
Recent Advances in Transducers for Intravascular Ultrasound (IVUS) Imaging



Abstract
:1. Introduction
2. Intravascular Ultrasound (IVUS) Imaging
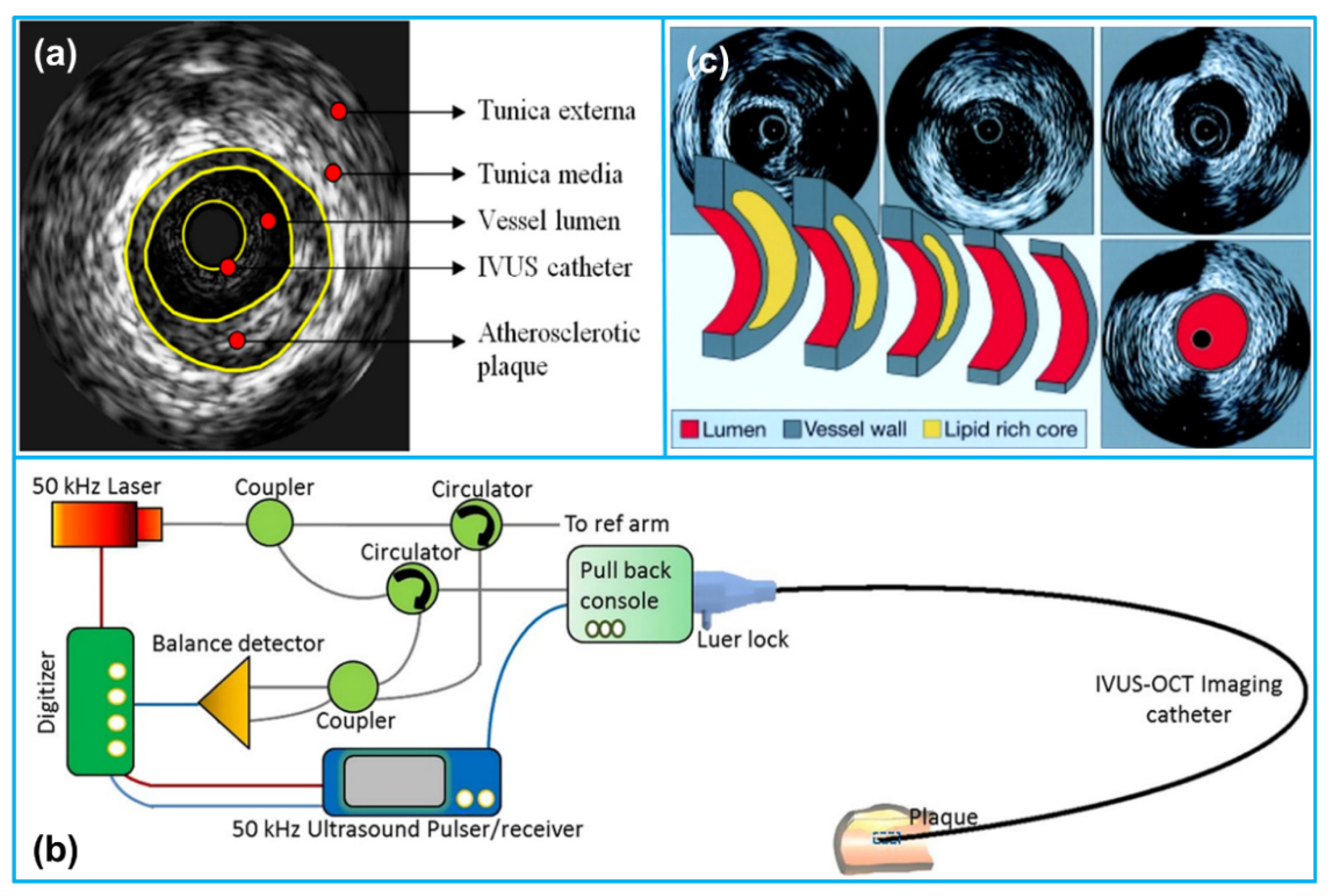
2.1. IVUS Imaging Principle
2.2. Evaluation Parameters for IVUS Imaging
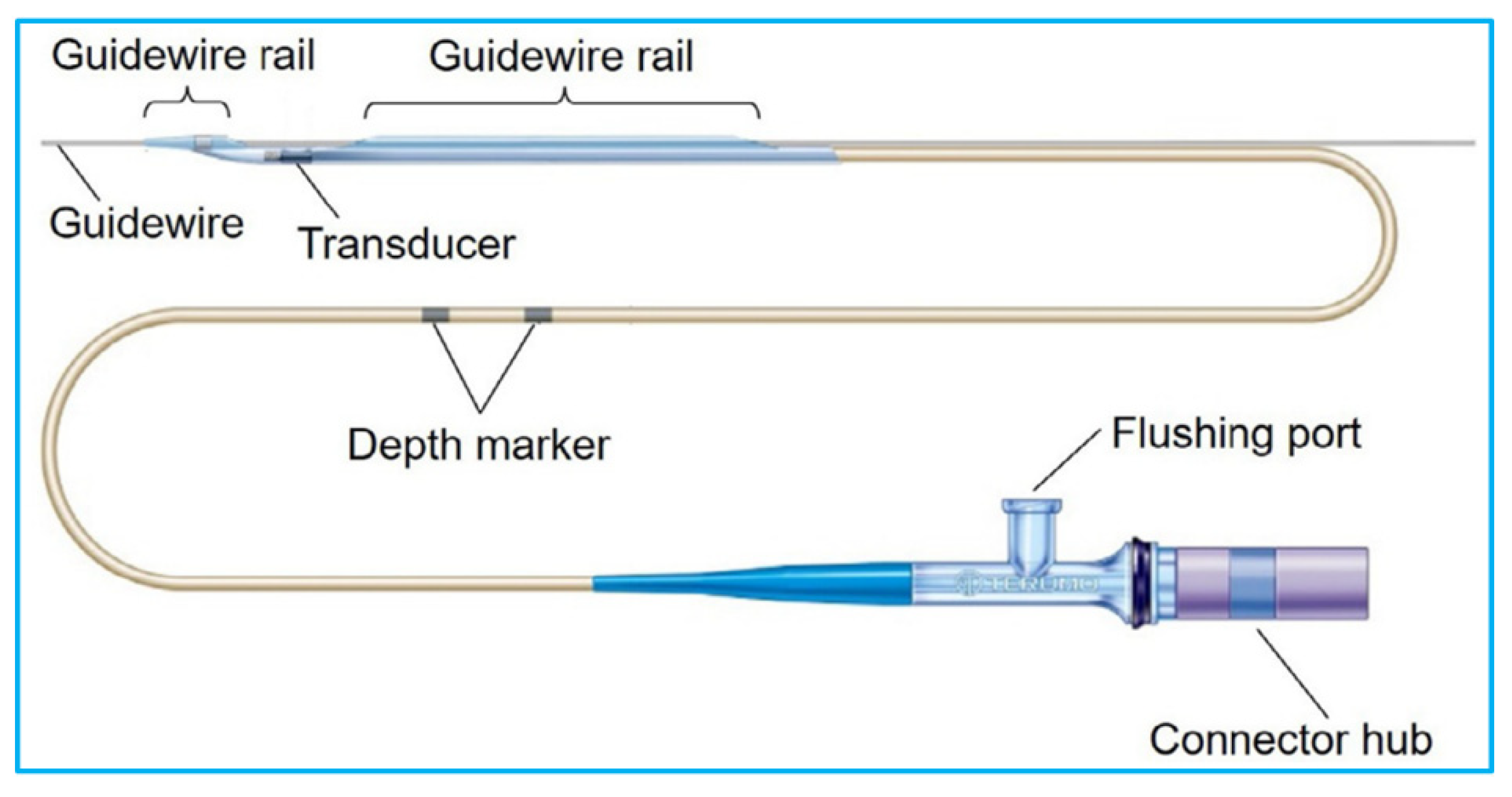
2.3. IVUS Catheter
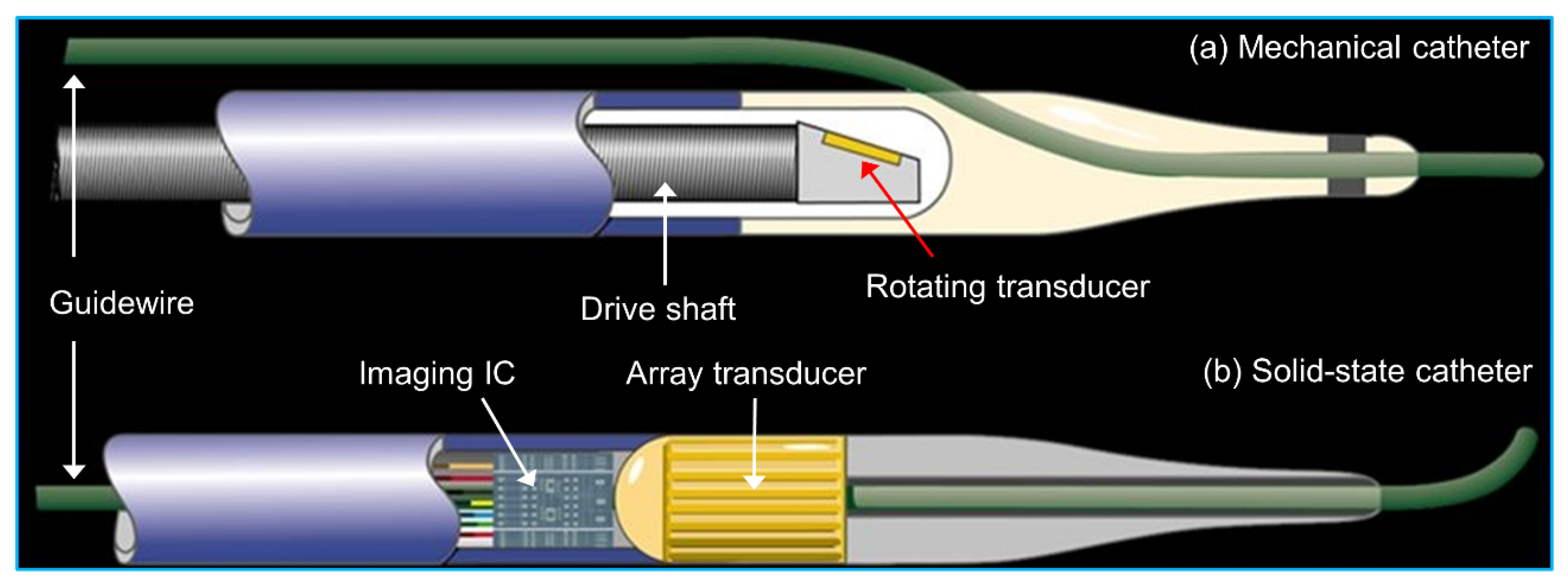
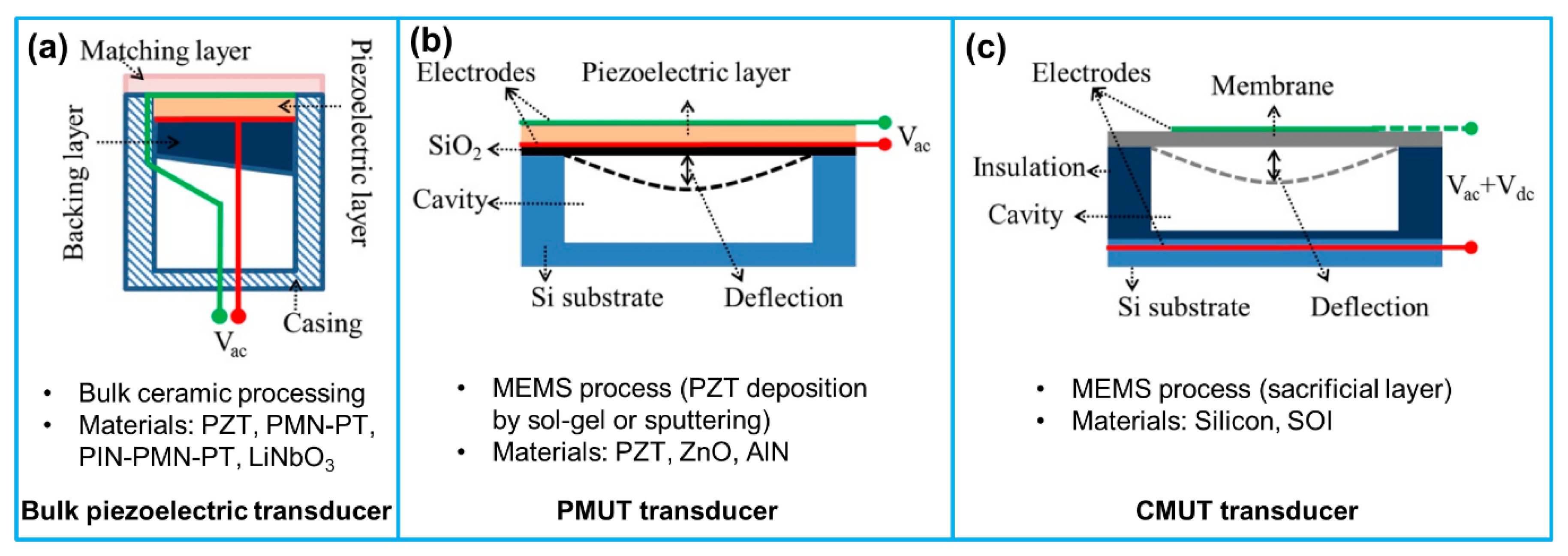
2.4. Ultrasound Transducers for IVUS Imaging
3. Piezoelectric Transducers for IVUS Imaging
3.1. Single Frequency IVUS Transducer
3.1.1. Conventional Piezoelectric IVUS Transducer
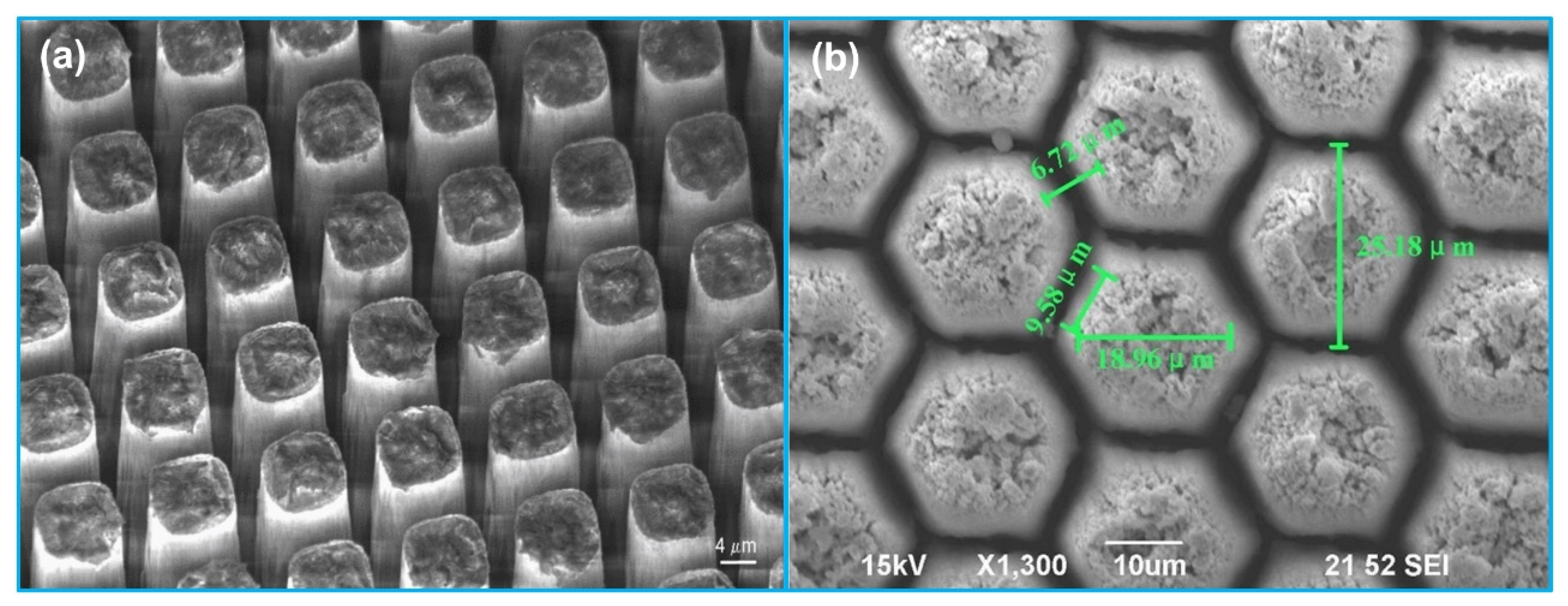
3.1.2. Piezo-Composite Micromachined Ultrasound Transducer (PC-MUT)
3.1.3. Micromotor Driven IVUS Imaging
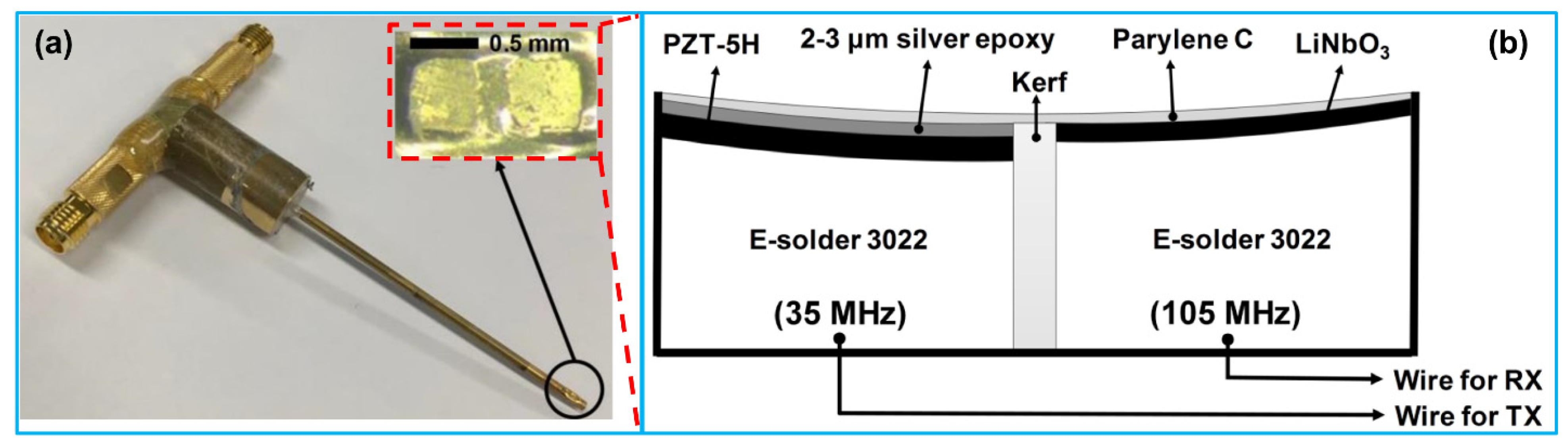
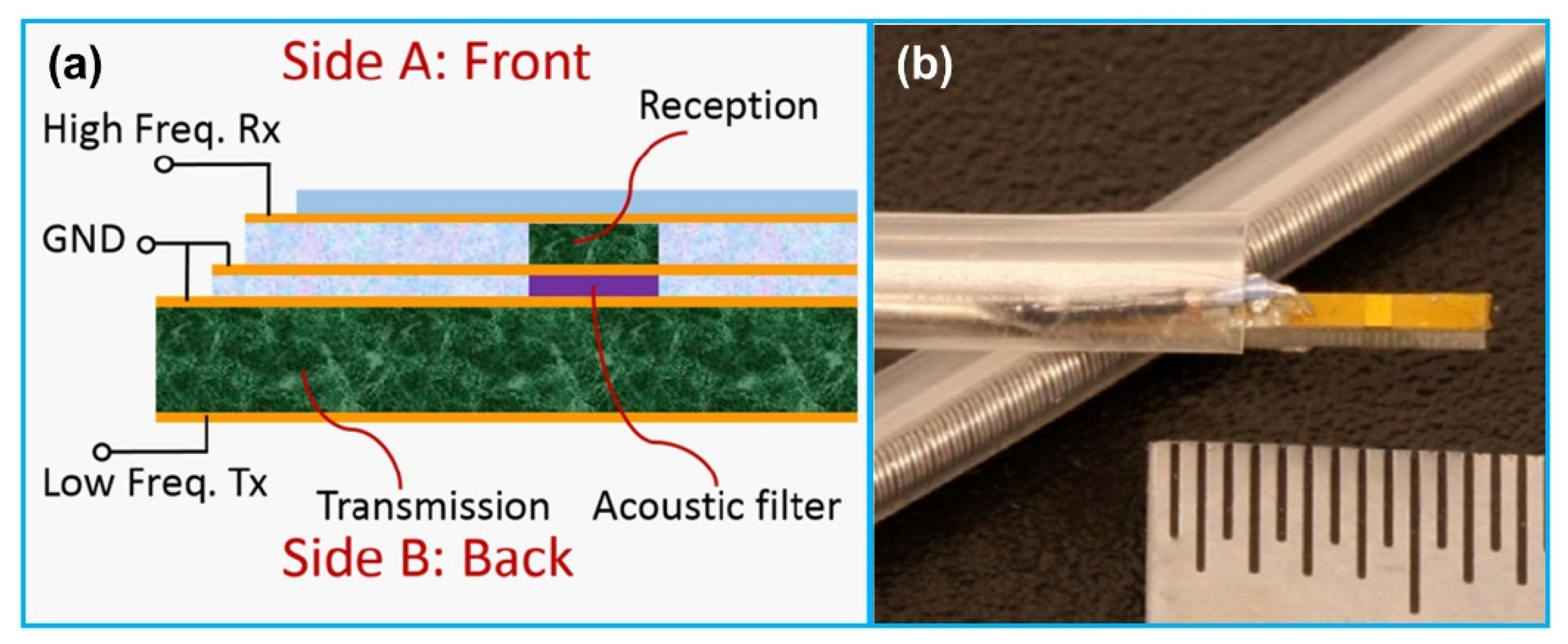
3.2. Dual Frequency IVUS Transducer
3.3. Multifrequency IVUS Imaging
3.4. Array for IVUS Imaging
3.4.1. Single Frequency Array
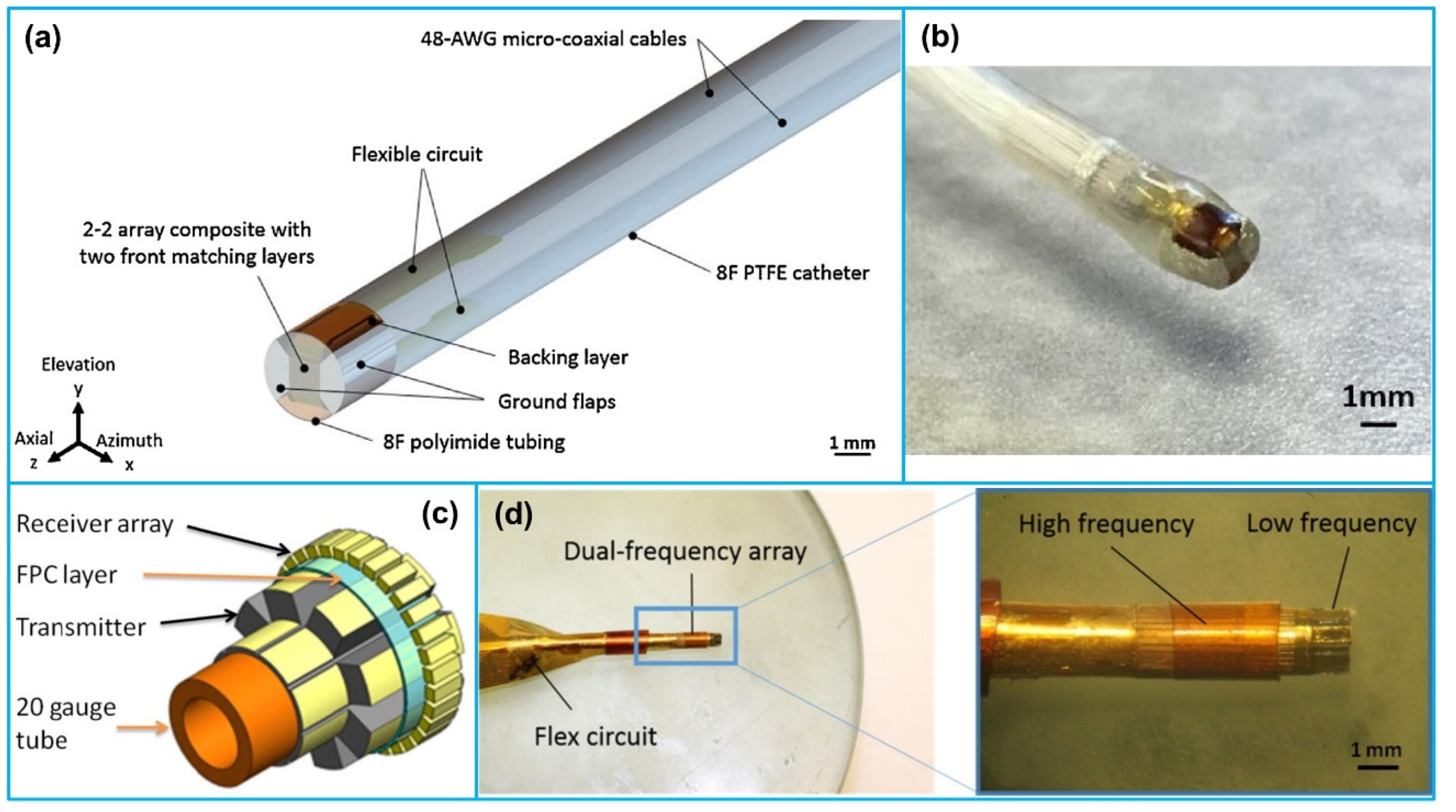
3.4.2. Dual Frequency Array
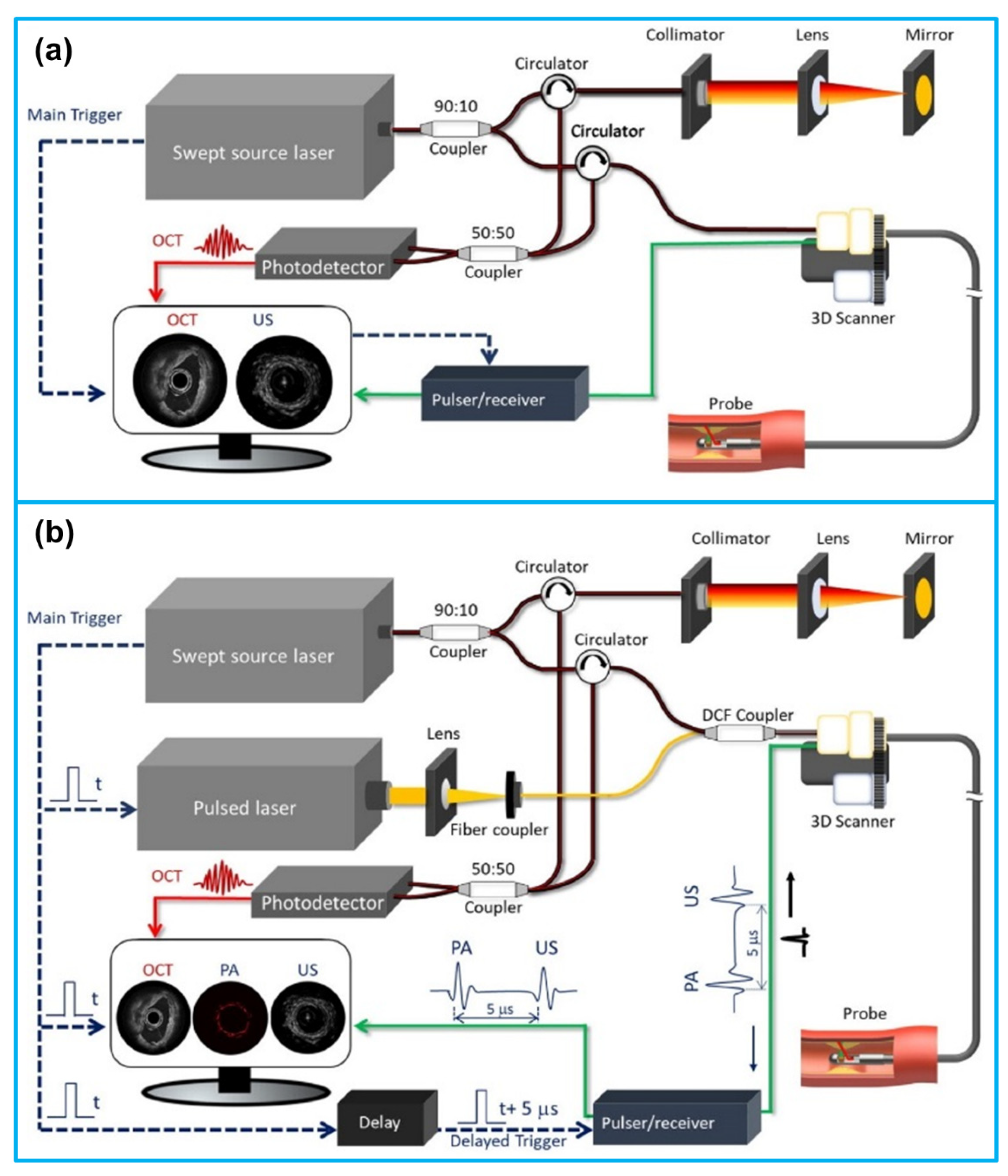
4. IVUS-Based Multimodality Intravascular Imaging
5. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Cardiovascular Diseases (CVDs). Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 6 January 2021).
- World Health Organization (WHO). About Cardiovascular Diseases. Available online: https://www.who.int/cardiovascular_diseases/about_cvd/en/ (accessed on 6 January 2021).
- Virmani, R.; Kolodgie, F.D.; Burke, A.P.; Farb, A.; Schwartz, S.M. Lessons from sudden coronary death: A comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler. Thromb. Vasc. Biol. 2000, 20, 1262–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Frostegård, J. Immunity, atherosclerosis and cardiovascular disease. BMC Med. 2013, 11, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, P.K. Mechanisms of plaque vulnerability and rupture. J. Am. Coll. Cardiol. 2003, 41, S15–S22. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.D. Orbicular origins. Nat. Mater. 2013, 12, 476–478. [Google Scholar] [CrossRef] [PubMed]
- Venugopal, S.K.; Anoruo, M.; Jialal, I. Biochemistry, Low Density Lipoprotein; StatPearls Publishing LLC: Treasure Island, FL, USA, 2020. [Google Scholar]
- Falk, E.; Nakano, M.; Bentzon, J.F.; Finn, A.V.; Virmani, R. Update on acute coronary syndromes: The pathologists’ view. Eur. Heart J. 2013, 34, 719–728. [Google Scholar] [CrossRef] [Green Version]
- Libby, P.; Theroux, P. Pathophysiology of coronary artery disease. Circulation 2005, 111, 3481–3488. [Google Scholar] [CrossRef] [Green Version]
- Liang, M.; Puri, A.; Devlin, G. The vulnerable plaque: The real villain in acute coronary syndromes. Open Cardiovasc. Med. J. 2011, 5, 123. [Google Scholar] [CrossRef] [Green Version]
- Stefanadis, C.; Antoniou, C.; Tsiachris, D.; Pietri, P. Coronary atherosclerotic vulnerable plaque: Current perspectives. J. Am. Heart Assoc. 2017, 6, e005543. [Google Scholar] [CrossRef] [Green Version]
- Virmani, R.; Burke, A.P.; Kolodgie, F.D.; Farb, A. Pathology of the thin-cap fibroatheroma: A type of vulnerable plaque. J. Interv. Cardiol. 2003, 16, 267–272. [Google Scholar] [CrossRef]
- Thim, T.; Hagensen, M.K.; Bentzon, J.F.; Falk, E. From vulnerable plaque to atherothrombosis. J. Intern. Med. 2008, 263, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Virmani, R.; Burke, A.P.; Farb, A.; Kolodgie, F.D. Pathology of the vulnerable plaque. J. Am. Coll. Cardiol. 2006, 47, C13–C18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakakura, K.; Nakano, M.; Otsuka, F.; Ladich, E.; Kolodgie, F.D.; Virmani, R. Pathophysiology of atherosclerosis plaque progression. Heart Lung Circ. 2013, 22, 399–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarkin, J.M.; Dweck, M.R.; Evans, N.R.; Takx, R.A.P.; Brown, A.J.; Tawakol, A.; Fayad, Z.A.; Rudd, J.H.F. Imaging atherosclerosis. Circ. Res. 2016, 118, 750–769. [Google Scholar] [CrossRef] [Green Version]
- Weinreich, M.; Litwok, Y.; Mui, L.W.; Lau, J.F. Advanced vascular imaging. Vasc. Med. 2017, 22, 73–76. [Google Scholar] [CrossRef]
- Mantella, L.E.; Liblik, K.; Johri, A.M. Vascular imaging of atherosclerosis: Strengths and weaknesses. Atherosclerosis 2021, 319, 42–50. [Google Scholar] [CrossRef]
- Joshi, F.R.; Lindsay, A.C.; Obaid, D.R.; Falk, E.; Rudd, J.H.F. Non-invasive imaging of atherosclerosis. Eur. Heart J. Cardiovasc. Imaging 2012, 13, 205–218. [Google Scholar] [CrossRef] [Green Version]
- Mushenkova, N.V.; Summerhill, V.I.; Zhang, D.; Romanenko, E.B.; Grechko, A.V.; Orekhov, A.N. Current Advances in the Diagnostic Imaging of Atherosclerosis: Insights into the Pathophysiology of Vulnerable Plaque. Int. J. Mol. Sci. 2020, 21, 2992. [Google Scholar] [CrossRef] [Green Version]
- Garcìa-Garcìa, H.M.; Gogas, B.D.; Serruys, P.W.; Bruining, N. IVUS-based imaging modalities for tissue characterization: Similarities and differences. Int. J. Cardiovasc. Imaging 2011, 27, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erglis, A.; Jegere, S.; Narbute, I. Intravascular ultrasound-based imaging modalities for tissue characterisation. Interv. Cardiol. Rev. 2014, 9, 151. [Google Scholar] [CrossRef] [PubMed]
- Koganti, S.; Kotecha, T.; Rakhit, R.D. Choice of intracoronary imaging: When to use intravascular ultrasound or optical coherence tomography. Interv. Cardiol. Rev. 2016, 11, 11. [Google Scholar] [CrossRef] [Green Version]
- Shammas, N.W.; Radaideh, Q.; Shammas, W.J.; Daher, G.E.; Rachwan, R.J.; Radaideh, Y. The role of precise imaging with intravascular ultrasound in coronary and peripheral interventions. Vasc. Health Risk Manag. 2019, 15, 283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Training in Diagnostic Ultrasound: Essentials, Principles and Standards: Report of a WHO Study Group; World Health Organization: Geneva, Switzerland, 1998; ISBN 9241208759. [Google Scholar]
- Shlofmitz, E.; Zhu, B.; Khalid, N. Intravascular Ultrasound (IVUS); StatPearls Publishing LLC: Treasure Island, FL, USA, 2021. [Google Scholar]
- Libby, P.; Buring, J.E.; Badimon, L.; Hansson, G.K.; Deanfield, J.; Bittencourt, M.S.; Tokgözoğlu, L.; Lewis, E.F. Atherosclerosis. Nat. Rev. Dis. Prim. 2019, 5, 56. [Google Scholar] [CrossRef]
- Schoenhagen, P.; Nissen, S.E. An Atlas and Manual of Coronary Intravascular Ultrasound Imaging; CRC Press: Boca Raton, FL, USA, 2003; ISBN 1135399433. [Google Scholar]
- Schoenhagen, P.; Nissen, S. Understanding coronary artery disease: Tomographic imaging with intravascular ultrasound. Heart 2002, 88, 91–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakabčin, J.; Špaček, R.; Bystroň, M.; Kvašňák, M.; Jager, J.; Veselka, J.; Kala, P.; Červinka, P. Long-term health outcome and mortality evaluation after invasive coronary treatment using drug eluting stents with or without the IVUS guidance. Randomized control trial. HOME DES IVUS. Catheter. Cardiovasc. Interv. 2010, 75, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, T.G.; Kalantzis, C.; Katsianos, E.; Sanoudou, D.; Vavuranakis, M.; Tousoulis, D. Personalized assessment of the coronary atherosclerotic arteries by intravascular ultrasound imaging: Hunting the vulnerable plaque. J. Pers. Med. 2019, 9, 8. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Ma, T.; Mohar, D.; Steward, E.; Yu, M.; Piao, Z.; He, Y.; Shung, K.K.; Zhou, Q.; Patel, P.M. Ultrafast optical-ultrasonic system and miniaturized catheter for imaging and characterizing atherosclerotic plaques in vivo. Sci. Rep. 2015, 5, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Murray, S.W.; Stables, R.H.; Palmer, N.D. Virtual histology imaging in acute coronary syndromes: Useful or just a research tool? J. Invasive Cardiol. 2010, 22, 84–91. [Google Scholar]
- Gao, J.; Wang, Y.-Y.; Liu, Y. Application of virtual histological intravascular ultrasound in plaque composition assessment of saphenous vein graft diseases. Chin. Med. J. 2019, 132, 957. [Google Scholar] [CrossRef]
- Nair, A.; Kuban, B.D.; Tuzcu, E.M.; Schoenhagen, P.; Nissen, S.E.; Vince, D.G. Coronary plaque classification with intravascular ultrasound radiofrequency data analysis. Circulation 2002, 106, 2200–2206. [Google Scholar] [CrossRef] [Green Version]
- Ng, A.; Swanevelder, J. Resolution in ultrasound imaging. Contin. Educ. Anaesth. Crit. Care Pain 2011, 11, 186–192. [Google Scholar] [CrossRef]
- Foster, F.S.; Pavlin, C.J.; Harasiewicz, K.A.; Christopher, D.A.; Turnbull, D.H. Advances in ultrasound biomicroscopy. Ultrasound Med. Biol. 2000, 26, 1–27. [Google Scholar] [CrossRef]
- Mintz, G.S.; Nissen, S.E.; Anderson, W.D.; Bailey, S.R.; Erbel, R.; Fitzgerald, P.J.; Pinto, F.J.; Rosenfield, K.; Siegel, R.J.; Tuzcu, E.M. American College of Cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravascular ultrasound studies (ivus) A report of the american college of cardiology task force on clinical expert consensus doc. J. Am. Coll. Cardiol. 2001, 37, 1478–1492. [Google Scholar] [CrossRef] [Green Version]
- Gougheri, H.S.; Dangi, A.; Kothapalli, S.-R.; Kiani, M. A comprehensive study of ultrasound transducer characteristics in microscopic ultrasound neuromodulation. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Üstüner, K.F.; Holley, G.L. Ultrasound imaging system performance assessment. In Proceedings of the AAPM Annual Meeting, San Diego, CA, USA, 10–14 August 2003. [Google Scholar]
- Agarwal, A.; Schneider, F.K.; Yoo, Y.M.; Kim, Y. Image quality evaluation with a new phase rotation beamformer. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2008, 55, 1947–1955. [Google Scholar] [CrossRef]
- Frimerman, A.; Abergel, E.; Blondheim, D.S.; Shotan, A.; Meisel, S.; Shochat, M.; Punjabi, P.; Roguin, A. Novel Method for Real Time Co-Registration of IVUS and Coronary Angiography. J. Interv. Cardiol. 2016, 29, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stigall, J.; Robinson, G. Flushing for Imaging Catheters. U.S. Patent Application No. 14/211,717, 2014. [Google Scholar]
- Balocco, S. Intravascular Ultrasound: From Acquisition to Advanced Quantitative Analysis; Elsevier: Amsterdam, The Netherlands, 2020; ISBN 0128188340. [Google Scholar]
- Nissen, S.E.; Yock, P. Intravascular ultrasound: Novel pathophysiological insights and current clinical applications. Circulation 2001, 103, 604–616. [Google Scholar] [CrossRef]
- Katouzian, A.; Angelini, E.D.; Carlier, S.G.; Suri, J.S.; Navab, N.; Laine, A.F. A state-of-the-art review on segmentation algorithms in intravascular ultrasound (IVUS) images. IEEE Trans. Inf. Technol. Biomed. 2012, 16, 823–834. [Google Scholar] [CrossRef] [Green Version]
- McDaniel, M.C.; Eshtehardi, P.; Sawaya, F.J.; Douglas, J.S.; Samady, H. Contemporary clinical applications of coronary intravascular ultrasound. JACC Cardiovasc. Interv. 2011, 4, 1155–1167. [Google Scholar] [CrossRef] [Green Version]
- Kitahara, H.; Honda, Y.; Fitzgerald, P.J. Intravascular Ultrasound BT—PanVascular Medicine; Lanzer, P., Ed.; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1379–1418. ISBN 978-3-642-37078-6. [Google Scholar]
- Kwon, T.-G.; Cho, Y.J.; Bae, J.-H. Physical principles and equipment: IVUS. In Coronary Imaging and Physiology; Springer: Berlin/Heidelberg, Germany, 2018; pp. 3–7. [Google Scholar]
- Bangalore, S.; Bhatt, D.L. Coronary intravascular ultrasound. Circulation 2013, 127, e868–e874. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Yuan, J.R.; Cheng, A.; Snook, K.; Rehrig, P.W.; Shrout, T.R.; Hackenberger, W.S.; Cao, P.; Lavalelle, G.; Geng, X. 5I-1 Microfabrication of piezoelectric composite ultrasound transducers (PC-MUT). In Proceedings of the 2006 IEEE Ultrasonics Symposium, Vancouver, BC, Canada, 3–6 October 2006; 2006; pp. 922–925. [Google Scholar]
- Jung, J.; Lee, W.; Kang, W.; Shin, E.; Ryu, J.; Choi, H. Review of piezoelectric micromachined ultrasonic transducers and their applications. J. Micromech. Microeng. 2017, 27, 113001. [Google Scholar] [CrossRef]
- Wang, J.; Zheng, Z.; Chan, J.; Yeow, J.T.W. Capacitive micromachined ultrasound transducers for intravascular ultrasound imaging. Microsyst. Nanoeng. 2020, 6, 1–13. [Google Scholar] [CrossRef]
- Qiu, Y.; Gigliotti, J.V.; Wallace, M.; Griggio, F.; Demore, C.E.M.; Cochran, S.; Trolier-McKinstry, S. Piezoelectric micromachined ultrasound transducer (PMUT) arrays for integrated sensing, actuation and imaging. Sensors 2015, 15, 8020–8041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erguri, A.S.; Huang, Y.; Zhuang, X.; Oralkan, O.; Yarahoglu, G.G.; Khuri-Yakub, B.T. Capacitive micromachined ultrasonic transducers: Fabrication technology. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2005, 52, 2242–2258. [Google Scholar] [CrossRef] [PubMed]
- Salim, M.S.; Abd Malek, M.F.; Heng, R.B.W.; Juni, K.M.; Sabri, N. Capacitive micromachined ultrasonic transducers: Technology and application. J. Med. Ultrasound 2012, 20, 8–31. [Google Scholar] [CrossRef] [Green Version]
- Maeder, M.D.; Damjanovic, D.; Setter, N. Lead free piezoelectric materials. J. Electroceram. 2004, 13, 385–392. [Google Scholar] [CrossRef]
- Chorsi, M.T.; Curry, E.J.; Chorsi, H.T.; Das, R.; Baroody, J.; Purohit, P.K.; Ilies, H.; Nguyen, T.D. Piezoelectric biomaterials for sensors and actuators. Adv. Mater. 2019, 31, 1802084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trolier-McKinstry, S.; Muralt, P. Thin film piezoelectrics for MEMS. J. Electroceram. 2004, 12, 7–17. [Google Scholar] [CrossRef]
- Zhou, Q.; Lau, S.; Wu, D.; Shung, K.K. Piezoelectric films for high frequency ultrasonic transducers in biomedical applications. Prog. Mater. Sci. 2011, 56, 139–174. [Google Scholar] [CrossRef] [Green Version]
- Dausch, D.E.; Gilchrist, K.H.; Carlson, J.B.; Hall, S.D.; Castellucci, J.B.; von Ramm, O.T. In vivo real-time 3-D intracardiac echo using PMUT arrays. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2014, 61, 1754–1764. [Google Scholar] [CrossRef]
- Eccardt, P.C.; Niederer, K. Micromachined ultrasound transducers with improved coupling factors from a CMOS compatible process. Ultrasonics 2000, 38, 774–780. [Google Scholar] [CrossRef]
- Oralkan, O.; Ergun, A.S.; Johnson, J.A.; Karaman, M.; Demirci, U.; Kaviani, K.; Lee, T.H.; Khuri-Yakub, B.T. Capacitive micromachined ultrasonic transducers: Next-generation arrays for acoustic imaging? IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2002, 49, 1596–1610. [Google Scholar] [CrossRef]
- Zhuang, X.; Lin, D.-S.; Oralkan, Ö.; Khuri-Yakub, B.T. Fabrication of flexible transducer arrays with through-wafer electrical interconnects based on trench refilling with PDMS. J. Microelectromech. Syst. 2008, 17, 446–452. [Google Scholar] [CrossRef]
- Xu, T.; Tekes, C.; Satir, S.; Arkan, E.; Ghovanloo, M.; Degertekin, F.L. Design, modeling and characterization of a 35MHz 1-D CMUT phased array. In Proceedings of the 2013 IEEE International Ultrasonics Symposium (IUS), Prague, Czech Republic, 21–25 July 2013; 2013; pp. 1987–1990. [Google Scholar]
- Lim, J.; Tekes, C.; Degertekin, F.L.; Ghovanloo, M. Towards a reduced-wire interface for CMUT-based intravascular ultrasound imaging systems. IEEE Trans. Biomed. Circuits Syst. 2016, 11, 400–410. [Google Scholar] [CrossRef]
- Pekař, M.; Mihajlović, N.; Belt, H.; Kolen, A.F.; Van Rens, J.; Budzelaar, F.; Jacobs, B.; Bosch, J.G.; Vos, H.J.; Rem-Bronneberg, D. Quantitative imaging performance of frequency-tunable capacitive micromachined ultrasonic transducer array designed for intracardiac application: Phantom study. Ultrasonics 2018, 84, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Degertekin, F.L.; Guldiken, R.O.; Karaman, M. Annular-ring CMUT arrays for forward-looking IVUS: Transducer characterization and imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2006, 53, 474–482. [Google Scholar] [CrossRef] [PubMed]
- Yeh, D.T.; Oralkan, O.; Wygant, I.O.; O’Donnell, M.; Khuri-Yakub, B.T. 3-D ultrasound imaging using a forward-looking CMUT ring array for intravascular/intracardiac applications. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2006, 53, 1202–1211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahorian, J.; Hochman, M.; Xu, T.; Satir, S.; Gurun, G.; Karaman, M.; Degertekin, F.L. Monolithic CMUT-on-CMOS integration for intravascular ultrasound applications. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 2659–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gurun, G.; Tekes, C.; Zahorian, J.; Xu, T.; Satir, S.; Karaman, M.; Hasler, J.; Degertekin, F.L. Single-chip CMUT-on-CMOS front-end system for real-time volumetric IVUS and ICE imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2014, 61, 239–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manwar, R.; Simpson, T.; Bakhtazad, A.; Chowdhury, S. Fabrication and characterization of a high frequency and high coupling coefficient CMUT array. Microsyst. Technol. 2017, 23, 4965–4977. [Google Scholar] [CrossRef]
- Ma, T.; Yu, M.; Li, J.; Munding, C.E.; Chen, Z.; Fei, C.; Shung, K.K.; Zhou, Q. Erratum: Multi-frequency intravascular ultrasound (IVUS) imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2015, 62, 604. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Wang, X.; Chen, Y.; Fu, Q.; Su, M.; Zhang, L.; Xia, J.; Dai, J.; Zhang, Y.; Zheng, H. Modulated excitation imaging system for intravascular ultrasound. IEEE Trans. Biomed. Eng. 2016, 64, 1935–1942. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, B.D.; Lowe, H.C.; Takano, M.; Fuster, V.; Jang, I.-K. Intravascular modalities for detection of vulnerable plaque: Current status. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1333–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Wal, A.C.; Becker, A.E. Atherosclerotic plaque rupture–pathologic basis of plaque stability and instability. Cardiovasc. Res. 1999, 41, 334–344. [Google Scholar] [CrossRef]
- Li, X.; Wu, W.; Chung, Y.; Shih, W.Y.; Shih, W.-H.; Zhou, Q.; Shung, K.K. 80-MHz intravascular ultrasound transducer using PMN-PT free-standing film. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2011, 58, 2281–2288. [Google Scholar]
- Sung, J.H.; Jeong, J.S. Development of high-frequency (>60 MHz) intravascular ultrasound (IVUS) transducer by using asymmetric electrodes for improved beam profile. Sensors 2018, 18, 4414. [Google Scholar] [CrossRef] [Green Version]
- Ma, X.; Cao, W. Single-Crystal High-Frequency Intravascular Ultrasound Transducer With 40-µm Axial Resolution. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 67, 810–816. [Google Scholar] [CrossRef]
- Zhang, Q.; Pang, X.; Zhang, Z.; Su, M.; Hong, J.; Zheng, H.; Qiu, W.; Lam, K.H. Miniature transducer using PNN-PZT-based ceramic for intravascular ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 1102–1109. [Google Scholar] [CrossRef]
- Fei, C.; Yang, Y.; Guo, F.; Lin, P.; Chen, Q.; Zhou, Q.; Sun, L. PMN-PT single crystal ultrasonic transducer with half-concave geometric design for IVUS imaging. IEEE Trans. Biomed. Eng. 2017, 65, 2087–2092. [Google Scholar] [CrossRef]
- Yoon, S.; Williams, J.; Kang, B.J.; Yoon, C.; Cabrera-Munoz, N.; Jeong, J.S.; Lee, S.G.; Shung, K.K.; Kim, H.H. Angled-focused 45 MHz PMN-PT single element transducer for intravascular ultrasound imaging. Sensors Actuators A Phys. 2015, 228, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Jang, J.; Chang, J.H. Oblong-shaped-focused transducers for intravascular ultrasound imaging. IEEE Trans. Biomed. Eng. 2016, 64, 671–680. [Google Scholar] [CrossRef] [PubMed]
- Panda, P.K. Environmental friendly lead-free piezoelectric materials. J. Mater. Sci. 2009, 44, 5049–5062. [Google Scholar] [CrossRef] [Green Version]
- Safari, A.; Abazari, M. Lead-free piezoelectric ceramics and thin films. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2010, 57, 2165–2176. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Lam, K.H.; Li, X.; Chen, R.; Ren, W.; Ren, X.; Zhou, Q.; Shung, K.K. Correspondence: Lead-free intravascular ultrasound transducer using BZT-50BCT ceramics. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2013, 60, 1272–1276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, B.; Zhang, Z.; Ma, T.; Yang, X.; Li, Y.; Shung, K.K.; Zhou, Q. (100)-Textured KNN-based thick film with enhanced piezoelectric property for intravascular ultrasound imaging. Appl. Phys. Lett. 2015, 106, 173504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fei, C.; Chiu, C.T.; Chen, X.; Chen, Z.; Ma, J.; Zhu, B.; Shung, K.K.; Zhou, Q. Ultrahigh frequency (100 MHz–300 MHz) ultrasonic transducers for optical resolution medical imagining. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Li, S.; Kim, J.; Ma, J. High Frequency Piezo-Composite Micromachined Ultrasound Transducer Array Technology for Biomedical Imaging; American Society of Mechanical Engineers: New York, NY, USA, 2017; ISBN 0791861635. [Google Scholar]
- Yin, J.; Lee, M.; Cherin, E.; Lukacs, M.; Foster, F.S. High frequency piezo-composite transducer with hexagonal pillars. In Proceedings of the 2009 IEEE International Ultrasonics Symposium, Rome, Italy, 20–23 September 2009; IEEE: Piscataway, NJ, USA, 2009; pp. 2750–2753. [Google Scholar]
- Brown, J.A.; Cherin, E.; Yin, J.; Foster, F.S. Fabrication and performance of high-frequency composite transducers with triangular-pillar geometry. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2009, 56, 827–836. [Google Scholar] [CrossRef]
- Yuan, J.R.; Jiang, X.; Cao, P.-J.; Sadaka, A.; Bautista, R.; Snook, K.; Rehrig, P.W. 5C-5 high frequency piezo composites microfabricated ultrasound transducers for intravascular imaging. In Proceedings of the 2006 IEEE Ultrasonics Symposium, Vancouver, BC, Canada, 3–6 October 2006; IEEE: Piscataway, NJ, USA, 2006; pp. 264–268. [Google Scholar]
- Yuan, J.; Rhee, S.; Jiang, X.N. 60 MHz PMN-PT based 1-3 composite transducer for IVUS imaging. In Proceedings of the 2008 IEEE Ultrasonics Symposiumn, Beijing, China, 2–5 November 2008; IEEE: Piscataway, NJ, USA, 2008; pp. 682–685. [Google Scholar]
- Jiang, X.; Snook, K.; Cheng, A.; Hackenberger, W.S.; Geng, X. Micromachined PMN-PT single crystal composite transducers--15–75 MHz PC-MUT. In Proceedings of the 2008 IEEE Ultrasonics Symposiumn, Beijing, China, 2–5 November 2008; IEEE: Piscataway, NJ, USA, 2008; pp. 164–167. [Google Scholar]
- Li, X.; Ma, T.; Tian, J.; Han, P.; Zhou, Q.; Shung, K.K. Micromachined PIN-PMN-PT crystal composite transducer for high-frequency intravascular ultrasound (IVUS) imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2014, 61, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Wu, J.; Lam, K.H.; Yao, L.; Zhou, Q.; Tian, J.; Han, P.; Shung, K.K. Thermal-independent properties of PIN-PMN-PT single-crystal linear-array ultrasonic transducers. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2012, 59, 2777–2784. [Google Scholar]
- Zhang, S.; Li, F.; Jiang, X.; Kim, J.; Luo, J.; Geng, X. Advantages and challenges of relaxor-PbTiO3 ferroelectric crystals for electroacoustic transducers–A review. Prog. Mater. Sci. 2015, 68, 1–66. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Li, F.; Yu, F.; Jiang, X.; Lee, H.-Y.; Luo, J.; Shrout, T.R. Recent developments in piezoelectric crystals. J. Korean Ceram. Soc. 2018, 55, 419–439. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Lv, J.; Zhu, X.; Cui, Y.; Jian, X. Development of High Frequency Piezocomposite with Hexagonal Pillars via Cold Ablation Process. Ultrasonics 2021, 114, 106404. [Google Scholar] [CrossRef]
- Xu, J.; Han, Z.; Wang, N.; Li, Z.; Lv, J.; Zhu, X.; Cui, Y.; Jian, X. Micromachined High Frequency 1-3 Piezocomposite Transducer using Picosecond Laser. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2021. [Google Scholar] [CrossRef] [PubMed]
- Uribe-Patarroyo, N.; Bouma, B.E. Rotational distortion correction in endoscopic optical coherence tomography based on speckle decorrelation. Opt. Lett. 2015, 40, 5518–5521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, J.; Ma, L.; Li, X.; Tang, H.; Li, Y.; Chen, S. A novel synchronous micro motor for intravascular ultrasound imaging. IEEE Trans. Biomed. Eng. 2018, 66, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Cagatay, S.; Koc, B.; Uchino, K. A 1.6-mm, metal tube ultrasonic motor. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2003, 50, 782–786. [Google Scholar] [CrossRef]
- Zhang, H.; Dong, S.; Zhang, S.; Wang, T.; Zhang, Z.; Fan, L. Ultrasonic micro-motor using miniature piezoelectric tube with diameter of 1.0 mm. Ultrasonics 2006, 44, e603–e606. [Google Scholar] [CrossRef]
- Tanabe, M.; Xie, S.; Tagawa, N.; Moriya, T.; Furukawa, Y. Development of a mechanical scanning-type intravascular ultrasound system using a miniature ultrasound motor. Jpn. J. Appl. Phys. 2007, 46, 4805. [Google Scholar] [CrossRef]
- Watson, B.; Friend, J.; Yeo, L. Piezoelectric ultrasonic micro/milli-scale actuators. Sensors Actuators A Phys. 2009, 152, 219–233. [Google Scholar] [CrossRef]
- Mashimo, T. Performance evaluation of a micro ultrasonic motor using a one-cubic-millimeter stator. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2015, 62, 1819–1826. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, S.; Liao, X.; Feng, Z. Construction of an intravascular ultrasound catheter with a micropiezoelectric motor internally installed. Rev. Sci. Instrum. 2021, 92, 15005. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Shin, E.-J.; Lee, C.; Chang, J.H. Development of dual-frequency oblong-shaped-focused transducers for intravascular ultrasound tissue harmonic imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2018, 65, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Munding, C.E.; Chérin, E.; Jourard, I.; Weyers, J.J.; Goertz, D.E.; Courtney, B.K.; Foster, F.S. Development of a 3 french dual-frequency intravascular ultrasound catheter. Ultrasound Med. Biol. 2018, 44, 251–266. [Google Scholar] [CrossRef] [PubMed]
- Qiu, W.; Chen, Y.; Wong, C.-M.; Liu, B.; Dai, J.; Zheng, H. A novel dual-frequency imaging method for intravascular ultrasound applications. Ultrasonics 2015, 57, 31–35. [Google Scholar] [CrossRef]
- Yoon, S.; Kim, M.G.; Williams, J.A.; Yoon, C.; Kang, B.J.; Cabrera-Munoz, N.; Shung, K.K.; Kim, H.H. Dual-element needle transducer for intravascular ultrasound imaging. J. Med. Imaging 2015, 2, 27001. [Google Scholar] [CrossRef]
- Lee, J.; Moon, J.-Y.; Chang, J.H. A 35 MHz/105 MHz dual-element focused transducer for intravascular ultrasound tissue imaging using the third harmonic. Sensors 2018, 18, 2290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Chang, J.H. Dual-element intravascular ultrasound transducer for tissue harmonic imaging and frequency compounding: Development and imaging performance assessment. IEEE Trans. Biomed. Eng. 2019, 66, 3146–3155. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Zhang, Z.; Hong, J.; Huang, Y.; Mu, P.; Yu, Y.; Liu, R.; Liang, S.; Zheng, H.; Qiu, W. Cable-shared dual-frequency catheter for intravascular ultrasound. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Szabo, T.L. Diagnostic Ultrasound Imaging: Inside Out; Academic Press: Cambridge, MA, USA, 2004; ISBN 0126801452. [Google Scholar]
- Cherin, E.W.; Poulsen, J.K.; Van Der Steen, A.F.W.; Lum, P.; Foster, F.S. Experimental characterization of fundamental and second harmonic beams for a high-frequency ultrasound transducer. Ultrasound Med. Biol. 2002, 28, 635–646. [Google Scholar] [CrossRef]
- Choudhry, S.; Gorman, B.; Charboneau, J.W.; Tradup, D.J.; Beck, R.J.; Kofler, J.M.; Groth, D.S. Comparison of tissue harmonic imaging with conventional US in abdominal disease. Radiographics 2000, 20, 1127–1135. [Google Scholar] [CrossRef]
- Anvari, A.; Forsberg, F.; Samir, A.E. A primer on the physical principles of tissue harmonic imaging. Radiographics 2015, 35, 1955–1964. [Google Scholar] [CrossRef] [PubMed]
- Bouakaz, A.; De Jong, N. Native tissue imaging at superharmonic frequencies. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2003, 50, 496–506. [Google Scholar] [CrossRef]
- Jian, X.; Han, Z.; Liu, P.; Xu, J.; Li, Z.; Li, P.; Shao, W.; Cui, Y. A high frequency geometric focusing transducer based on 1-3 piezocomposite for intravascular ultrasound imaging. Biomed Res. Int. 2017, 2017, 9327270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frijlink, M.E.; Goertz, D.E.; Van Damme, L.C.; Krams, R.; Van Der Steen, A.F.W. Intravascular ultrasound tissue harmonic imaging in vivo. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2006, 53, 1844–1852. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Li, X.; Zhou, Q.; Shung, K.K. Combined chirp coded tissue harmonic and fundamental ultrasound imaging for intravascular ultrasound: 20–60 MHz phantom and ex vivo results. Ultrasonics 2013, 53, 369–376. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Martin, K.H.; Dayton, P.A.; Jiang, X. A preliminary engineering design of intravascular dual-frequency transducers for contrast-enhanced acoustic angiography and molecular imaging. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2014, 61, 870–880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, K.H.; Lindsey, B.D.; Ma, J.; Lee, M.; Li, S.; Foster, F.S.; Jiang, X.; Dayton, P.A. Dual-frequency piezoelectric transducers for contrast enhanced ultrasound imaging. Sensors 2014, 14, 20825–20842. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Jiang, X. Contrast-Enhanced Dual-Frequency Super-Harmonic Intravascular Ultrasound (IVUS) Imaging. In Multimodality Imaging; Springer: Berlin/Heidelberg, Germany, 2020; pp. 105–151. [Google Scholar]
- Finn, A.V.; Nakano, M.; Narula, J.; Kolodgie, F.D.; Virmani, R. Concept of vulnerable/unstable plaque. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 1282–1292. [Google Scholar] [CrossRef] [Green Version]
- Kwon, H.M.; Sangiorgi, G.; Ritman, E.L.; Lerman, A.; McKenna, C.; Virmani, R.; Edwards, W.D.; Holmes, D.R.; Schwartz, R.S. Adventitial vasa vasorum in balloon-injured coronary arteries: Visualization and quantitation by a microscopic three-dimensional computed tomography technique. J. Am. Coll. Cardiol. 1998, 32, 2072–2079. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Jiang, X.; Martin, K.H.; Dayton, P.A. Small aperture, dual frequency ultrasound transducers for intravascular contrast imaging. In Proceedings of the 2013 IEEE International Ultrasonics Symposium (IUS), Prague, Czech Republic, 21–25 July 2013; IEEE: Piscataway, NJ, USA, 2013; pp. 769–772. [Google Scholar]
- Ma, J.; Jiang, X.; Martin, K.H.; Dayton, P.A.; Li, Y.; Zhou, Q. Dual frequency transducers for intravascular ultrasound super-harmonic imaging and acoustic angiography. In Proceedings of the 2014 IEEE International Ultrasonics Symposium, Chicago, IL, USA, 3–6 September 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 675–678. [Google Scholar]
- Lindsey, B.D.; Martin, K.H.; Dayton, P.A.; Ma, J.; Wang, Z.; Jiang, X. Dual-frequency intravascular ultrasound imaging of microbubble contrast agents: Ex vivo and in vivo demonstration. In Proceedings of the 2015 IEEE International Ultrasonics Symposium (IUS), Taipei, Taiwan, 21–24 October 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 1–4. [Google Scholar]
- Kim, J.; Kasoji, S.; Markley, E.; Jiang, X.; Dayton, P. Catheter-mounted dual-frequency ultrasound transducers for intravascular contrast-enhanced superharmonic imaging. J. Acoust. Soc. Am. 2019, 146, 3031. [Google Scholar] [CrossRef]
- Martin, K.H.; Lindsey, B.D.; Ma, J.; Nichols, T.C.; Jiang, X.; Dayton, P.A. Ex vivo porcine arterial and chorioallantoic membrane acoustic angiography using dual-frequency intravascular ultrasound probes. Ultrasound Med. Biol. 2016, 42, 2294–2307. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.; Steer, M.B.; Jiang, X. An acoustic filter based on layered structure. Appl. Phys. Lett. 2015, 106, 111903. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Martin, K.H.; Li, Y.; Dayton, P.A.; Shung, K.K.; Zhou, Q.; Jiang, X. Design factors of intravascular dual frequency transducers for super-harmonic contrast imaging and acoustic angiography. Phys. Med. Biol. 2015, 60, 3441. [Google Scholar] [CrossRef] [Green Version]
- Lindsey, B.D.; Martin, K.H.; Jiang, X.; Dayton, P.A. Adaptive windowing in contrast-enhanced intravascular ultrasound imaging. Ultrasonics 2016, 70, 123–135. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ma, J.; Martin, K.H.; Yu, M.; Ma, T.; Dayton, P.A.; Jiang, X.; Shung, K.K.; Zhou, Q. An integrated system for superharmonic contrast-enhanced ultrasound imaging: Design and intravascular phantom imaging study. IEEE Trans. Biomed. Eng. 2015, 63, 1933–1943. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Martin, K.H.; Huang, W.; Dayton, P.A.; Jiang, X. Contrast enhanced superharmonic imaging for acoustic angiography using reduced form-factor lateral mode transmitters for intravascular and intracavity applications. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2016, 64, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Munoz, N.E.; Eliahoo, P.; Wodnicki, R.; Jung, H.; Chiu, C.T.; Williams, J.A.; Kim, H.H.; Zhou, Q.; Shung, K.K. Forward-looking 30-MHz phased-array transducer for peripheral intravascular imaging. Sensors Actuators A Phys. 2018, 280, 145–163. [Google Scholar] [CrossRef]
- Cabrera-Munoz, N.E.; Eliahoo, P.; Wodnicki, R.; Jung, H.; Chiu, C.T.; Williams, J.A.; Kim, H.H.; Zhou, Q.; Yang, G.-Z.; Shung, K.K. Fabrication and characterization of a miniaturized 15-MHz side-looking phased-array transducer catheter. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2019, 66, 1079–1092. [Google Scholar] [CrossRef]
- Li, S.; Tian, J.; Jiang, X. A micromachined Pb (Mg1/3Nb2/3) O3-PbTiO3 single crystal composite circular array for intravascular ultrasound imaging. J. Eng. Sci. Med. Diagn. Ther. 2019, 2, 021001. [Google Scholar] [CrossRef]
- Wang, Z.; Martin, K.H.; Dayton, P.A.; Jiang, X. Real-time ultrasound angiography using superharmonic dual-frequency (2.25 MHz/30 MHz) cylindrical array: In vitro study. Ultrasonics 2018, 82, 298–303. [Google Scholar] [CrossRef]
- Wang, Z.; Huang, W.; Jiang, X.; Martin, K.H.; Dayton, P.A. Dual-frequency IVUS array for contrast enhanced intravascular ultrasound imaging. In Proceedings of the 2015 IEEE International Ultrasonics Symposium (IUS), Taipei, Taiwan, 21–24 October 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 1–4. [Google Scholar]
- Wu, H.; Li, S.; Jiang, X.; Kasoji, S.; Dayton, P.A.; Tian, J. Micromachined 1–3 composite dual frequency IVUS array for contrast enhanced intravascular ultasound imaging. In Proceedings of the 2017 IEEE International Ultrasonics Symposium (IUS), Washington, DC, USA, 6–9 September 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–4. [Google Scholar]
- Yock, P.G.; Linker, D.T.; Angelsen, B.A.J. Two-dimensional intravascular ultrasound: Technical development and initial clinical experience. J. Am. Soc. Echocardiogr. 1989, 2, 296–304. [Google Scholar] [CrossRef]
- Nissen, S.E.; Gurley, J.C.; Grines, C.L.; Booth, D.C.; McClure, R.; Berk, M.; Fischer, C.; DeMaria, A.N. Intravascular ultrasound assessment of lumen size and wall morphology in normal subjects and patients with coronary artery disease. Circulation 1991, 84, 1087–1099. [Google Scholar] [CrossRef] [Green Version]
- Calvert, P.A.; Obaid, D.R.; O’Sullivan, M.; Shapiro, L.M.; McNab, D.; Densem, C.G.; Schofield, P.M.; Braganza, D.; Clarke, S.C.; Ray, K.K. Association between IVUS findings and adverse outcomes in patients with coronary artery disease: The VIVA (VH-IVUS in Vulnerable Atherosclerosis) Study. JACC Cardiovasc. Imaging 2011, 4, 894–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, G.W.; Maehara, A.; Lansky, A.J.; De Bruyne, B.; Cristea, E.; Mintz, G.S.; Mehran, R.; McPherson, J.; Farhat, N.; Marso, S.P. A prospective natural-history study of coronary atherosclerosis. N. Engl. J. Med. 2011, 364, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Stone, P.H.; Saito, S.; Takahashi, S.; Makita, Y.; Nakamura, S.; Kawasaki, T.; Takahashi, A.; Katsuki, T.; Nakamura, S.; Namiki, A. Prediction of progression of coronary artery disease and clinical outcomes using vascular profiling of endothelial shear stress and arterial plaque characteristics: The PREDICTION Study. Circulation 2012, 126, 172–181. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [Green Version]
- Bezerra, H.G.; Costa, M.A.; Guagliumi, G.; Rollins, A.M.; Simon, D.I. Intracoronary optical coherence tomography: A comprehensive review: Clinical and research applications. JACC Cardiovasc. Interv. 2009, 2, 1035–1046. [Google Scholar] [CrossRef] [Green Version]
- Hoang, V.; Grounds, J.; Pham, D.; Virani, S.; Hamzeh, I.; Qureshi, A.M.; Lakkis, N.; Alam, M. The role of intracoronary plaque imaging with intravascular ultrasound, optical coherence tomography, and near-infrared spectroscopy in patients with coronary artery disease. Curr. Atheroscler. Rep. 2016, 18, 1–9. [Google Scholar] [CrossRef]
- Karlsson, S.; Anesäter, E.; Fransson, K.; Andell, P.; Persson, J.; Erlinge, D. Intracoronary near-infrared spectroscopy and the risk of future cardiovascular events. Open Heart 2019, 6, e000917. [Google Scholar] [CrossRef]
- Cao, Y.; Hui, J.; Kole, A.; Wang, P.; Yu, Q.; Chen, W.; Sturek, M.; Cheng, J.-X. High-sensitivity intravascular photoacoustic imaging of lipid–laden plaque with a collinear catheter design. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; van der Steen, A.F.W.; Regar, E.; van Soest, G. Emerging technology update intravascular photoacoustic imaging of vulnerable atherosclerotic plaque. Interv. Cardiol. Rev. 2016, 11, 120. [Google Scholar] [CrossRef] [Green Version]
- Calfon, M.A.; Rosenthal, A.; Mallas, G.; Mauskapf, A.; Nudelman, R.N.; Ntziachristos, V.; Jaffer, F.A. In vivo near infrared fluorescence (NIRF) intravascular molecular imaging of inflammatory plaque, a multimodal approach to imaging of atherosclerosis. J. Vis. Exp. JoVE 2011. [Google Scholar] [CrossRef] [Green Version]
- Hara, T.; Jaffer, F.A. Intravascular NIRF molecular imaging approaches in coronary artery disease. Curr. Cardiovasc. Imaging Rep. 2016, 9, 13. [Google Scholar] [CrossRef]
- Xie, H.; Bec, J.; Liu, J.; Sun, Y.; Lam, M.; Yankelevich, D.R.; Marcu, L. Multispectral scanning time-resolved fluorescence spectroscopy (TRFS) technique for intravascular diagnosis. Biomed. Opt. Express 2012, 3, 1521–1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yankelevich, D.R.; Ma, D.; Liu, J.; Sun, Y.; Sun, Y.; Bec, J.; Elson, D.S.; Marcu, L. Design and evaluation of a device for fast multispectral time-resolved fluorescence spectroscopy and imaging. Rev. Sci. Instrum. 2014, 85, 34303. [Google Scholar] [CrossRef] [Green Version]
- Bec, J.; Ma, D.M.; Yankelevich, D.R.; Liu, J.; Ferrier, W.T.; Southard, J.; Marcu, L. Multispectral Fluorescence Lifetime Imaging System for Intravascular Diagnostics with Ultrasound Guidance: In Vivo Validation in Swine Arteries. J. Biophotonics. 2014, 7, 281–285. [Google Scholar] [CrossRef] [Green Version]
- Ma, D.M.; Bec, J.; Yankelevich, D.R.; Gorpas, D.S.; Fatakdawala, H.; Marcu, L. Rotational multispectral fluorescence lifetime imaging and intravascular ultrasound: Bimodal system for intravascular applications. J. Biomed. Opt. 2014, 19, 66004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Amorim Garcia Filho, C.A.; Yehoshua, Z.; Gregori, G.; Puliafito, C.A.; Rosenfeld, P.J. Chapter 3—Optical Coherence Tomography; Ryan, S.J., Sadda, S.R., Hinton, D.R., Schachat, A.P., Sadda, S.R., Wilkinson, C.P., Wiedemann, P., Schachat, A.P.B.T.-R., Eds.; W.B. Saunders: London, UK, 2013; pp. 82–110. ISBN 978-1-4557-0737-9. [Google Scholar]
- Prati, F.; Regar, E.; Mintz, G.S.; Arbustini, E.; Di Mario, C.; Jang, I.-K.; Akasaka, T.; Costa, M.; Guagliumi, G.; Grube, E. Expert review document on methodology, terminology, and clinical applications of optical coherence tomography: Physical principles, methodology of image acquisition, and clinical application for assessment of coronary arteries and atherosclerosis. Eur. Heart J. 2010, 31, 401–415. [Google Scholar] [CrossRef] [PubMed]
- Tearney, G.J.; Regar, E.; Akasaka, T.; Adriaenssens, T.; Barlis, P.; Bezerra, H.G.; Bouma, B.; Bruining, N.; Cho, J.; Chowdhary, S. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: A report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J. Am. Coll. Cardiol. 2012, 59, 1058–1072. [Google Scholar] [CrossRef] [Green Version]
- Beć, K.B.; Huck, C.W. Breakthrough potential in near-infrared spectroscopy: Spectra simulation. A review of recent developments. Front. Chem. 2019, 7, 48. [Google Scholar] [CrossRef] [Green Version]
- Kuku, K.O.; Singh, M.; Ozaki, Y.; Dan, K.; Chezar-Azerrad, C.; Waksman, R.; Garcia-Garcia, H.M. Near-infrared spectroscopy intravascular ultrasound Imaging: State of the Art. Front. Cardiovasc. Med. 2020, 7, 107. [Google Scholar] [CrossRef] [PubMed]
- Masagounder, K.; Ramos, S.; Reimann, I.; Channarayapatna, G. 6—Optimizing Nutritional Quality of Aquafeeds; Academic Press: Cambridge, MA, USA, 2016; pp. 239–264. ISBN 978-0-12-800873-7. [Google Scholar]
- Gardner, C.M.; Tan, H.; Hull, E.L.; Lisauskas, J.B.; Sum, S.T.; Meese, T.M.; Jiang, C.; Madden, S.P.; Caplan, J.D.; Burke, A.P. Detection of lipid core coronary plaques in autopsy specimens with a novel catheter-based near-infrared spectroscopy system. JACC Cardiovasc. Imaging 2008, 1, 638–648. [Google Scholar] [CrossRef] [Green Version]
- Sethuraman, S.; Amirian, J.H.; Litovsky, S.H.; Smalling, R.W.; Emelianov, S.Y. Spectroscopic intravascular photoacoustic imaging to differentiate atherosclerotic plaques. Opt. Express 2008, 16, 3362–3367. [Google Scholar] [CrossRef] [PubMed]
- Jansen, K.; Wu, M.; van der Steen, A.F.W.; van Soest, G. Lipid detection in atherosclerotic human coronaries by spectroscopic intravascular photoacoustic imaging. Opt. Express 2013, 21, 21472–21484. [Google Scholar] [CrossRef] [Green Version]
- Jansen, K.; van der Steen, A.F.W.; Wu, M.; van Beusekom, H.M.M.; Springeling, G.; Li, X.; Zhou, Q.; Shung, K.K.; de Kleijn, D.P.V.; van Soest, G. Spectroscopic intravascular photoacoustic imaging of lipids in atherosclerosis. J. Biomed. Opt. 2014, 19, 26006. [Google Scholar] [CrossRef] [Green Version]
- Allen, T.J.; Beard, P.C.; Hall, A.; Dhillon, A.P.; Owen, J.S. Spectroscopic photoacoustic imaging of lipid-rich plaques in the human aorta in the 740 to 1400 nm wavelength range. J. Biomed. Opt. 2012, 17, 61209. [Google Scholar] [CrossRef]
- Khraishah, H.; Jaffer, F.A. Intravascular Molecular Imaging: Near-Infrared Fluorescence as a New Frontier. Front. Cardiovasc. Med. 2020, 7. [Google Scholar] [CrossRef]
- Jaffer, F.A.; Calfon, M.A.; Rosenthal, A.; Mallas, G.; Razansky, R.N.; Mauskapf, A.; Weissleder, R.; Libby, P.; Ntziachristos, V. Two-dimensional intravascular near-infrared fluorescence molecular imaging of inflammation in atherosclerosis and stent-induced vascular injury. J. Am. Coll. Cardiol. 2011, 57, 2516–2526. [Google Scholar] [CrossRef] [Green Version]
- Bourantas, C.V.; Jaffer, F.A.; Gijsen, F.J.; Van Soest, G.; Madden, S.P.; Courtney, B.K.; Fard, A.M.; Tenekecioglu, E.; Zeng, Y.; Van Der Steen, A.F.W. Hybrid intravascular imaging: Recent advances, technical considerations, and current applications in the study of plaque pathophysiology. Eur. Heart J. 2017, 38, 400–412. [Google Scholar] [CrossRef] [Green Version]
- Stephens, D.N.; Park, J.; Sun, Y.; Papaioannou, T.; Marcu, L. Intraluminal fluorescence spectroscopy catheter with ultrasound guidance. J. Biomed. Opt. 2009, 14, 30505. [Google Scholar] [CrossRef]
- Berezin, M.Y.; Achilefu, S. Fluorescence lifetime measurements and biological imaging. Chem. Rev. 2010, 110, 2641–2684. [Google Scholar] [CrossRef] [Green Version]
- Marcu, L.; Jo, J.A.; Fang, Q.; Papaioannou, T.; Reil, T.; Qiao, J.-H.; Baker, J.D.; Freischlag, J.A.; Fishbein, M.C. Detection of rupture-prone atherosclerotic plaques by time-resolved laser-induced fluorescence spectroscopy. Atherosclerosis 2009, 204, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Phipps, J.E.; Sun, Y.H.; Hatami, N.; Marcu, L.; Saroufeem, R.M.G.; Fishbein, M.C. Fluorescence lifetime imaging for the characterization of the biochemical composition of atherosclerotic plaques. J. Biomed. Opt. 2011, 16, 96018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourantas, C.V.; Garcia-Garcia, H.M.; Naka, K.K.; Sakellarios, A.; Athanasiou, L.; Fotiadis, D.I.; Michalis, L.K.; Serruys, P.W. Hybrid intravascular imaging: Current applications and prospective potential in the study of coronary atherosclerosis. J. Am. Coll. Cardiol. 2013, 61, 1369–1378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, T.; Zhou, B.; Hsiai, T.K.; Shung, K.K. A review of intravascular ultrasound-based multimodal intravascular imaging: The synergistic approach to characterizing vulnerable plaques. Ultrason. Imaging 2016, 38, 314–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katagiri, Y.; Tenekecioglu, E.; Serruys, P.W.; Collet, C.; Katsikis, A.; Asano, T.; Miyazaki, Y.; Piek, J.J.; Wykrzykowska, J.J.; Bourantas, C. What does the future hold for novel intravascular imaging devices: A focus on morphological and physiological assessment of plaque. Expert Rev. Med. Devices 2017, 14, 985–999. [Google Scholar] [CrossRef]
- Li, Y.; Chen, J.; Chen, Z. Multimodal intravascular imaging technology for characterization of atherosclerosis. J. Innov. Opt. Health Sci. 2020, 13, 2030001. [Google Scholar] [CrossRef]
- Ono, M.; Kawashima, H.; Hara, H.; Gao, C.; Wang, R.; Kogame, N.; Takahashi, K.; Chichareon, P.; Modolo, R.; Tomaniak, M. Advances in IVUS/OCT and Future Clinical Perspective of Novel Hybrid Catheter System in Coronary Imaging. Front. Cardiovasc. Med. 2020, 7. [Google Scholar] [CrossRef]
- Li, J.; Ma, T.; Jing, J.C.; Zhang, J.; Patel, P.M.; Shung, K.K.; Zhou, Q.; Chen, Z. Miniature optical coherence tomography-ultrasound probe for automatically coregistered three-dimensional intracoronary imaging with real-time display. J. Biomed. Opt. 2013, 18, 100502. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Li, J.; Jing, J.; Ma, T.; Liang, S.; Zhang, J.; Mohar, D.; Raney, A.; Mahon, S.; Brenner, M. Integrated IVUS-OCT imaging for atherosclerotic plaque characterization. IEEE J. Sel. Top. Quantum Electron. 2013, 20, 196–203. [Google Scholar]
- Waksman, R.; Di Mario, C.; Torguson, R.; Ali, Z.A.; Singh, V.; Skinner, W.H.; Artis, A.K.; Ten Cate, T.; Powers, E.; Kim, C. Identification of patients and plaques vulnerable to future coronary events with near-infrared spectroscopy intravascular ultrasound imaging: A prospective, cohort study. Lancet 2019, 394, 1629–1637. [Google Scholar] [CrossRef]
- Li, X.; Wei, W.; Zhou, Q.; Shung, K.K.; Chen, Z. Intravascular photoacoustic imaging at 35 and 80 MHz. J. Biomed. Opt. 2012, 17, 106005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Gong, X.; Liu, C.; Lin, R.; Hau, W.; Bai, X.; Song, L. High-speed intravascular spectroscopic photoacoustic imaging at 1000 A-lines per second with a 0.9-mm diameter catheter. J. Biomed. Opt. 2015, 20, 65006. [Google Scholar] [CrossRef] [PubMed]
- Piao, Z.; Ma, T.; Li, J.; Wiedmann, M.T.; Huang, S.; Yu, M.; Kirk Shung, K.; Zhou, Q.; Kim, C.-S.; Chen, Z. High speed intravascular photoacoustic imaging with fast optical parametric oscillator laser at 1.7 μ m. Appl. Phys. Lett. 2015, 107, 83701. [Google Scholar] [CrossRef] [Green Version]
- Hui, J.; Cao, Y.; Zhang, Y.; Kole, A.; Wang, P.; Yu, G.; Eakins, G.; Sturek, M.; Chen, W.; Cheng, J.-X. Real-time intravascular photoacoustic-ultrasound imaging of lipid-laden plaque in human coronary artery at 16 frames per second. Sci. Rep. 2017, 7, 1–11. [Google Scholar] [CrossRef]
- Li, Y.; Lin, R.; Liu, C.; Chen, J.; Liu, H.; Zheng, R.; Gong, X.; Song, L. In vivo photoacoustic/ultrasonic dual-modality endoscopy with a miniaturized full field-of-view catheter. J. Biophoton. 2018, 11, e201800034. [Google Scholar] [CrossRef]
- Dixon, A.J.; Hossack, J.A. Intravascular near-infrared fluorescence catheter with ultrasound guidance and blood attenuation correction. J. Biomed. Opt. 2013, 18, 56009. [Google Scholar] [CrossRef] [Green Version]
- Abran, M.; Stähli, B.E.; Merlet, N.; Mihalache-Avram, T.; Mecteau, M.; Rhéaume, E.; Busseuil, D.; Tardif, J.-C.; Lesage, F. Validating a bimodal intravascular ultrasound (IVUS) and near-infrared fluorescence (NIRF) catheter for atherosclerotic plaque detection in rabbits. Biomed. Opt. Express 2015, 6, 3989–3999. [Google Scholar] [CrossRef] [Green Version]
- Gorpas, D.; Fatakdawala, H.; Bec, J.; Ma, D.; Yankelevich, D.R.; Qi, J.; Marcu, L. Fluorescence lifetime imaging and intravascular ultrasound: Co-registration study using ex vivo human coronaries. IEEE Trans. Med. Imaging 2014, 34, 156–166. [Google Scholar] [CrossRef] [Green Version]
- Liang, S.; Ma, T.; Jing, J.; Li, X.; Li, J.; Shung, K.K.; Zhou, Q.; Zhang, J.; Chen, Z. Trimodality imaging system and intravascular endoscopic probe: Combined optical coherence tomography, fluorescence imaging and ultrasound imaging. Opt. Lett. 2014, 39, 6652–6655. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Jing, J.; Qu, Y.; Miao, Y.; Zhang, B.; Ma, T.; Yu, M.; Zhou, Q.; Chen, Z. Fully integrated optical coherence tomography, ultrasound, and indocyanine green-based fluorescence tri-modality system for intravascular imaging. Biomed. Opt. Express 2017, 8, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Dai, X.; Yang, H.; Shan, T.; Xie, H.; Berceli, S.A.; Jiang, H. Miniature endoscope for multimodal imaging. ACS Photon. 2017, 4, 174–180. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IVUS | VH-IVUS | iMapTM | IB-IVUS | |
|---|---|---|---|---|
| Type of device | Mechanical and electrical | Mechanical and electrical | Mechanical | Mechanical |
| Transducer frequency | 20–60 MHz | 20–45 MHz | 40 MHz | 40 MHz |
| Color code | Grayscale | Fibrous: green Fibro-fatty: light green Necrotic core: red Dense calcium: white | Fibrotic: light green Lipidic: yellow Necrotic: pink Calcified: blue | Fibrosis: light green Dense fibrosis: yellow Lipid: blue Calcified: red |
| Backscatter radiofrequency signal analysis | Amplitude (dB) | Autoregressive model | Fast Fourier Transformation | Fast Fourier Transformation |
| Manufacturer | Product Name | Transducer Frequency | Distal Shaft Profile | Proximal Shaft Profile | Transducer to Tip Length | Axial Resolution | Transducer Type |
|---|---|---|---|---|---|---|---|
| Boston scientific | OptiCrossTM | 40 MHz | 2.6 Fr | 3.1 Fr | 20 mm | 38 µm | Rotational |
| OptiCrossTM 6 | 40 MHz | 2.9 Fr | 3.1 Fr | 20 mm | 38 µm | Rotational | |
| OptiCrossTM 18 | 30 MHz | 2.9 Fr | 3.5 Fr | 20 mm | N/A | Rotational | |
| OptiCrossTM 35 | 15 MHz | 6 Fr | 8 Fr | 10 mm | N/A | Rotational | |
| OptiCrossTM HD | 60 MHz | 2.6 Fr | 3.1 Fr | 20 mm | 22 µm | Rotational | |
| Philip (Volcano) | Eagle Eye® | 20 MHz | 3.3 Fr | 2.9 Fr | 10 mm | <170 µm | Phased array |
| Revolution® | 45 MHz | 3.2 Fr | 3.5 Fr | 30 mm | 50 µm | Rotational | |
| Refinity® | 45 MHz | 3.0 Fr | 3.0 Fr | 20.5 mm | 50 µm | Rotational | |
| Terumo | View IT® | 40 MHz | 2.6 Fr | 3.2 Fr | 29 mm | 69 µm | Rotational |
| AltaView® | 60 MHz | 2.6 Fr | 3.2 Fr | 24 mm | <30 µm | Rotational | |
| AnteOwl WR® | 40 MHz | 2.6 Fr | 3.1 Fr | 8 mm | N/A | Rotational | |
| Navifocus WR® | 40 MHz | 2.5 Fr | 3.1 Fr | 9 mm | N/A | Rotational | |
| Intrafocus WR® | 40 MHz | 2.8 Fr | 3.2 Fr | 30 mm | N/A | Rotational | |
| Infraredx | DualproTM | 50 MHz | 3.2 Fr | 3.6 Fr | 20 mm | 40 µm | Rotational |
| ACIST | Kodama® | 40/60 MHz | 3.2 Fr | 3.6 Fr | 20 mm | 40 µm | Rotational |
| Type | Principle | Feature | IVUS Image Quality | Advantage | Disadvantage |
|---|---|---|---|---|---|
| Mechanical/rotational catheter | A single element ultrasound transducer rotates mechanically inside an echolucent distal sheath. |
| Higher image resolution due to the higher frequencies and larger effective aperture size. |
|
|
| Solid-state catheter | A phased-array ultrasound transducer is activated sequentially in a circular way. |
| Larger scanning depth due to the lower ultrasound frequency. |
|
|
| Ultrasound Transducer | Transducer Type | Frequency | Aperture Size | Penetration Depth | Axial Resolution | Lateral Resolution |
|---|---|---|---|---|---|---|
| PMUT | 2D array [62] | 5 MHz | 1.1 mm × 6.3 mm | 30 mm | 500 µm | 1 mm |
| CMUT | 1D array [66] | 35.6 MHz | 0.3 mm × 1.0 mm | 2.4 mm | N/A | 277 µm |
| 1D array [68] | 20.8 MHz | Diameter 2.97 mm | 16 mm | 55 µm | 0.035 rad | |
| 1D array [68] | 5 MHz | Diameter 2.97 mm | 71 mm | 440 µm | 0.12 rad | |
| 2D dual-ring array [72] | 20.1 MHz | Outer diameter 1.4 mm | 4–8.2 mm | 92 µm | 251 µm | |
| Piezoelectric transducer | Single element [74] | 30 MHz | 0.5 mm × 0.5 mm | 5 mm | 46.0 µm | 231.5 µm |
| 90 MHz | 2 mm | 21.5 µm | 123.5 µm | |||
| 120 MHz | 1 mm | 25.7 µm | 105.3 µm | |||
| 150 MHz | 0.5 mm | 17.2 µm | 87.3 µm |
| Piezoelectric Material | Aperture Size | Frequency | −6 dB Bandwidth | Penetration Depth | Axial Resolution | Lateral Resolution |
|---|---|---|---|---|---|---|
| PMN-PT [78] | 0.4 mm × 0.4 mm | 80 MHz | 65% | 2 mm | 35 µm | 176 µm |
| PMN-PT [79] | 0.49 mm × 0.4 mm | 60 MHz | 60.2% | ~5 mm | 24.8 µm | 156.1 µm |
| PMN-PT [80] | 0.4 mm × 0.5 mm | 45 MHz | 61% | 5 mm | 41.6 µm | 214.7 µm |
| PNN-PZT [81] | 0.33 mm × 0.33 mm | 40 MHz | 79% | N/A | 36 µm | 141 µm |
| PMN-PT [82] | 1.2 mm × 1.2 mm Focused | 35 MHz | 54% | N/A | 34.5 µm | 392 µm |
| PMN-PT [83] | 0.57 mm × 0.57 mm 60° Focused | 45 MHz | 72% | N/A | 25 µm | 120 µm |
| PZT [84] | 0.5 mm × 1.0 mm Focused | 50 MHz | 57% | N/A | N/A | 150 µm |
| BZT-50BCT [87] | 0.8 mm × 0.8 mm | 30 MHz | 53% | N/A | N/A | N/A |
| Li doped KNN [88] | 0.4 mm × 0.4 mm | 50 MHz | 61.5% | N/A | N/A | N/A |
| PIN-PMN-PT 1-3 composite [96] | 0.5 mm × 0.4 mm | 40 MHz | 86% | N/A | 43 µm | 226 µm |
| PZT-5H 1-3 composite [100] | 0.5 mm × 0.6 mm | 50 MHz | 68.8% | N/A | 22 µm | N/A |
| PZT-5H 1-3 composite [101] | 0.5 mm × 0.6 mm | 50 MHz | 56.9% | N/A | 26.7 µm | 120.1 µm |
| PMN-PT 1-3 composite [103] | 0.5 mm × 0.5 mm | 34 MHz | 72% | N/A | 92 µm | 135 µm |
| Study | Transducer Configuration | Frequency | Aperture Size | Piezoelectric Material | Axial Resolution | Lateral Resolution | Penetration Depth | |
|---|---|---|---|---|---|---|---|---|
| Qiu et al. [112] | Side-by-side | Low | 36 MHz | 0.7 mm × 0.7 mm | PMN-PT | 78 µm | 132 µm | N/A |
| High | 78 MHz | 0.35 mm × 0.35 mm | PMN-PT | 34 µm | 106 µm | N/A | ||
| Yoon et al. [113] | Side-by-side | Low | 48 MHz | 0.57 mm × 0.57 mm | PMN-PT | 27 µm | 122 µm | N/A |
| High | 152 MHz | 0.57 mm × 0.57 mm | LiNbO3 | 14 µm | 40 µm | N/A | ||
| Lee et al. [114] | Side-by-side Oblong shaped focused | Low | 35 MHz | 0.5 mm × 0.5 mm | PZT-5H | 40 µm | 153 µm | N/A |
| High | 105 MHz | 0.5 mm × 0.5 mm | LiNbO3 | 25 µm | 46 µm | <1 mm | ||
| Lee et al. [115] | Side-by-side | Low | 35 MHz | 0.5 mm × 0.5 mm | PZT-5H | 104 µm | 180 µm | N/A |
| High | 70 MHz | 0.5 mm × 0.5 mm | PZT-5H | 28 µm | 65 µm | N/A | ||
| Ma et al. [74] | Back-to-back | Low | 35 MHz | 0.5 mm × 0.5 mm | PMN-PT | 46.0 µm | 231.5 µm | 5 mm |
| High | 150 MHz | 0.5 mm × 0.5 mm | LiNbO3 | 17.2 µm | 87.3 µm | 0.5 mm | ||
| Munding et al. [111] | Back-to-back | Low | 30 MHz | 0.5 mm × 0.5 mm | PZT-5H | 50 µm | 224 µm | >5 mm |
| High | 80 MHz | 0.27 mm × 0.27 mm | PZT-5H | 16 µm | 120 µm | <3 mm | ||
| Su et al. [116] | Back-to-back | Low | 35 MHz | 0.4 mm × 0.6 mm | PZT-5H | 37 µm | 199 µm | 4 mm |
| High | 80 MHz | 0.3 mm × 0.4 mm | PZT-5H | 19 µm | 128 µm | 0.95 mm | ||
| Study | Transducer Configuration | Frequency | Aperture Size | Piezoelectric Material | Image Types | Axial Resolution | Lateral Resolution | |
|---|---|---|---|---|---|---|---|---|
| Lee et al. [110] | Dual frequency Three elements formed a spherical shape | Low | 35 MHz | 0.5 mm × 0.5 mm | PZT-5H | Fundamental | 75.5 µm | 330 µm |
| High | 70 MHz | 0.5 mm × 0.5 mm | PZT-5H | Fundamental | 68.1 µm | 110 µm | ||
| Second harmonic | 31.1 µm | 70 µm | ||||||
| Lee et al. [114] | Dual frequency Dual elements formed a spherical shape | Low | 35 MHz | 0.5 mm × 0.5 mm | PZT-5H | Fundamental | 40 µm | 153 µm |
| High | 105 MHz | 0.5 mm × 0.5 mm | LiNbO3 | Fundamental | 25 µm | 46 µm | ||
| Third harmonic | 25 µm | 46 µm | ||||||
| Lee et al. [115] | Dual frequency Dual elements spherically deformed | Low | 30 MHz | 0.5 mm × 0.5 mm | PZT-5H | Fundamental | 70 µm | 215 µm |
| High | 70 MHz | 0.5 mm × 0.5 mm | PZT-5H | Fundamental | 30 µm | 112 µm | ||
| Second harmonic | 32 µm | 155 µm | ||||||
| Ma et al. [125] | Dual frequency Dual element stacked vertically | Low | 6.5 MHz | 0.6 mm × 3 mm | PMN-PT | Superharmonic | 35 µm | N/A |
| High | 30 MHz | 0.6 mm × 0.5 mm | PMN-PT | |||||
| Martin et al. [134] | Dual frequency Dual element stacked vertically | Low | 5.5 MHz | 0.6 mm × 3 mm | PMN-PT | Superharmonic | N/A | N/A |
| High | 37 MHz | 0.6 mm × 0.5 mm | PMN-PT | |||||
| Li et al. [138] | Dual frequency Dual element stacked vertically | Low | 6 MHz | 0.6 mm × 3 mm | PMN-PT | Superharmonic | N/A | N/A |
| High | 35 MHz | 0.6 mm × 0.5 mm | PMN-PT | |||||
| Wang et al. [139] | Dual frequency Dual element stacked vertically | Low | 2.25 MHz | 0.37 mm × 5 mm | PMN-PT | Superharmonic | 40 µm | N/A |
| High | 30 MHz | 0.37 mm × 0.6 mm | PMN-PT | |||||
| Imaging Modality | Fibrous Cap Thickness (<65 µm) | Lipid Pool Composition | Dimension Assessment | Inflammatory Reaction |
|---|---|---|---|---|
| IVUS | Poor | Necrotic core, microcalcifications, positive arterial remodeling | Excellent | Poor |
| OCT | Excellent | Microcalcifications, neo-angiogenesis, fibrous cup disruption, erosion and thrombus | Moderate | Excellent |
| NIRS | Moderate | Necrotic core | Poor | Not applicable |
| IVPA | Poor | Necrotic core | Poor | Moderate |
| NIRF | Poor | Necrotic core | Poor | Excellent |
| TRFS (FLIM) | Moderate | Necrotic core | Poor | Moderate |
| Imaging Modality | Characteristics of Vulnerable Plaques | Current Status | |||||
|---|---|---|---|---|---|---|---|
| Lumen Size | Plaque Burden | Lipid Pool | Fibrous Cap Thickness | Neo-Angiogenesis | Inflammation | ||
| IVUS-OCT | Excellent | Excellent | Moderate | Excellent | Moderate | Poor | Commercially available |
| IVUS-NIRS | Excellent | Excellent | Excellent | Moderate | Not applicable | Not applicable | Commercially available |
| IVUS-IVPA | Excellent | Excellent | Moderate | Poor | Poor | Moderate | In vivo validation |
| IVUS-NIRF | Excellent | Excellent | Poor | Poor | Not applicable | Excellent | In vivo validation |
| IVUS-TRFS (FLIM) | Excellent | Excellent | Moderate | Excellent | Not applicable | Moderate | In vivo validation |
| IVUS-OCT-NIRF | Excellent | Excellent | Moderate | Excellent | Moderate | Excellent | Under development |
| IVUS-OCT-IVPA | Excellent | Excellent | Moderate | Excellent | Moderate | Moderate | Under development |
| Imaging Modality | Catheter Size | Transducer-Probe Arrangement | Transducer-Probe Parameter | Image Resolution | Penetration Depth | Frame Rate |
|---|---|---|---|---|---|---|
| IVUS-OCT | 3.3 Fr [185] (Conavi Medical) | Co-linear arrangement | IVUS: 40 MHz OCT: 1310 nm | N/A | N/A | 100/s (hybrid use) |
| 3.2 Fr [185] (Terumo) | Sequential arrangement | IVUS: 40 MHz OCT: 1300 nm | IVUS: 200 µm OCT: 15 µm | N/A | 100–160/s (hybrid use) | |
| 2.7 Fr [186] | Back-to-back | IVUS: 45 MHz OCT: N/A | N/A | N/A | 10/s | |
| 3.6 Fr [187] | Side-by-side | IVUS: 40MHz OCT: 1310 nm | IVUS: 57 µm OCT: 8 µm | N/A | 20/s | |
| IVUS-NIRS | 3.2 Fr [188] | IVUS transducer and NIRS optics at 180° apart | IVUS: 40 MHz NIRS: 800–2500 nm | IVUS: >100 µm | IVUS: 8 mm NIRS: ~5 mm | IVUS: 16/s NIRS: 160 spectra/s |
| IVUS-IVPA | 3.6 Fr [189] | Parallel alignment | IVUS: 35 MHz IVPA: 532 nm | IVUS: 59 µm | IVUS: 5 mm | N/A |
| 3.6 Fr [189] | Parallel alignment | IVUS: 80 MHz IVPA: 532 nm | IVUS: 35 µm | IVUS: 4 mm | N/A | |
| 2.7 Fr [190] (Core size) | Sequential arrangement | IVUS: 40 MHz IVPA: 1210 nm | IVUS: 100 µm IVPA: 100 µm | IVUS: 4.5 mm IVPA: 4.5 mm | 5/s | |
| 3 Fr [191] (Core size) | Sequential arrangement | IVUS: 45 MHz IVPA: 1725 nm | IVUS: 52 µm IVPA: 60 µm | N/A | 1/s | |
| 3 Fr [192] (Core size) | Parallel alignment | IVUS: 40 MHz IVPA: 1725 nm | IVPA: 81 µm | N/A | 25/s | |
| 7.5 Fr [193] | Parallel alignment | IVUS: 40 MHz IVPA: 532 nm | IVUS: 36.3 µm IVPA: 48.5 µm | N/A | 5/s | |
| IVUS-NIRF | 4.2 Fr [194] | Side-by-side | IVUS: 45 MHz NIRF: 750 nm | N/A | IVUS: 4 mm NIRF: 2 mm | 30/s |
| 4.2 Fr [195] | Side-by-side | IVUS: 45 MHz NIRF: 780 nm | N/A | N/A | 10/s | |
| IVUS-TRFS (FLIM) | 7 Fr [161] | Side-by-side | IVUS: 40 MHz FLIM: 300 nm | N/A | N/A | IVUS: 30/s FLIM: 6.7/s |
| 5 Fr [162] | Side-by-side | IVUS: 40 MHz FLIM: 390–629 nm | FLIM: 160 µm | N/A | IVUS: 30/s FLIM: 40/s | |
| 3.7 Fr [196] | Side-by-side | IVUS: 40 MHz FLIM: 355 nm | N/A | N/A | IVUS: 30/s FLIM: 150/s | |
| IVUS-OCT-NIRF | 3.6 Fr [197] | Side-by-side | IVUS: 45 MHz OCT: 1310 nm NIRF: 635 nm | IVUS: 40 µm OCT: 8 µm | N/A | 10/s |
| 3.9 Fr [198] | Side-by-side | IVUS: 40 MHz OCT: 1310 nm NIRF: 785 nm | N/A | N/A | 20/s | |
| IVUS-OCT-IVPA | 6 Fr [199] | Side-by-side | IVUS: 40 MHz OCT: 1310 nm IVPA: 1250–1600 nm | N/A | >5 mm | 20/s |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, C.; Wu, H.; Kim, S.; Dai, X.; Jiang, X. Recent Advances in Transducers for Intravascular Ultrasound (IVUS) Imaging. Sensors 2021, 21, 3540. https://doi.org/10.3390/s21103540
Peng C, Wu H, Kim S, Dai X, Jiang X. Recent Advances in Transducers for Intravascular Ultrasound (IVUS) Imaging. Sensors. 2021; 21(10):3540. https://doi.org/10.3390/s21103540
Chicago/Turabian StylePeng, Chang, Huaiyu Wu, Seungsoo Kim, Xuming Dai, and Xiaoning Jiang. 2021. "Recent Advances in Transducers for Intravascular Ultrasound (IVUS) Imaging" Sensors 21, no. 10: 3540. https://doi.org/10.3390/s21103540