
A Comprehensive Review of Techniques for Processing and Analyzing Fetal Heart Rate Signals

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
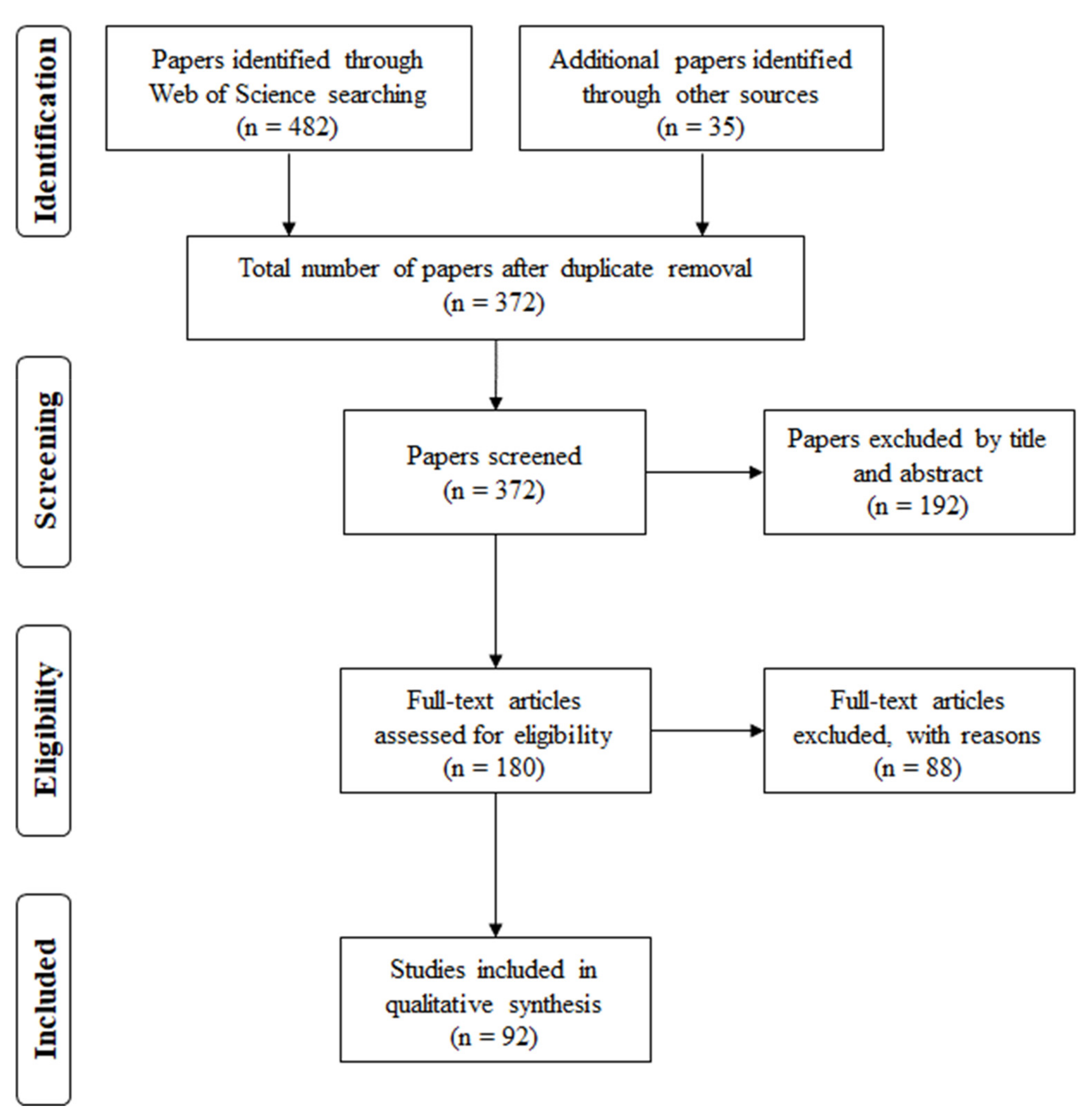
2.1. Eligibility Criteria and Information Sources
- Date of publication not older than 1990;
- Date of publication not newer than 2020;
- Kind of FHR recording and processing technique explicitly cited;
- Details about obtained results clearly reported.
2.2. Search Strategy
- Time domain analysis;
- Frequency domain analysis;
- Fourier Transform, Fast Fourier Transform (FFT), Short Time Fourier Transform (STFT);
- Autoregressive models;
- Wavelet transform (WT);
- Entropy indices;
- Symbolic Dynamics;
- Fractal analysis;
- Detrended Fluctuation Analysis (DFA);
- Poincaré maps;
- Hilbert and Hilbert–Huang transform;
- Complexity of Lempel Ziv (LZ);
- Markov models;
- Lyapunov exponent;
- Lomb method;
- Matching Pursuit (MP).
2.3. Selection Process
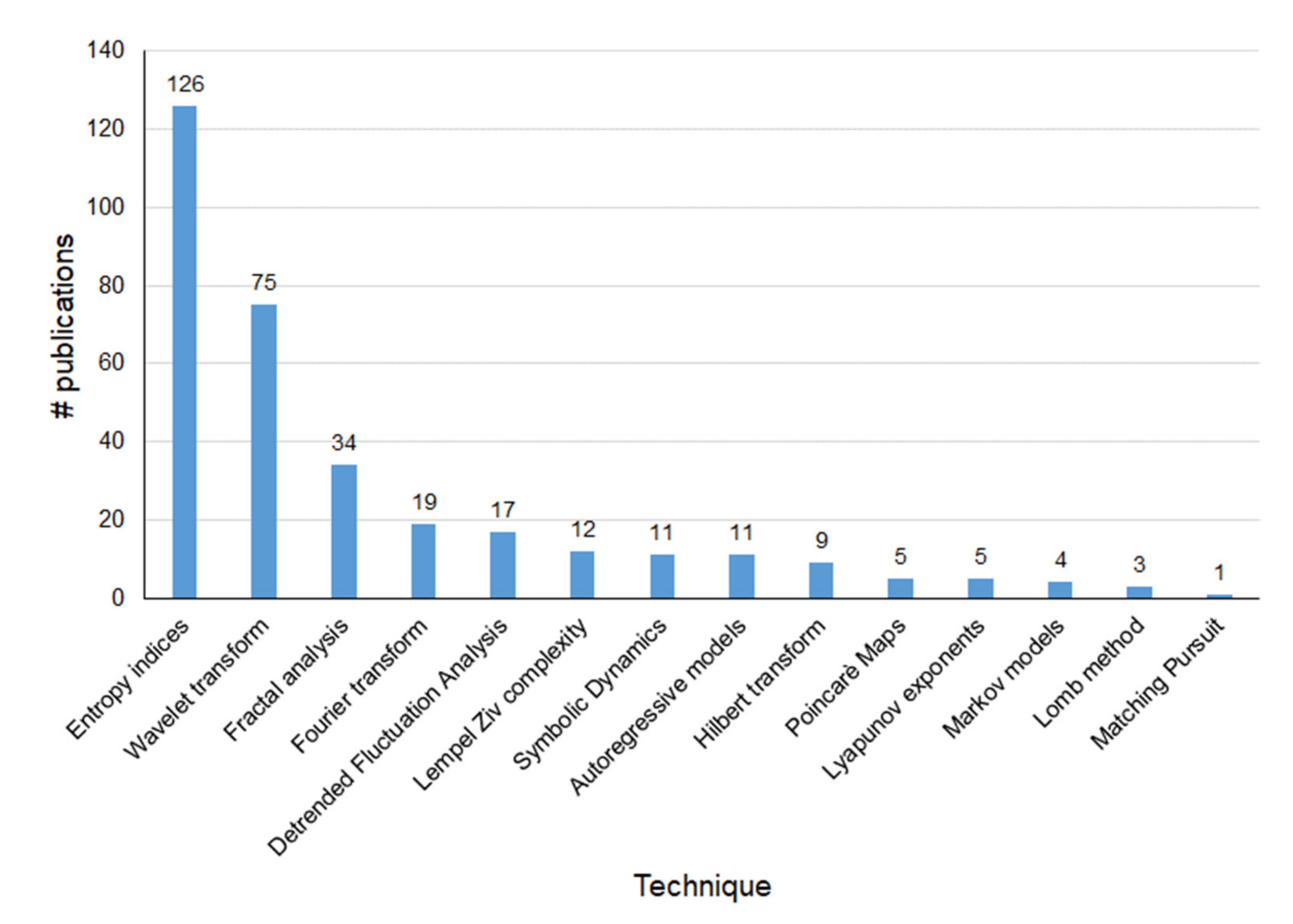
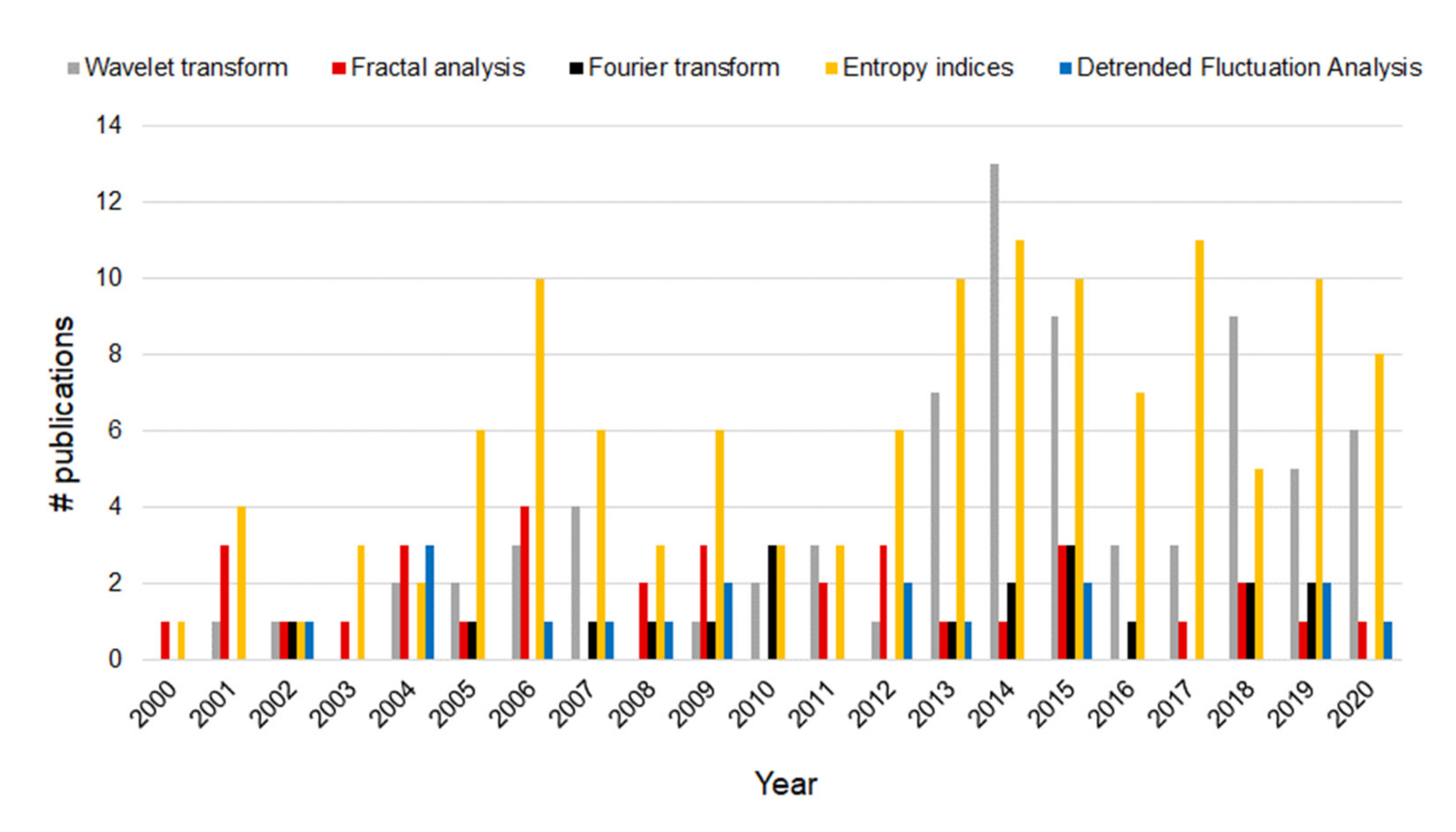
2.4. Characteristics of the Screened Studies
2.5. Characteristics of the Included Studies
3. State of the Art
3.1. Time Domain Indices
3.2. Frequency Domain Analysis
3.2.1. Fast Fourier Transform and Short-Time Fourier Transform
3.2.2. Autoregressive Models
3.2.3. Wavelet Transform
3.3. Nonlinear Techniques
3.3.1. Entropy Measurements
3.3.2. Symbolic Dynamics Analysis
3.3.3. Fractal Analysis
3.3.4. Detrended Fluctuation Analysis
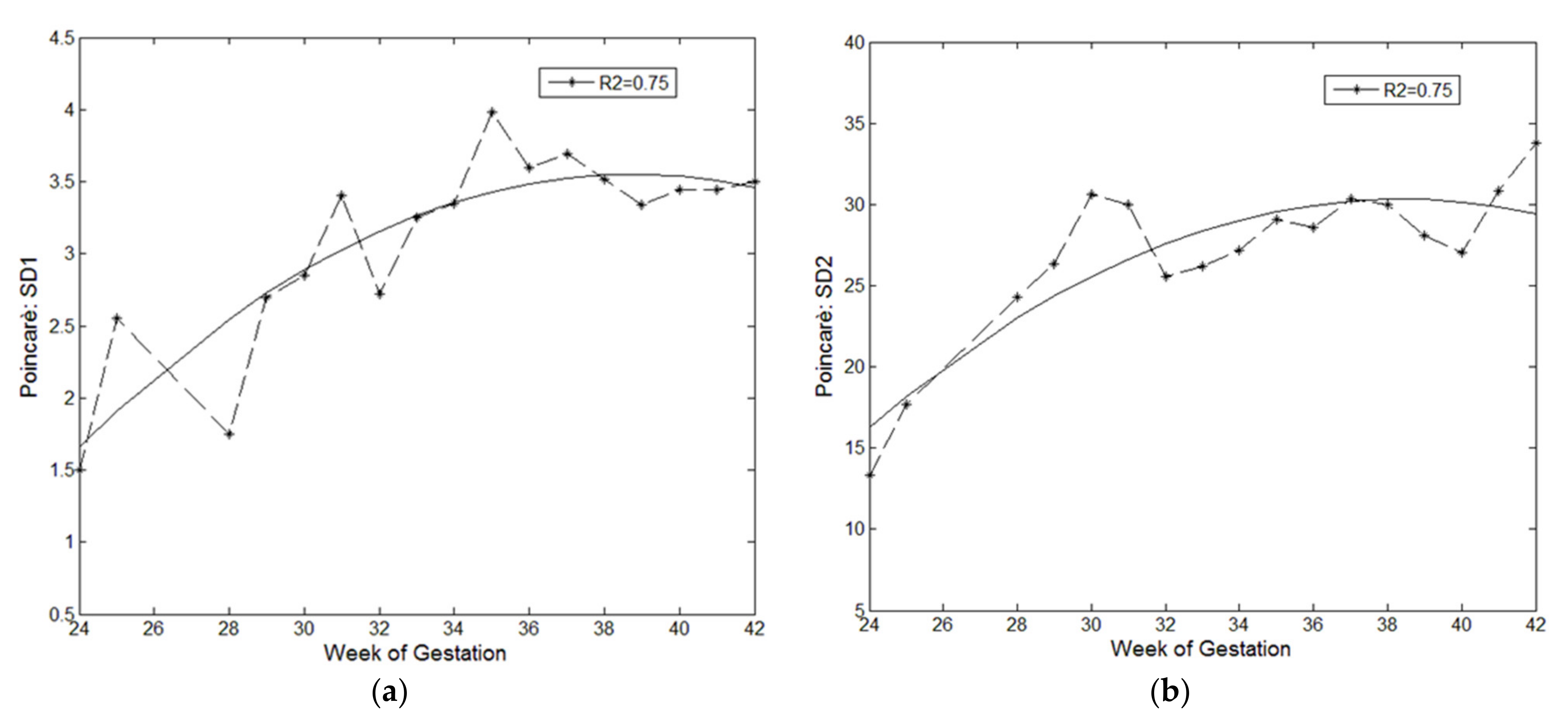
3.3.5. Poincaré Maps
3.3.6. Hypothesis Tests Based on Surrogate Data
- The two series (original and surrogate) are Fourier transformed;
- A random number uniformly distributed between 0 and 2π is generated and added to both phases of the Fourier transforms of the two series to preserve their difference (cross-spectrum);
- The two series are then anti-transformed.
3.3.7. Overview of Advantages and Disadvantages of the Reviewed Techniques
3.4. Other Methods for FHR Analysis
3.4.1. Hilbert and Hilbert–Huang Transform
3.4.2. Lomb Method
3.4.3. Matching Pursuits
3.4.4. Lyapunov Exponents
3.4.5. Hidden Markov Models
3.4.6. Complexity of Lempel Ziv
3.4.7. Principal Dynamic Models
3.5. Artificial Neural Networks for the Classification of FHR Signals
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Abdulhay, E.W.; Oweis, R.J.; Alhaddad, A.M.; Sublaban, F.N.; Radwan, M.A.; Almasaeed, H.M. Review Article: Non-Invasive Fetal Heart Rate Monitoring Techniques. Biomed. Sci. Eng. 2014, 2, 53–67. [Google Scholar] [CrossRef]
- Stylios, C. Methods and Tools for Processing Biosignals: A Survey Paper. In IFMBE Proceedings; Springer: Berlin/Heidelberg, Germany, 2005; Volume 11, pp. 1727–1983. [Google Scholar]
- Lobo Marques, J.A.; Cortez, P.C.; Madeiro, J.P.D.V.; Fong, S.J.; Schlindwein, F.S.; Albuquerque, V.H.C.D. Automatic Cardiotocography Diagnostic System Based on Hilbert Transform and Adaptive Threshold Technique. IEEE Access 2019, 7, 73085–73094. [Google Scholar] [CrossRef]
- Cesarelli, M.; Romano, M.; Bifulco, P.; Improta, G.; D’Addio, G. An Application of Symbolic Dynamics for FHRV Assessment; IOS Press: Amsterdam, The Netherlands, 2012; Volume 180, ISBN 09269630. [Google Scholar]
- Romano, M.; Iuppariello, L.; Ponsiglione, A.M.; Improta, G.; Bifulco, P.; Cesarelli, M. Frequency and Time Domain Analysis of Foetal Heart Rate Variability with Traditional Indexes: A Critical Survey. Comput. Math. Methods Med. 2016, 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oppenheimer, L.W.; Lewinsky, R.M. 7 Power Spectral Analysis of Fetal Heart Rate. Baillières Clin. Obstet. Gynaecol. 1994, 8, 643–661. [Google Scholar] [CrossRef]
- Ayres-de Campos, D.; Bernardes, J.; Garrido, A.; Marques-de-Sá, J.; Pereira-Leite, L. SisPorto 2.0: A Program for Automated Analysis of Cardiotocograms. J. Matern. Fetal Med. 2000, 9, 311–318. [Google Scholar] [CrossRef]
- Czabanski, R.; Jezewski, J.; Matonia, A.; Jezewski, M. Computerized Analysis of Fetal Heart Rate Signals as the Predictor of Neonatal Acidemia. Expert Syst. Appl. 2012, 39, 11846–11860. [Google Scholar] [CrossRef]
- Pardey, J.; Moulden, M.; Redman, C.W.G. A Computer System for the Numerical Analysis of Nonstress Tests. Am. J. Obstet. Gynecol. 2002, 186, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Bifulco, P.; Ruffo, M.; Improta, G.; Clemente, F.; Cesarelli, M. Software for Computerised Analysis of Cardiotocographic Traces. Comput. Methods Programs Biomed. 2016, 124, 121–137. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F. Open-Access Software for Analysis of Fetal Heart Rate Signals. Biomed. Signal Process. Control 2018, 45, 98–108. [Google Scholar] [CrossRef]
- The Dimension of Chaos in the Fetal Heart Rate. Am. J. Obstet. Gynecol. 1991, 165, 1425–1429. [CrossRef]
- Akay, M.; Mulder, E. Examining Fetal Heart-Rate Variability Using Matching Pursuits. IEEE Eng. Med. Biol. Mag. 1996, 15, 64–67. [Google Scholar] [CrossRef]
- Felgueiras, C.S.; Marques de Sá, J.P.; Bernardes, J.; Gama, S. Classification of Foetal Heart Rate Sequences Based on Fractal Features. Med. Biol. Eng. Comput. 1998, 36, 197. [Google Scholar] [CrossRef]
- Hoyer, D.; Heinicke, E.; Jaekel, S.; Tetschke, F.; Di Pietro Paolo, D.; Haueisen, J.; Schleußner, E.; Schneider, U. Indices of Fetal Development Derived from Heart Rate Patterns. Early Hum. Dev. 2009, 85, 379–386. [Google Scholar] [CrossRef]
- Li, X.; Zheng, D.; Zhou, S.; Tang, D.; Wang, C.; Wu, G. Approximate Entropy of Fetal Heart Rate Variability as a Predictor of Fetal Distress in Women at Term Pregnancy. Acta Obstet. Gynecol. Scand. 2005, 84, 837–843. [Google Scholar] [CrossRef] [PubMed]
- Signorini, M.G.; Magenes, G.; Cerutti, S.; Arduini, D. Linear and Nonlinear Parameters for the Analysisof Fetal Heart Rate Signal from Cardiotocographic Recordings. IEEE Trans. Biomed. Eng. 2003, 50, 365–374. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, Z.-Z.; Huang, L.; Fang, M.; Li, B.; Fu, X.; Wang, H.; Zhao, Q. Automatic Classification of Fetal Heart Rate Based on Convolutional Neural Network. IEEE Internet Things J. 2019, 6, 1394–1401. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F. A Study of Artificial Neural Network Training Algorithms for Classification of Cardiotocography Signals. Bitlis Eren Univ. J. Sci. Technol. 2017, 7, 93–103. [Google Scholar] [CrossRef]
- Zhao, Z.; Deng, Y.; Zhang, Y.; Zhang, Y.; Zhang, X.; Shao, L. DeepFHR: Intelligent Prediction of Fetal Acidemia Using Fetal Heart Rate Signals Based on Convolutional Neural Network. BMC Med. Inform. Decis. Mak. 2019, 19, 286. [Google Scholar] [CrossRef] [Green Version]
- Yılmaz, E.; Kılıkçıer, Ç. Determination of Fetal State from Cardiotocogram Using LS-SVM with Particle Swarm Optimization and Binary Decision Tree. Available online: https://www.hindawi.com/journals/cmmm/2013/487179/ (accessed on 6 October 2020).
- Cattani, C.; Doubrovina, O.; Rogosin, S.; Voskresensky, S.L.; Zelianko, E. On the Creation of a New Diagnostic Model for Fetal Well-Being on the Base of Wavelet Analysis of Cardiotocograms. J. Med. Syst. 2006, 30, 489–494. [Google Scholar] [CrossRef]
- Spyridou, K.K.; Hadjileontiadis, L.J. Analysis of Fetal Heart Rate in Healthy and Pathological Pregnancies Using Wavelet-Based Features. In Proceedings of the 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Lyon, France, 22–26 August 2007; pp. 1908–1911. [Google Scholar] [CrossRef]
- Fuentealba, P.; Illanes, A.; Ortmeier, F. Foetal Heart Rate Signal Spectral Analysis by Using Time-Varying Autoregressive Modelling. Curr. Dir. Biomed. Eng. 2018, 4, 579–582. [Google Scholar] [CrossRef]
- Marques, J.L.; Cortez, P.; Madeiro, J.P.V.; Schlindwein, F. Classification System for Fetal Heart Rate Variability Measures Based on Cardiotocographies. J. Life Sci. Technol. 2013. [Google Scholar] [CrossRef]
- Bracale, M.; Romano, M.; Cesarelli, M.; Bifulco, P.; Sansone, M. Cardiotocographic Data Pre-Processing and AR Modelling of Fetal Heart Rate Signals. Available online: /paper/Cardiotocographic-Data-Pre-Processing-and-AR-of-Bracale-Romano/91ce144cb1bd034733fde5670dc669041e83fbf4 (accessed on 31 August 2020).
- Romano, M.; Bifulco, P.; Improta, G.; Faiella, G.; Cesarelli, M.; Fabrizio, C.; D’Addio, G. Symbolic Dynamics in Cardiotocographic Monitoring. In Proceedings of the 2013 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 21–23 November 2013; ISBN ISBN 978-1-4799-2373-1. [Google Scholar]
- Montalvo-Jaramillo, C.I.; Pliego-Carrillo, A.C.; Peña-Castillo, M.Á.; Echeverría, J.C.; Becerril-Villanueva, E.; Pavón, L.; Ayala-Yáñez, R.; González-Camarena, R.; Berg, K.; Wessel, N.; et al. Comparison of Fetal Heart Rate Variability by Symbolic Dynamics at the Third Trimester of Pregnancy and Low-Risk Parturition. Heliyon 2020, 6, e03485. [Google Scholar] [CrossRef] [PubMed]
- Citi, L.; Valenza, G.; Barbieri, R. Instantaneous Estimation of High-Order Nonlinear Heartbeat Dynamics by Lyapunov Exponents. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 13–16. [Google Scholar]
- Saleem, S.; Naqvi, S.S.; Manzoor, T.; Saeed, A.; Rehman, N.; Mirza, J. A Strategy for Classification of “Vaginal vs. Cesarean Section” Delivery: Bivariate Empirical Mode Decomposition of Cardiotocographic Recordings. Front. Physiol. 2019, 10, 246. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [Green Version]
- Falahati, M.; Abbasi, M.; Taheri, F.; Najafi Mojre, M.; Zokaei, M. Common Methods in the Analysis of Heart Rate Variability: A Review Study. Iran Occup. Health 2020, 17, 43. [Google Scholar]
- Holzman, J.B.; Bridgett, D.J. Heart Rate Variability Indices as Bio-Markers of Top-down Self-Regulatory Mechanisms: A Meta-Analytic Review. Neurosci. Biobehav. Rev. 2017, 74, 233–255. [Google Scholar] [CrossRef]
- Pham, T.; Lau, Z.J.; Chen, S.H.A.; Makowski, D. Heart Rate Variability in Psychology: A Review of HRV Indices and an Analysis Tutorial. Sensors 2021, 21, 3998. [Google Scholar] [CrossRef]
- Chiera, M.; Cerritelli, F.; Casini, A.; Barsotti, N.; Boschiero, D.; Cavigioli, F.; Corti, C.G.; Manzotti, A. Heart Rate Variability in the Perinatal Period: A Critical and Conceptual Review. Front. Neurosci. 2020, 14, 561186. [Google Scholar] [CrossRef]
- Cardoso, S.; Silva, M.J.; Guimarães, H. Autonomic Nervous System in Newborns: A Review Based on Heart Rate Variability. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2017, 33, 1053–1063. [Google Scholar] [CrossRef]
- Romano, M.; Bifulco, P.; Ponsiglione, A.M.; Gargiulo, G.D.; Amato, F.; Cesarelli, M. Evaluation of Floatingline and Foetal Heart Rate Variability. Biomed. Signal Process. Control 2018, 39, 185–196. [Google Scholar] [CrossRef]
- Romano, M.; Bracale, M.; Cesarelli, M.; Campanile, M.; Bifulco, P.; De Falco, M.; Sansone, M.; Di Lieto, A. Antepartum Cardiotocography: A Study of Fetal Reactivity in Frequency Domain. Comput. Biol. Med. 2006, 36, 619–633. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Bifulco, P.; Cesarelli, M.; Sansone, M.; Bracale, M. Foetal Heart Rate Power Spectrum Response to Uterine Contraction. Med. Biol. Eng. Comput. 2006, 44, 188–201. [Google Scholar] [CrossRef] [Green Version]
- Schneider, U.; Schleussner, E.; Fiedler, A.; Jaekel, S.; Liehr, M.; Haueisen, J.; Hoyer, D. Fetal Heart Rate Variability Reveals Differential Dynamics in the Intrauterine Development of the Sympathetic and Parasympathetic Branches of the Autonomic Nervous System. Physiol. Meas. 2009, 30, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Cesarelli, M.; Romano, M.; Bifulco, P. Comparison of Short Term Variability Indexes in Cardiotocographic Foetal Monitoring. Comput. Biol. Med. 2009, 39, 106–118. [Google Scholar] [CrossRef]
- Organ, L.W.; Hawrylyshyn, P.A.; Goodwin, J.W.; Milligan, J.E.; Bernstein, A. Quantitative Indices of Short- and Long-Term Heart Rate Variability. Am. J. Obstet. Gynecol. 1978, 130, 20–27. [Google Scholar] [CrossRef]
- Redman, C. SonicaidFetalCare. Clinical Application Guide; Oxford Instruments Medical Ltd.: Abingdon, UK, 2003. [Google Scholar]
- Esposito, F.G.; Tagliaferri, S.; Giudicepietro, A.; Giuliano, N.; Maruotti, G.M.; Saccone, G.; Signorini, M.G.; Magenes, G.; Campanile, M.; Zullo, F. Fetal Heart Rate Monitoring and Neonatal Outcome in a Population of Early- and Late-Onset Intrauterine Growth Restriction. J. Obstet. Gynaecol. Res. 2019, 45, 1343–1351. [Google Scholar] [CrossRef]
- Pels, A.; Mensing van Charante, N.A.; Vollgraff Heidweiller-Schreurs, C.A.; Limpens, J.; Wolf, H.; de Boer, M.A.; Ganzevoort, W. The Prognostic Accuracy of Short Term Variation of Fetal Heart Rate in Early-Onset Fetal Growth Restriction: A Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 234, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Sankhe, M.S.; Desai, K.D.; Gadam, M.A. An Estimate of Fetal Autonomic State by Time Spectral and Nonlinear Analysis of Fetal Heart Rate Variability. Auton. Nerv. Syst. 2016, 1, 3. [Google Scholar]
- Kwon, J.Y.; Park, I.Y.; Shin, J.C.; Song, J.; Tafreshi, R.; Lim, J. Specific Change in Spectral Power of Fetal Heart Rate Variability Related to Fetal Acidemia during Labor: Comparison between Preterm and Term Fetuses. Early Hum. Dev. 2012, 88, 203–207. [Google Scholar] [CrossRef]
- Rantonen, T.; Ekholm, E.; Siira, S.; Metsälä, T.; Leino, R.; Ekblad, U.; Välimäki, I. Periodic Spectral Components of Fetal Heart Rate Variability Reflect the Changes in Cord Arterial Base Deficit Values: A Preliminary Report. Early Hum. Dev. 2001, 60, 233–238. [Google Scholar] [CrossRef]
- Romano, M.; Cesarelli, M.; Bifulco, P.; Sansone, M.; Bracale, M. Study of Fetal Autonomous Nervous System’s Response by Means of FHRV Frequency Analysis. In Proceedings of the First International IEEE EMBS Conference on Neural Engineering, Capri, Italy, 20–22 March 2003; pp. 399–402. [Google Scholar]
- Karin, J.; Hirsch, M.; Sagiv, C.; Akselrod, S. Fetal Autonomic Nervous System Activity Monitoring by Spectral Analysis of Heart Rate Variations. In Proceedings of the Proceedings Computers in Cardiology, Durham, NC, USA, 11–14 October 1992; pp. 479–482. [Google Scholar]
- Van Laar, J.O.E.H.; Peters, C.H.L.; Vullings, R.; Houterman, S.; Oei, S.G. Power Spectrum Analysis of Fetal Heart Rate Variability at near Term and Post Term Gestation during Active Sleep and Quiet Sleep. Early Hum. Dev. 2009, 85, 795–798. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F.; Subha, V. Prognostic Model Based on Image-Based Time-Frequency Features and Genetic Algorithm for Fetal Hypoxia Assessment. Comput. Biol. Med. 2018, 99, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Ansourian, M.N.; Dripps, J.H.; Beattie, G.J.; Boddy, K. Autoregressive Spectral Estimation of Fetal Breathing Movement. IEEE Trans. Biomed. Eng. 1989, 36, 1076–1084. [Google Scholar] [CrossRef]
- Cazares, S.; Moulden, M.; Redman, W.G.; Tarassenko, L. Tracking Poles with an Autoregressive Model: A Confidence Index for the Analysis of the Intrapartum Cardiotocogram. Med. Eng. Phys. 2001, 23, 603–614. [Google Scholar] [CrossRef]
- Vasios, G.; Prentza, A.; Blana, D.; Salamalekis, E.; Thomopoulos, P.; Giannaris, D.; Koutsouris, D. Classification of Fetal Heart Rate Tracings Based on Wavelet-Transform and Self-Organizing-Map Neural Networks. In Proceedings of the 2001 Conference Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istanbul, Turkey, 25–28 October 2001. [Google Scholar] [CrossRef]
- Salamalekis, E.; Thomopoulos, P.; Giannaris, D.; Salloum, I.; Vasios, G.; Prentza, A.; Koutsouris, D. Computerised Intrapartum Diagnosis of Fetal Hypoxia Based on Fetal Heart Rate Monitoring and Fetal Pulse Oximetry Recordings Utilising Wavelet Analysis and Neural Networks. BJOG Int. J. Obstet. Gynaecol. 2002, 109, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Cömert, Z.; Kocamaz, A.F. Evaluation of Fetal Distress Diagnosis during Delivery Stages Based on Linear and Nonlinear Features of Fetal Heart Rate for Neural Network Community. Int. J. Comput. Appl. 2016, 156, 26–31. [Google Scholar] [CrossRef]
- Gonçalves, H.; Amorim-Costa, C.; Ayres-de-Campos, D.; Bernardes, J. Evolution of Linear and Nonlinear Fetal Heart Rate Indices throughout Pregnancy in Appropriate, Small for Gestational Age and Preterm Fetuses: A Cohort Study. Comput. Methods Programs Biomed. 2018, 153, 191–199. [Google Scholar] [CrossRef]
- Gonçalves, H.; Rocha, A.P.; Ayres-de-Campos, D.; Bernardes, J. Linear and Nonlinear Fetal Heart Rate Analysis of Normal and Acidemic Fetuses in the Minutes Preceding Delivery. Med. Biol. Eng. Comput. 2006, 44, 847. [Google Scholar] [CrossRef]
- Magenes, G.; Pedrinazzi, L.; Signorini, M.G. Identification of Fetal Sufferance Antepartum through a Multiparametric Analysis and a Support Vector Machine. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; Volume 1, pp. 462–465. [Google Scholar]
- Cysarz, D.; Van Leeuwen, P.; Bettermann, H. Irregularities and Nonlinearities in Fetal Heart Period Time Series in the Course of Pregnancy. Herzschrittmacherther. Elektrophysiol. 2000, 11, 179–183. [Google Scholar] [CrossRef]
- Lim, J.; Kwon, J.Y.; Song, J.; Choi, H.; Shin, J.C.; Park, I.Y. Quantitative Comparison of Entropy Analysis of Fetal Heart Rate Variability Related to the Different Stages of Labor. Early Hum. Dev. 2014, 90, 81–85. [Google Scholar] [CrossRef]
- Pincus, S.M.; Gladstone, I.M.; Ehrenkranz, R.A. A Regularity Statistic for Medical Data Analysis. J. Clin. Monit. 1991, 7, 335–345. [Google Scholar] [CrossRef]
- Moraes, E.R.; Murta, L.O.; Baffa, O.; Wakai, R.T.; Comani, S. Linear and Nonlinear Measures of Fetal Heart Rate Patterns Evaluated on Very Short Fetal Magnetocardiograms. Physiol. Meas. 2012, 33, 1563–1583. [Google Scholar] [CrossRef]
- Gonçalves, H.; Bernardes, J.; Paula Rocha, A.; Ayres-de-Campos, D. Linear and Nonlinear Analysis of Heart Rate Patterns Associated with Fetal Behavioral States in the Antepartum Period. Early Hum. Dev. 2007, 83, 585–591. [Google Scholar] [CrossRef]
- Van Leeuwen, P.; Cysarz, D.; Bettermann, H. Presence of Irregularity in Fetal Heart Period Time Series. Med. Biol. Eng. Comput. 1999, 37, 2. [Google Scholar]
- Ferrario, M.; Signorini, M.G.; Magenes, G.; Cerutti, S. Comparison of Entropy-Based Regularity Estimators: Application to the Fetal Heart Rate Signal for the Identification of Fetal Distress. IEEE Trans. Biomed. Eng. 2006, 53, 119–125. [Google Scholar] [CrossRef]
- Padhye, N.S.; Brazdeikis, A.; Verklan, M.T. Change in Complexity of Fetal Heart Rate Variability. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 1796–1798. [Google Scholar]
- Khandoker, A.H.; Schulz, S.; Kimura, Y.; Palaniswami, M.; Voss, A. Investigating Maternal-Fetal Heart Rate Coupling by High Resolution Joint Symbolic Dynamics. In Proceedings of the Computing in Cardiology 2014, Cambridge, MA, USA, 7–10 September 2014; pp. 441–444. [Google Scholar]
- Van Leeuwen, P.; Cysarz, D.; Lange, S.; Geue, D.; Groenemeyer, D. Quantification of Fetal Heart Rate Regularity Using Symbolic Dynamics. Chaos Interdiscip. J. Nonlinear Sci. 2007, 17, 015119. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; D’Addio, G.; Clemente, F.; Ponsiglione, A.M.; Improta, G.; Cesarelli, M. Symbolic Dynamic and Frequency Analysis in Foetal Monitoring. In Proceedings of the 2014 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Lisbon, Portugal, 11–12 June 2014; pp. 1–5. [Google Scholar]
- Cesarelli, M.; Romano, M.; Bifulco, P.; Improta, G.; D’Addio, G. Prognostic decision support using symbolic dynamics in CTG monitoring. In Proceeding of the 13th EFMI Special Topic Conference: Data and Knowledge for Medical Decision Support, EFMI STC 2013; IOS Press: Amsterdam, The Netherlands, 2013; Volume 186, pp. 140–144. ISBN 978-1-61499-239-4. [Google Scholar]
- Hoyer, D.; Schneider, U.; Kowalski, E.-M.; Schmidt, A.; Witte, O.W.; Schleußner, E.; Hatzmann, W.; Grönemeyer, D.H.; van Leeuwen, P. Validation of Functional Fetal Autonomic Brain Age Score FABAS in 5\hspace0.167emmin Short Recordings. Physiol. Meas. 2015, 36, 2369–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renzo, G.C.D.; Montani, M.; Fioriti, V.; Clerici, G.; Branconi, F.; Pardini, A.; Indraccolo, R.; Cosmi, E.V. Fractal Analysis: A New Method for Evaluating Fetal Heart Rate Variability. J. Perinat. Med. 1996, 24, 261–269. [Google Scholar] [CrossRef]
- Hopkins, P.; Sneyd, R.; Outram, N.; Rosén, K.; Ifeachor, E. Suitability of Fractal Dimension Analysis of Foetal Heart Rate as an Indicator for Asphyxia. In Proceedings of the International Conference on Computational Intelligence in Medicine and Healthcare (CIMED2005), Lisbon, Portugal, 29 June–1 July 2005; Volume 2, pp. 480–485. [Google Scholar]
- Echeverría, J.C.; Woolfson, M.S.; Crowe, J.A.; Hayes-Gill, B.R.; Piéri, J.F.; Spencer, C.J.; James, D.K. Does Fractality in Heart Rate Variability Indicate the Development of Fetal Neural Processes? Phys. Lett. A 2004, 331, 225–230. [Google Scholar] [CrossRef]
- Morren, G.; Lemmerling, P.; Daniels, H.; Naulaers, G.; Van Huffel, S. Sensitivity of Detrended Fluctuation Analysis Applied to Heart Rate Variability of Preterm Newborns. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2005; pp. 319–322. [Google Scholar]
- Echeverría, J.C.; Hayes-Gill, B.R.; Crowe, J.A.; Woolfson, M.S.; Croaker, G.D.H. Detrended Fluctuation Analysis: A Suitable Method for Studying Fetal Heart Rate Variability? Physiol. Meas. 2004, 25, 763–774. [Google Scholar] [CrossRef]
- Mooney, D.M.; Groome, L.J.; Bentz, L.S.; Holland, S. Poincare Analysis of Fetal Heart Rate Pattern: Effect of Observation Period. In Proceedings of the 17th International Conference of the Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–23 September 1995; Volume 2, pp. 1471–1472. [Google Scholar]
- Taralunga, D.D.; Tautan, A.M.; Ungureanu, G.M. An Efficient Method for Fetal Heart Sounds Detection Based on Hilbert Transform. In Proceedings of the 2018 International Conference and Exposition on Electrical and Power Engineering (EPE), Iasi, Romania, 18–19 October 2018; pp. 0916–0919. [Google Scholar]
- Yacin, S.M.; Vennila, M. Analysis of Foetal Electrocardiogram Extraction Methods and Enhancement Using Hilbert-Huang Transform. Int. J. Biomed. Eng. Technol. 2015, 18, 14–29. [Google Scholar] [CrossRef]
- Computerized Cardiotocography Analysis System Based on Hilbert Transform. Available online: https://www.researchgate.net/publication/234036154_Computerized_Cardiotocography_Analysis_System_based_on_Hilbert_Transform (accessed on 1 September 2021).
- Cesarelli, M.; Romano, M.; Ruffo, M.; Bifulco, P.; Pasquariello, G.; Fratini, A. PSD Modifications of FHRV Due to Interpolation and CTG Storage Rate. Biomed. Signal Process. Control 2011, 6, 225–230. [Google Scholar] [CrossRef]
- Cao, H.; Lake, D.E.; Ferguson, J.E.; Chisholm, C.A.; Griffin, M.P.; Moorman, J.R. Toward Quantitative Fetal Heart Rate Monitoring. IEEE Trans. Biomed. Eng. 2006, 53, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.; Cesarelli, M.; Bifulco, P.; Ruffo, M.; Fratini, A.; Pasquariello, G. Time-Frequency Analysis of CTG Signals. Available online: https://www.semanticscholar.org/paper/Time-frequency-analysis-of-CTG-signals-Romano-Cesarelli/07a0bd05e28d1bf82744c082d3553505f271b64a (accessed on 20 February 2021).
- Professor, E.S.A.; Hintipas, E.; Salloum, I.; Vasios, G.; Loghis, C.; Vitoratos, N.; Chrelias, C.; Creatsas, G. Computerized Analysis of Fetal Heart Rate Variability Using the Matching Pursuit Technique as an Indicator of Fetal Hypoxia during Labor. J. Matern. Fetal Neonatal Med. 2006, 19, 165–169. [Google Scholar] [CrossRef]
- Van Leeuwen, P.; Lange, S.; Bettermann, H.; Grönemeyer, D.; Hatzmann, W. Fetal Heart Rate Variability and Complexity in the Course of Pregnancy. Early Hum. Dev. 1999, 54, 259–269. [Google Scholar] [CrossRef]
- Kikuchi, A.; Shimizu, T.; Hayashi, A.; Horikoshi, T.; Unno, N.; Kozuma, S.; Taketani, Y. Nonlinear Analyses of Heart Rate Variability in Normal and Growth-Restricted Fetuses. Early Hum. Dev. 2006, 82, 217–226. [Google Scholar] [CrossRef]
- Georgoulas, G.G.; Stylios, C.D.; Nokas, G.; Groumpos, P.P. Classification of Fetal Heart Rate during Labour Using Hidden Markov Models. In Proceedings of the 2004 IEEE International Joint Conference on Neural Networks (IEEE Cat. No.04CH37541), Budapest, Hungary, 25–29 July 2004; Volume 3, pp. 2471–2475. [Google Scholar]
- Ferrario, M.; Signorini, M.G.; Magenes, G. Complexity Analysis of the Fetal Heart Rate Variability: Early Identification of Severe Intrauterine Growth-Restricted Fetuses. Med. Biol. Eng. Comput. 2009, 47, 911–919. [Google Scholar] [CrossRef] [Green Version]
- Ferrario, M.; Signorini, M.G.; Magenes, G. Complexity Analysis of the Fetal Heart Rate for the Identification of Pathology in Fetuses. In Proceedings of the Computers in Cardiology, Lyon, France, 25–28 September 2005; pp. 989–992. [Google Scholar]
- Magenes, G.; Bellazzi, R.; Fanelli, A.; Signorini, M.G. Multivariate Analysis Based on Linear and Non-Linear FHR Parameters for the Identification of IUGR Fetuses. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 1868–1871. [Google Scholar]
- Marques de Sa, J.P.; Reis, L.P.; Lau, J.N.; Bernardes, J. Estimation and Classification of Fetal Heart Rate Baselines Using Artificial Neural Networks. In Proceedings of the Computers in Cardiology 1994, Bethesda, MD, USA, 25–28 September 1994; pp. 541–544. [Google Scholar]
- Liszka-Hackzell, J.J. Categorization of Fetal Heart Rate Patterns Using Neural Networks. J. Med. Syst. 2001, 25, 269–276. [Google Scholar] [CrossRef]
- Kol, S.; Thaler, I.; Paz, N.; Shmueli, O. Interpretation of Nonstress Tests by an Artificial Neural Network. Am. J. Obstet. Gynecol. 1995, 172, 1372–1379. [Google Scholar] [CrossRef]
- Devoe, L.D.; Carlton, E.; Prescott, P. Neural Network Prediction of Nonstress Test Results: How Often Should We Perform Nonstress Tests? Am. J. Obstet. Gynecol. 1995, 173, 1128–1131. [Google Scholar] [CrossRef]
- Magenes, G.; Signorini, M.G.; Arduini, D. Classification of Cardiotocographic Records by Neural Networks. In Proceedings of the IEEE-INNS-ENNS International Joint Conference on Neural Networks. IJCNN 2000. Neural Computing: New Challenges and Perspectives for the New Millennium, Como, Italy, 27 July 2000; Volume 3, pp. 637–641. [Google Scholar]
- Jadhav, S.; Nalbalwar, S.; Ghatol, A. Modular Neural Network Model Based Foetal State Classification. In Proceedings of the 2011 IEEE International Conference on Bioinformatics and Biomedicine Workshops (BIBMW), Atlanta, GA, USA, 12–15 November 2011; pp. 915–917. [Google Scholar]
- Sundar, C.; Chitradevi, M.; Geetharamani, G. Classification of Cardiotocogram Data Using Neural Network Based Machine Learning Technique. Int. J. Comput. Appl. 2012, 47, 19–25. [Google Scholar]
- Huang, M.-L.; Hsu, Y.-Y. Fetal Distress Prediction Using Discriminant Analysis, Decision Tree, and Artificial Neural Network. J. Biomed. Sci. Eng. 2012, 5, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Yılmaz, E. Fetal State Assessment from Cardiotocogram Data Using Artificial Neural Networks. J. Med. Biol. Eng. 2016, 36, 820–832. [Google Scholar] [CrossRef]
- Cömert, Z.; Kocamaz, A.F. Comparison of Machine Learning Techniques for Fetal Heart Rate Classification. Acta Physica Polonica A 2017, 132, 451–454. [Google Scholar] [CrossRef]
- Tang, H.; Wang, T.; Li, M.; Yang, X. The Design and Implementation of Cardiotocography Signals Classification Algorithm Based on Neural Network. Available online: https://www.hindawi.com/journals/cmmm/2018/8568617/ (accessed on 20 February 2021).
- Amin, B.; Gamal, M.; Salama, A.A.; El-Henawy, I.M.; Mahfouz, K. Classifying Cardiotocography Data Based on Rough Neural Network. Int. J. Adv. Comput. Sci. Appl. IJACSA 2019, 10. [Google Scholar] [CrossRef]
- Improta, G.; Faiella, G.; Romano, M.; Bifulco, P.; Clemente, F.; Cesarelli, M. Power Spectral Analysis of Foetal Heart Rate Variability. In Proceedings of the GNB 2014-IV Congresso Nazionale di Bioingegneria, Pavia, Italy, 25–27 June 2014. [Google Scholar]
- Ayres-de-Campos, D.; Spong, C.Y.; Chandraharan, E. FIGO Consensus Guidelines on Intrapartum Fetal Monitoring: Cardiotocography. Int. J. Gynecol. Obstet. 2015, 131, 13–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rooth, G.; Huch, A.; Huch, R. Guidelines for the Use of Fetal Monitoring. FIGO News. Int. J. Gynecol. Obstet. 1987, 25, 159–167. [Google Scholar]
- RCOG. The Use of Electronic Fetal Monitoring: The Use and Interpretation of Cardiotocography in Intrapartum Fetal Surveillance: 8; RCOG Press: London, UK, 2001; ISBN 978-1-900364-49-2. [Google Scholar]
- NCC. National Certification Corporation NICHD Definitions and Classifications: Application to Electronic Fetal Monitoring Interpretation; NCC Monograph: Chicago, IL, USA, 2010; Volume 3. [Google Scholar]
- Shibata, R. Selection of the Order of an Autoregressive Model by Akaike’s Information Criterion. Biometrika 1976, 63, 117–126. [Google Scholar] [CrossRef]
- Tzabazis, A.; Eisenried, A.; Yeomans, D.C.; Hyatt, M.I. Wavelet Analysis of Heart Rate Variability: Impact of Wavelet Selection. Biomed. Signal Process. Control 2018, 40, 220–225. [Google Scholar] [CrossRef]
- Li, K.; Rüdiger, H.; Ziemssen, T. Spectral Analysis of Heart Rate Variability: Time Window Matters. Front. Neurol. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Rangayyan, R.M. Biomedical Signal Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2015; ISBN 978-1-119-06793-1. [Google Scholar]
- Groome, L.J.; Mooney, D.M.; Holland, S.B.; Smith, L.A.; Atterbury, J.L.; Loizou, P.C. Human Fetuses Have Nonlinear Cardiac Dynamics. J. Appl. Physiol. 1999, 87, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Billman, G.E. The LF/HF Ratio Does Not Accurately Measure Cardiac Sympatho-Vagal Balance. Front. Physiol. 2013, 4, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germán-Salló, Z.; Germán-Salló, M. Non-Linear Methods in HRV Analysis. Procedia Technol. 2016, 22, 645–651. [Google Scholar] [CrossRef] [Green Version]
- Bartels, R.; Peçanha, T. HRV: A Pythonic Package for Heart Rate Variability Analysis. J. Open Source Softw. 2020, 5, 1867. [Google Scholar] [CrossRef]
- Van Leeuwen, P.; Bettermann, H. The Status of Nonlinear Dynamics in the Analysis of Heart Rate Variability. Herzschrittmacherther. Elektrophysiol. 2000, 11, 127–130. [Google Scholar] [CrossRef]
- Garner, D.; Souza, N.; Vanderlei, L. Unreliability of Approximate Entropy to Locate Optimal Complexity in Diabetes Mellitus via Heart Rate Variability. Ser. Endocrinol. Diabetes Metab. 2020, 2, 32–40. [Google Scholar]
- Cysarz, D.; Lange, S.; Matthiessen, P.F.; van Leeuwen, P. Regular Heartbeat Dynamics Are Associated with Cardiac Health. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2007, 292, R368–R372. [Google Scholar] [CrossRef]
- Pincus, S.M.; Goldberger, A.L. Physiological Time-Series Analysis: What Does Regularity Quantify? Am. J. Physiol.-Heart Circ. Physiol. 1994, 266, H1643–H1656. [Google Scholar] [CrossRef]
- Wessel, N.; Schumann, A.; Schirdewan, A.; Voss, A.; Kurths, J. Entropy Measures in Heart Rate Variability Data. In Medical Data Analysis; Brause, R.W., Hanisch, E., Eds.; Springer: Berlin/Heidelberg, Germany, 2000; pp. 78–87. [Google Scholar]
- Richman, J.S.; Moorman, J.R. Physiological Time-Series Analysis Using Approximate Entropy and Sample Entropy. Am. J. Physiol.-Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, K.K.; Moody, G.B.; Peng, C.K.; Mietus, J.E.; Larson, M.G.; Levy, D.; Goldberger, A.L. Predicting Survival in Heart Failure Case and Control Subjects by Use of Fully Automated Methods for Deriving Nonlinear and Conventional Indices of Heart Rate Dynamics. Circulation 1997, 96, 842–848. [Google Scholar] [CrossRef]
- Li, P.; Liu, C.; Li, K.; Zheng, D.; Liu, C.; Hou, Y. Assessing the Complexity of Short-Term Heartbeat Interval Series by Distribution Entropy. Med. Biol. Eng. Comput. 2015, 53, 77–87. [Google Scholar] [CrossRef]
- Lake, D.E.; Richman, J.S.; Griffin, M.P.; Moorman, J.R. Sample Entropy Analysis of Neonatal Heart Rate Variability. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2002, 283, R789–R797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cysarz, D.; Van Leeuwen, P.; Edelhäuser, F.; Montano, N.; Porta, A. Binary Symbolic Dynamics Classifies Heart Rate Variability Patterns Linked to Autonomic Modulations. Comput. Biol. Med. 2012, 42, 313–318. [Google Scholar] [CrossRef]
- Yao, W.; Wang, J. Double Symbolic Joint Entropy in Nonlinear Dynamic Complexity Analysis. AIP Adv. 2017, 7, 075313. [Google Scholar] [CrossRef] [Green Version]
- D’Addio, G.; Romano, M.; Maestri, R.; Bifulco, P.; Cesarelli, M. Indices of Symbolic Dynamic Distribution in Cardiac Patients. In Proceedings of the Computing in Cardiology 2013, Zaragoza, Spain, 22–25 September 2013; pp. 437–440. [Google Scholar]
- Voss, A.; Schulz, S.; Schroeder, R.; Baumert, M.; Caminal, P. Methods Derived from Nonlinear Dynamics for Analysing Heart Rate Variability. Philos. Trans. R. Soc. Math. Phys. Eng. Sci. 2009, 367, 277–296. [Google Scholar] [CrossRef]
- Li, C.; Tang, D.-K.; Zheng, D.-A.; Ding, G.-H.; Poon, C.-S.; Wu, G.-Q. Comparison of Nonlinear Indices in Analyses of Heart Rate Variability. In Proceedings of the 2008 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Vancouver, BC, Canada, 20–25 August 2008; pp. 2145–2148. [Google Scholar]
- Sassi, R.; Cerutti, S.; Lombardi, F.; Malik, M.; Huikuri, H.V.; Peng, C.-K.; Schmidt, G.; Yamamoto, Y.; Gorenek, B.; Lip, G.Y.; et al. Advances in Heart Rate Variability Signal Analysis: Joint Position Statement by the e-Cardiology ESC Working Group and the European Heart Rhythm Association Co-Endorsed by the Asia Pacific Heart Rhythm Society. EP Eur. 2015, 17, 1341–1353. [Google Scholar] [CrossRef]
- Penzel, T.; Kantelhardt, J.W.; Grote, L.; Peter, J.H.; Bunde, A. Comparison of Detrended Fluctuation Analysis and Spectral Analysis for Heart Rate Variability in Sleep and Sleep Apnea. IEEE Trans. Biomed. Eng. 2003, 50, 1143–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, R.-G.; Shieh, J.-S.; Han, Y.-Y.; Wang, Y.-J.; Tseng, S.-C. Detrended Fluctuation Analyses of Short-Term Heart Rate Variability in Surgical Intensive Care Units. Biomed. Eng. Appl. Basis Commun. 2006, 18, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Almeida, D.L.F.; Soares, F.A.; Carvalho, J.L.A. A Sliding Window Approach to Detrended Fluctuation Analysis of Heart Rate Variability. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 3278–3281. [Google Scholar] [CrossRef]
- Bilchick, K.C.; Berger, R.D. Heart Rate Variability. J. Cardiovasc. Electrophysiol. 2006, 17, 691–694. [Google Scholar] [CrossRef]
- Castiglioni, P.; Faini, A. A Fast DFA Algorithm for Multifractal Multiscale Analysis of Physiological Time Series. Front. Physiol. 2019, 10, 115. [Google Scholar] [CrossRef] [Green Version]
- Tayel, M.B.; AlSaba, E.I. Poincaré Plot for Heart Rate Variability. Int. J. Biomed. Biol. Eng. 2015, 9, 708–711. [Google Scholar]
- D’Addio, G.; Pinna, G.D.; Maestri, R.; Corbi, G.; Ferrara, N.; Rengo, F. Quantitative Poincare Plots Analysis Contains Relevant Information Related to Heart Rate Variability Dynamics of Normal and Pathological Subjects. In Proceedings of the Computers in Cardiology, Chicago, IL, USA, 19–22 September 2004; pp. 457–460. [Google Scholar]
- D’Addio, G.; Accardo, A.; Corbi, G.; Russo, G.; Pinna, G.D.; Ferrara, N.; Rengo, F. Effects of Stroke Localization on Nonlinear Indexes of HRV. In Proceedings of the 2006 Computers in Cardiology, Valencia, Spain, 17–20 September 2006; pp. 621–624. [Google Scholar]
- Fishman, M.; Jacono, F.J.; Park, S.; Jamasebi, R.; Thungtong, A.; Loparo, K.A.; Dick, T.E. A Method for Analyzing Temporal Patterns of Variability of a Time Series from Poincaré Plots. J. Appl. Physiol. 2012, 113, 297–306. [Google Scholar] [CrossRef] [Green Version]
- Theiler, J.; Eubank, S.; Longtin, A.; Galdrikian, B.; Doyne Farmer, J. Testing for Nonlinearity in Time Series: The Method of Surrogate Data. Phys. Nonlinear Phenom. 1992, 58, 77–94. [Google Scholar] [CrossRef] [Green Version]
- Porta, A.; Guzzetti, S.; Furlan, R.; Gnecchi-Ruscone, T.; Montano, N.; Malliani, A. Complexity and Nonlinearity in Short-Term Heart Period Variability: Comparison of Methods Based on Local Nonlinear Prediction. IEEE Trans. Biomed. Eng. 2007, 54, 94–106. [Google Scholar] [CrossRef]
- Ma, Y.; Wu, C.-W.; Peng, C.-K.; Ahn, A.; Bertisch, S.M.; Lipsitz, L.A.; Yeh, G.Y.; Manor, B.; Novak, V.; Hausdorff, J.M.; et al. Complexity-Based Measures of Heart Rate Dynamics in Older Adults Following Long- and Short-Term Tai Chi Training: Cross-Sectional and Randomized Trial Studies. Sci. Rep. 2019, 9, 7500. [Google Scholar] [CrossRef] [PubMed]
- Mäkikallio, T.H.; Seppänen, T.; Niemelä, M.; Airaksinen, K.E.; Tulppo, M.; Huikuri, H.V. Abnormalities in Beat to Beat Complexity of Heart Rate Dynamics in Patients with a Previous Myocardial Infarction. J. Am. Coll. Cardiol. 1996, 28, 1005–1011. [Google Scholar] [CrossRef] [Green Version]
- Kazmi, S.Z.H.; Zhang, H.; Aziz, W.; Monfredi, O.; Abbas, S.A.; Shah, S.A.; Kazmi, S.S.H.; Butt, W.H. Inverse Correlation between Heart Rate Variability and Heart Rate Demonstrated by Linear and Nonlinear Analysis. PLoS ONE 2016, 11, e0157557. [Google Scholar] [CrossRef] [Green Version]
- Porta, A.; Tobaldini, E.; Guzzetti, S.; Furlan, R.; Montano, N.; Gnecchi-Ruscone, T. Assessment of Cardiac Autonomic Modulation during Graded Head-up Tilt by Symbolic Analysis of Heart Rate Variability. Am. J. Physiol.-Heart Circ. Physiol. 2007, 293, H702–H708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, Z.; Xueyun, W.; Jian, Z.J.; Hongxing, L. Fetal Heart Beat Detection by Hilbert Transform and Non-Linear State-Space Projections. IET Sci. Meas. Technol. 2015, 9, 85–92. [Google Scholar] [CrossRef]
- Li, H.; Kwong, S.; Yang, L.; Huang, D.; Xiao, D. Hilbert-Huang Transform for Analysis of Heart Rate Variability in Cardiac Health. IEEE/ACM Trans. Comput. Biol. Bioinform. 2011, 8, 1557–1567. [Google Scholar] [CrossRef]
- Romano, M.; Faiella, G.; Clemente, F.; Iuppariello, L.; Bifulco, P.; Cesarelli, M. Analysis of Foetal Heart Rate Variability Components by Means of Empirical Mode Decomposition. In Proceedings of the XIV Mediterranean Conference on Medical and Biological Engineering and Computing 2016, Paphos, Cyprus, 31 March–2 April 2016; Kyriacou, E., Christofides, S., Pattichis, C.S., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 71–74. [Google Scholar]
- Ortiz, M.R.; Bojorges, E.R.; Aguilar, S.D.; Echeverria, J.C.; Gonzalez-Camarena, R.; Carrasco, S.; Gaitan, M.J.; Martinez, A. Analysis of High Frequency Fetal Heart Rate Variability Using Empirical Mode Decomposition. In Proceedings of the Computers in Cardiology, Lyon, France, 25–28 September 2005; pp. 675–678. [Google Scholar]
- Laguna, P.; Moody, G.B.; Mark, R.G. Power Spectral Density of Unevenly Sampled Data by Least-Square Analysis: Performance and Application to Heart Rate Signals. IEEE Trans. Biomed. Eng. 1998, 45, 698–715. [Google Scholar] [CrossRef]
- Ruf, T. The Lomb-Scargle Periodogram in Biological Rhythm Research: Analysis of Incomplete and Unequally Spaced Time-Series. Biol. Rhythm Res. 1999, 30, 178–201. [Google Scholar] [CrossRef]
- Clifford, G.D.; Tarassenko, L. Quantifying Errors in Spectral Estimates of HRV Due to Beat Replacement and Resampling. IEEE Trans. Biomed. Eng. 2005, 52, 630–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallverdu, M.; Palacios, M.; Caminal, P. Modeling the Dynamics of the Heart Rate Variability by Hidden Markov Models. In Proceedings of the Computers in Cardiology, Thessaloniki, Greece, 21–24 September 2003; pp. 461–464. [Google Scholar]
- Balasubramanian, K.; Nagaraj, N. Cardiac Aging Detection Using Complexity Measures. arXiv 2016, arXiv:160300817. [Google Scholar]
- Voss, A.; Schroeder, R.; Vallverdú, M.; Schulz, S.; Cygankiewicz, I.; Vázquez, R.; Bayés de Luna, A.; Caminal, P. Short-Term vs. Long-Term Heart Rate Variability in Ischemic Cardiomyopathy Risk Stratification. Front. Physiol. 2013, 4, 364. [Google Scholar] [CrossRef] [Green Version]
- Signorini, M.G.; Fanelli, A.; Magenes, G. Monitoring Fetal Heart Rate during Pregnancy: Contributions from Advanced Signal Processing and Wearable Technology. Comput. Math. Methods Med. 2014, 2014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frank, B.; Pompe, B.; Schneider, U.; Hoyer, D. Permutation Entropy Improves Fetal Behavioural State Classification Based on Heart Rate Analysis from Biomagnetic Recordings in near Term Fetuses. Med. Biol. Eng. Comput. 2006, 44, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Signorini, M.G.; Ferrario, M.; Cerutti, S.; Magenes, G. Advances in Monitoring Cardiovascular Signals. Contribution of Nonlinear Signal Processing. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 6568–6571. [Google Scholar]
- Georgoulas, G.; Stylios, D.; Groumpos, P. Predicting the Risk of Metabolic Acidosis for Newborns Based on Fetal Heart Rate Signal Classification Using Support Vector Machines. IEEE Trans. Biomed. Eng. 2006, 53, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Ricciardi, C.; Improta, G.; Amato, F.; Cesarelli, G.; Romano, M. Classifying the Type of Delivery from Cardiotocographic Signals: A Machine Learning Approach. Comput. Methods Programs Biomed. 2020, 196, 105712. [Google Scholar] [CrossRef] [PubMed]
- Fergus, P.; Selvaraj, M.; Chalmers, C. Machine Learning Ensemble Modelling to Classify Caesarean Section and Vaginal Delivery Types Using Cardiotocography Traces. Comput. Biol. Med. 2018, 93, 7–16. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Approach | Technique | Acronym | Reference |
|---|---|---|---|
| Time domain measurements | General Description | - | [7,8,9,10,40] |
| Short-Term Variability | STV | [9,22,25,41,42,43,44,45] | |
| Long-Term Variability | LTV | ||
| Interval Index | II | ||
| Long-Term Irregularity | LTI | ||
| Frequency domain analysis | General Description | - | [5,6,17,46,47,48] |
| Fast Fourier Transform | FFT | [5,11,38,46,48,49,50,51,52] | |
| Short Time Fourier Transform | STFT | ||
| Autoregressive Models | AR | [6,24,26,46,49,53,54] | |
| Wavelet Transform | WT | [22,23,55,56] | |
| Nonlinear methods | General Description | - | [12,17,57,58,59] |
| Entropy Indices | ApEn 1 | [17,60,61,62,63,64,65,66,67,68] | |
| SampEn 2 | |||
| MSE 3 | |||
| Symbolic Dynamics | SD | [4,27,28,69,70,71,72,73] | |
| Fractal Analysis | - | [14,74,75,76] | |
| Detrended Fluctuation Analysis | DFA | [68,77,78] | |
| Poincaré Maps | SD1 4 | [25,79] | |
| SD2 5 | |||
| Other methods | Hilbert–Huang Transform | HHT | [80,81,82] |
| Lomb Method | - | [83,84,85] | |
| Matching Pursuit | MP | [13,86] | |
| Lyapunov Exponents | - | [87,88] | |
| Hidden Markov Models | HMM | [89] | |
| Lempel Ziv Complexity | LZ | [90,91,92] | |
| Artificial Intelligence | Artificial Neural Networks | ANNs | [19,20,57,93,94,95,96,97,98,99,100,101,102,103,104] |
| Approach | Technique | Main Pros | Main Cons |
|---|---|---|---|
| Time domain measurements | General considerations | Despite their widespread use and recognized clinical value, time domain indices rely mainly on descriptive statistical measurements of the FHR and, therefore, they do not allow inferring the physiological processes controlling the variation in the heart rhythm. | |
| STV | It correlates well with the development of metabolic academia, and it is recognized as a valuable antenatal monitoring tool. | There is no agreement on the formula used to calculate the STV, and its effectiveness can be influenced by frequency oscillations. | |
| LTV | It shows good sensitivity to sinusoidal fluctuations in the heart rhythms. | It can be complex to quantify numerically. | |
| Frequency domain analysis | General considerations | Even though frequency domain indicators are widely employed and studied in the literature, particularly for their capability of investigating periodic trends in the heart rate fluctuations, it should be taken into account that these parameters are sensitive to artifacts and, since the heart is not a periodic oscillator, do not allow the inspection of non-periodic trends or transient changes embedded in the variability signal. In addition, power spectral indices are not able to characterize nonreciprocal changes of sympathetic and parasympathetic modulations. | |
| Fourier Transform | It is relatively simple and does not require high computational power; therefore, it is widely employed in the literature. Specific conditions such as the cord arterial base deficit and changes in the behavioral state as well as in the gestational age cause variations in the FHRV spectrum. | The stationarity of the FHRV signal is an essential requirement.Limitations in describing the nonlinear structure of sympatho–vagal interactions. The length of data segments influences the frequency resolution. | |
| AR models | They provide better identification of discrete frequency oscillations for non-stationary and relatively short time series. | The determination of the optimal order of the AR model is not trivial, and a wrong choice can compromise the reliability of the model. | |
| WT | It allows proper processing of the FHR signal, avoiding the problem of long-term non-stationary behavior as well as the extraction of the FHR power at different scale levels. It uses short windows at high frequencies and long windows at low frequencies, thereby obtaining more precise spectral components and enabling a multi-resolution time-frequency representation of the signal. | There is still a lack of a gold standard procedure for the use of WT in the analysis of heart rate variations, even in the analysis of HRV in adults. In particular, it is not clear how the mother wavelet impacts the results and if results obtained using different mother wavelets can be compared. The performance can be unsatisfactory when more than one spectral component is present. Despite its better tunability compared to Fourier Transform, the time and frequency resolutions of wavelet transform cannot be arbitrarily good. Despite the undoubted theory advantages of the WT over traditional time-domain and frequency-domain analysis methods, there seem to be no direct comparisons with nonlinear techniques of FHRV analysis. | |
| Nonlinear methods | Entropy indices (general considerations) | Entropy measurements provide a global index of the overall regularity of the time series under study, but they are not able to detect the dynamics that generate such behavior. In particular, entropy values should be interpreted carefully since they are not always a result of differences in regularity or complexity of the time series, but they can be an effect of the presence of outliers that affect the variance in the heart rate signal. | |
| ApEn | It allows inferring the level of complexity of the FHR signal. | Results are highly dependent on the signal length and lack relative consistency since the algorithm also counts self-matches, thus introducing a bias in the results. The choice of the optimal parameters for the calculation of the ApEn is difficult. | |
| SampEn | Similar to ApEn, it allows quantifying the complexity of a time series, but it eliminates self-matches, requires lower computational time, and it is largely independent of the signal length. | The choice of the parameters to calculate the SampEn is critical, and there are no guidelines nor a gold standard on their use and optimization. It appears to be more sensitive than ApEn to noise and non-normal beats. | |
| SD | The signal’s samples are reduced to a few possible patterns of symbols, thereby simplifying the study and the classification of the underlying dynamics of the system. | The choice of the alphabet of symbols and the criteria to form words of symbols is complex, and a standard has not been achieved yet. The symbolization can cause loss of information and can be influenced by the presence of outliers. | |
| Fractal analysis | It allows calculating the degree of irregularity of the system by splitting it into a number of fundamental units (fractals) with the same shape at different scales of observation. | Algorithms for a reliable application of fractal analysis are not optimized for real-time monitoring. It is preferred for the analysis of time series of normal-to-normal interbeat intervals from long-term recording. | |
| DFA | Useful for removing external interference (signal noise). Over other conventional fractal methods, it permits the detection of long-range correlations embedded in raw non-stationary time series. | The signal segmentation can produce two undesirable effects: (i) if the signal length is not a multiple of the window length, at least one block will have fewer samples than the others; (ii) when one block is considerably shorter than the others, discontinuities will be observed in the detrended signal. A minimum signal length of 8000 samples and normal-to-normal interbeat intervals are requirements to apply the DFA. High computational load prevents the application of long series of data. | |
| Poincaré maps | They provide an easily and immediately readable visual representation of the results. A signal duration of 3–5 min is sufficient for FHRV analysis. | Visual interpretation can lead to subjective evaluation. SD1 and SD2 indices do not provide much additional information compared to time-domain measurements. Temporal information, which is crucial for the detection of nonlinear dynamics, is lost in traditional Poincaré analyses that focus on mere statistical indices extracted from a cumulative distribution of points. | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ponsiglione, A.M.; Cosentino, C.; Cesarelli, G.; Amato, F.; Romano, M. A Comprehensive Review of Techniques for Processing and Analyzing Fetal Heart Rate Signals. Sensors 2021, 21, 6136. https://doi.org/10.3390/s21186136
Ponsiglione AM, Cosentino C, Cesarelli G, Amato F, Romano M. A Comprehensive Review of Techniques for Processing and Analyzing Fetal Heart Rate Signals. Sensors. 2021; 21(18):6136. https://doi.org/10.3390/s21186136
Chicago/Turabian StylePonsiglione, Alfonso Maria, Carlo Cosentino, Giuseppe Cesarelli, Francesco Amato, and Maria Romano. 2021. "A Comprehensive Review of Techniques for Processing and Analyzing Fetal Heart Rate Signals" Sensors 21, no. 18: 6136. https://doi.org/10.3390/s21186136