
Circulating Interlukin-32 and Altered Blood Pressure Control in Individuals with Metabolic Dysfunction
 , , ,
, , ,
Abstract
:1. Introduction
2. Results
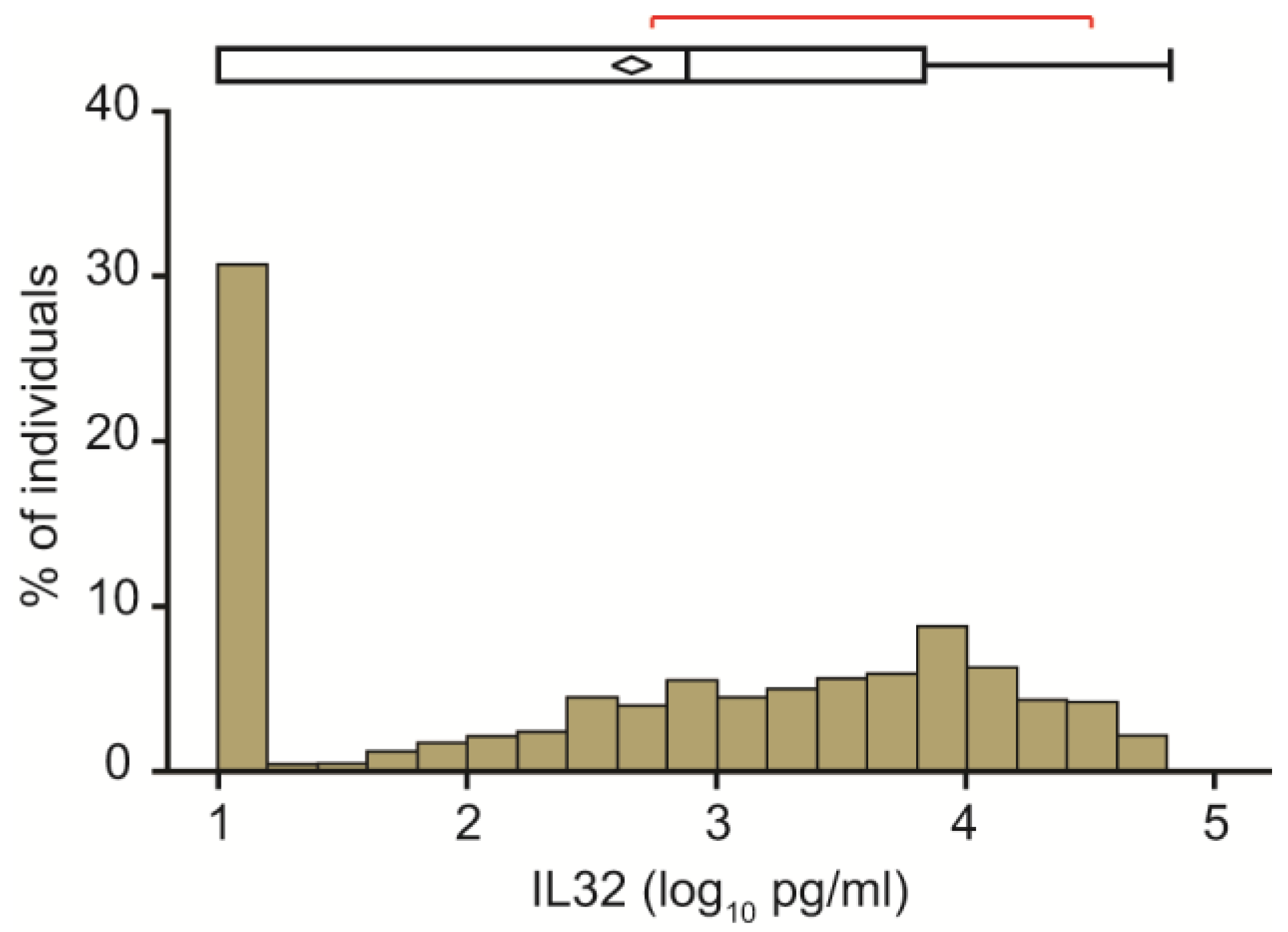
2.1. Clinical Features of the Study Cohort and Circulating IL32 Distribution
2.2. Relationship between Circulating IL32 Levels and Metabolic Features
2.3. Sensitivity Analyses
2.4. Impact of Blood Pressure Lowering Medications
2.5. Independent Determinants of Arterial Blood Pressure
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.2. Anthropometric Measurements
4.3. Laboratory Analysis
4.4. Liver Fat Quantification
4.5. Measurement of Circulating IL32
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global Burden of NAFLD and NASH: Trends, Predictions, Risk Factors and Prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- López-Suárez, A.; Guerrero, J.M.R.; Elvira-González, J.; Beltrán-Robles, M.; Cañas-Hormigo, F.; Bascuñana-Quirell, A. Nonalcoholic Fatty Liver Disease Is Associated with Blood Pressure in Hypertensive and Nonhypertensive Individuals from the General Population with Normal Levels of Alanine Aminotransferase. Eur. J. Gastroenterol. Hepatol. 2011, 23, 1011–1017. [Google Scholar] [CrossRef] [PubMed]
- Lorbeer, R.; Bayerl, C.; Auweter, S.; Rospleszcz, S.; Lieb, W.; Meisinger, C.; Heier, M.; Peters, A.; Bamberg, F.; Hetterich, H. Association between MRI-Derived Hepatic Fat Fraction and Blood Pressure in Participants without History of Cardiovascular Disease. J. Hypertens 2017, 35, 737–744. [Google Scholar] [CrossRef]
- Kasper, P.; Martin, A.; Lang, S.; Demir, M.; Steffen, H.-M. Hypertension in NAFLD: An Uncontrolled Burden. J. Hepatol. 2021, 74, 1258–1260. [Google Scholar] [CrossRef] [PubMed]
- Lonardo, A.; Nascimbeni, F.; Mantovani, A.; Targher, G. Hypertension, Diabetes, Atherosclerosis and NASH: Cause or Consequence? J. Hepatol. 2018, 68, 335–352. [Google Scholar] [CrossRef]
- Oikonomou, D.; Georgiopoulos, G.; Katsi, V.; Kourek, C.; Tsioufis, C.; Alexopoulou, A.; Koutli, E.; Tousoulis, D. Non-Alcoholic Fatty Liver Disease and Hypertension: Coprevalent or Correlated? Eur. J. Gastroenterol. Hepatol. 2018, 30, 979–985. [Google Scholar] [CrossRef]
- Ruscica, M.; Ferri, N.; Macchi, C.; Meroni, M.; Lanti, C.; Ricci, C.; Maggioni, M.; Fracanzani, A.L.; Badiali, S.; Fargion, S.; et al. Liver Fat Accumulation Is Associated with Circulating PCSK9. Ann. Med. 2016, 48, 384–391. [Google Scholar] [CrossRef] [PubMed]
- Santos, R.D.; Valenti, L.; Romeo, S. Does Nonalcoholic Fatty Liver Disease Cause Cardiovascular Disease? Current Knowledge and Gaps. Atherosclerosis 2019, 282, 110–120. [Google Scholar] [CrossRef]
- Coffman, T.M. Under Pressure: The Search for the Essential Mechanisms of Hypertension. Nat. Med. 2011, 17, 1402–1409. [Google Scholar] [CrossRef]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global Epidemiology, Health Burden and Effective Interventions for Elevated Blood Pressure and Hypertension. Nat. Rev. Cardiol. 2021, 18, 785–802. [Google Scholar] [CrossRef]
- Norlander, A.E.; Madhur, M.S.; Harrison, D.G. The Immunology of Hypertension. J. Exp. Med. 2018, 215, 21–33. [Google Scholar] [CrossRef] [PubMed]
- Caillon, A.; Paradis, P.; Schiffrin, E.L. Role of Immune Cells in Hypertension. Br. J. Pharmacol. 2019, 176, 1818–1828. [Google Scholar] [CrossRef] [PubMed]
- Senchenkova, E.Y.; Russell, J.; Yildirim, A.; Granger, D.N.; Gavins, F.N.E. Novel Role of T Cells and IL-6 (Interleukin-6) in Angiotensin II-Induced Microvascular Dysfunction. Hypertension 2019, 73, 829–838. [Google Scholar] [CrossRef]
- Elijovich, F.; Laffer, C.L.; Sahinoz, M.; Pitzer, A.; Ferguson, J.F.; Kirabo, A. The Gut Microbiome, Inflammation, and Salt-Sensitive Hypertension. Curr. Hypertens Rep. 2020, 22, 79. [Google Scholar] [CrossRef]
- Zhang, L.; Che, C.; Lin, J.; Liu, K.; Li, D.-Q.; Zhao, G. TLR-Mediated Induction of Proinflammatory Cytokine IL-32 in Corneal Epithelium. Curr. Eye Res. 2013, 38, 630–638. [Google Scholar] [CrossRef]
- Zhang, Y.-Y.; Xu, L.; Li, D.-Q.; Shao, J.-H.; Chen, P.; Zhao, H.-Y.; Dong, X.-B.; Gu, L.-P.; Wu, W. IL-32 mRNA Expression of Bone Marrow Stromal Cells and Its Correlation with Cell Apoptosis in Patients with Myelodysplastic Syndrome. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2016, 24, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Wen, S.; Hou, Y.; Fu, L.; Xi, L.; Yang, D.; Zhao, M.; Qin, Y.; Sun, K.; Teng, Y.; Liu, M. Cancer-Associated Fibroblast (CAF)-Derived IL32 Promotes Breast Cancer Cell Invasion and Metastasis via Integrin Β3-P38 MAPK Signalling. Cancer Lett. 2019, 442, 320–332. [Google Scholar] [CrossRef]
- Choi, J.-D.; Bae, S.-Y.; Hong, J.-W.; Azam, T.; Dinarello, C.A.; Her, E.; Choi, W.-S.; Kim, B.-K.; Lee, C.-K.; Yoon, D.-Y.; et al. Identification of the Most Active Interleukin-32 Isoform. Immunology 2009, 126, 535–542. [Google Scholar] [CrossRef]
- Gautam, A.; Pandit, B. IL32: The Multifaceted and Unconventional Cytokine. Hum. Immunol. 2021, 82, 659–667. [Google Scholar] [CrossRef]
- Baselli, G.A.; Dongiovanni, P.; Rametta, R.; Meroni, M.; Pelusi, S.; Maggioni, M.; Badiali, S.; Pingitore, P.; Maurotti, S.; Montalcini, T.; et al. Liver Transcriptomics Highlights Interleukin-32 as Novel NAFLD-Related Cytokine and Candidate Biomarker. Gut 2020, 69, 1855–1866. [Google Scholar] [CrossRef]
- Dali-Youcef, N.; Vix, M.; Costantino, F.; El-Saghire, H.; Lhermitte, B.; Callari, C.; D’Agostino, J.; Perretta, S.; Paveliu, S.; Gualtierotti, M.; et al. Interleukin-32 Contributes to Human Nonalcoholic Fatty Liver Disease and Insulin Resistance. Hepatol. Commun. 2019, 3, 1205–1220. [Google Scholar] [CrossRef] [PubMed]
- Nold-Petry, C.A.; Nold, M.F.; Zepp, J.A.; Kim, S.-H.; Voelkel, N.F.; Dinarello, C.A. IL-32-Dependent Effects of IL-1beta on Endothelial Cell Functions. Proc. Natl. Acad. Sci. USA 2009, 106, 3883–3888. [Google Scholar] [CrossRef] [PubMed]
- Law, C.C.; Puranik, R.; Fan, J.; Fei, J.; Hambly, B.D.; Bao, S. Clinical Implications of IL-32, IL-34 and IL-37 in Atherosclerosis: Speculative Role in Cardiovascular Manifestations of COVID-19. Front. Cardiovasc. Med. 2021, 8, 630767. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Li, Q.; Ding, H.; Zhao, G.; Wang, Z.; Cao, C.; Dai, Y.; Zheng, M.; Zhu, X.; Wu, Q.; et al. Placenta-Derived IL-32β Activates Neutrophils to Promote Preeclampsia Development. Cell. Mol. Immunol. 2021, 18, 979–991. [Google Scholar] [CrossRef]
- Nold-Petry, C.A.; Rudloff, I.; Baumer, Y.; Ruvo, M.; Marasco, D.; Botti, P.; Farkas, L.; Cho, S.X.; Zepp, J.A.; Azam, T.; et al. IL-32 Promotes Angiogenesis. J. Immunol. 2014, 192, 589–602. [Google Scholar] [CrossRef]
- Hasegawa, H.; Thomas, H.J.; Schooley, K.; Born, T.L. Native IL-32 Is Released from Intestinal Epithelial Cells via a Non-Classical Secretory Pathway as a Membrane-Associated Protein. Cytokine 2011, 53, 74–83. [Google Scholar] [CrossRef]
- Zahoor, M.; Westhrin, M.; Aass, K.R.; Moen, S.H.; Misund, K.; Psonka-Antonczyk, K.M.; Giliberto, M.; Buene, G.; Sundan, A.; Waage, A.; et al. Hypoxia Promotes IL-32 Expression in Myeloma Cells, and High Expression Is Associated with Poor Survival and Bone Loss. Blood Adv. 2017, 1, 2656–2666. [Google Scholar] [CrossRef]
- Sun, Y.; Qian, Y.; Chen, C.; Wang, H.; Zhou, X.; Zhai, W.; Qiu, L.; Zhou, X.; Ning, H.; Zhao, Y.; et al. Extracellular Vesicle IL-32 Promotes the M2 Macrophage Polarization and Metastasis of Esophageal Squamous Cell Carcinoma via FAK/STAT3 Pathway. J. Exp. Clin. Cancer Res. 2022, 41, 145. [Google Scholar] [CrossRef]
- Goda, C.; Kanaji, T.; Kanaji, S.; Tanaka, G.; Arima, K.; Ohno, S.; Izuhara, K. Involvement of IL-32 in Activation-Induced Cell Death in T Cells. Int. Immunol. 2006, 18, 233–240. [Google Scholar] [CrossRef]
- Kobayashi, H.; Lin, P.C. Molecular Characterization of IL-32 in Human Endothelial Cells. Cytokine 2009, 46, 351–358. [Google Scholar] [CrossRef]
- Kim, D.H.; Park, E.-S.; Lee, A.R.; Park, S.; Park, Y.K.; Ahn, S.H.; Kang, H.S.; Won, J.H.; Ha, Y.N.; Jae, B.; et al. Intracellular Interleukin-32γ Mediates Antiviral Activity of Cytokines against Hepatitis B Virus. Nat. Commun. 2018, 9, 3284. [Google Scholar] [CrossRef] [PubMed]
- Chae, C.U.; Lee, R.T.; Rifai, N.; Ridker, P.M. Blood Pressure and Inflammation in Apparently Healthy Men. Hypertension 2001, 38, 399–403. [Google Scholar] [CrossRef] [PubMed]
- Yu, Z.; Kim, S.C.; Vanni, K.; Huang, J.; Desai, R.; Murphy, S.N.; Solomon, D.H.; Liao, K.P. Association between Inflammation and Systolic Blood Pressure in RA Compared to Patients without RA. Arthritis Res. Ther. 2018, 20, 107. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-E.; Kim, G.-T.; Lee, S.-G.; Park, S.-H.; Baek, S.-H.; Kim, S.-I.; Kim, J.-I.; Jin, H.-S. IL-32 Aggravates Synovial Inflammation and Bone Destruction and Increases Synovial Natural Killer Cells in Experimental Arthritis Models. Rheumatol. Int. 2013, 33, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Yamamoto, M.; Yajima, H.; Suzuki, C.; Naishiro, Y.; Takahashi, H.; Imai, K.; Shinomura, Y. Role of Interleukin-32 in the Mechanism of Chronic Inflammation in IgG4-Related Disease and as a Predictive Biomarker for Drug-Free Remission. Mod. Rheumatol. 2016, 26, 391–397. [Google Scholar] [CrossRef]
- Yang, Z.; Shi, L.; Xue, Y.; Zeng, T.; Shi, Y.; Lin, Y.; Liu, L. Interleukin-32 Increases in Coronary Arteries and Plasma from Patients with Coronary Artery Disease. Clin. Chim. Acta 2019, 497, 104–109. [Google Scholar] [CrossRef]
- Shim, S.; Lee, S.; Hisham, Y.; Kim, S.; Nguyen, T.T.; Taitt, A.S.; Hwang, J.; Jhun, H.; Park, H.-Y.; Lee, Y.; et al. A Paradoxical Effect of Interleukin-32 Isoforms on Cancer. Front. Immunol. 2022, 13, 837590. [Google Scholar] [CrossRef]
- Di Benedetto, P.; Guggino, G.; Manzi, G.; Ruscitti, P.; Berardicurti, O.; Panzera, N.; Grazia, N.; Badagliacca, R.; Riccieri, V.; Vizza, C.D.; et al. Interleukin-32 in Systemic Sclerosis, a Potential New Biomarker for Pulmonary Arterial Hypertension. Arthritis Res. Ther. 2020, 22, 127. [Google Scholar] [CrossRef]
- Mazlum, F.; Gharesi-Fard, B.; Hadinedoushan, H.; Bakhshizadeh Ghashti, Y. Association between Interleukin-32 Gene Polymorphism and Susceptibility to Preeclampsia. Hypertens Pregnancy 2021, 40, 218–225. [Google Scholar] [CrossRef]
- Gaba, P.; Gersh, B.J.; Muller, J.; Narula, J.; Stone, G.W. Evolving Concepts of the Vulnerable Atherosclerotic Plaque and the Vulnerable Patient: Implications for Patient Care and Future Research. Nat. Rev. Cardiol. 2022, 20, 181–196. [Google Scholar] [CrossRef]
- Jin, S.; Liu, X.; Wang, Y.; Yu, J.; Jiang, M. Effects of IL-32 Polymorphisms and IL-32 Levels on the Susceptibility and Severity of Coronary Artery Disease. J. Clin. Lab. Anal. 2022, 36, e24114. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuka, T.; Hamada, M.; Hiasa, G.; Sasaki, O.; Suzuki, M.; Hara, Y.; Shigematsu, Y.; Hiwada, K. Effect of Beta-Blockers on Circulating Levels of Inflammatory and Anti-Inflammatory Cytokines in Patients with Dilated Cardiomyopathy. J. Am. Coll. Cardiol. 2001, 37, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Gullestad, L.; Aukrust, P.; Ueland, T.; Espevik, T.; Yee, G.; Vagelos, R.; Frøland, S.S.; Fowler, M. Effect of High- versus Low-Dose Angiotensin Converting Enzyme Inhibition on Cytokine Levels in Chronic Heart Failure. J. Am. Coll. Cardiol. 1999, 34, 2061–2067. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Pelusi, S.; Bianco, C.; Ceriotti, F.; Berzuini, A.; Iogna Prat, L.; Trotti, R.; Malvestiti, F.; D’Ambrosio, R.; Lampertico, P.; et al. Definition of Healthy Ranges for Alanine Aminotransferase Levels: A 2021 Update. Hepatol. Commun. 2021, 5, 1824–1832. [Google Scholar] [CrossRef] [PubMed]
- Valenti, L.; Tripodi, A.; La Mura, V.; Pelusi, S.; Bianco, C.; Scalambrino, E.; Margarita, S.; Malvestiti, F.; Ronzoni, L.; Clerici, M.; et al. Clinical and Genetic Determinants of the Fatty Liver-Coagulation Balance Interplay in Individuals with Metabolic Dysfunction. JHEP Rep. 2022, 4, 100598. [Google Scholar] [CrossRef] [PubMed]
- Sofi, F.; Cesari, F.; Abbate, R.; Gensini, G.F.; Casini, A. Adherence to Mediterranean Diet and Health Status: Meta-Analysis. BMJ 2008, 337, a1344. [Google Scholar] [CrossRef]
- Ferrario, M.; Chiodini, P.; Chambless, L.E.; Cesana, G.; Vanuzzo, D.; Panico, S.; Sega, R.; Pilotto, L.; Palmieri, L.; Giampaoli, S.; et al. Prediction of Coronary Events in a Low Incidence Population. Assessing Accuracy of the CUORE Cohort Study Prediction Equation. Int. J. Epidemiol. 2005, 34, 413–421. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 Practice Guidelines for the Management of Arterial Hypertension of the European Society of Hypertension and the European Society of Cardiology: ESH/ESC Task Force for the Management of Arterial Hypertension. J. Hypertens 2018, 36, 2284–2309. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An Inexpensive and Accurate Marker of Fibrosis in HCV Infection. Comparison with Liver Biopsy and Fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Newsome, P.N.; Sasso, M.; Deeks, J.J.; Paredes, A.; Boursier, J.; Chan, W.-K.; Yilmaz, Y.; Czernichow, S.; Zheng, M.-H.; Wong, V.W.-S.; et al. FibroScan-AST (FAST) Score for the Non-Invasive Identification of Patients with Non-Alcoholic Steatohepatitis with Significant Activity and Fibrosis: A Prospective Derivation and Global Validation Study. Lancet Gastroenterol. Hepatol. 2020, 5, 362–373. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Overall (n = 949) | Males (n = 791, 83.3%) | Females (n = 158, 16.7%) | p-Value * | |
|---|---|---|---|---|
| Age, years | 53.9 ± 6.4 | 53.9 ± 6.5 | 53.6 ± 5.8 | 0.6 |
| BMI, Kg/m2 | 28.5 ± 3.1 | 28.5 ± 3.0 | 28.9 ± 3.5 | 0.1 |
| Obesity, yes | 214 (22.5) | 166 (20.9) | 48 (30.9) | 9.4 × 10−3 |
| Diabetes, yes | 35 (3.7) | 29 (3.7) | 6 (3.8) | 0.9 |
| ALT, IU/l | 30 ± 14.3 | 31.3 ± 14.2 | 23.3 ± 12.8 | 5.6 × 10−11 |
| AST, IU/l | 24 ± 8 | 24.5 ± 7.9 | 21.5 ± 8.3 | 3.9 × 10−6 |
| CAP ≥ 275 dB/m, yes | 470 (49.5) | 400 (50.6) | 70 (44.3) | 0.2 |
| LSM ≥ 8.0 kPa, yes | 20 (2.1) | 20 (2.5) | 0 | 1.0 |
| LDL, mg/dL | 123.2 ± 29.4 | 122.5 ± 28.5 | 126.4 ± 28.9 | 0.12 |
| HDL, mg/dL | 45.3 ± 10.1 | 44 ± 9.4 | 51.8 ± 10.8 | 6.1 × 10−16 |
| TG, mg/dL | 168.4 ± 86.5 | 171.4 ± 90.3 | 153 ± 62.2 | 0.014 |
| SBP, mmHg | 136.2 ± 12.1 | 136.0 ± 11.9 | 137.2 ± 12.6 | 0.27 |
| DBP, mmHg | 85.5 ± 7.9 | 85.6 ± 7.8 | 84.7 ± 8.2 | 0.18 |
| Arterial hypertension, yes | 654 (68.9) | 552 (69.8) | 102 (64.6) | 0.22 |
| Smoke, yes | 86 (9.1) | 71 (9.0) | 15 (9.5) | 0.85 |
| 10-years cardiovascular risk °, % | 0.047 ± 0.030 | 0.053 ± 0.030 | 0.018 ± 0.010 | 7.7 × 10−112 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| Estimate | 95% C.I. | p-Value * | Estimate | 95% C.I. | p-Value ** | |
| Age, years | −0.001 | −0.014–0.012 | 0.87 | |||
| Sex, F | 0.110 | 0.000–0.219 | 0.049 | 0.070 | −0.040–0.018 | 0.22 |
| Abdominal circumference, cm | −0.011 | −0.020–−0.001 | 0.022 | −0.009 | −0.019–−0.000 | 0.040 |
| BMI, Kg/m2 | −0.004 | −0.030–0.023 | 0.079 | |||
| Diabetes, yes | −0.159 | −0.376–0.058 | 0.15 | |||
| Obesity, Yes | 0.013 | −0.086–0.111 | 0.80 | |||
| HbA1c, mmol/mol | −0.020 | −0.039–0.000 | 0.051 | |||
| Increased blood pressure (≥130/85 mmHg), yes | 0.160 | 0.067–0.253 | 0.0007 | 0.167 | 0.070–0.256 | 0.0006 |
| Hypertension, yes | 0.084 | 0.002–0.166 | 0.043 | 0.092 | 0.009–0.174 | 0.029 |
| SBP, mmHg | 0.008 | 0.001–0.015 | 0.017 | 0.008 | 0.002–0.015 | 0.016 |
| DBP, mmHg | 0.008 | −0.002–0.019 | 0.11 | |||
| LDL, mg/dL | 0.000 | −0.004–0.002 | 0.60 | |||
| HDL, mg/dL | −0.190 | −0.583–0.203 | 0.34 | |||
| Triglycerides, mg/dL | 0.028 | −0.153–0.209 | 0.76 | |||
| Insulin, mU/L | 0.001 | −0.008–0.010 | 0.76 | |||
| Hyperglycemia, Yes | −0.101 | −0.271–0.068 | 0.24 | |||
| Log10 ALT, IU/l | 0.060 | −0.136–0.258 | 0.55 | |||
| Log10 AST, IU/l | −0.038 | −0.219–0.144 | 0.68 | |||
| CAP ≥ 275 | −0.023 | −0.105–0.058 | 0.57 | |||
| LSM ≥ 7.9 | −0.104 | −0.412–0.205 | 0.51 | |||
| MDS > 7, Yes | 0.090 | 0.005–0.175 | 0.037 | 0.072 | −0.013–0.157 | 0.097 |
| Cardiovascular risk °, % | −1.080 | −3.758–1.560 | 0.47 | |||
| Unadjusted | Adjusted | ||||||
|---|---|---|---|---|---|---|---|
| Overall (n = 949) | Estimate | 95% c.i. | p-Value | Estimate | 95% c.i. | p-Value | |
| Any anti-hypertensive, yes | 254 (26.7) | −0.162 | −0.254–−0.070 | 0.0005 | −0.189 | −0.291–−0.088 | 0.0002 |
| ACE inhibitors, yes | 120 (12.6) | −0.137 | −0.159–−0.014 | 0.029 | −0.123 | −0.247–−0.001 | 0.049 |
| ARB, yes | 100 (10.5) | −0.093 | −0.226–0.040 | 0.17 | - | - | - |
| Beta-blockers, yes | 31 (32.6) | −0.233 | −0.462–−0.003 | 0.047 | −0.205 | −0.462–0.024 | 0.079 |
| Alpha-blockers, yes | 5 (0.005) | −0.157 | −0.721–0.408 | 0.58 | - | - | - |
| Calcium channel blockers, yes | 49 (0.05) | −0.076 | −0.261–0.109 | 0.42 | - | - | - |
| Diuretics, yes | 56 (0.060) | −0.191 | −0.364–0.018 | 0.031 | −0.177 | −0.350–0.004 | 0.044 |
| SBP | DBP | Impaired Blood Pressure Control | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | Lower | Upper | p-Value | Estimate | Lower | Upper | p-Value | OR | Lower | Upper | p-Value | |
| Age, years | 0.346 | 0.226 | 0.466 | 2 × 10−8 | 0.006 | −0.076 | 0.088 | 0.89 | 1.03 | 1.01 | 1.06 | 0.007 |
| BMI, Kg/m2 | 0.295 | 0.055 | 0.536 | 0.016 | 0.237 | 0.072 | 0.401 | 0.005 | 1.05 | 1.00 | 1.11 | 0.053 |
| HDL-C, mg/dL | 0.173 | 0.099 | 0.248 | 5 × 10−6 | 0.067 | 0.016 | 0.118 | 0.010 | 1.04 | 1.02 | 1.06 | 4 × 10−6 |
| LDL-C, mg/dL | 0.029 | 0.004 | 0.054 | 0.022 | 0.020 | 0.003 | 0.037 | 0.024 | 1.006 | 1.00 | 1.01 | 0.031 |
| HbA1c, mmol/mol | 0.219 | 0.036 | 0.401 | 0.018 | 0.040 | −0.084 | 0.165 | 0.53 | 1.01 | 0.97 | 1.05 | 0.45 |
| Alcoholic drinks, n/week | 0.184 | 0.058 | 0.311 | 0.004 | 0.102 | 0.016 | 0.188 | 0.020 | 1.02 | 0.99 | 1.04 | 0.25 |
| Anti-hypertensive drugs, yes | −2.097 | −2.949 | −1.244 | 1 × 10−6 | −0.381 | −0.964 | 0.202 | 0.20 | 0.53 | 0.38 | 0.75 | 0.0003 |
| IL-32, log10 pg/mL | 0.746 | 0.173 | 1.318 | 0.010 | 0.363 | −0.028 | 0.755 | 0.068 | 1.22 | 1.09 | 1.38 | 0.0009 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomasi, M.; Cherubini, A.; Pelusi, S.; Margarita, S.; Bianco, C.; Malvestiti, F.; Miano, L.; Romeo, S.; Prati, D.; Valenti, L. Circulating Interlukin-32 and Altered Blood Pressure Control in Individuals with Metabolic Dysfunction. Int. J. Mol. Sci. 2023, 24, 7465. https://doi.org/10.3390/ijms24087465
Tomasi M, Cherubini A, Pelusi S, Margarita S, Bianco C, Malvestiti F, Miano L, Romeo S, Prati D, Valenti L. Circulating Interlukin-32 and Altered Blood Pressure Control in Individuals with Metabolic Dysfunction. International Journal of Molecular Sciences. 2023; 24(8):7465. https://doi.org/10.3390/ijms24087465
Chicago/Turabian StyleTomasi, Melissa, Alessandro Cherubini, Serena Pelusi, Sara Margarita, Cristiana Bianco, Francesco Malvestiti, Lorenzo Miano, Stefano Romeo, Daniele Prati, and Luca Valenti. 2023. "Circulating Interlukin-32 and Altered Blood Pressure Control in Individuals with Metabolic Dysfunction" International Journal of Molecular Sciences 24, no. 8: 7465. https://doi.org/10.3390/ijms24087465