
Neutrophil Extracellular Traps and Platelet Activation for Identifying Severe Episodes and Clinical Trajectories in COVID-19
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
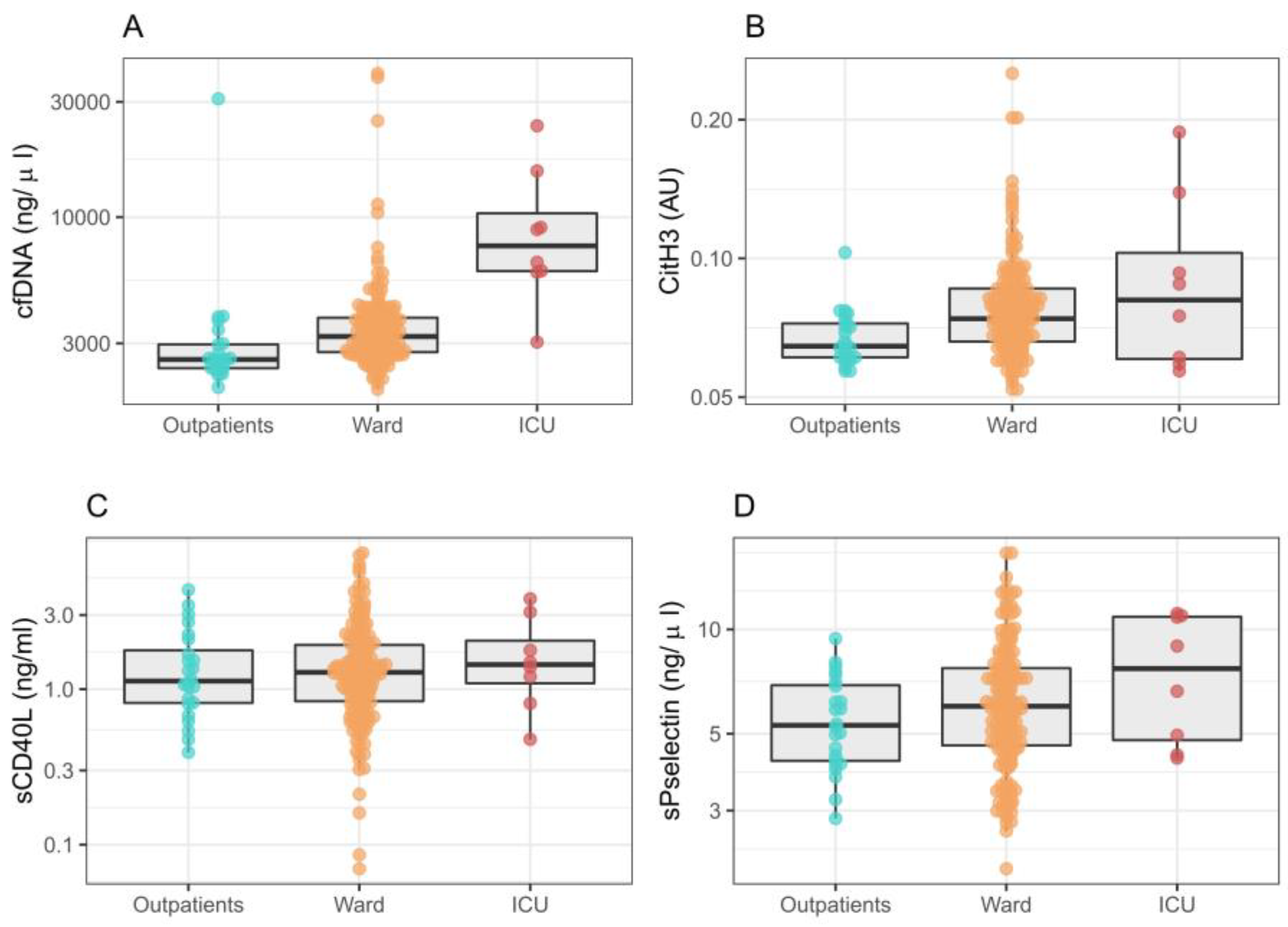
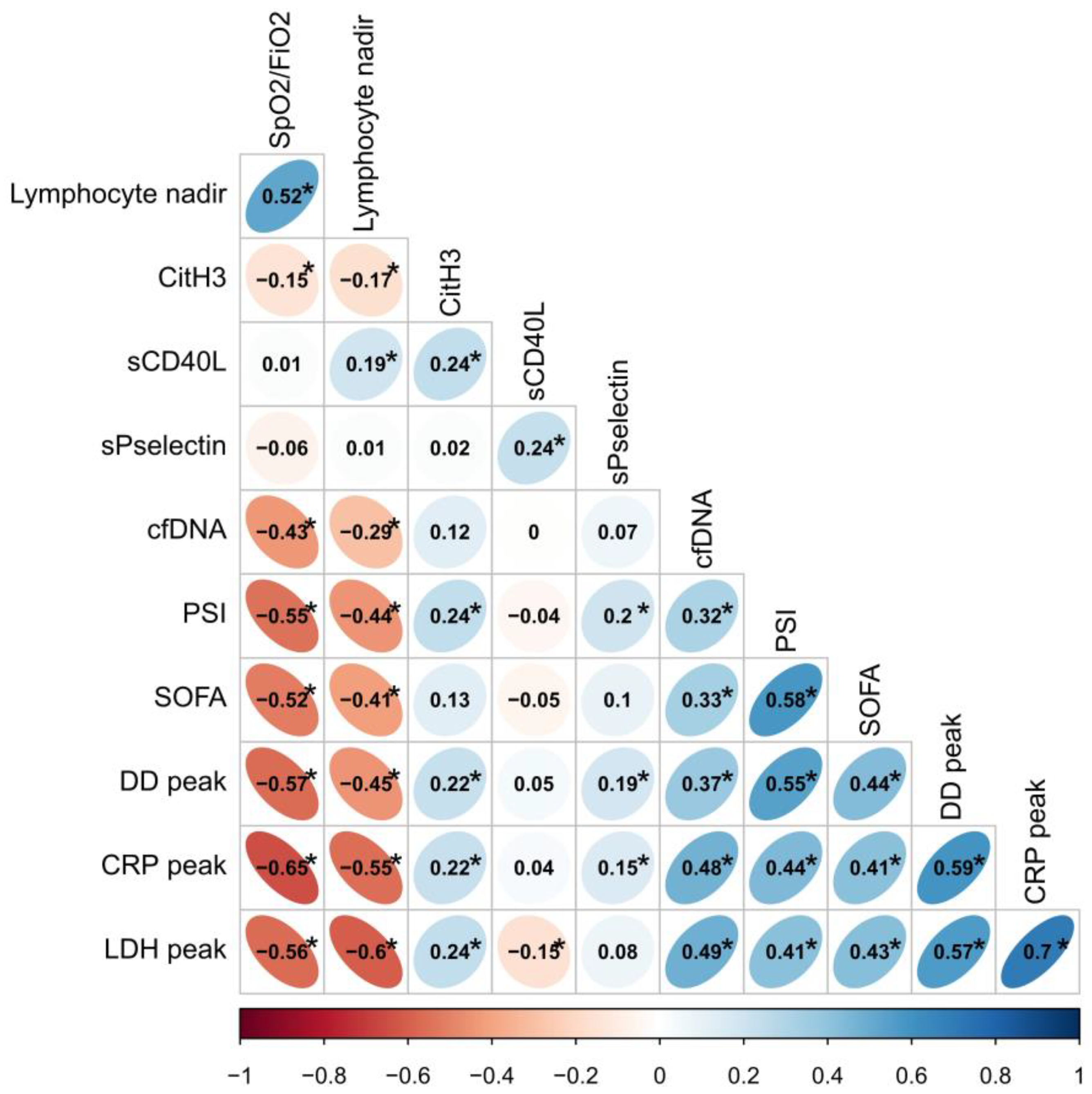
2.2. NETs, Platelet Activation and Initial Severity
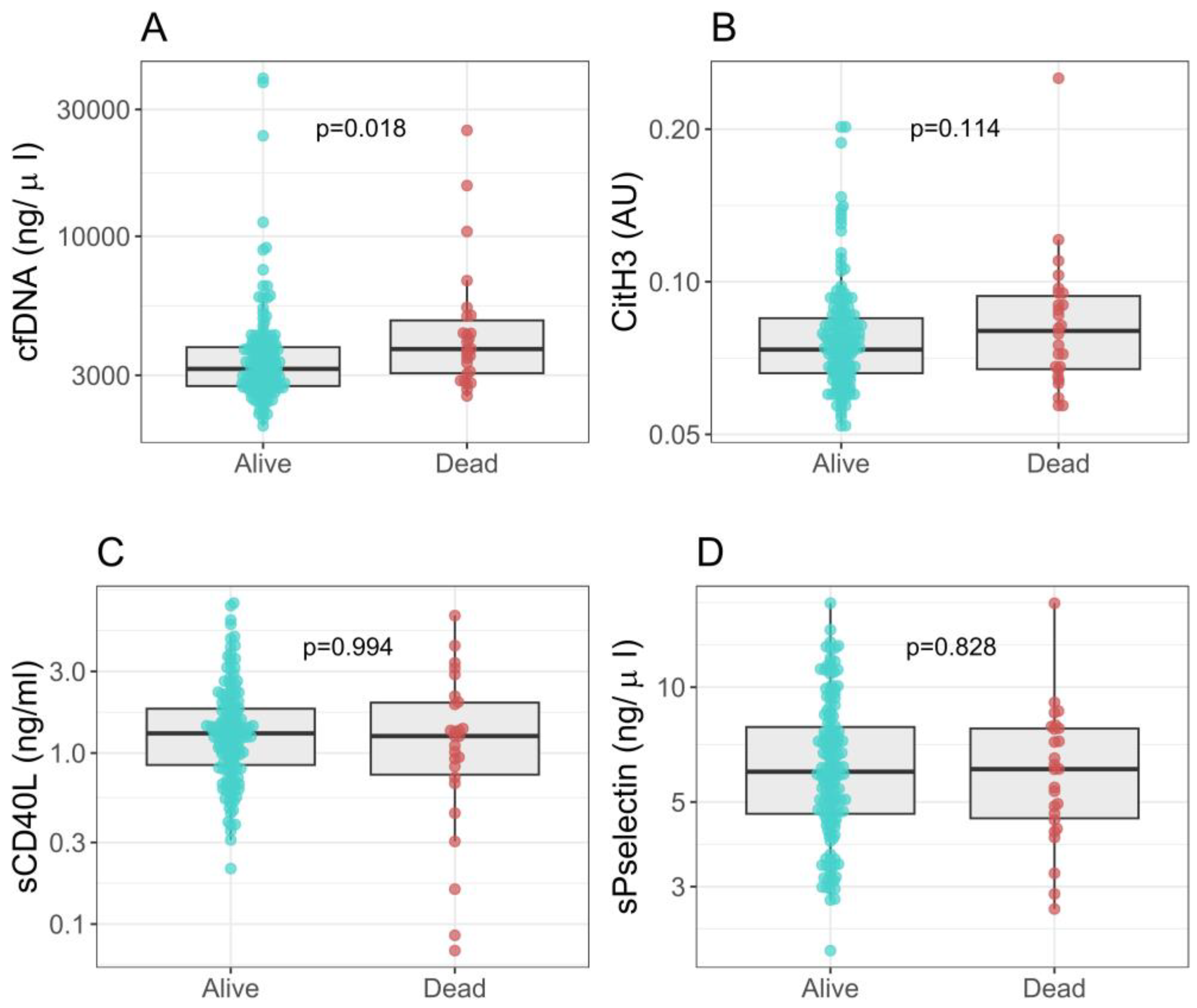
2.3. NETs, Platelet Activation Markers and Clinical Outcomes
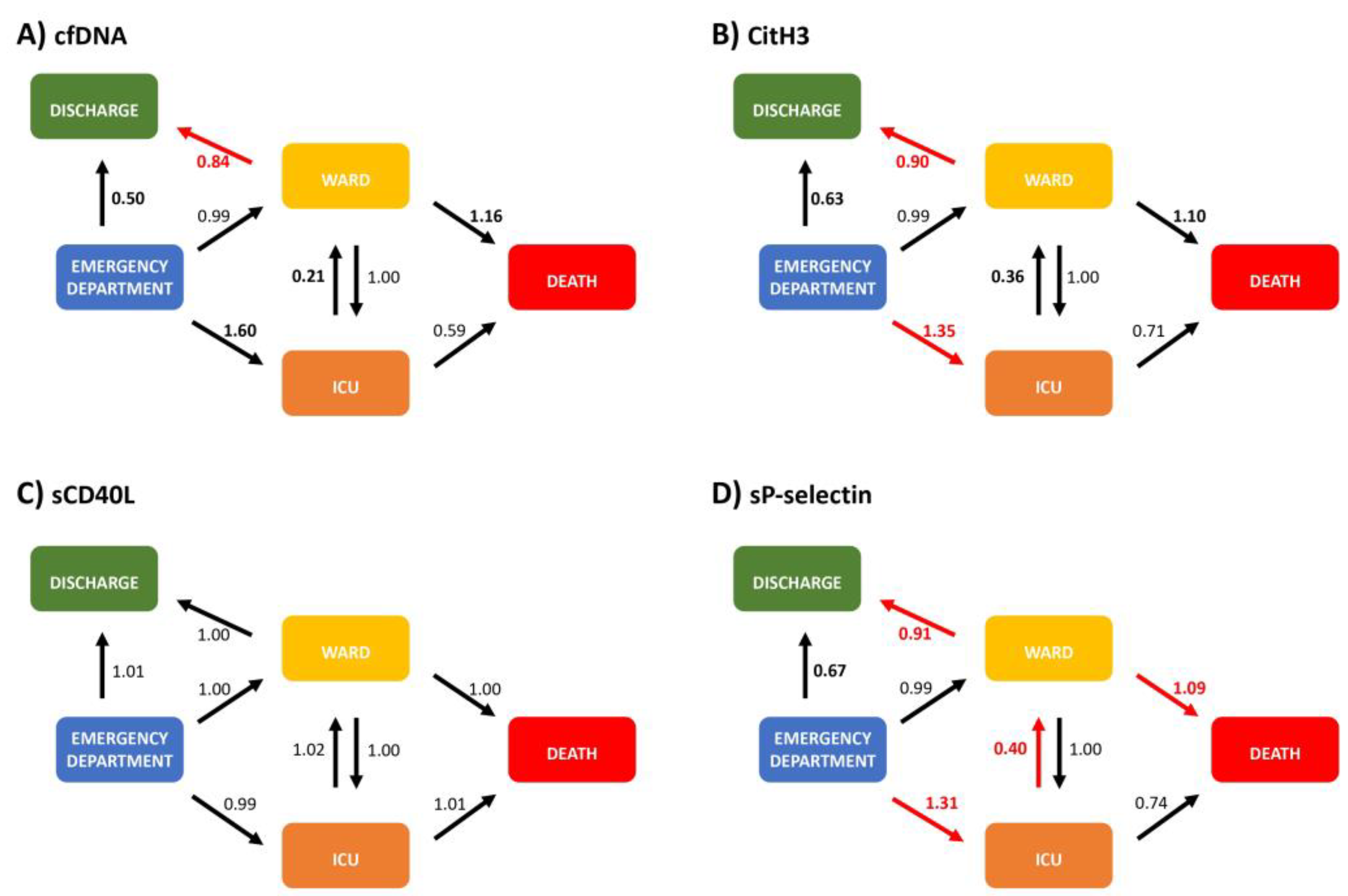
2.4. NETs and Platelet Activation Markers—A Multistate Model for Allocation and Progression
3. Discussion
Potential Limitations
4. Materials and Methods
4.1. Design, Participants and Outcomes
4.2. Blood Samples
4.3. Neutrophil Extracellular Traps
4.4. Platelet Activation
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Martin, J.F.; González-Rivera, M.; Almansa, R.; Micheloud, D.; Tedim, A.P.; Domínguez-Gil, M.; Resino, S.; Martín-Fernández, M.; Murua, P.R.; Pérez-García, F.; et al. Viral RNA load in plasma is associated with critical illness and a dysregulated host response in COVID-19. Crit. Care 2020, 24, 691. [Google Scholar] [CrossRef] [PubMed]
- Brinkmann, V.; Reichard, U.; Goosmann, C.; Fauler, B.; Uhlemann, Y.; Weiss, D.S.; Weinrauch, Y.; Zychlinsky, A. Neutrophil Extracellular Traps Kill Bacteria. Science 2004, 303, 1532–1535. [Google Scholar] [CrossRef] [PubMed]
- Jenne, C.N.; Wong, C.H.; Zemp, F.J.; McDonald, B.; Rahman, M.M.; Forsyth, P.A.; McFadden, G.; Kubes, P. Neutrophils Recruited to Sites of Infection Protect from Virus Challenge by Releasing Neutrophil Extracellular Traps. Cell Host Microbe 2013, 13, 169–180. [Google Scholar] [CrossRef] [Green Version]
- McDonald, B.; Urrutia, R.; Yipp, B.G.; Jenne, C.N.; Kubes, P. Intravascular Neutrophil Extracellular Traps Capture Bacteria from the Bloodstream during Sepsis. Cell Host Microbe 2012, 12, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, S.R.; Ma, A.C.; Tavener, S.A.; McDonald, B.; Goodarzi, Z.; Kelly, M.M.; Patel, K.D.; Chakrabarti, S.; McAvoy, E.; Sinclair, G.D.; et al. Platelet TLR4 activates neutrophil extracellular traps to ensnare bacteria in septic blood. Nat. Med. 2007, 13, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guan, L.; Yu, J.; Zhao, Z.; Mao, L.; Li, S.; Zhao, J. Pulmonary endothelial activation caused by extracellular histones contributes to neutrophil activation in acute respiratory distress syndrome. Respir. Res. 2016, 17, 155. [Google Scholar] [CrossRef] [Green Version]
- Gould, T.J.; Vu, T.; Swystun, L.; Dwivedi, D.; Weitz, J.; Liaw, P. Neutrophil extracellular traps promote thrombin generation through platelet-dependent and platelet-independent mechanisms. Arter. Thromb. Vasc. Biol. 2014, 34, 1977–1984. [Google Scholar] [CrossRef] [Green Version]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.N.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil extracellular traps in COVID-19. JCI Insight 2020, 5, e138999. [Google Scholar] [CrossRef] [Green Version]
- Garnier, Y.; Claude, L.; Hermand, P.; Sachou, E.; Claes, A.; Desplan, K.; Chahim, B.; Roger, P.-M.; Martino, F.; Colin, Y.; et al. Plasma microparticles of intubated COVID-19 patients cause endothelial cell death, neutrophil adhesion and netosis, in a phosphatidylserine-dependent manner. Br. J. Haematol. 2022, 196, 1159–1169. [Google Scholar] [CrossRef]
- Koupenova, M.; Clancy, L.; Corkrey, H.A.; Freedman, J.E. Circulating Platelets as Mediators of Immunity, Inflammation, and Thrombosis. Circ. Res. 2018, 122, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Kapur, R.; Zufferey, A.; Boilard, E.; Semple, J.W. Nouvelle Cuisine: Platelets Served with Inflammation. J. Immunol. 2015, 194, 5579–5587. [Google Scholar] [CrossRef] [Green Version]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in COVID-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Hottz, E.D.; Azevedo-Quintanilha, I.G.; Palhinha, L.; Teixeira, L.; Barreto, E.A.; Pão, C.R.R.; Righy, C.; Franco, S.; Souza, T.M.L.; Kurtz, P.; et al. Platelet activation and platelet-monocyte aggregates formation trigger tissue factor expression in severe COVID-19 patients. Blood 2020, 136, 1330–1341. [Google Scholar] [CrossRef]
- Fernández-Pérez, M.P.; Águila, S.; Reguilón-Gallego, L.; Reyes-García, A.M.L.; Miñano, A.; Bravo-Pérez, C.; Morena, M.E.; Corral, J.; García-Barberá, N.; Gómez-Verdú, J.M.; et al. Neutrophil extracellular traps and von Willebrand factor are allies that negatively influence COVID-19 outcomes. Clin. Transl. Med. 2021, 11, e268. [Google Scholar] [CrossRef] [PubMed]
- Huckriede, J.; Anderberg, S.B.; Morales, A.; de Vries, F.; Hultström, M.; Bergqvist, A.; Ortiz-Pérez, J.T.; Sels, J.W.; Wichapong, K.; Lipcsey, M.; et al. Evolution of NETosis markers and DAMPs have prognostic value in critically ill COVID-19 patients. Sci. Rep. 2021, 11, 15701. [Google Scholar] [CrossRef] [PubMed]
- Ng, H.; Havervall, S.; Rosell, A.; Aguilera, K.; Parv, K.; Von Meijenfeldt, F.A.; Lisman, T.; Mackman, N.; Thålin, C.; Phillipson, M. Circulating Markers of Neutrophil Extracellular Traps Are of Prognostic Value in Patients with COVID-19. Arter. Thromb. Vasc. Biol. 2021, 41, 988–994. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Chen, X.; Liu, X. NETosis and Neutrophil Extracellular Traps in COVID-19: Immunothrombosis and Beyond. Front. Immunol. 2022, 13, 838011. [Google Scholar] [CrossRef] [PubMed]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of COVID-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Obermayer, A.; Jakob, L.M.; Haslbauer, J.D.; Matter, M.S.; Tzankov, A.; Stoiber, W. Neutrophil Extracellular Traps in Fatal COVID-19-Associated Lung Injury. Dis. Markers 2021, 30, 5566826. [Google Scholar] [CrossRef]
- A Masso-Silva, J.; Moshensky, A.; Lam, M.T.Y.; Odish, M.F.; Patel, A.; Xu, L.; Hansen, E.; Trescott, S.; Nguyen, C.; Kim, R.; et al. Increased Peripheral Blood Neutrophil Activation Phenotypes and Neutrophil Extracellular Trap Formation in Critically Ill Coronavirus Disease 2019 (COVID-19) Patients: A Case Series and Review of the Literature. Clin. Infect. Dis. 2022, 74, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Melero, I.; Villalba-Esparza, M.; Recalde-Zamacona, B.; Jiménez-Sánchez, D.; Teijeira, E.; Argueta, A.; García-Tobar, L.; Álvarez-Gigli, L.; Sainz, C.; Garcia-Ros, D.; et al. Neutrophil Extracellular Traps, Local IL-8 Expression, and Cytotoxic T-Lymphocyte Response in the Lungs of Patients With Fatal COVID-19. Chest 2022, 162, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Petito, E.; Falcinelli, E.; Paliani, U.; Cesari, E.; Vaudo, G.; Sebastiano, M.; Cerotto, V.; Guglielmini, G.; Gori, F.; Malvestiti, M.; et al. Association of Neutrophil Activation, More Than Platelet Activation, with Thrombotic Complications in Coronavirus Disease 2019. J. Infect. Dis. 2021, 223, 933–944. [Google Scholar] [CrossRef]
- Ebrahimi, F.; Giaglis, S.; Hahn, S.; Blum, C.A.; Baumgartner, C.; Kutz, A.; Van Breda, S.V.; Mueller, B.; Schuetz, P.; Christ-Crain, M.; et al. Markers of neutrophil extracellular traps predict adverse outcome in community-acquired pneumonia: Secondary analysis of a randomised controlled trial. Eur. Respir. J. 2018, 51, 1701389. [Google Scholar] [CrossRef] [PubMed]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandia, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [Google Scholar] [CrossRef]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [Google Scholar] [CrossRef]
- Cataudella, E.; Giraffa, C.M.; Di Marca, S.; Pulvirenti, A.; Alaimo, S.; Pisano, M.; Terranova, V.; Corriere, T.; Ronsisvalle, M.L.; Di Quattro, R.; et al. Neutrophil-To-Lymphocyte Ratio: An Emerging Marker Predicting Prognosis in Elderly Adults with Community-Acquired Pneumonia. J. Am. Geriatr. Soc. 2017, 65, 1796–1801. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Ni Choileain, O.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the Inflammatory Response to Severe COVID-19 Illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef]
- Patel, B.V.; Arachchillage, D.J.; Ridge, C.A.; Bianchi, P.; Doyle, J.F.; Garfield, B.; Ledot, S.; Morgan, C.; Passariello, M.; Price, S.; et al. Pulmonary Angiopathy in Severe COVID-19: Physiologic, Imaging and Hematologic Observations. Am. J. Respir. Crit. Care Med. 2020, 202, 690–699. [Google Scholar] [CrossRef]
- Zuo, Y.; Zuo, M.; Yalavarthi, S.; Gockman, K.; Madison, J.A.; Shi, H.; Woodard, W.; Lezak, S.P.; Lugogo, N.L.; Knight, J.S.; et al. Neutrophil extracellular traps and thrombosis in COVID-19. J. Thromb. Thrombolysis 2021, 51, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Lucas, C.; Wong, P.; Klein, J.; Castro, T.B.R.; Silva, J.; Sundaram, M.; Ellingson, M.K.; Mao, T.; Oh, J.E.; Israelow, B.; et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature 2020, 584, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Menéndez, R.; Méndez, R.; González-Jiménez, P.; Zalacain, R.; Ruiz, L.A.; Serrano, L.; España, P.P.; Uranga, A.; Cillóniz, C.; Pérez-de-Llano, L.; et al. Early recognition of low-risk SARS-CoV-2 pneumonia: A model validated with initial data and IDSA/ATS minor criteria. Chest 2022, 162, 768–781. [Google Scholar] [CrossRef]
- Grover, S.P.; Mackman, N. Neutrophils, NETs, and immunothrombosis. Blood 2018, 136, 1169–1179. [Google Scholar] [CrossRef]
- Wagner, D.D.; Heger, L.A. Thromboinflammation: From Atherosclerosis to COVID-19. Arter. Thromb. Vasc. Biol. 2022, 42, 1103–1112. [Google Scholar] [CrossRef]
- Middleton, E.A.; He, X.-Y.; Denorme, F.; Campbell, R.A.; Ng, D.; Salvatore, S.P.; Mostyka, M.; Baxter-Stoltzfus, A.; Borczuk, A.C.; Loda, M.; et al. Neutrophil Extracellular Traps (NETs) Contribute to Immunothrombosis in COVID-19 Acute Respiratory Distress Syndrome. Blood 2020, 136, 1169–1179. [Google Scholar] [CrossRef]
- Vulesevic, B.; Lavoie, S.S.; Neagoe, P.-E.; Dumas, E.; Räkel, A.; White, M.; Sirois, M.G. CRP Induces NETosis in Heart Failure Patients with or without Diabetes. Immunohorizons 2019, 3, 378–388. [Google Scholar] [CrossRef] [Green Version]
- Keshari, R.S.; Jyoti, A.; Dubey, M.; Kothari, N.; Kohli, M.; Bogra, J.; Barthwal, M.K.; Dikshit, M. Cytokines Induced Neutrophil Extracellular Traps Formation: Implication for the Inflammatory Disease Condition. PLoS ONE 2012, 7, e48111. [Google Scholar] [CrossRef] [Green Version]
- Pulavendran, S.; Rudd, J.M.; Maram, P.; Thomas, P.G.; Akhilesh, R.; Malayer, J.R.; Chow, V.T.K.; Teluguakula, N. Combination therapy targeting platelet activation and virus replication protects mice against lethal influenza pneumonia. Am. J. Respir. Cell Mol. Biol. 2019, 61, 689–701. [Google Scholar] [CrossRef] [PubMed]
- Jamasbi, J.; Ayabe, K.; Goto, S.; Nieswandt, B.; Peter, K.; Siess, W. Platelet receptors as therapeutic targets: Past, present and future. Thromb. Haemost. 2017, 117, 1249–1257. [Google Scholar] [CrossRef] [Green Version]
- Hassan, G.S.; Merhi, Y.; Mourad, W. CD40 Ligand: A neo-inflammatory molecule in vascular diseases. Immunobiology 2012, 217, 521–532. [Google Scholar] [CrossRef]
- Vats, R.; Kaminski, T.W.; Brzoska, T.; Leech, J.A.; Tutuncuoglu, E.; Katoch, O.; Jonassaint, J.C.; Tejero, J.; Novelli, E.M.; Pradhan-Sundd, T.; et al. Liver-to-lung microembolic NETs promote gasdermin D–dependent inflammatory lung injury in sickle cell disease. Blood 2022, 140, 1020–1037. [Google Scholar] [CrossRef] [PubMed]
- Vallés, J.; Lago, A.; Santos, M.T.; Latorre, A.M.; Tembl, J.I.; Salom, J.B.; Nieves, C.; Moscardó, A. Neutrophil Extracellular Traps Are Increased in Patients With Acute Ischemic Stroke: Prognostic Significance. Thromb. Haemost. 2017, 117, 1919–1929. [Google Scholar] [CrossRef]
- Wong, S.L.; Demers, M.; Martinod, K.; Gallant, M.; Wang, Y.; Goldfine, A.B.; Kahn, C.R.; Wagner, D.D. Diabetes primes neutrophils to undergo NETosis which severely impairs wound healing. Nat. Med. 2015, 21, 815. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steven, S.; Dib, M.; Hausding, M.; Kashani, F.; Oelze, M.; Kröller-Schön, S.; Hanf, A.; Daub, S.; Roohani, S.; Gramlich, Y.; et al. CD40L controls obesity-associated vascular inflammation, oxidative stress, and endothelial dysfunction in high fat diet-treated and db/db mice. Cardiovasc. Res. 2018, 114, 312–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Méndez, R.; Moscardó, A.; Latorre, A.; Feced, L.; González-Jiménez, P.; Piró, A.; Alcaraz-Serrano, V.; Scioscia, G.; Amaro, R.; Torres, A.; et al. Soluble P-selectin in Acute Exacerbations and Stable Bronchiectasis in Adults. Ann. Am. Thorac. Soc. 2019, 16, 1587–1591. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 204) | Outpatients (n = 24) | Ward (n = 172) | ICU (First 24 h) (n = 8) |
|---|---|---|---|---|
| Age, years, median (1st quartile, 3rd quartile) | 64 (51, 77) | 49 (39, 58) | 66 (53, 79) | 63 (54, 66) |
| Distribution, no. (%) | ||||
| <50 years | 5 (22.1) | 12 (50) | 32 (18.6) | 1 (12.5) |
| 50 to <70 years | 86 (42.2) | 10 (41.7) | 69 (40.1) | 7 (87.5) |
| ≥70 years | 73 (35.8) | 2 (8.3) | 71 (41.3) | 0 (0) |
| Male sex, no. (%) | 109 (53.4) | 4 (16.7) | 98 (57) | 7 (87.5) |
| Co-existing conditions, no. (%) | ||||
| Any | 136 (66.7) | 15 (62.5) | 116 (67.4) | 5 (62.5) |
| Hypertension | 86 (42.2) | 7 (29.2) | 74 (43) | 5 (62.5) |
| Diabetes | 46 (22.5) | 1 (4.2) | 42 (24.4) | 3 (37.5) |
| Dyslipidemia | 62 (30.4) | 4 (16.7) | 55 (32) | 3 (37.5) |
| Chronic heart disease | 25 (12.3) | 2 (8.3) | 23 (13.4) | 0 (0) |
| Chronic renal disease * | 27 (13.2) | 0 (0) | 27 (15.7) | 0 (0) |
| Chronic liver disease | 6 (2.9) | 0 (0) | 6 (3.5) | 0 (0) |
| Neurological disease | 25 (12.3) | 1 (4.2) | 24 (14) | 0 (0) |
| Chronic respiratory disease | 23 (11.3) | 5 (20.8) | 18 (10.5) | 0 (0) |
| No. of days since symptom onset, median (1st quartile, 3rd quartile) † | 7 (5, 10) | 10 (5, 15) | 7 (5, 10) | 5 (3, 6) |
| SpO2/FiO2 at admission (1st quartile, 3rd quartile) | 452.4 (438.1, 461.9) | 466.7 (461.9, 471.4) | 452.4 (438.1, 457.1) | 264.3 (168, 326) |
| Radiological data at admission | ||||
| Bilateral infiltrates, no. (%) | 112 (63.6) | 0 (0) | 104 (65) | 8 (100) |
| Severity | ||||
|
PSI score, median (1st quartile, 3rd quartile) | 68 (48, 91) | 42 (32, 53) | 71 (51, 95) | 89 (75, 101) |
| I-III, no. (%) | 151 (74.4) | 24 (100) | 123 (71.9) | 4 (50) |
| IV-V, no. (%) | 52 (25.6) | 0 (0) | 48 (28.1) | 4 (50) |
|
SOFA score, median (1st quartile, 3rd quartile) | 1 (0, 2) | 0 (0, 0) | 1 (0, 2) | 2 (1, 4) |
| Analytical parameters | ||||
|
Peak LDH, UI/L, median (1st quartile, 3rd quartile) | 295.5 (238, 420) | 170 (156, 225.5) | 310 (249, 423) | 494 (427.5, 674.5) |
|
Peak C-reactive protein, mg/L, median (1st quartile, 3rd quartile) | 87.2 (31.3, 200.9) | 5.7 (1.4, 12.2) | 104.7 (41.6, 205.1) | 372.2 (302.9, 530.3) |
|
Lymphocyte count nadir, cells/mL, median (1st quartile, 3rd quartile) | 910 (640, 1305) | 1500 (1075, 2175) | 860 (640, 1245) | 480 (425, 610) |
|
Peak D-dimer, ng/mL, median (1st quartile, 3rd quartile) ** | 958.5 (477, 2143) | 353 (215, 567) | 1014 (527, 2143) | 25,677 (11,486, 43,961) |
| Respiratory support, no. (%) | ||||
| O2 nasal cannula, no. (%) | 19 (8.1) | 0 (0) | 19 (11) | 0 (0) |
|
O2 Venturi or reservoir mask, no. (%) | 55 (23.5) | 0 (0) | 55 (32) | 0 (0) |
| HFNC/CPAP, no. (%) | 10 (4.3) | 0 (0) | 10 (5.8) | 0 (0) |
| MV, no. (%) | 15 (6.4) | 0 (0) | 7 (4.1) | 8 (100) |
|
Median length of MV, days, median (1st quartile, 3rd quartile) | NA | NA | 12 (11, 14) | 13.5 (11, 16.5) |
| Outcomes and complications | ||||
|
Median length of hospital stay, days, median (1st quartile, 3rd quartile) | 12 (9, 20.5) | NA | 12 (9, 19) | 32.5 (18, 45) |
|
Transfer to ICU from ward, no. (%) †† | 17 (8.3) | NA | 17 (9.9) | NA |
| In-hospital mortality, no. (%) | 26 (12.7) | 0 (0) | 24 (14) | 2 (25) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-Jiménez, P.; Méndez, R.; Latorre, A.; Piqueras, M.; Balaguer-Cartagena, M.N.; Moscardó, A.; Alonso, R.; Hervás, D.; Reyes, S.; Menéndez, R. Neutrophil Extracellular Traps and Platelet Activation for Identifying Severe Episodes and Clinical Trajectories in COVID-19. Int. J. Mol. Sci. 2023, 24, 6690. https://doi.org/10.3390/ijms24076690
González-Jiménez P, Méndez R, Latorre A, Piqueras M, Balaguer-Cartagena MN, Moscardó A, Alonso R, Hervás D, Reyes S, Menéndez R. Neutrophil Extracellular Traps and Platelet Activation for Identifying Severe Episodes and Clinical Trajectories in COVID-19. International Journal of Molecular Sciences. 2023; 24(7):6690. https://doi.org/10.3390/ijms24076690
Chicago/Turabian StyleGonzález-Jiménez, Paula, Raúl Méndez, Ana Latorre, Mónica Piqueras, María Nieves Balaguer-Cartagena, Antonio Moscardó, Ricardo Alonso, David Hervás, Soledad Reyes, and Rosario Menéndez. 2023. "Neutrophil Extracellular Traps and Platelet Activation for Identifying Severe Episodes and Clinical Trajectories in COVID-19" International Journal of Molecular Sciences 24, no. 7: 6690. https://doi.org/10.3390/ijms24076690