
New Perspectives of Multiplex Mass Spectrometry Blood Protein Quantification on Microsamples in Biological Monitoring of Elderly Patients

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
2.1. Participants
2.2. Primary Outcome
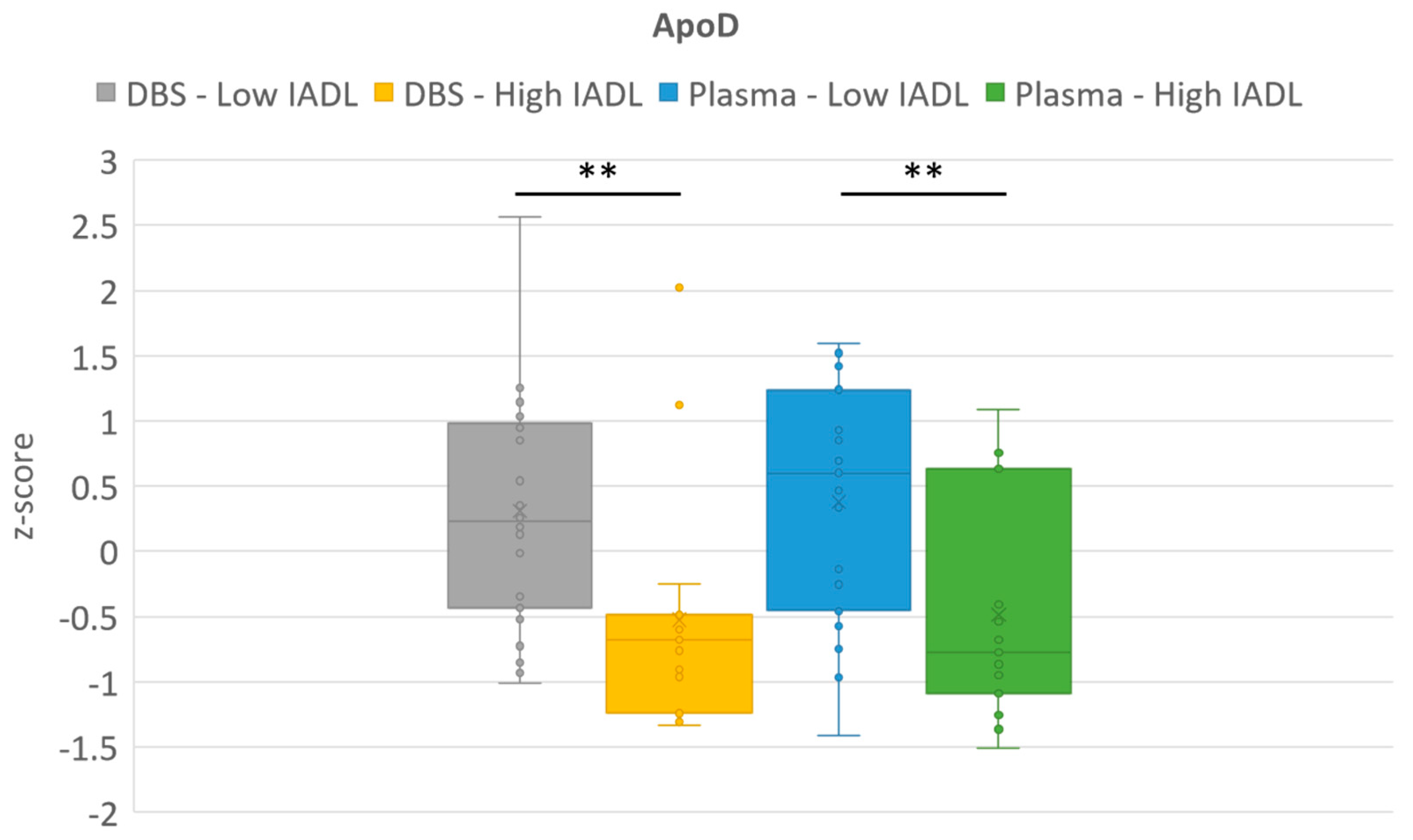
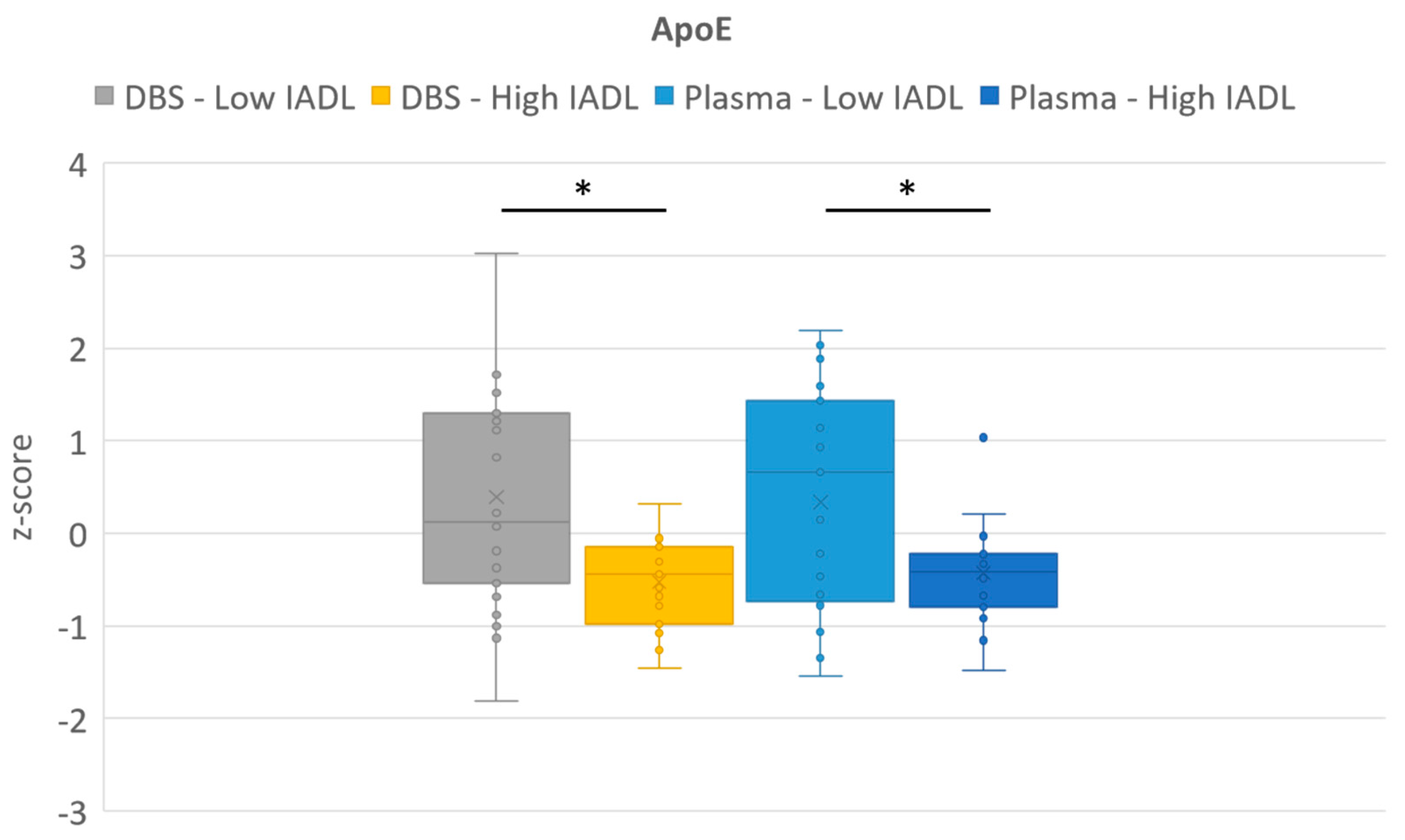
2.3. Secondary Outcomes
3. Discussion
4. Materials and Methods
4.1. Design and Setting
4.2. Study Population
4.3. Blood Collection
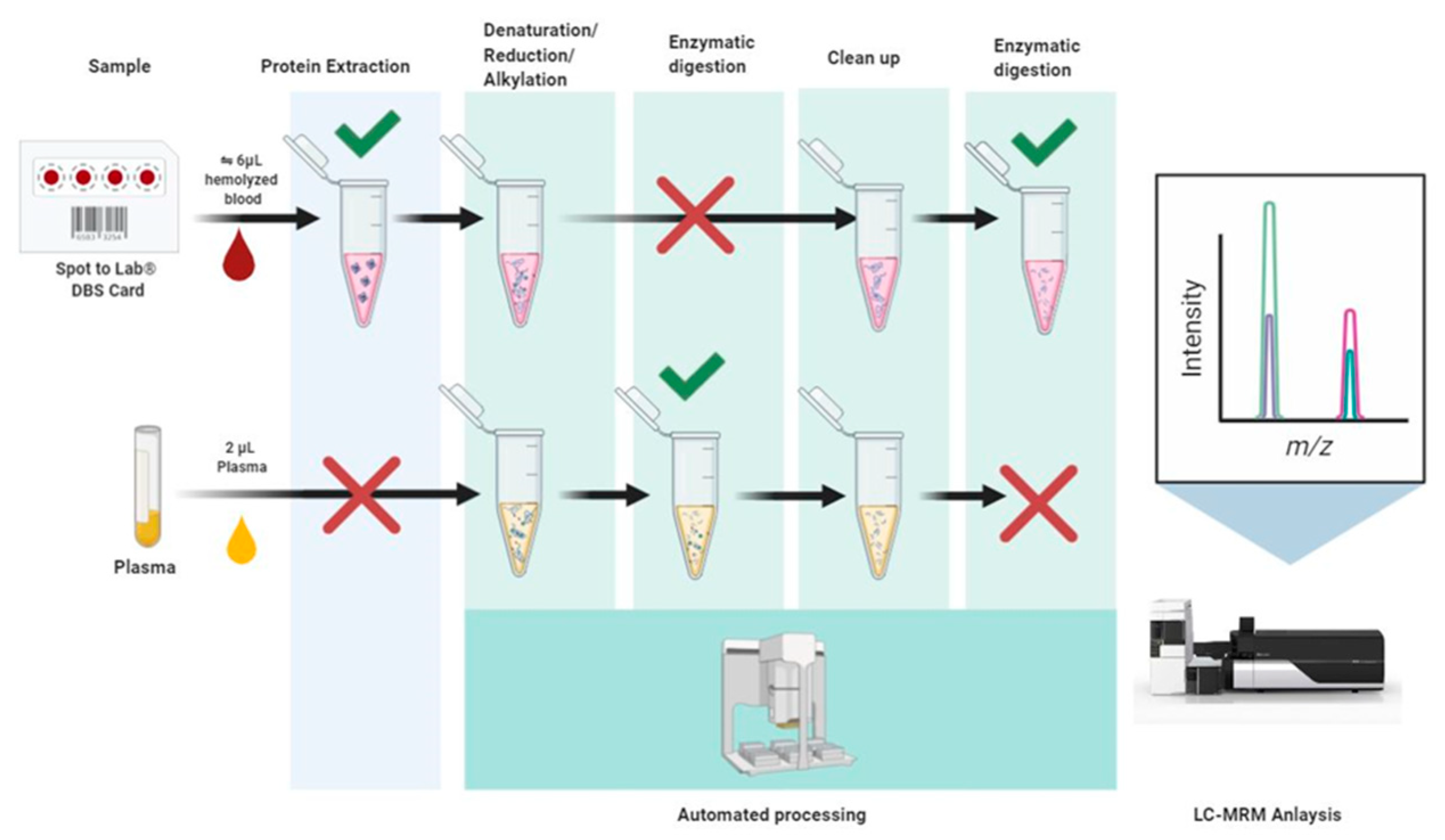
4.4. Mass Spectrometry (MS) Analysis of Microsamples
4.5. Outcomes
4.6. Statistical Analysis
4.7. Study Approval
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lei, B.U.W.; Prow, T.W. A review of microsampling techniques and their social impact. Biomed. Microdevices 2019, 21, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Londhe, V.; Rajadhyaksha, M. Opportunities and obstacles for microsampling techniques in bioanalysis: Special focus on DBS and VAMS. J. Pharm. Biomed. Anal. 2020, 182, 113102. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.G.; Percy, A.J.; Yang, J.; Camenzind, A.G.; Borchers, C.H. Multiplexed Quantitation of Endogenous Proteins in Dried Blood Spots by Multiple Reaction Monitoring-Mass Spectrometry. Mol. Cell. Proteom. 2013, 12, 781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirby, J.B.; Yabroff, K.R. Rural–Urban Differences in Access to Primary Care: Beyond the Usual Source of Care Provider. Am. J. Prev. Med. 2020, 58, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Atella, V.; Piano Mortari, A.; Kopinska, J.; Belotti, F.; Lapi, F.; Cricelli, C.; Fontana, L. Trends in age-related disease burden and healthcare utilization. Aging Cell 2019, 18, e12861. [Google Scholar] [CrossRef] [PubMed]
- Malentacchi, F.; Mancini, I.; Brandslund, I.; Vermeersch, P.; Schwab, M.; Marc, J.; van Schaik, R.H.; Siest, G.; Theodorsson, E.; Pazzagli, M.; et al. Is laboratory medicine ready for the era of personalized medicine? A survey addressed to laboratory directors of hospitals/academic schools of medicine in Europe. Drug Metab. Pers. Ther. 2015, 30, 121–128. [Google Scholar]
- Zengin, N.; Enç, N. Comparison of two blood sampling methods in anticoagulation therapy: Venipuncture and peripheral venous catheter. J. Clin. Nurs. 2007, 17, 386–393. [Google Scholar] [CrossRef]
- Kimori, K.; Konya, C.; Matsumoto, M. Venipuncture-Induced Hematomas Alter Skin Barrier Function in the Elderly Patients. SAGE Open Nurs. 2018, 4, 2377960818782050. [Google Scholar] [CrossRef] [Green Version]
- Liu, G.; Ji, Q.C.; Jemal, M.; Tymiak, A.A.; Arnold, M.E. Approach To Evaluating Dried Blood Spot Sample Stability during Drying Process and Discovery of a Treated Card To Maintain Analyte Stability by Rapid On-Card pH Modification. Anal. Chem. 2011, 83, 9033–9038. [Google Scholar] [CrossRef]
- Crimmins, E.M.; Zhang, Y.S.; Kim, J.K.; Frochen, S.; Kang, H.; Shim, H.; Ailshire, J.; Potter, A.; Cofferen, J.; Faul, J. Dried blood spots: Effects of less than optimal collection, shipping time, heat, and humidity. Am. J. Hum. Biol. 2020, 32, e23390. [Google Scholar] [CrossRef] [Green Version]
- Matos, A.L.S.; Moreira, J.P.D.L.; Luiz, R.R.; da Silva, E.P.; Rodacki, M.; Gómez, J.F.B.; Zajdenverg, L. Comparison of glucose measurement on dried blood spots versus plasma samples in pregnant women with and without anemia. Arq. Bras. Endocrinol. Metabol. 2020, 64, 454–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maleska, A.; Hirtz, C.; Casteleyn, E.; Villard, O.; Ducos, J.; Avignon, A.; Sultan, A.; Lehmann, S. Comparison of HbA1c detection in whole blood and dried blood spots using an automated ion-exchange HPLC system. Bioanalysis 2017, 9, 427–434. [Google Scholar] [CrossRef]
- Stinton, C.; Fraser, H.; Geppert, J.; Johnson, R.; Connock, M.; Johnson, S.; Clarke, A.; Taylor-Phillips, S. Newborn Screening for Long-Chain 3-Hydroxyacyl-CoA Dehydrogenase and Mitochondrial Trifunctional Protein Deficiencies Using Acylcarnitines Measurement in Dried Blood Spots-A Systematic Review of Test Accuracy. Front. Pediatr. 2021, 9, 606194. [Google Scholar] [CrossRef]
- Olivier, M.; Asmis, R.; Hawkins, G.A.; Howard, T.D.; Cox, L.A. The Need for Multi-Omics Biomarker Signatures in Precision Medicine. Int. J. Mol. Sci. 2019, 20, 4781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, N.; Priefer, R. Retinol binding protein 4 antagonists and protein synthesis inhibitors: Potential for therapeutic development. Eur. J. Med. Chem. 2021, 226, 113856. [Google Scholar] [CrossRef] [PubMed]
- Angelo, M.S.; Scanu, A.M.; Nakajima, K.; Edelstein, C. Apolipoprotein(a): Structure and biology. Front. Biosci. 2001, 6, D546–D554. [Google Scholar]
- Bhosale, S.D.; Moulder, R.; Venäläinen, M.S.; Koskinen, J.S.; Pitkänen, N.; Juonala, M.T.; Kähönen, M.A.P.; Lehtimäki, T.J.; Viikari, J.S.A.; Elo, L.L.; et al. Serum Proteomic Profiling to Identify Biomarkers of Premature Carotid Atherosclerosis. Sci. Rep. 2018, 8, 9209. [Google Scholar] [CrossRef] [Green Version]
- Luo, G.; Xu, N. Apolipoprotein M: Research Progress and Clinical Perspective. In Lipid Transfer in Lipoprotein Metabolism and Cardiovascular Disease; Springer: Singapore, 2020; Volume 1276, pp. 85–103. [Google Scholar]
- Clare, F.; Eleftherios, D. Theranos: Almost Complete Absence of Laboratory Medicine Input. J. Appl. Lab. Med. 2019, 3, 749–752. [Google Scholar]
- Simon, S.; Ezan, E. Ultrasensitive bioanalysis: Current status and future trends. Bioanalysis 2017, 9, 753–764. [Google Scholar] [CrossRef]
- Brandhorst, G.; Oellerich, M.; Maine, G.; Taylor, P.; Veen, G.; Wallemacq, P. Liquid chromatography-tandem mass spectrometry or automated immunoassays: What are the future trends in therapeutic drug monitoring? Clin. Chem. 2012, 58, 821–825. [Google Scholar] [CrossRef] [Green Version]
- Percy, A.J.; Chambers, A.G.; Parker, C.E.; Borchers, C.H. Absolute Quantitation of Proteins in Human Blood by Multiplexed Multiple Reaction Monitoring Mass Spectrometry. In Vascular Proteomics: Methods and Protocols; Humana Press: Totowa, NJ, USA, 2013; Volume 1000, pp. 167–189. [Google Scholar]
- Kuzyk, M.A.; Smith, D.; Yang, J.; Cross, T.J.; Jackson, A.M.; Hardie, D.B.; Anderson, N.L.; Borchers, C.H. Multiple Reaction Monitoring-based, Multiplexed, Absolute Quantitation of 45 Proteins in Human Plasma. Mol. Cell. Proteom. 2009, 8, 1860–1877. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirtz, C.; Vialaret, J.; Nowak, N.; Gabelle, A.; de Périère, D.D.; Lehmann, S. Absolute quantification of 35 plasma biomarkers in human saliva using targeted MS. Bioanalysis 2016, 8, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, S.; Brede, C.; Lescuyer, P.; Cocho, J.A.; Vialaret, J.; Bros, P.; Delatour, V.; Hirtz, C. Clinical mass spectrometry proteomics (cMSP) for medical laboratory: What does the future hold? Clin. Chim. Acta Int. J. Clin. Chem. 2017, 467, 51–58. [Google Scholar] [CrossRef]
- Bonnefoy, M.; Berrut, G.; LeSourd, B.; Ferry, M.; Gilbert, T.; Guerin, O.; Hanon, O.; Jeandel, C.; Paillaud, E.; Raynaud-Simon, A.; et al. Frailty and nutrition: Searching for evidence. J. Nutr. Health Aging 2015, 19, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Anderson, L.; Hunter, C.L. Quantitative mass spectrometric multiple reaction monitoring assays for major plasma proteins. Mol. Cell. Proteom. 2006, 5, 573–588. [Google Scholar] [CrossRef] [Green Version]
- Domanski, D.; Percy, A.J.; Yang, J.; Chambers, A.G.; Hill, J.S.; Freue, G.V.C.; Borchers, C.H. MRM-based multiplexed quantitation of 67 putative cardiovascular disease biomarkers in human plasma. Proteomics 2012, 12, 1222–1243. [Google Scholar] [CrossRef]
- Anderson, N.; Anderson, N.; Haines, L.; Hardie, D.; Olafson, R.; Pearson, T. Mass Spectrometric Quantitation of Peptides and Proteins Using Stable Isotope Standards and Capture by Anti-Peptide Antibodies (SISCAPA). J. Proteome Res. 2004, 3, 235–244. [Google Scholar] [CrossRef]
- Van Vliet, P.; Mooijaart, S.P.; de Craen, A.J.M.; Rensen, P.C.N.; van Heemst, D.; Westendorp, R.G.J. Plasma levels of apolipoprotein E and risk of stroke in old age. Ann. N. Y. Acad. Sci. 2007, 1100, 140–147. [Google Scholar] [CrossRef]
- Mooijaart, S.P.; van Vliet, P.; van Heemst, D.; Rensen, P.C.N.; Berbée, J.F.P.; Jolles, J.; De Craen, A.J.M.; Westendorp, R.G.J. Plasma levels of apolipoprotein E and cognitive function in old age. Ann. N. Y. Acad. Sci. 2007, 1100, 148–161. [Google Scholar] [CrossRef] [Green Version]
- Palmqvist, S.; Stomrud, E.; Cullen, N.; Janelidze, S.; Manuilova, E.; Jethwa, A.; Bittner, T.; Eichenlaub, U.; Suridjan, I.; Kollmorgen, G.; et al. An accurate fully automated panel of plasma biomarkers for Alzheimer’s disease. Alzheimer’s Dement. 2022. [Google Scholar] [CrossRef] [PubMed]
- Waldner, A.; Dassati, S.; Redl, B.; Smania, N.; Gandolfi, M. Apolipoprotein D Concentration in Human Plasma during Aging and in Parkinson’s Disease: A Cross-Sectional Study. Park. Dis. 2018, 2018, 3751516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graf, C. The Lawton instrumental activities of daily living scale. Am. J. Nurs. 2008, 108, 52–62. [Google Scholar] [CrossRef] [Green Version]
- ISO 15189:2022; Medical laboratories—Requirements for quality and competence. International Organization for Standardization: Geneva, Switzerland, 2022.
- Moat, S.J.; Dibden, C.; Tetlow, L.; Griffith, C.; Chilcott, J.; George, R.; Hamilton, L.; Wu, T.H.; MacKenzie, F.; Hall, S.K. Effect of blood volume on analytical bias in dried blood spots prepared for newborn screening external quality assurance. Bioanalysis 2020, 12, 99–109. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| N | Minimum | Maximum | Median | 25–75 P | |
|---|---|---|---|---|---|
| Age | 46 | 69.8 | 95.3 | 84 | 80.3–87.7 |
| Sex | 46 | 15 males | 31 females | ||
| BMI | 43 | 16.2 | 42.2 | 25.5 | 22.1–29.2 |
| IADL | 38 | 0 | 8 | 3 | 1.0–6.0 |
| MMSE | 30 | 3 | 29 | 23.5 | 19.25–25.75 |
| Pearson Correlation Coefficient | p-Value | |
|---|---|---|
| C-reactive protein | 0.984 | p < 0.0001 |
| Apolipoprotein A-IV | 0.931 | p < 0.0001 |
| CD5_antigen-like | 0.919 | p < 0.0001 |
| Alpha-1-antichymotrypsin | 0.874 | p < 0.0001 |
| Lipopolysaccharide-binding_protein | 0.873 | p < 0.0001 |
| Apolipoprotein(a) | 0.872 | p < 0.0001 |
| Haptoglobin | 0.849 | p < 0.0001 |
| Complement_factor_I | 0.845 | p < 0.0001 |
| Beta-Ala-His_dipeptidase | 0.844 | p < 0.0001 |
| Beta-2-microglobulin | 0.83 | p < 0.0001 |
| Neuropilin-2 | 0.822 | p < 0.0001 |
| Serum_amyloid_A-4_protein | 0.816 | p < 0.0001 |
| Retinol-binding protein 4 | 0.81 | p < 0.0001 |
| Apolipoprotein M | 0.794 | p < 0.0001 |
| Complement_component_C9 | 0.781 | p < 0.0001 |
| Protein_AMBP | 0.781 | p < 0.0001 |
| Heparin_cofactor_2 | 0.779 | p < 0.0001 |
| Alpha-2-macroglobulin | 0.764 | p < 0.0001 |
| Prealbumin | 0.76 | p < 0.0001 |
| Complement_C2 | 0.758 | p < 0.0001 |
| Insulin-like_growth_factor_binding_protein_acid_labile_subunit | 0.755 | p < 0.0001 |
| Complement_C4-B | 0.754 | p < 0.0001 |
| Coagulation_factor_XII | 0.747 | p < 0.0001 |
| Apolipoprotein B-100 | 0.738 | p < 0.0001 |
| Complement_factor_D | 0.73 | p < 0.0001 |
| Apolipoprotein C-II | 0.723 | p < 0.0001 |
| Beta-2-glycoprotein 1 | 0.718 | p < 0.0001 |
| Transferrin | 0.708 | p < 0.0001 |
| Coagulation_factor_X | 0.707 | p < 0.0001 |
| Pigment epithelium-derived factor | 0.706 | p < 0.0001 |
| C4b-binding_protein_alpha_chain | 0.7 | p < 0.0001 |
| Alpha-1-acid glycoprotein 1 | 0.691 | p < 0.0001 |
| Apolipoprotein E | 0.689 | p < 0.0001 |
| Complement_C3 | 0.687 | p < 0.0001 |
| Vitamin_K-dependent_protein_S | 0.684 | p < 0.0001 |
| Lumican | 0.674 | p < 0.0001 |
| Fibulin-1 | 0.668 | p < 0.0001 |
| Gelsolin | 0.657 | p < 0.0001 |
| Alpha-2-HS-glycoprotein | 0.651 | p < 0.0001 |
| Cholinesterase | 0.651 | p < 0.0001 |
| Afamin | 0.649 | p < 0.0001 |
| Apolipoprotein D | 0.648 | p < 0.0001 |
| Fibrinogen_alpha_chain | 0.63 | p < 0.0001 |
| sp|P00751|CFAB | 0.626 | p < 0.0001 |
| Inter-alpha-trypsin_inhibitor_heavy_chain_H2 | 0.614 | p < 0.0001 |
| Prothrombin | 0.563 | p < 0.0001 |
| Clusterin | 0.56 | p = 0.0001 |
| Apolipoprotein A-I | 0.545 | p = 0.0001 |
| Complement_C1q_subcomponent_subunit_C | 0.53 | p = 0.0002 |
| Insulin-like_growth_factor-binding_protein_3 | 0.515 | p = 0.0003 |
| Hemopexin | 0.498 | p = 0.0004 |
| Alpha-1B-glycoprotein | 0.468 | p = 0.0010 |
| Thyroxine-binding_globulin | 0.447 | p = 0.0018 |
| Complement_C1q_subcomponent_subunit_B | 0.446 | p = 0.0019 |
| Vitamin_D-binding_protein | 0.442 | p = 0.0021 |
| Complement_C5 | 0.434 | p = 0.0026 |
| Complement_C1r_subcomponent | 0.424 | p = 0.0033 |
| Corticosteroid-binding_globulin | 0.417 | p = 0.0040 |
| Alpha-2-antiplasmin | 0.401 | p = 0.0058 |
| Albumin | 0.319 | p = 0.0307 |
| Antithrombin-III | 0.291 | p = 0.0495 |
| Complement_component_C8_beta_chain | 0.258 | p = 0.0834 |
| Hemoglobin_subunit_alpha | −0.07 | p = 0.6420 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vialaret, J.; Vignon, M.; Badiou, S.; Baptista, G.; Fichter, L.; Dupuy, A.-M.; Maceski, A.M.; Fayolle, M.; Brousse, M.; Cristol, J.-P.; et al. New Perspectives of Multiplex Mass Spectrometry Blood Protein Quantification on Microsamples in Biological Monitoring of Elderly Patients. Int. J. Mol. Sci. 2023, 24, 6989. https://doi.org/10.3390/ijms24086989
Vialaret J, Vignon M, Badiou S, Baptista G, Fichter L, Dupuy A-M, Maceski AM, Fayolle M, Brousse M, Cristol J-P, et al. New Perspectives of Multiplex Mass Spectrometry Blood Protein Quantification on Microsamples in Biological Monitoring of Elderly Patients. International Journal of Molecular Sciences. 2023; 24(8):6989. https://doi.org/10.3390/ijms24086989
Chicago/Turabian StyleVialaret, Jérôme, Margaux Vignon, Stéphanie Badiou, Gregory Baptista, Laura Fichter, Anne-Marie Dupuy, Aleksandra Maleska Maceski, Martin Fayolle, Mehdi Brousse, Jean-Paul Cristol, and et al. 2023. "New Perspectives of Multiplex Mass Spectrometry Blood Protein Quantification on Microsamples in Biological Monitoring of Elderly Patients" International Journal of Molecular Sciences 24, no. 8: 6989. https://doi.org/10.3390/ijms24086989