
Indigenous Knowledge on the Uses, Sustainability and Conservation of African Ginger (Siphonochilus aethiopicus) among Two Communities in Mpumalanga Province, South Africa



Abstract
:1. Introduction
- What are the traditional uses of African ginger?
- Which traditional approaches are adopted for harvesting African ginger from natural environment?
- How are indigenous strategies and practices used to conserve African ginger?
2. Materials and Methods
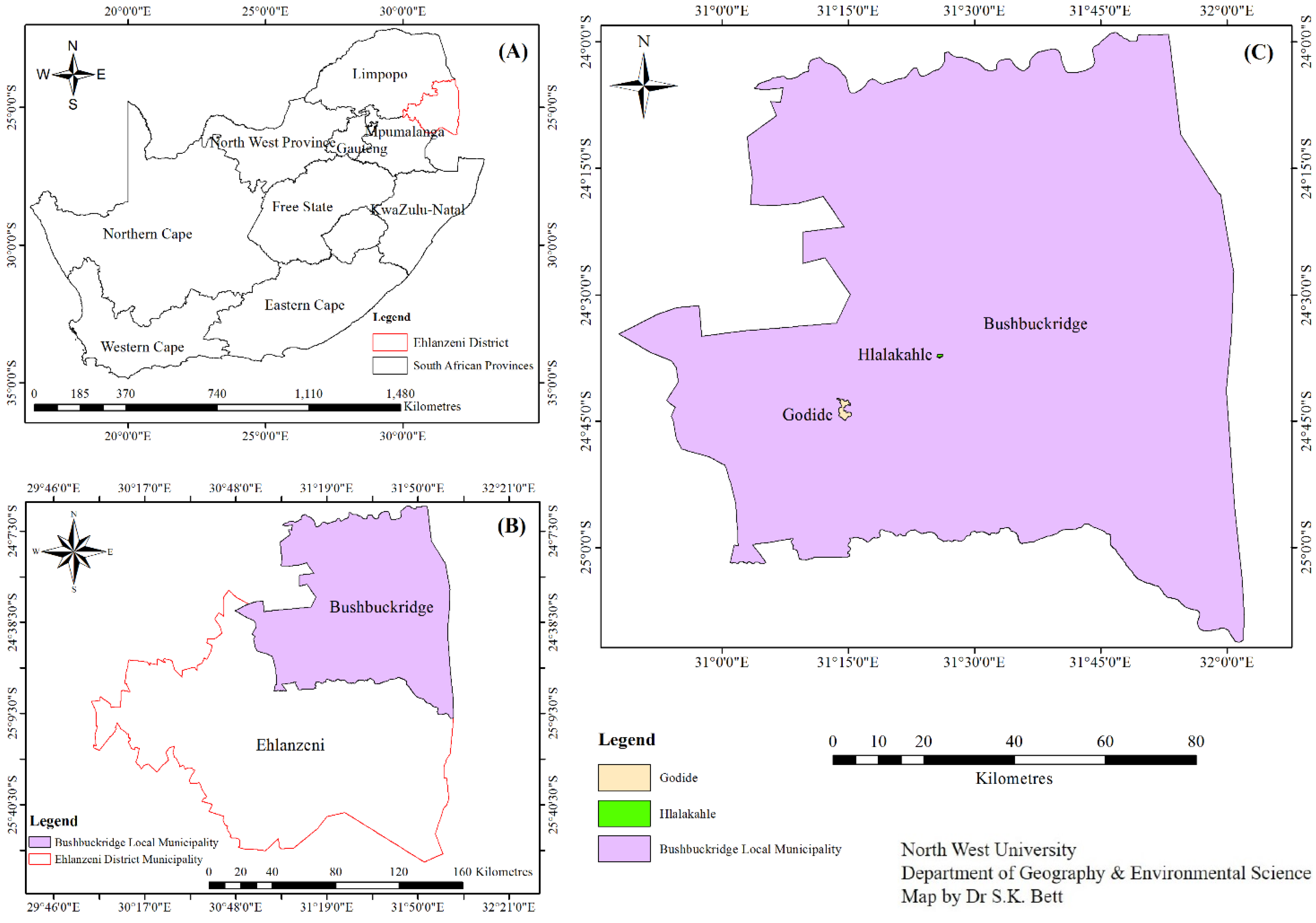
2.1. Description of the Study Area
2.2. Data Collection and Analysis
2.3. Ethics Approval
3. Results and Discussion
3.1. Demography of the Participants
3.2. Sources of Indigenous Knowledge on African Ginger
3.3. Indigenous Uses of African Ginger
3.3.1. Medicinal Uses of African Ginger
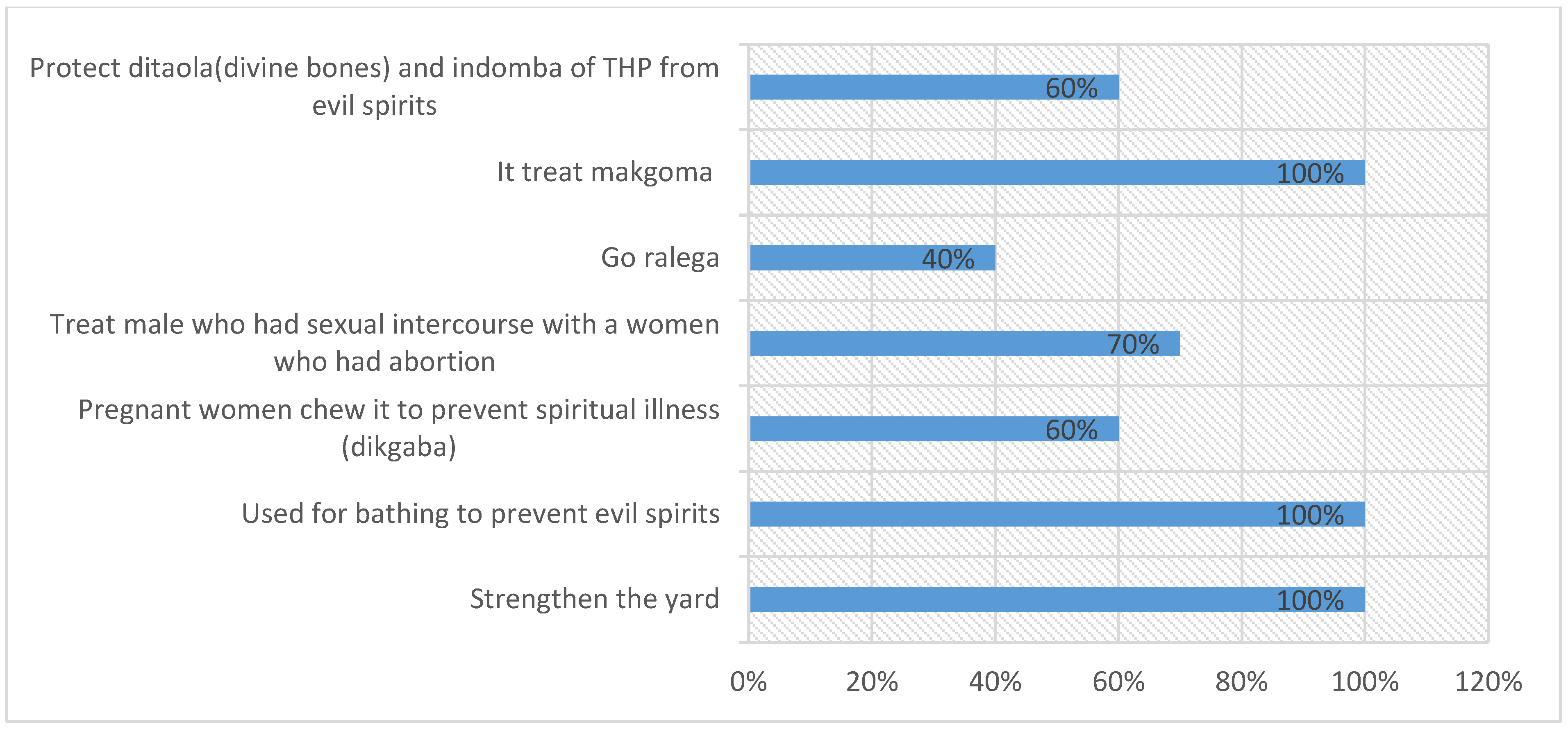
3.3.2. Spiritual and Cultural Uses of African Ginger
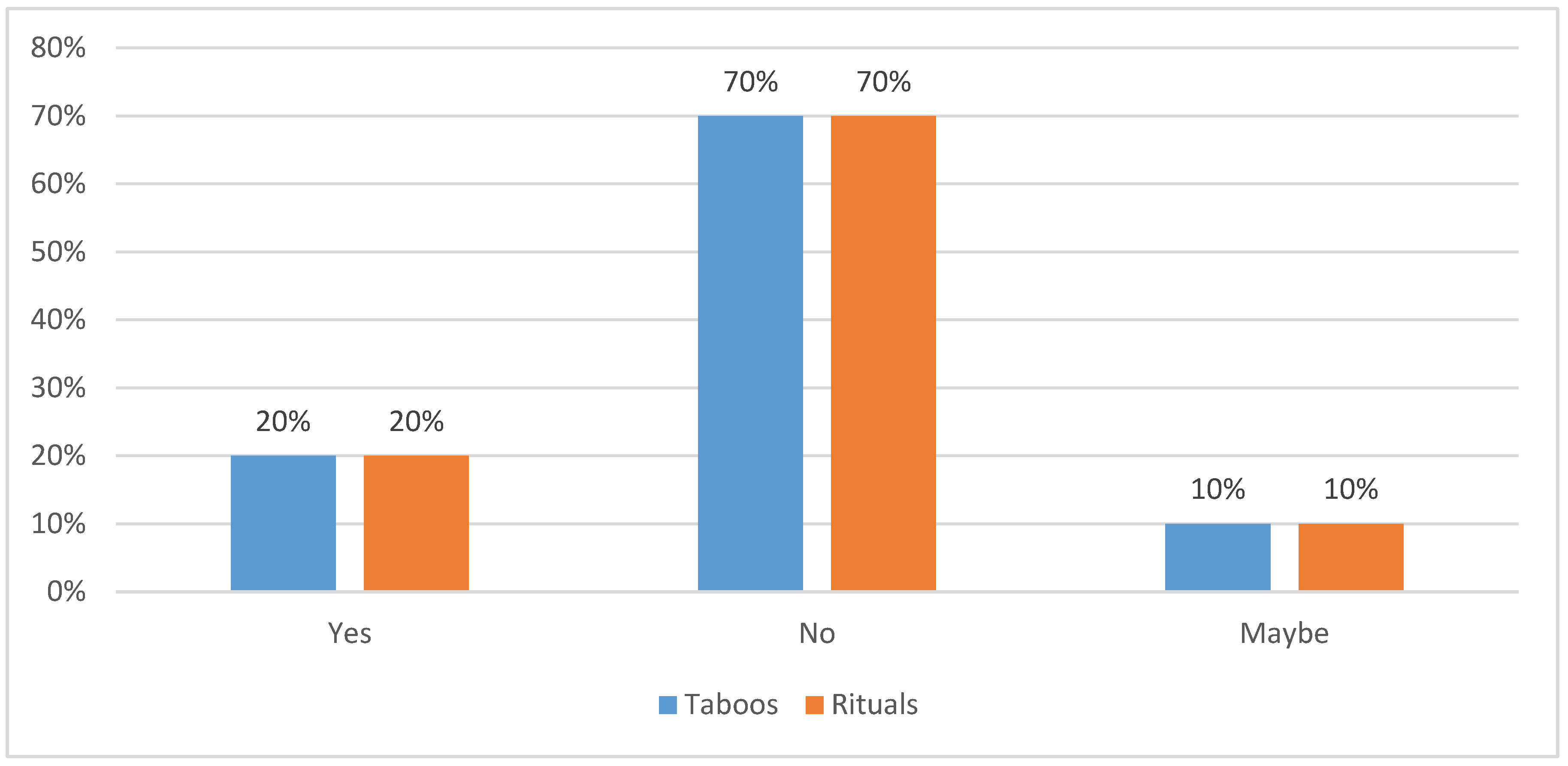
3.4. Indigenous Protocols for Harvesting of African Ginger
3.5. Indigenous Conservation Methods for African Ginger
3.6. Preservation Methods for African Ginger
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alberts, R.; Khalala, G.; Molefe, O. Collecting structured indigenous knowledge for enhanced exploration: The National Recordal System (NRS), South Africa. Knowl. Manag. Dev. J. 2011, 7, 291–307. [Google Scholar] [CrossRef]
- Lwoga, E.T.; Ngulube, P.; Stilwell, C. Understanding indigenous knowledge: Bridging the knowledge gap through a knowledge creation model for agricultural development. S. Afr. J. Inf. Manag. 2010, 12, 436–444. [Google Scholar] [CrossRef] [Green Version]
- Gadgil, M.; Berkes, F.; Folke, C. Indigenous Knowledge for Biodiversity Conservation. Ambio 1993, 22, 151–156. [Google Scholar]
- Mathibela, M.K.; Egan, B.A.; Du Plessis, H.J.; Potgieter, M.J. Socio-cultural profile of Bapedi traditional healers as indigenous knowledge custodians and conservation partners in the Blouberg area, Limpopo Province, South Africa. J. Ethnobiol. Ethnomed. 2015, 11, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahlberg, A.C.; Trygger, S.B. Indigenous medicine and primary health care: The importance of lay knowledge and use of medicinal plants in rural South Africa. Hum. Ecol. 2009, 37, 79–94. [Google Scholar] [CrossRef]
- Chakale, M.V.; Mwanza, M.; Aremu, A.O. Ethnoveterinary knowledge and biological evaluation of plants used for mitigating cattle diseases: A critical insight into the trends and patterns in South Africa. Front. Vet. Sci. 2021, 8, 710884. [Google Scholar] [CrossRef] [PubMed]
- Ndhlovu, P.T.; Omotayo, A.O.; Otang-Mbeng, W.; Aremu, A.O. Ethnobotanical review of plants used for the management and treatment of childhood diseases and well-being in South Africa. S. Afr. J. Bot. 2021, 137, 197–215. [Google Scholar] [CrossRef]
- McGaw, L.J.; Famuyide, I.M.; Khunoana, E.T.; Aremu, A.O. Ethnoveterinary botanical medicine in South Africa: A review of research from the last decade (2009 to 2019). J. Ethnopharmacol. 2020, 257, 112864. [Google Scholar] [CrossRef]
- Moyo, M.; Aremu, A.O.; van Staden, J. Ethnopharmacology in Sub-Sahara Africa: Current Trends and Future Perspectives. In Ethnopharmacology; Heinrich, M., Jäger, A.K., Eds.; Wiley Blackwell: West Sussex, UK, 2015; pp. 263–278. [Google Scholar]
- Malangu, N. Self-reported use of traditional, complementary and over-the-counter medicines by HIV-infected patients on antiretroviral therapy in Pretoria, South Africa. Afr. J. Tradit. Complemen. Altern. Med. 2007, 4, 273–278. [Google Scholar] [CrossRef] [Green Version]
- Gqaleni, N.; Moodley, I.; Kruger, H.; Ntuli, A.; McLeod, H. Traditional and complementary medicine care delivery. S. Afr. Health Rev. 2007, 2007, 175–188. [Google Scholar]
- Light, M.E.; Sparg, S.G.; Stafford, G.I.; Van Staden, J. Riding the wave: South Africa’s contribution to ethnopharmacological research over the last 25 years. J. Ethnopharmacol. 2005, 100, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Maundu, P.; Kariuki, P.; Eyog-Matig, O. Threats to medicinal plant species—An African perspective. In Conserving Medicinal Species: Securing a Healthy Future; Miththapala, S., Ed.; International Union for Conservation of Nature and Natural Resources (IUCN), Ecosystems and Livelihoods Group: Colombo, Sri Lanka, 2006; pp. 47–63. [Google Scholar]
- McGeoch, L.; Gordon, I.; Schmitt, J. Impacts of land use, anthropogenic disturbance, and harvesting on an African medicinal liana. Biol. Conserv. 2008, 141, 2218–2229. [Google Scholar] [CrossRef]
- Van Andel, T.R.; Croft, S.; van Loon, E.E.; Quiroz, D.; Towns, A.M.; Raes, N. Prioritizing West African medicinal plants for conservation and sustainable extraction studies based on market surveys and species distribution models. Biol. Conserv. 2015, 181, 173–181. [Google Scholar] [CrossRef]
- Wiersum, K.F.; Dold, A.P.; Husselman, M.; Cocks, M. Cultivation of medicinal plants as a tool for biodiversity conservation and poverty alleviation in the Amatola region, South Africa. In Medicinal and Aromatic Plants; Bogers, R.J., Craker, L.E., Lange, D., Eds.; Springer: Dordrecht, The Nertherlands, 2006; pp. 43–57. [Google Scholar]
- Mander, M. An overview of the medicinal plant market in South Africa. In Journal Indigenous Forests and Woodlands in South Africa: Policy, People and Practice; University of KwaZulu-Natal Press: Scottsville, South Africa, 2004; pp. 440–445. [Google Scholar]
- Botha, J.; Witkowski, E.T.; Shackleton, C.M. Market profiles and trade in medicinal plants in the Lowveld, South Africa. J. Environ. Conserv. 2004, 31, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Williams, V.L.; Victor, J.E.; Crouch, N.R. Red Listed medicinal plants of South Africa: Status, trends, and assessment challenges. S. Afr. J. Bot. 2013, 86, 23–35. [Google Scholar] [CrossRef] [Green Version]
- Tshisikhawe, M.P. Trade of Indigenous Medicinal Plants in the Northern Province, Venda Region: Their Ethnobotanical Importance and Sustainable Use; University of Venda for Science and Technology: Thohoyandou, South Africa, 2002. [Google Scholar]
- Mander, M. Marketing of Indigenous Medicinal Plants in South Africa: A Case Study in KwaZulu-Natal; Food and Agriculture Organization: Rome, Italy, 1998. [Google Scholar]
- Botha, J. Perceptions of Species Availability and Values of Medicinal Plants Traded in Areas Adjacent to the Kruger National Park. Ph.D. Thesis, University of the Witwatersrand, Johannesburg, South Africa, 2001. [Google Scholar]
- Moyo, M.; Aremu, A.O.; Van Staden, J. Medicinal plants: An invaluable, dwindling resource in sub-Saharan Africa. J. Ethnopharmacol. 2015, 174, 595–606. [Google Scholar] [CrossRef] [PubMed]
- Adebayo, S.A.; Amoo, S.O.; Mokgehle, S.N.; Aremu, A.O. Ethnomedicinal uses, biological activities, phytochemistry and conservation of African ginger (Siphonochilus aethiopicus): A commercially important and endangered medicinal plant. J. Ethnopharmacol. 2021, 266, 113459. [Google Scholar] [CrossRef]
- Makhuvha, N.; Van Wyk, B.-E.; Van der Bank, H.; Van der Bank, M. Genetic polymorphism in wild and cultivated Siphonochilus aethiopicus (Zingiberaceae). Biochem. Syst. Ecol. 1997, 25, 343–351. [Google Scholar] [CrossRef]
- Mokgehle, S.N. Variations in Growth, Yield and Metabolites of African Ginger (Siphonochilus aethiopicus) in Responses to Irrigation Regimes and Nitrogen Levels. Ph.D. Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2017. [Google Scholar]
- Gatabazi, A.; Marais, D.; Steyn, M.J.; Araya, H.T.; Mofokeng, M.M.; Mokgehle, S.N. Evaluating growth, yield, and water use efficiency of African and commercial ginger species in South Africa. Water 2019, 11, 548. [Google Scholar] [CrossRef] [Green Version]
- Hartzell, J.F. Response of the Endangered Medicinal Plant: Siphonochilus aethiopicus (Schweif) BL Burt. to Agronomic Practices. Master’s Thesis, University of KwaZulu-Natal, Pietermaritzburg, South Africa, 2011. [Google Scholar]
- Manzini, T.Z. Production of Wild Ginger (Siphonochilus aethiopicus) under Protection and Indigenous Knowledge of the Plant from Traditional Healers. Ph.D. Thesis, University of Pretoria, Pretoria, South Africa, 2007. [Google Scholar]
- Constant, N.L.; Tshisikhawe, M.P. Hierarchies of knowledge: Ethnobotanical knowledge, practices and beliefs of the Vhavenda in South Africa for biodiversity conservation. J. Ethnobiol. Ethnomed. 2018, 14, 56. [Google Scholar] [CrossRef]
- Izidine, S.A.; Siebert, S.J.; van Wyk, A.E.; Zobolo, A.M. Taboo and political authority in conservation policy: A case study of the Licuáti forest in Maputaland, Mozambique. J. Study Relig. Nat. Cult. 2008, 2, 373–390. [Google Scholar]
- Magoro, M.D.; Masoga, M.A.; Mearns, M.A. Traditional health practitioners’ practices and the sustainability of extinction-prone traditional medicinal plants. Int. J. Afr. Renaiss. Stud. 2010, 5, 229–241. [Google Scholar] [CrossRef]
- Quiroz, D.; van Andel, T. Evidence of a link between taboos and sacrifices and resource scarcity of ritual plants. J. Ethnobiol. Ethnomedicine 2015, 11, 5. [Google Scholar] [CrossRef] [Green Version]
- Molobela, L. Exploring Black Rural Bushbuck Ridge Women’s Constructions and Perceptions of the Practise of Abortion; University of South Africa: Pretoria, South Africa, 2017. [Google Scholar]
- Mavungu, E.M. Frontiers of Prosperity and Power: Explaining Provincial Boundary Disputes in Post Apartheid South Africa. Ph.D. Thesis, University of the Witwatersrand, Johannesburg, South Africa, 2011. [Google Scholar]
- Statistics, S.A. The South Africa I know, the Home I Understand; Statistics South Africa: Pretoria, South Africa, 2011. [Google Scholar]
- Samal, P.K.; Dhyani, P.P. Gender in the management of indigenous knowledge: Reflections from Indian Central Himalaya. Curr. Sci. 2006, 91, 104–108. [Google Scholar]
- Mokganya, M.G.; Tshisikhawe, M.P. Medicinal uses of selected wild edible vegetables consumed by Vhavenda of the Vhembe District Municipality, South Africa. S. Afr. J. Bot. 2019, 122, 184–188. [Google Scholar] [CrossRef]
- Da Costa, F.V.; Guimarães, M.F.M.; Messias, M.C.T.B. Gender differences in traditional knowledge of useful plants in a Brazilian community. PLoS ONE 2021, 16, e0253820. [Google Scholar] [CrossRef]
- Teklehaymanot, T.; Giday, M.; Medhin, G.; Mekonnen, Y. Knowledge and use of medicinal plants by people around Debre Libanos monastery in Ethiopia. J. Ethnopharmacol. 2007, 111, 271–283. [Google Scholar] [CrossRef]
- Moichwanetse, B.I.; Ndhlovu, P.T.; Sedupane, G.; Aremu, A.O. Ethno-veterinary plants used for the treatment of retained placenta and associated diseases in cattle among Dinokana communities, North West Province, South Africa. S. Afr. J. Bot. 2020, 132, 108–116. [Google Scholar] [CrossRef]
- Semenya, S.S.; Potgieter, M.J. Bapedi traditional healers in the Limpopo Province, South Africa: Their socio-cultural profile and traditional healing practice. J. Ethnobiol. Ethnomed. 2014, 10, 4. [Google Scholar] [CrossRef] [Green Version]
- Maluleka, J.R. Acquisition, transfer and preservation of indigenous knowledge by traditional healers in the Limpopo province of South Africa. Ph.D. Thesis, University of South Africa, Pretoria, South Africa, 2017. [Google Scholar]
- Sodi, T.; Mudhovozi, P.; Mashamba, T.; Radzilani-Makatu, M.; Takalani, J.; Mabunda, J. Indigenous healing practices in Limpopo Province of South Africa: A qualitative study. Int. J. Health Promot. Educ. 2011, 49, 101–110. [Google Scholar] [CrossRef]
- Cheikhyoussef, A.; Shapi, M.; Matengu, K.; Ashekele, H.M. Ethnobotanical study of indigenous knowledge on medicinal plant use by traditional healers in Oshikoto region, Namibia. J. Ethnobiol. Ethnomed. 2011, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Watt, J.M.; Breyer-Brandwijk, M.G. The Medicinal and Poisonous Plants of Southern and Eastern Africa, 2nd ed.; Livingstone: London, UK, 1962. [Google Scholar]
- Noudogbessi, J.; Tchobo, P.; Alitonou, G.; Avlessi, F.; Soumanou, M.; Chalard, P.; Figueredo, G.; Chalchat, J.; Sohounhloue, D. Chemical study of extracts of Siphonochilus aethiopicus (Schweinf.) BL Burtt (Zingiberaceae) from Benin. J. Asian Chem 2013, 25, 8489–8492. [Google Scholar] [CrossRef]
- Van Wyk, B.-E.; Gericke, N. People’s Plants: A Guide to Useful Plants of Southern Africa; Briza Publications: Pretoria, South Africa, 2000. [Google Scholar]
- Semenya, S.S.; Maroyi, A. Plants used by Bapedi traditional healers to treat asthma and related symptoms in Limpopo province, South Africa. Evid. Based Complementary Altern. Med. 2018, 2018, 2183705. [Google Scholar] [CrossRef] [PubMed]
- Makgopa, M.; Koma, M. The use of ditaola (divination bones) among indigenous healers in Sekhukhune District, Limpopo Province: Indigenous African healing practices. Indilinga Afr. J. Indig. Knowl. Syst. 2009, 8, 51–58. [Google Scholar]
- Hutchings, A.; Scott, A.H.; Lewis, G.; Cunningham, A. Zulu Medicinal Plants. In An Inventory; University of Natal Press: Pietermaritzburg, South Africa, 1996. [Google Scholar]
- Rankoana, S.A. Perceptions of climate change and the potential for adaptation in a rural community in Limpopo Province, South Africa. Sustainability 2016, 8, 672. [Google Scholar] [CrossRef] [Green Version]
- Mathibela, M.K.; Potgieter, M.J.; Tshikalange, T.E. Medicinal plants used to manage sexually transmitted infections by Bapedi traditional health practitioners in the Blouberg area, South Africa. S. Afr. J. Bot. 2019, 122, 385–390. [Google Scholar] [CrossRef]
- Kock, K. The Influence of Culture on the Utilization of Traditional Leafy Vegetables among VaTsonga and Ba-Pedi Women of Bushbuckridge, Mpumalanga Province. Master’s Thesis, North-West University, Mahikeng, South Africa, 2020. [Google Scholar]
- Shirindi, M.; Makofane, M. Ritual impurities: Perspectives of women living with HIV and AIDS. Afr. J. Phys. Health Educ. Recreat. Danc. 2015, 21, 941–952. [Google Scholar]
- Sharma, A.; Thakur, D.; Uniyal, S.K. Taboos: Traditional beliefs and customs for resource management in the western Himalaya. Ind. J. Tradit. Knowl. 2021, 20, 575–581. [Google Scholar]
- Avakoudjo, H.G.G.; Hounkpèvi, A.; Idohou, R.; Koné, M.W.; Assogbadjo, A.E. Local knowledge, uses, and factors determining the use of Strychnos spinosa organs in Benin (West Africa). Econ. Bot. 2020, 74, 15–31. [Google Scholar] [CrossRef]
- Kurui, M.C.; Kiptui, M.; Chelang’a, J.K.; Omondi, P. Traditional controls of harvesting and conserving medicinal plants in Keiyo South. Int. J. Humanit. Soc. Sci. 2016, 6, 54–63. [Google Scholar]
- Semenya, S.S.; Maroyi, A. Medicinal plants used for the treatment of tuberculosis by Bapedi traditional healers in three districts of the Limpopo Province, South Africa. Afr. J. Tradit. Complemen. Altern. Med. 2013, 10, 316–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canter, P.H.; Thomas, H.; Ernst, E. Bringing medicinal plants into cultivation: Opportunities and challenges for biotechnology. Trends Biotechnol. 2005, 23, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Boafo, Y.A.; Saito, O.; Kato, S.; Kamiyama, C.; Takeuchi, K.; Nakahara, M. The role of traditional ecological knowledge in ecosystem services management: The case of four rural communities in Northern Ghana. Int. J. Biodivers. Sci. Ecosyst. Serv. Manag. 2016, 12, 24–38. [Google Scholar] [CrossRef] [Green Version]
- Zschocke, S.; Rabe, T.; Taylor, J.L.S.; Jäger, A.K.; Van Staden, J. Plant part substitution—A way to conserve endangered medicinal plants? J. Ethnopharmacol. 2000, 71, 281–292. [Google Scholar] [CrossRef]
- Okoye, J.; Oni, K. Promotion of indigenous food preservation and processing knowledge and the challenge of food security in Africa. J. Food Secur. 2017, 5, 75–87. [Google Scholar]
- Ndhlala, A.R.; Ncube, B.; Van Staden, J. Ensuring quality in herbal medicines: Toxic phthalates in plastic-packaged commercial herbal products. S. Afr. J. Bot. 2012, 82, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Amoo, S.O.; Aremu, A.O.; Moyo, M.; Van Staden, J. Antioxidant and acetylcholinesterase-inhibitory properties of long-term stored medicinal plants. BMC Complemen. Altern. Med. 2012, 12, 87. [Google Scholar] [CrossRef] [Green Version]
- Amoo, S.O.; Aremu, A.O.; Moyo, M.; Van Staden, J. Assessment of long-term storage on antimicrobial and cyclooxygenase-inhibitory properties of South African medicinal plants. Phytother. Res. 2013, 27, 1029–1035. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Frequency (n) | Percentage (%) |
|---|---|---|
| Age group | ||
| 26–40 | 3 | 30 |
| 41–54 | 1 | 10 |
| 55–69 | 4 | 40 |
| 70 and above | 2 | 20 |
| Type of stakeholder | ||
| Traditional healer | 4 | 40 |
| Knowledge holder | 4 | 40 |
| Herbalist | 2 | 20 |
| Gender | ||
| Male | 6 | 60 |
| Female | 4 | 40 |
| Marital status | ||
| Widower/widow | 4 | 40 |
| single | 1 | 10 |
| married | 4 | 40 |
| divorced | 1 | 10 |
| Religion | ||
| African tradition | 7 | 70 |
| Christian | 3 | 30 |
| Years of experience with the use of African ginger | ||
| 11–20 | 3 | 30 |
| 21–30 | 2 | 20 |
| 30 and above | 5 | 50 |
| Formal educational level | ||
| None | 7 | 70 |
| Primary | 1 | 10 |
| Secondary | 2 | 20 |
| Tertiary | 0 | 0 |
| Work status | ||
| Employed | 2 | 20 |
| Unemployed | 1 | 10 |
| Self-employed | 1 | 10 |
| Retired | 6 | 60 |
| Disease/Health Conditions | Number of Mention | Relative Frequency | Percentage (%) | |
|---|---|---|---|---|
| Common Name | Local Name | |||
| Asthma | Bolwetši bja mafahla | 10 | 1 | 100 |
| Chest pains | Go baba ga mafatlha | 10 | 1 | 100 |
| Cough | Go gohlola | 8 | 0.8 | 80 |
| Headache | Go remiwa ke hlogo | 10 | 1 | 100 |
| Influenza | Mokomana | 3 | 0.3 | 30 |
| Menstruation pains | Go bona ngwedi ka maima | 2 | 0.2 | 20 |
| Navel pains | Khubjana yago baba | 1 | 0.1 | 10 |
| Sexually transmitted infections | Bolwetši bjo bo fetelago ka thobalano | 7 | 0.7 | 70 |
| Stomach-ache | Mpa yago baba | 8 | 0.8 | 80 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seile, B.P.; Bareetseng, S.; Koitsiwe, M.T.; Aremu, A.O. Indigenous Knowledge on the Uses, Sustainability and Conservation of African Ginger (Siphonochilus aethiopicus) among Two Communities in Mpumalanga Province, South Africa. Diversity 2022, 14, 192. https://doi.org/10.3390/d14030192
Seile BP, Bareetseng S, Koitsiwe MT, Aremu AO. Indigenous Knowledge on the Uses, Sustainability and Conservation of African Ginger (Siphonochilus aethiopicus) among Two Communities in Mpumalanga Province, South Africa. Diversity. 2022; 14(3):192. https://doi.org/10.3390/d14030192
Chicago/Turabian StyleSeile, Boinelo P., Sechaba Bareetseng, Motheo T. Koitsiwe, and Adeyemi O. Aremu. 2022. "Indigenous Knowledge on the Uses, Sustainability and Conservation of African Ginger (Siphonochilus aethiopicus) among Two Communities in Mpumalanga Province, South Africa" Diversity 14, no. 3: 192. https://doi.org/10.3390/d14030192