
Inclisiran—A Revolutionary Addition to a Cholesterol-Lowering Therapy
 ,
,
Abstract
:1. Introduction
2. Causes of Hyperlipidemia
3. The Assessment of Cardiovascular Risk
4. Lipid-Lowering Therapies
4.1. Nonpharmacological Methods
4.2. Statins
4.3. Ezetimibe
4.4. Combined Therapy
4.5. PCSK9 Inhibitors
4.5.1. PCSK9
- Monoclonal antibodies (mAbs)—alirocumab and evolocumab;
- Small interfering RNA (siRNA)—inclisiran.
4.5.2. Anti-PCSK9 Monoclonal Antibodies
5. Inclisiran—A Novel PCSK9 Inhibitor
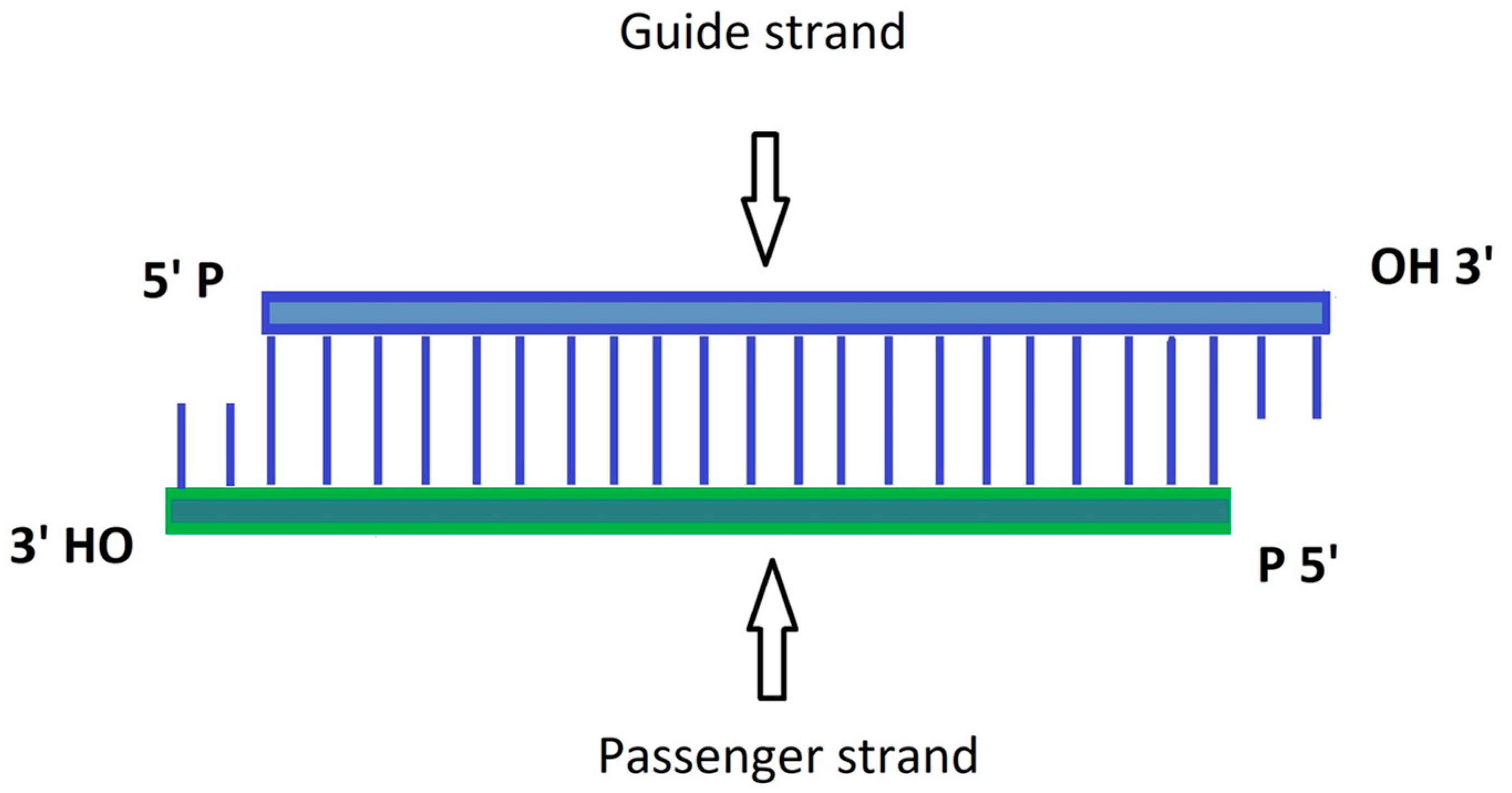
5.1. siRNA
- Patisiran (2018) for hereditary transthyretin-mediated amyloidosis treatment;
- Givosiran (2019) for acute hepatic porphyria therapy;
- Lumasiran (2020) for the treatment of primary hyperoxaluria type 1;
- Inclisiran (2021) as a hypolipidemic drug.
5.2. Inclisiran
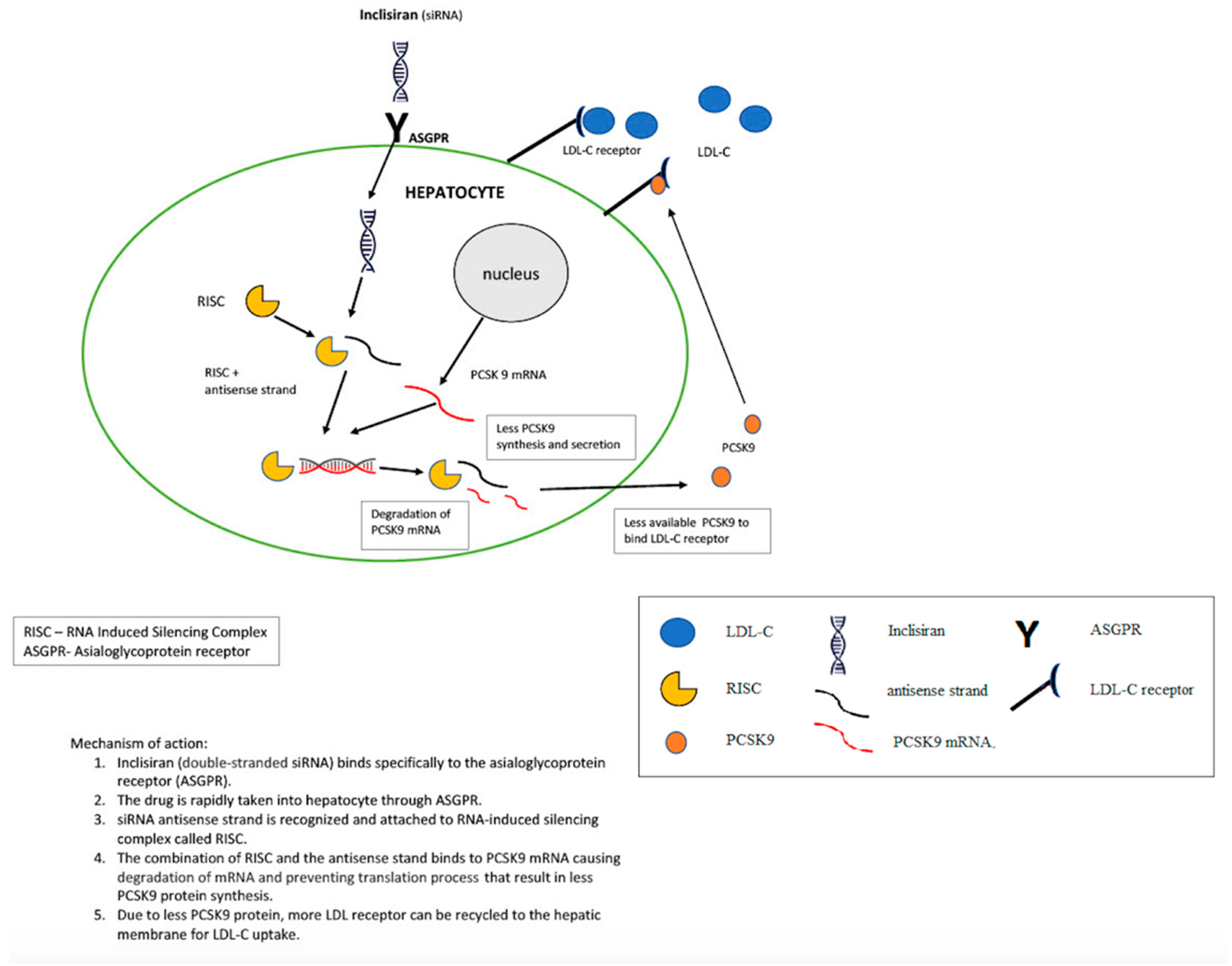
5.2.1. Mechanism of Action
5.2.2. Safety and Adverse Effects
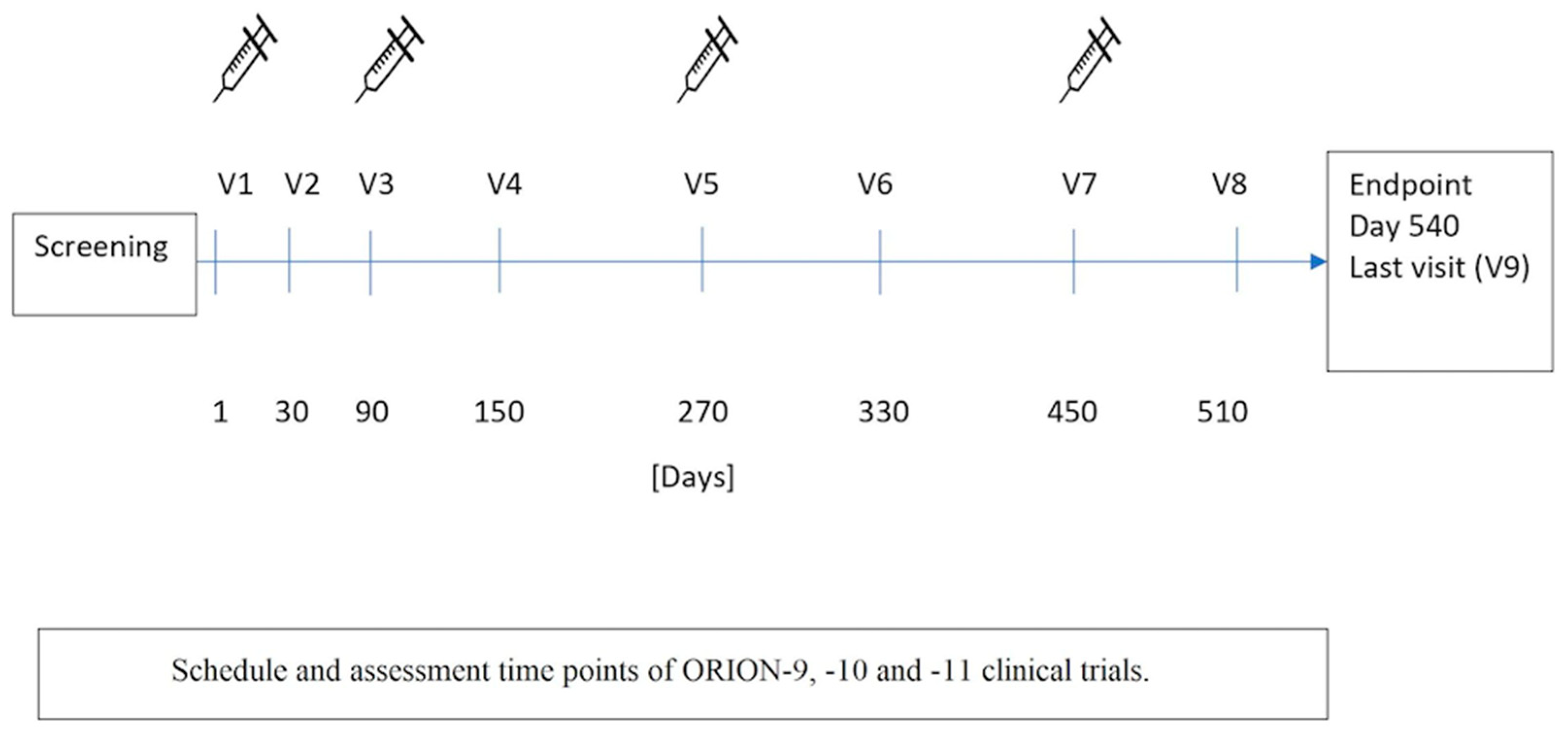
5.2.3. Efficacy
6. Possible Future Lipid-Lowering Treatment
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASCVD | Atherosclerotic cardiovascular disease |
| ASGPRs | Asialoglycoprotein receptors |
| CKD | Chronic kidney disease |
| CRISPR | Clustered regularly interspaced short palindromic repeats |
| CVDs | Cardiovascular diseases |
| eNOS | Endothelial nitric oxide synthase |
| FH | Familial hypercholesterolemia |
| GalNAc | Triantennary N-acetylgalactosamine |
| HeFH | Heterozygous familial hypercholesterolemia |
| HMG-CoA | 3-hydroxy-3-methylglutaryl-coenzyme A |
| HoFH | Homozygous familial hypercholesterolemia |
| IMPROVE-IT | The Improved Reduction of Outcomes: Vytorin Efficacy International Trial |
| LDL-C | Low-density lipoprotein cholesterol |
| LDLR | Low-density lipoprotein receptor |
| LDLRAP | Low-density lipoprotein receptor adaptor protein |
| mAb | Monoclonal antibody |
| MMPs | Matrix metalloproteinases |
| mRNA | Messenger ribonucleic acid |
| NHEJ | Nonhomologous end joining |
| PCSK9 | Proprotein convertase subtilisin/kexin type 9 |
| PREDIMED | PREvención con DIeta MEDiterránea |
| PROCAM | Prospective Cardiovascular Münster |
| RACING | Randomized comparison of efficacy and safety of lipid lowering with statin monotherapy versus statin–ezetimibe combination for high-risk cardiovascular disease |
| SCORE2 | Systematic Coronary Risk Estimation 2 |
| siRNA | Small interfering ribonucleic acid |
References
- Tejada, S.; Martorell, M.; Capo, X.; Tur, J.; Pons, A.; Sureda, A. Coumarin and Derivates as Lipid Lowering Agents. Curr. Top. Med. Chem. 2016, 17, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Bułdak, Ł.; Marek, B.; Kajdaniuk, D.; Urbanek, A.; Janyga, S.; Bołdys, A.; Basiak, M.; Maligłówka, M.; Okopień, B. Endocrine diseases as causes of secondary hyperlipidemia. Endokrynol. Pol. 2019, 70, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viñals, C.; Zambón, D.; Yago, G.; Domenech, M.; Ortega, E. Secondary hypertriglyceridemia. Clin. Investig. Arterioscler. 2021, 33, 29–36. [Google Scholar] [PubMed]
- Vallejo-Vaz, A.J.; Akram, A.; Seshasai, S.R.K.; Cole, D.; Watts, G.F.; Hovingh, G.K. Pooling and expanding registries of familial hypercholesterolaemia to assess gaps in care and improve disease management and outcomes: Rationale and design of the global EAS Familial Hypercholesterolaemia Studies Collabo-ration. Atheroscler. Suppl. 2016, 22, 1–32. [Google Scholar] [CrossRef]
- Singh, S.; Bittner, V. Familial hypercholesterolemia--epidemiology, diagnosis, and screening. Curr. Atheroscler. Rep. 2015, 17, 482. [Google Scholar] [CrossRef]
- Martinez-Hervas, S.; Ascaso, J.F. Hypercholesterolemia. In Encyclopedia of Endocrine Diseases, 2nd ed.; Huhtaniemi, I., Martini, L., Eds.; Academic Press: Oxford, UK, 2019; pp. 320–326. [Google Scholar]
- Benito-Vicente, A.; Uribe, K.B.; Jebari, S.; Galicia-Garcia, U.; Ostolaza, H.; Martin, C. Molecular Sciences Familial Hypercholesterolemia: The Most Frequent Cholesterol Metabolism Disorder Caused Disease. Int. J. Mol. Sci 2018, 19, 3426. [Google Scholar] [CrossRef] [Green Version]
- Karr, S. Epidemiology and management of hyperlipidemia. Am. J. Manag. Care 2017, 23, S139–S148. [Google Scholar]
- Li, J.; Lei, X.; Yang, X. Effectiveness and safety of Inclisiran in hyperlipidemia treatment: An overview of systematic reviews. Medicine 2023, 102, e32728. [Google Scholar] [CrossRef]
- Smith, K.W.; White, C.M. Inclisiran: A Novel Small Interfering RNA Drug for Low-Density Lipoprotein Reduction. J. Clin. Pharmacol. 2022, 62, 1079–1085. [Google Scholar] [CrossRef]
- Banach, M.; Kaźmierczak, J.; Mitkowski, P.; Wita, K.; Broncel, M.; Gąsior, M.; Witkowski, A. Which patients at risk of cardiovascular disease might benefit the most from inclisiran? Polish experts’ opinion. The compromise between EBM and possibilities in healthcare. Arch. Med. Sci. 2022, 18, 569–576. [Google Scholar] [CrossRef]
- Nelson, R.H. Hyperlipidemia as a Risk Factor for Cardiovascular Disease. Prim. Care Clin. Off. Pract. 2012, 40, 195–211. [Google Scholar] [CrossRef] [Green Version]
- SCORE2 Working Group and ESC Cardiovascular Risk Collaboration. SCORE2 risk prediction algorithms: New models to estimate 10-year risk of cardiovascular disease in Europe. Eur. Heart J. 2021, 42, 2439–2454. [Google Scholar] [CrossRef]
- Ritchie, H.; Spooner, F.; Roser, M. “Causes of Death”. Published Online at OurWorldInData.org. 2018. Available online: https://ourworldindata.org/causes-of-death (accessed on 20 January 2023).
- The Top 10 Causes of Death–Factsheet. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 25 October 2022).
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Wiklund, O. ESC Scientific Document Group, 2019 ESC/EAS Guidelines for the management of dyslipidaemias: Lipid modifi-cation to reduce cardiovascular risk: The Task Force for the management of dyslipidaemias of the European Society of Cardi-ology (ESC) and European Atherosclerosis Society (EAS). Eur. Heart J. 2020, 41, 111–188. [Google Scholar]
- Hippisley-Cox, J.; Coupland, C.; Vinogradova, Y.; Robson, J.; Brindle, P. Performance of the QRISK cardiovascular risk prediction algorithm in an independent UK sample of patients from general practice: A validation study. Heart 2008, 94, 34–39. [Google Scholar] [CrossRef] [Green Version]
- D’Agostino, R.B., Sr.; Grundy, S.; Sullivan, L.M.; Wilson, P.; CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigation. JAMA 2001, 286, 180–187. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of Coronary Heart Disease Using Risk Factor Categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.A.; Miller, G.J.; Humphries, S.E. A comparison of the PROCAM and Framingham point-scoring systems for estimation of individual risk of coronary heart disease in the Second Northwick Park Heart Study. Atherosclerosis 2005, 181, 93–100. [Google Scholar] [CrossRef]
- Schwingshackl, L.; Bogensberger, B.; Benčič, A.; Knüppel, S.; Boeing, H.; Hoffmann, G. Effects of oils and solid fats on blood lipids: A systematic review and network meta-analysis. J. Lipid Res. 2018, 59, 1771–1782. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Enkhmaa, B.; Surampudi, P.; Anuurad, E.; Berglund, L. Lifestyle Changes: Effect of Diet, Exercise, Functional Food, and Obesity Treatment on Lipids and Lipoproteins. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Blackman, M.R., Eds.; South Dartmouth: Dartmouth, MA, USA, 2018; MDText.com. Available online: https://www.ncbi.nlm.nih.gov/books/NBK326737/ (accessed on 20 January 2023).
- Musa-Veloso, K.; Poon, T.H.; Elliot, J.A.; Chung, C. A comparison of the LDL-cholesterol lowering efficacy of plant stanols and plant sterols over a continuous dose range: Results of a meta-analysis of randomized, placebo-controlled trials. Prostaglandins Leukot. Essent. Fat. Acids 2011, 85, 9–28. [Google Scholar] [CrossRef]
- De Backer, G.G. Food supplements with red yeast rice: More regulations are needed. Eur. J. Prev. Cardiol. 2017, 24, 1429–1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.; Karl, M.; Santini, A. Red Yeast Rice. Foods 2017, 6, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS); Younes, M.; Aggett, P.; Aguilar, F.; Crebelli, R.; Dusemund, B.; Wright, M. Scientific opinion on the safety of monacolins in red yeast rice. EFSA J. 2018, 16, e05368. [Google Scholar] [PubMed] [Green Version]
- The American College of Cardiology. Odyssey High FH. Presented at Henry N. Ginsberg at the American Heart Association Scientific Sessions, Chicago, IL, USA. 19 November 2014. Available online: http://www.acc.org/latest-in-cardiology/clinical-trials/2014/11/18/15/23/odyssey-high-fh (accessed on 9 December 2015).
- Reiner, Z.; Catapano, A.L.; De Backer, G.; Graham, I.; Taskinen, M.R.; Wiklund, O.; Zamorano, J.L. ESC/EAS Guidelines for the management of dyslipidaemias: The Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur. Heart J. 2011, 32, 1769–1818. [Google Scholar] [PubMed] [Green Version]
- Wożakowska-Kapłon, B. Treatment of hypercholesterolaemia in cardiovascular diseases—What target, which statin, what dose? Folia Cardiol. 2014, 9, 55–66. [Google Scholar]
- Liao, J.K.; Laufs, U. Pleiotropic effects of statins. Annu. Rev. Pharmacol Toxicol. 2005, 45, 89–118. [Google Scholar] [CrossRef] [Green Version]
- Kavalipati, N.; Shah, J.; Ramakrishan, A.; Vasnawala, H. Pleiotropic effects of statins. Indian J. Endocrinol. Metab. 2015, 19, 554–562. [Google Scholar]
- Endo, A. A historical perspective on the discovery of statins. Proc. Jpn. Acad. Ser. B 2010, 86, 484–493. [Google Scholar] [CrossRef] [Green Version]
- Climent, E.; Benaiges, D.; Pedro-Botet, J. Hydrophilic or Lipophilic Statins? Front. Cardiovasc. Med. 2021, 8, 687585. [Google Scholar] [CrossRef]
- Pinal-Fernandez, I.; Casal-Dominguez, M.; Mammen, A.L. Statins: Pros and cons. Med. Clin. 2018, 150, 398–402. [Google Scholar] [CrossRef]
- Ramkumar, S.; Raghunath, A.; Raghunath, S. Statin Therapy: Review of Safety and Potential Side Effects. Acta Cardiol. Sin. 2016, 32, 631–639. [Google Scholar] [PubMed]
- Curran, M.P.; Goa, K.L. Lovastatin extended release: A review of its use in the management of hypercholesterolaemia. Drugs 2003, 63, 685–699. [Google Scholar] [CrossRef]
- Pedersen, T.R.; Tobert, J.A. Simvastatin: A review. Expert Opin. Pharmacother. 2004, 5, 2583–2596. [Google Scholar] [CrossRef]
- Adams, S.P.; Sekhon, S.S.; Wright, J.M. Lipid lowering efficacy of rosuvastatin. Cochrane Database Syst. Rev. 2014, 2014, CD010254. [Google Scholar] [CrossRef] [Green Version]
- Karlson, B.W.; Palmer, M.K.; Nicholls, S.; Lundman, P.; Barter, P.J. Doses of rosuvastatin, atorvastatin and simvastatin that induce equal reductions in LDL-C and non-HDL-C: Results from the VOYAGER meta-analysis. Eur. J. Prev. Cardiol. 2015, 23, 744–747. [Google Scholar] [CrossRef]
- Toth, P.; Phan, B.A.; Dayspring, T. Ezetimibe therapy: Mechanism of action and clinical update. Vasc. Health Risk Manag. 2012, 8, 415–427. [Google Scholar] [CrossRef] [Green Version]
- Florentin, M.; Liberopoulos, E.N.; Elisaf, M.S. Ezetimibe-associated adverse effects: What the clinician needs to know. Int. J. Clin. Pract. 2007, 62, 88–96. [Google Scholar] [CrossRef]
- Pandor, A.; Ara, R.M.; Tumur, I.; Wilkinson, A.J.; Paisley, S.; Duenas, A.; Durrington, P.N.; Chilcott, J. Ezetimibe monotherapy for cholesterol lowering in 2722 people: Systematic review and meta-analysis of randomized controlled trials. J. Intern. Med. 2009, 265, 568–580. [Google Scholar] [CrossRef]
- Hammersley, D.; Signy, M. Ezetimibe: An update on its clinical usefulness in specific patient groups. Ther. Adv. Chronic Dis. 2016, 8, 4–11. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.K.; Hong, S.J.; Lee, Y.J.; Hong, S.J.; Yun, K.H.; Hong, B.K. RACING investigators. Long-term efficacy and safety of moderate-intensity statin with ezetimibe combination therapy versus high-intensity statin monotherapy in patients with atherosclerotic cardiovascular disease (RACING): A randomised, open-label, non-inferiority trial. Lancet 2022, 400, 380–390. [Google Scholar]
- Starzyk, K.; Wożakowska-Kapłon, B. Gdy statyna to za mało—Skojarzenie statyny z ezetimibem w terapii hipercholesterolemii. Folia Cardiol. 2016, 10, 428–437. [Google Scholar] [CrossRef] [Green Version]
- Gagné, C.; Gaudet, D.; Bruckert, E. Efficacy and Safety of Ezetimibe Coadministered With Atorvastatin or Simvastatin in Patients With Homozygous Familial Hypercholesterolemia. Circulation 2002, 105, 2469–2475. [Google Scholar] [CrossRef]
- Davidson, M.; Ballantyne, C.; Kerzner, B.; Melani, L.; Sager, P.; Lipka, L.; Strony, J.; Suresh, R.; Veltri, E. Efficacy and safety of ezetimibe coadministered with statins: Randomised, placebo-controlled, blinded experience in 2382 patients with primary hypercholesterolemia. Int. J. Clin. Pract. 2004, 58, 746–755. [Google Scholar] [CrossRef] [PubMed]
- Kerzner, B.; Corbelli, J.; Sharp, S.; Lipka, L.J.; Melani, L.; LeBeaut, A.; Suresh, R.; Mukhopadhyay, P.; Veltri, E.P. Efficacy and safety of ezetimibe coadministered with lovastatin in primary hypercholesterolemia. Am. J. Cardiol. 2003, 91, 418–424. [Google Scholar] [CrossRef]
- Xia, X.-D.; Peng, Z.-S.; Gu, H.-M.; Wang, M.; Wang, G.-Q.; Zhang, D.-W. Regulation of PCSK9 Expression and Function: Mechanisms and Therapeutic Implications. Front. Cardiovasc. Med. 2021, 8, 764038. [Google Scholar] [CrossRef]
- Schlüter, K.-D.; Wolf, A.; Schreckenberg, R. Coming Back to Physiology: Extra Hepatic Functions of Proprotein Convertase Subtilisin/Kexin Type 9. Front. Physiol. 2020, 11, 598649. [Google Scholar] [CrossRef]
- Chiang, L.W.; Grenier, J.M.; Ettwiller, L.; Jenkins, L.P.; Ficenec, D.; Martin, J.; Jin, F.; DiStefano, P.S.; Wood, A. An orches-trated gene expression component of neuronal programmed cell death revealed by cDNA array analysis. Proc. Natl. Acad. Sci. USA 2001, 98, 2814–2819. [Google Scholar] [CrossRef] [Green Version]
- Blanchard, V.; Khantalin, I.; Ramin-Mangata, S.; Chémello, K.; Nativel, B.; Lambert, G. PCSK9: From biology to clinical applications. Pathology 2018, 51, 177–183. [Google Scholar] [CrossRef]
- Melendez, Q.M.; Krishnaji, S.T.; Wooten, C.J.; Lopez, D. Hypercholesterolemia: The role of PCSK9. Arch. Biochem. Biophys. 2017, 625–626, 39–53. [Google Scholar] [CrossRef]
- Oleaga, C.; Hay, J.; Gurcan, E.; David, L.L.; Mueller, P.A.; Tavori, H.; Shapiro, M.D.; Pamir, N.; Fazio, S. Insights into the kinetics and dynamics of the furin-cleaved form of PCSK9. J. Lipid Res. 2021, 62, 100003. [Google Scholar] [CrossRef]
- Benjannet, S.; Rhainds, D.; Hamelin, J.; Nassoury, N.; Seidah, N.G. The proprotein convertase (PC) PCSK9 is inactivated by furin and/or PC5/6A: Functional consequences of natural mutations and post-translational modifications. J. Biol. Chem. 2006, 281, 30561–30572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, A.; Kanazawa, M.; Kagaya, Y.; Kondo, M.; Sato, K.; Endo, H.; Nozaki, E. Plasma kinetics of mature PCSK9, furin-cleaved PCSK9, and Lp(a) with or without administration of PCSK9 inhibitors in acute myocardial infarction. J. Cardiol. 2020, 76, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, Y.; Harada-Shiba, M.; Nakao, K.; Nakashima, T.; Kawakami, S.; Fujino, M.; Kanaya, T.; Nagai, T.; Tahara, Y.; Asaumi, Y.; et al. Mature proprotein convertase subtilisin/kexin type 9, coronary atheroma burden, and vessel remodeling in heterozygous familial hypercholesterolemia. J. Clin. Lipidol. 2017, 11, 413–421.e3. [Google Scholar] [CrossRef] [PubMed]
- Lipari, M.T.; Li, W.; Moran, P.; Kong-Beltran, M.; Sai, T.; Lai, J.; Lin, S.J.; Kolumam, G.; Zavala-Solorio, J.; Izrael-Tomasevic, A.; et al. Furin-cleaved proprotein convertase subtilisin/kexin type 9 (PCSK9) is active and modulates low density lipoprotein receptor and serum cholesterol levels. J. Biol. Chem. 2012, 287, 43482–43491. [Google Scholar] [CrossRef] [Green Version]
- Soffer, D.; Stoekenbroek, R.; Plakogiannis, R. Small interfering ribonucleic acid for cholesterol lowering–Inclisiran: Inclisiran for cholesterol lowering. J. Clin. Lipidol. 2022, 16, 574–582. [Google Scholar] [CrossRef] [PubMed]
- Dyrbuś, K.; Gąsior, M.; Penson, P.; Ray, K.K.; Banach, M. Inclisiran-New hope in the management of lipid disorders? J. Clin. Lipidol. 2020, 14, 16–27. [Google Scholar] [CrossRef]
- Stoekenbroek, R.M.; Lambert, G.; Cariou, B.; Hovingh, G.K. Inhibiting PCSK9—Biology beyond LDL control. Nat. Rev. Endocrinol. 2018, 15, 52–62. [Google Scholar] [CrossRef]
- Maxwell, K.N.; Fisher, E.A.; Breslow, J.L. Overexpression of PCSK9 accelerates the degradation of the LDLR in a post-endoplasmic reticulum compartment. Proc. Natl. Acad. Sci. USA 2005, 102, 2069–2074. [Google Scholar] [CrossRef] [Green Version]
- Abifadel, M.; Varret, M.; Rabès, J.-P.; Allard, D.; Ouguerram, K.; Devillers, M.; Cruaud, C.; Benjannet, S.; Wickham, L.; Erlich, D.; et al. Mutations in PCSK9 cause autosomal dominant hypercholesterolemia. Nat. Genet. 2003, 34, 154–156. [Google Scholar] [CrossRef]
- Chaudhary, R.; Garg, J.; Shah, N.; Sumner, A. PCSK9 inhibitors: A new era of lipid lowering therapy. World J. Cardiol. 2017, 9, 76–91. [Google Scholar] [CrossRef]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef]
- O’Donoghue, M.L.; Giugliano, R.P.; Wiviott, S.D.; Atar, D.; Keech, A.; Kuder, J.F.; Im, K.; Murphy, S.A.; Flores-Arredondo, J.H.; López, J.A.G.; et al. Long-Term Evolocumab in Patients with Established Atherosclerotic Cardiovascular Dis-ease. Circulation 2022, 146, 1109–1119. [Google Scholar] [CrossRef]
- Regeneron and Sanofi Announce Positive Topline Results from First Phase 3 Trials Evaluating Monthly Dosing of Alirocumab in Patients with Hypercholesterolemia. Available online: http://www.prnewswire.com/news-releases/regeneron-and-sanofi-announce-positive-topline-results-from-first-phase-3-trials-evaluating-monthly-dosing-of-alirocumab-in-patients-with-hypercholesterolemia-300017492.html (accessed on 9 December 2015).
- Stroes, E.; Colquhoun, D.; Sullivan, D.; Civeira, F.; Rosenson, R.S.; Watts, G.F.; Rocco, M.; GAUSS-2 Investigators. Anti-PCSK9 antibody effectively lowers cholesterol in patients with statin intolerance: The GAUSS-2 randomized, placebo-controlled phase 3 clinical trial of evolocumab. J. Am. Coll. Cardiol. 2014, 63, 2541–2548. [Google Scholar] [CrossRef] [Green Version]
- Raal, F.J.; Stein, E.A.; Dufour, R.; Turner, T.; Civeira, F.; Burgess, L.; Langslet, G.; Scott, R.; Olsson, A.G.; Sullivan, D.; et al. PCSK9 inhibition with evolocumab (AMG 145) in heterozygous familial hypercholesterolaemia (RUTHERFORD-2): A randomised, double-blind, placebo-controlled trial. Lancet 2014, 385, 331–340. [Google Scholar] [CrossRef]
- Alshaer, W.; Zureigat, H.; Al Karaki, A.; Al-Kadash, A.; Gharaibeh, L.; Hatmal, M.M.; Aljabali, A.A.; Awidi, A. siRNA: Mechanism of action, challenges, and therapeutic approaches. Eur. J. Pharmacol. 2021, 905, 174178. [Google Scholar] [CrossRef]
- Banerjee, Y.; Stoian, A.P.; Cicero, A.F.G.; Fogacci, F.; Nikolic, D.; Sachinidis, A.; Rizvi, A.A.; Janez, A.; Rizzo, M. Inclisiran: A small interfering RNA strategy targeting PCSK9 to treat hypercholesterolemia. Expert Opin. Drug Saf. 2021, 21, 9–20. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Addison, M.L.; Dear, J.W.; Webb, D.J. Small interfering RNA: Discovery, pharmacology and clinical de-velopment-An introductory review. Br. J. Pharmacol. 2022. [CrossRef]
- Zhang, M.M.; Bahal, R.; Rasmussen, T.P.; Manautou, J.E.; Zhong, X.B. The growth of siRNA-based therapeutics: Updated clinical studies. Biochem. Pharmacol. 2021, 189, 114432. [Google Scholar] [CrossRef]
- Traber, G.M.; Yu, A.-M. RNAi-Based Therapeutics and Novel RNA Bioengineering Technologies. Experiment 2022, 384, 133–154. [Google Scholar] [CrossRef]
- Lamb, Y.N. Inclisiran: First Approval. Drugs 2021, 81, 389–395. [Google Scholar] [CrossRef]
- Prakash, T.P.; Graham, M.J.; Yu, J.; Carty, R.; Low, A.; Chappell, A.; Schmidt, K.; Zhao, C.; Aghajan, M.; Murray, H.F.; et al. Targeted delivery of antisense oligonucleotides to hepatocytes using triantennary N-acetyl galactosamine improves potency 10-fold in mice. Nucleic Acids Res. 2014, 42, 8796–8807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khvorova, A. Oligonucleotide Therapeutics—A New Class of Cholesterol-Lowering Drugs. N. Engl. J. Med. 2017, 376, 4–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Medicines Agency. Available online: https://www.ema.europa.eu (accessed on 1 October 2021).
- Merćep, I.; Friščić, N.; Strikić, D.; Reiner, Ž. Advantages and Disadvantages of Inclisiran: A Small Interfering Ribonucleic Acid Molecule Targeting PCSK9—A Narrative Review. Cardiovasc. Ther. 2022, 2022, 8129513. [Google Scholar] [CrossRef]
- Strilchuck, L.; Fogacci, F.; Cicero, A.F. Safety and tolerability of injectable lipid-lowering drugs: An update of clinical data. Expert Opin. Drug Saf. 2019, 18, 611–621. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Troquay, R.P.T.; Visseren, F.L.J.; Leiter, L.A.; Wright, R.S.; Vikarunnessa, S.; Talloczy, Z.; Zang, X.; Maheux, P.; Lesogor, A.; et al. Long-term efficacy and safety of inclisiran in patients with high cardiovascular risk and elevated LDL cholesterol (ORION-3): Results from the 4-year open-label extension of the ORION-1 trial. Lancet Diabetes Endocrinol. 2023, 11, 109–119. [Google Scholar] [CrossRef]
- Chi, X.; Gatti, P.; Papoian, T. Safety of antisense oligonucleotide and siRNA-based therapeutics. Drug Discov. Today 2017, 22, 823–833. [Google Scholar] [CrossRef]
- Cicero, A.F.G.; Fogacci, F.; Zambon, A.; Toth, P.P.; Borghi, C. Efficacy and safety of inclisiran a newly approved FDA drug: A systematic review and pooled analysis of available clinical studies. Am. Heart J. 2022, 13, 100127. [Google Scholar] [CrossRef]
- Roth, E.M.; Goldberg, A.C.; Catapano, A.L.; Torri, A.; Yancopoulos, G.D.; Stahl, N.; Brunet, A.; Lecorps, G.; Colhoun, H.M. Antidrug Antibodies in Patients Treated with Alirocumab. N. Engl. J. Med. 2017, 376, 1589–1590. [Google Scholar] [CrossRef] [Green Version]
- Wright, R.S.; Collins, M.G.; Stoekenbroek, R.M.; Robson, R.; Wijngaard, P.L.; Landmesser, U.; Leiter, L.A.; Kastelein, J.J.; Ray, K.K.; Kallend, D. Effects of Renal Impairment on the Pharmacokinetics, Efficacy, and Safety of Inclisiran: An Analysis of the ORION-7 and ORION-1 Studies. Mayo Clin. Proc. 2019, 95, 77–89. [Google Scholar] [CrossRef] [Green Version]
- Zijlstra, L.E.; Trompet, S.; Mooijaart, S.P.; van Buren, M.; Jukema, J.W. Renal Impairment, Cardiovascular Disease, and the Short-Term Efficacy and Safety of PCSK9 Targeted by Inclisiran. Mayo Clin. Proc. 2020, 95, 12–14. [Google Scholar] [CrossRef] [Green Version]
- Coppinger, C.; Movahed, M.R.; Azemawah, V.; Peyton, L.; Gregory, J.; Hashemzadeh, M. A Comprehensive Review of PCSK9 Inhibitors. J. Cardiovasc. Pharmacol. Ther. 2022, 27, 10742484221100107. [Google Scholar] [CrossRef]
- Hermel, M.; Lieberman, M.; Slipczuk, L.; Rana, J.S.; Virani, S.S. Monoclonal Antibodies, Gene Silencing and Gene Editing (CRISPR) Therapies for the Treatment of Hyperlipidemia-The Future Is Here. Pharmaceutics. 2023, 15, 459. [Google Scholar] [CrossRef]
- Vijay, N.; Ali, A. Inclisiran: A Game Changer in a Changing Game. J. Am. Coll. Cardiol. 2021, 77, 1194–1196. [Google Scholar]
- Gupta, S. LDL Cholesterol, Statins And PCSK 9 Inhibitors. Indian Heart J. 2015, 67, 419–424. [Google Scholar] [CrossRef] [Green Version]
- Pirillo, A.; Catapano, A.L. Inclisiran: How Widely and When Should We Use It? Curr. Atheroscler. Rep. 2022, 24, 803–811. [Google Scholar] [CrossRef]
- Koenig, W.; Conde, L.G.; Landmesser, U.; Leiter, L.A.; Ray, K.K.; Schwartz, G.G.; Raal, F.J. Efficacy and Safety of Inclisiran in Patients with Polyvascular Disease: Pooled, Post Hoc Analysis of the ORION-9, ORION-10, and ORION-11 Phase 3 Randomized Controlled Trials. Cardiovasc Drugs Ther. 2022. Available online: https://linkspringer.53yu.com/article/10.1007/s10557-022-07413-0 (accessed on 23 January 2023). [CrossRef]
- Ray, K.K.; Raal, F.J.; Kallend, D.G.; Jaros, M.J.; Koenig, W.; Leiter, L.A. Clinical Research Epidemiology and prevention Inclisiran and cardiovascular events: A patient-level analysis of phase III trials. Eur. Heart J. 2022, 44, 129–138. [Google Scholar] [CrossRef]
- Raal, F.J.; Kallend, D.; Ray, K.K.; Turner, T.; Koenig, W.; Wright, R.S.; Wijngaard, P.L.; Curcio, D.; Jaros, M.J.; Leiter, L.A.; et al. Inclisiran for the Treatment of Heterozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 382, 1520–1530. [Google Scholar] [CrossRef]
- U.S. National Library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/results/NCT03851705 (accessed on 15 January 2023).
- Kramer, A.I.; Akioyamen, L.E.; Lee, S.; Bélanger, A.; Ruel, I.; Hales, L.; Genest, J.; Brunham, L.R. Major adverse cardiovascular events in homozygous familial hypercholesterolaemia: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2021, 29, 817–828. [Google Scholar] [CrossRef]
- Bianconi, V.; Banach, M.; Pirro, M. Why patients with familial hypercholesterolemia are at high cardiovascular risk? Beyond LDL-C levels. Trends Cardiovasc. Med. 2020, 31, 205–215. [Google Scholar] [CrossRef]
- Aldono, R.; Díaz-Díaz, J.L.; Arrieta, F.; Fuentes-Jimenez, F.; Illán, F.; Mata, F. Current Therapy for Homozygous Familial Hypercholesterolaemia. EMJ. 2021, 6, 76–86. [Google Scholar]
- Nordestgaard, B.G.; Chapman, M.J.; Ray, K.; Borén, J.; Andreotti, F.; Watts, G.; Ginsberg, H.; Amarenco, P.; Catapano, A.L.; Descamps, O.S.; et al. Lipoprotein(a) as a cardiovascular risk factor: Current status. Eur. Heart J. 2010, 31, 2844–2853. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.A.; Park, H.-J. New Therapeutic Approaches to the Treatment of Dyslipidemia 2: LDL-C and Lp(a). J. Lipid Atheroscler. 2023, 12, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Ballantyne, C.M. Existing and emerging strategies to lower Lipoprotein(a). Atherosclerosis 2022, 349, 110–122. [Google Scholar] [CrossRef]
- Walker, H.E.; Rizzo, M.; Fras, Z.; Jug, B.; Banach, M.; Penson, P.E. CRISPR Gene Editing in Lipid Disorders and Athero-sclerosis: Mechanisms and Opportunities. Metabolites 2021, 9, 857. [Google Scholar] [CrossRef]
- Hille, F.; Charpentier, E. CRISPR-Cas: Biology, mechanisms and relevance. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2016, 371, 20150496. [Google Scholar] [CrossRef] [Green Version]
- Chadwick, A.C.; Musunuru, K. Genome Editing for the Study of Cardiovascular Diseases. Curr. Cardiol. Rep. 2017, 19, 22. [Google Scholar] [CrossRef]
- Strong, A.; Musunuru, K. Genome editing in cardiovascular diseases. Nat. Rev. Cardiol. 2016, 14, 11–20. [Google Scholar] [CrossRef]
- Ding, Q.; Strong, A.; Patel, K.M.; Ng, S.-L.; Gosis, B.S.; Regan, S.N.; Cowan, C.A.; Rader, D.J.; Musunuru, K. Permanent Alteration of PCSK9 With In Vivo CRISPR-Cas9 Genome Editing. Circ. Res. 2014, 115, 488–492. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Raghavan, A.; Chen, T.; Qiao, L.; Zhang, Y.; Ding, Q.; Musunuru, K. CRISPR-Cas9 Targeting of PCSK9 in Human Hepatocytes In Vivo—Brief Report. Arter. Thromb. Vasc. Biol. 2016, 36, 783–786. [Google Scholar] [CrossRef] [Green Version]
- Ran, F.A.; Cong, L.; Yan, W.X.; Scott, D.A.; Gootenberg, J.S.; Kriz, A.J.; Zetsche, B.; Shalem, O.; Wu, X.; Makarova, K.S.; et al. In vivo genome editing using Staphylococcus aureus Cas9. Nature 2015, 520, 186–191. [Google Scholar] [CrossRef] [Green Version]
- Arnold, N.; Koenig, W. PCSK9 Inhibitor Wars: How Does Inclisiran Fit in with Current Monoclonal Antibody Inhibitor Therapy? Considerations for Patient Selection. Curr. Cardiol. Rep. 2022, 24, 1657–1667. [Google Scholar] [CrossRef]
- Stein, E.; Toth, P.; Butcher, M.; Kereiakes, D.; Magnu, P.; Bays, H.; Zhou, R.; Turner, T. Safety, Tolerability and Ldl-C Reduction with a Novel Anti-Pcsk9 Recombinant Fusion Protein (Lib003): Results of A Randomized, Double-Blind, Placebo-Controlled, Phase 2 Study. Atherosclerosis 2019, 287, e7. [Google Scholar] [CrossRef]
- Gennemark, P.; Walter, K.; Clemmensen, N.; Rekić, D.; Nilsson, C.A.; Knöchel, J.; Davies, N. An oral antisense oligonucleotide for PCSK9 inhibition. Sci. Transl. Med. 2021, 13, eabe9117. [Google Scholar] [CrossRef]
- ClinicalTrials.gov NCT05261126. A Study of the Efficacy and Safety of MK-0616 (Oral PCSK9 Inhibitor) in Adults with Hyper-cholesterolemia (MK-0616-008). Available online: https://clinicaltrials.gov/ct2/show/NCT05261126 (accessed on 17 June 2022).
- Liu, C.; Chen, J.; Chen, H.; Zhang, T.; He, D.; Luo, Q.; Chi, J.; Hong, Z.; Liao, Y.; Zhang, S.; et al. PCSK9 Inhibition: From Current Advances to Evolving Future. Cells 2022, 11, 2972. [Google Scholar] [CrossRef]
- Johns, D.G.; Almonte, A.; Bautmans, A.; Campeau, L.; Cancilla, M.T.; Chapman, J.; Banka, P. The clinical safety, pharmacokinetics, and LDL-cholesterol lowering efficacy of MK-0616, an oral PCSK9 inhibitor. Circulation 2021, 144, e573. [Google Scholar]
- Sahebkar, A.; Momtazi-Borojeni, A.A.; Banach, M. PCSK9 vaccine: So near, yet so far! Eur. Heart J. 2021, 42, 4007–4010. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Anti-PCSK9 Monoclonal Antibodies (Evolocumab, Alirocumab) | siRNA Targeting PCSK9 (Inclisiran) | |
|---|---|---|
| Route of administration | Injectable (s.c.) | Injectable (s.c.) |
| Dose | 140 mg/420 mg | 284 mg |
| Dosing frequency | Every two weeks or once monthly | 0–90–180 days and every 6 months thereafter |
| LDL-C plasma level reduction [88,89] | ~ 50–60% | ~ 50% |
| PCSK9 reduction [82,89] | ~90% | ~ 60–80% |
| Relative reduction in cardiovascular events | ~15% | ~17% |
| Mechanism of action | Blocking of the extracellular interaction of PCSK9 LDLR | PCSK9 synthesis inhibition through RNA interference |
| Advantages |
|
|
| Disadvantages |
|
|
| Adverse effects [90,91] |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dec, A.; Niemiec, A.; Wojciechowska, E.; Maligłówka, M.; Bułdak, Ł.; Bołdys, A.; Okopień, B. Inclisiran—A Revolutionary Addition to a Cholesterol-Lowering Therapy. Int. J. Mol. Sci. 2023, 24, 6858. https://doi.org/10.3390/ijms24076858
Dec A, Niemiec A, Wojciechowska E, Maligłówka M, Bułdak Ł, Bołdys A, Okopień B. Inclisiran—A Revolutionary Addition to a Cholesterol-Lowering Therapy. International Journal of Molecular Sciences. 2023; 24(7):6858. https://doi.org/10.3390/ijms24076858
Chicago/Turabian StyleDec, Adrianna, Aleksandra Niemiec, Eliza Wojciechowska, Mateusz Maligłówka, Łukasz Bułdak, Aleksandra Bołdys, and Bogusław Okopień. 2023. "Inclisiran—A Revolutionary Addition to a Cholesterol-Lowering Therapy" International Journal of Molecular Sciences 24, no. 7: 6858. https://doi.org/10.3390/ijms24076858