] [PubMed]
- Finney, H.; Newman, D.J.; Gruber, W.; Merle, P.; Price, C.P. Initial evaluation of cystatin-C measurement by particle-enhanced immunonephelometry on the Behring nephelometer systems (BNA, BN II). Clin. Chem. 1997, 43, 1016–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Findlay, J.; Smith, W.; Lee, J.; Nordblom, G.; Das, I.; DeSilva, B.; Khan, M.; Bowsher, R. Validation of immunoassays for bioanalysis: A pharmaceutical industry perspective. J. Pharm. Biomed. Anal. 2000, 21, 1249–1273. [Google Scholar] [CrossRef]
- Liu, A.; Yin, K.; Mi, L.; Ma, M.; Liu, Y.; Li, Y.; Wei, W.; Zhang, Y.; Liu, S. A novel photoelectrochemical immunosensor by integration of nanobody and ZnO nanorods for sensitive detection of nucleoside diphosphatase kinase-A. Anal. Chim. Acta 2017, 973, 82–90. [Google Scholar] [CrossRef]
- Lin, H.; Li, L.; Lei, C.; Xu, X.; Nie, Z.; Guo, M.; Huang, Y.; Yao, S. Immune-independent and label-free fluorescent assay for Cystatin-C detection based on protein-stabilized Au nanoclusters. Biosens. Bioelectron. 2013, 41, 256–261. [Google Scholar] [CrossRef]
- Tao, J.; Zhao, P.; Zeng, Q. The determination of cystatin-C in serum based on label-free and near-infrared light emitted PbS BSA QDs. J. Mater. Chem. B 2016, 4, 4258–4262. [Google Scholar] [CrossRef] [PubMed]
- Hawkridge, A.M.; Muddiman, D.C. Mass spectrometry–based biomarker discovery: Toward a global proteome index of individuality. Annu. Rev. Anal. Chem. 2009, 2, 265–277. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Zhang, M.; Dreher, D.D.; Zeng, Y. Ultrasensitive microfluidic solid-phase ELISA using an actuatable microwell-patterned PDMS chip. Lab A Chip 2013, 13, 4190–4197. [Google Scholar] [CrossRef]
- Ouyang, W.; Han, J. Universal amplification-free molecular diagnostics by billion-fold hierarchical nanofluidic concentration. Proc. Natl. Acad. Sci. USA 2019, 116, 16240–16249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouyang, W.; Han, J.; Wang, W. Enabling electrical biomolecular detection in high ionic concentrations and enhancement of the detection limit thereof by coupling a nanofluidic crystal with reconfigurable ion concentration polarization. Lab A Chip 2017, 17, 3772–3784. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, A.I.; Reis, N.M. A critical insight into the development pipeline of microfluidic immunoassay devices for the sensitive quantitation of protein biomarkers at the point of care. Analyst 2017, 142, 858–882. [Google Scholar] [CrossRef] [Green Version]
- Grubb, A.; Horio, M.; Hansson, L.-O.; Björk, J.; Nyman, U.; Flodin, M.; Larsson, A.; Bökenkamp, A.; Yasuda, Y.; Blufpand, H. Generation of a New Cystatin-C–based estimating equation for glomerular filtration rate by use of 7 assays standardized to the international calibrator. Clin. Chem. 2014, 60, 974–986. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.R.; Hu, J.; Tang, R.; Gong, Y.; Feng, S.; Ren, H.; Wen, T.; Li, X.; Abas, W.A.B.W.; Pingguan-Murphy, B. An integrated paper-based sample-to-answer biosensor for nucleic acid testing at the point of care. Lab A Chip 2016, 16, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.; Vasan, J.K.; Shah, M.; Sivaprakasam, M.; Mahajan, L. iQuant™ Analyser: A rapid quantitative immunoassay reader. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju, Korea, 11–15 July 2017; pp. 3732–3736. [Google Scholar]
- Shah, M.I.; Rajagopalan, A.; Joseph, J.; Sivaprakasam, M. An Improved System for Quantitative Immunoassay Measurement in ImageQuant. In Proceedings of the 2018 IEEE SENSORS, New Delhi, India, 28–31 October 2018; pp. 1–4. [Google Scholar]
- Bheemavarapu, L.P.; Shah, M.I.; Joseph, J.; Sivaprakasam, M. Image-based Tracking of Immunoassay Reaction Progress in Quantitative Lateral Flow Kits. In Proceedings of the 2019 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Istanbul, Turkey, 26–28 June 2019; pp. 1–6. [Google Scholar]
- Ramamohan, V.; Chandrasekar, V.; Abbott, J.; Klee, G.G.; Yih, Y. A Monte Carlo approach to the estimation & analysis of uncertainty in clinical laboratory measurement processes. IIE Trans. Healthc. Syst. Eng. 2012, 2, 1–13. [Google Scholar]
- Higgins, C.E.; Neybold, P.; Holdridge, M.B.; Barnes, C.R.; Dong, Y.; Reeve, M.; Mathur, V.; Weisberger, J.; Linder, V. Performance of the 4Kscore test in plasma and serum and stability of the component analytes in clinical samples. J. Appl. Lab. Med. 2018, 3, 185–199. [Google Scholar] [CrossRef] [Green Version]
- Stevens, L.A.; Coresh, J.; Schmid, C.H.; Feldman, H.I.; Froissart, M.; Kusek, J.; Rossert, J.; Van Lente, F.; Bruce III, R.D.; Zhang, Y.L. Estimating GFR using serum cystatin-C alone and in combination with serum creatinine: A pooled analysis of 3,418 individuals with CKD. Am. J. Kidney Dis. 2008, 51, 395–406. [Google Scholar] [CrossRef] [Green Version]
- Finney, H.; Newman, D.J.; Price, C.P. Adult reference ranges for serum cystatin-C, creatinine and predicted creatinine clearance. Ann. Clin. Biochem. 2000, 37, 49–59. [Google Scholar] [CrossRef] [Green Version]
- Glynou, K.; Ioannou, P.C.; Christopoulos, T.K.; Syriopoulou, V. Oligonucleotide-functionalized gold nanoparticles as probes in a dry-reagent strip biosensor for DNA analysis by hybridization. Anal. Chem. 2003, 75, 4155–4160. [Google Scholar] [CrossRef] [PubMed]
- Qie, Z.; Shi, J.; Yan, W.; Gao, Z.; Meng, W.; Xiao, R.; Wang, S. Immunochromatographic assay for T-2 toxin based on luminescent quantum dot beads. RSC Adv. 2019, 9, 38697–38702. [Google Scholar] [CrossRef] [Green Version]
- Jeyachandran, Y.; Mielczarski, J.; Mielczarski, E.; Rai, B. Efficiency of blocking of non-specific interaction of different proteins by BSA adsorbed on hydrophobic and hydrophilic surfaces. J. Colloid Interface Sci. 2010, 341, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Hansson, L.-O.; Grubb, A.; Lidén, A.; Flodin, M.; Berggren, A.; Delanghe, J.; Stove, V.; Luthe, H.; Rhode, K.-H.; Beck, C. Performance evaluation of a turbidimetric cystatin-C assay on different high-throughput platforms. Scand. J. Clin. Lab. Investig. 2010, 70, 347–353. [Google Scholar] [CrossRef]
- Gorodkiewicz, E.; Luszczyn, J. Surface Plasmon Resonance Imaging (SPRI) sensor for cystatin determination based on immobilized papain. Protein Pept. Lett. 2011, 18, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Stephen, B.J.; Desai, D.; Datta, M. An alternative diagnostic design for chronic kidney disease detection based on cystatin-c. Asian J. Pharm. Clin. Res. 2017, 10, 425–429. [Google Scholar]
- Laidler, K.J. The development of the Arrhenius equation. J. Chem. Educ. 1984, 61, 494. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Experimental Condition | Value Tested | Optimal Value |
|---|---|---|
| Capture antibody on T line | 0.2, 0.5, 1, 1.5 mg/ml | 1 mg/mL |
| Detection antibody on conjugation pad | 0.15, 0.2, 0.3, 0.5 µg/mL | 0.3 µg/mL |
| BSA percentage in the running buffer | 3%, 2%, 1% | 1% |
| S.No | Detection Methods | Limit of Detection (µg/mL) | Detection Time (Min) | References |
|---|---|---|---|---|
| 1 | PENIA (Siemens) | 0.53 | 6 | [37] |
| 2 | PETIA (COBAS) | 0.47 | 10 | [37] |
| 3 | PETIA (Genzyme) | 0.61 | 10 | [37] |
| 4 | SPRI sensor | 0.09 | 10 | [38] |
| 5 | SPMWE sensor | 0.006 | 10 | [3] |
| 6 | Fluorescent LFIA | 0.023 | 15 | Present study |
| Sample | Mean | Inter Assay (%CV) | Intra Assay (%CV) | Total | CV% |
|---|---|---|---|---|---|
| 1 | 0.15 | 0.01 | 0.152 | 0.162 | 2.13 |
| 2 | 0.03 | 0.245 | 0.325 | 0.57 | 2.25 |
| 3 | 0.06 | 0.125 | 0.452 | 0.577 | 2.35 |
| 4 | 0.12 | 0.325 | 0.524 | 0.849 | 3.12 |
| 5 | 1 | 0.345 | 0.527 | 0.872 | 3.21 |
| 6 | 2 | 0.345 | 0.538 | 0.883 | 3.41 |
| 7 | 4 | 0.521 | 0.652 | 1.173 | 3.5 |
| 8 | 8 | 0.521 | 0.650 | 1.171 | 3.45 |
| 9 | 16 | 0.510 | 0.649 | 1.159 | 3.46 |
| 10 | 32 | 0.521 | 0.642 | 1.163 | 3.47 |
| Theoretical Concentration (µg/mL) | Measured Concentration (µg/mL) | Recovery (%) |
|---|---|---|
| 0.03 | 0.026 | 92 |
| 1 | 1.37 | 117 |
| 16 | 16.5 | 102 |
| 32 | 32.6 | 105 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Natarajan, S.; DeRosa, M.C.; Shah, M.I.; Jayaraj, J. Development and Evaluation of a Quantitative Fluorescent Lateral Flow Immunoassay for Cystatin-C, a Renal Dysfunction Biomarker. Sensors 2021, 21, 3178. https://doi.org/10.3390/s21093178
Natarajan S, DeRosa MC, Shah MI, Jayaraj J. Development and Evaluation of a Quantitative Fluorescent Lateral Flow Immunoassay for Cystatin-C, a Renal Dysfunction Biomarker. Sensors. 2021; 21(9):3178. https://doi.org/10.3390/s21093178
Chicago/Turabian StyleNatarajan, Satheesh, Maria C. DeRosa, Malay Ilesh Shah, and Joseph Jayaraj. 2021. "Development and Evaluation of a Quantitative Fluorescent Lateral Flow Immunoassay for Cystatin-C, a Renal Dysfunction Biomarker" Sensors 21, no. 9: 3178. https://doi.org/10.3390/s21093178