
Incidence of Bloodstream Infection in Patients with Pulmonary Hypertension under Intravenous Epoprostenol or Iloprost—A Multicentre, Retrospective Study
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics
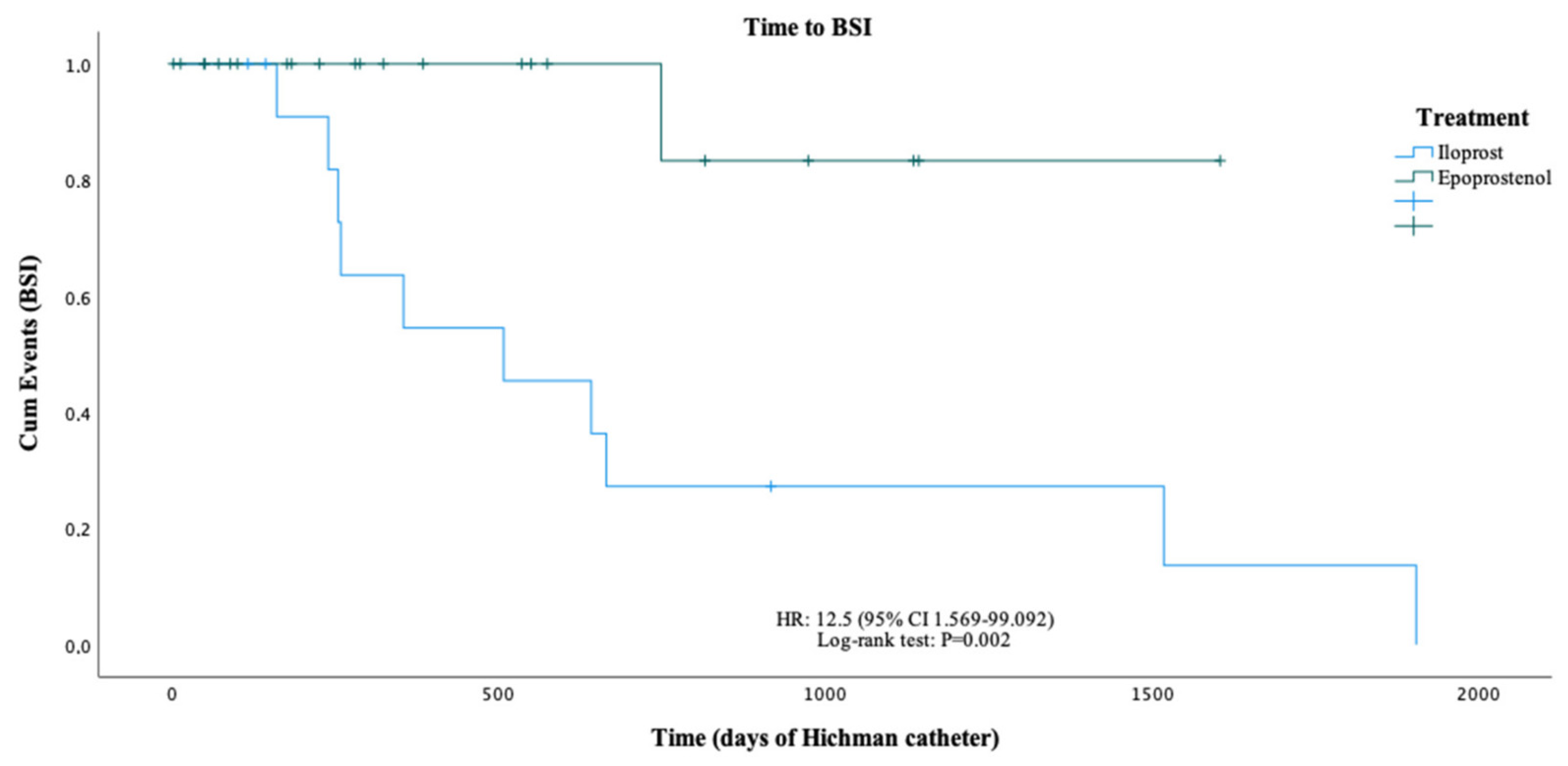
2.2. Treatment Periods and BSI Incidence
2.3. Microbiologic Features in BSI Patients
3. Discussion

{kind=link}
| Study | Duration | Total BSI (n) | BSI Global Rate * | Gram-Negative (%) |
|---|---|---|---|---|
| Iloprost | ||||
| Knudsen et al., 2011 [12] | 2002–2009 | 9 | 0.41 | N/A |
| Keusch et al., 2013 [13] | 2000–2012 | 11 | 1.28 | 27 |
| Sammut et al., 2013 [10] | 2007–2012 | 15 | 0.65 | 60 |
| Camara & Coelho et al. º | 2004–2019 | 26 | 3.38 | 67.9 |
| Epoprostenol | ||||
| Rublin et al., 1990 [15] | 8 weeks | N/A | 0 | N/A |
| Barst et al., 1996 [5] | 12 weeks | N/A | 1.16 | N/A |
| McLaughlin et al., 1998 [16] | 1994–1995 | N/A | 0.22 | N/A |
| Badesch et al., 2000 [17] | 12 weeks | N/A | 0.43 | N/A |
| Sitbon et al., 2002 [18] | 1992–2001 | N/A | 0.55 | N/A |
| McLaughlin et al., 2002 [19] | 1991–2001 | N/A | 0.45 | N/A |
| Oudiz et al., 2004 [20] | 1987–2000 | 88 | 0.26 | 4 |
| Barst et al., 2007 [21] | 2003–2006 | N/A | 0.43 | N/A |
| Akagi et al., 2007 [22] | 1999–2005 | 21 6 | 0.89 0.1 | 0 0 |
| Kallen et al., 2008 [23] | 2004–2006 | 49 | 0.42 | 15 |
| Hiremath et al., 2010 [24] | 12 weeks | N/A | 2.16 | N/A |
| Kitterman et al., 2012 [9] | 2006–2009 | 66 | 0.12 | 28.3 |
| Rich et al., 2012 [25] | 2009–2010 | 12 | 0.4 | 50 |
| López-Medrano et al., 2012 [26] | 1991–2012 | 7 | 0.12 | 0 |
| Nagai et al., 2012 [27] | 1998–2008 | N/A | 0.18 | N/A |
| Chin et al., 2014 [28] | 8 weeks | N/A | 0.57 | N/A |
| Sitbon et al., 2014 [29] | 12 weeks | N/A | 0.81 | N/A |
| Frantz et al., 2015 [30] | 2010–2012 | N/A | 0.2 | N/A |
| Courtney et al., 2015 [31] | 1999–2014 | N/A | 0.21 | N/A |
| McCarthy et al., 2018 [32] | 2000–2014 | 15 | 0.73 | 13.3 |
| Camara & Coelho et al. º | 2004–2019 | 1 | 0.09 | 0 |
- (1)
- There are only four specialized PH centers in Portugal, and the geographical distribution of patients impairs their ability to attend the hospital every 72 h to recharge their pumps. Additionally, primary care units are not prepared to manage these patients and devices properly. Thus, to ensure that the best medical care is provided to all patients without sacrificing their autonomy, the hospitals provide medication and the necessary material for self-preparation and administration of iPCAs, as well as regular training towards the asepsis maintenance in long-term catheters, management of home therapy, recognition of potential problems with the pump or other parts of the system and when to call hospital lines upon recognition of symptoms. The real impact of these measures on the prevalence of BSI is not fully elucidated, but it is reasonable to assume that intravenous therapy prepared by individuals who are not healthcare professionals may constitute an increased risk of contamination. Nevertheless, since this factor applies to patients from both therapy groups, this explanation itself seems to be insufficient to explain the discrepancy in BSI incidence rates found.
- (2)
- The learning curve for a period of >15 years in the two centers is another important factor that must be considered. Iloprost was the first iPCA available in Portugal in 2004, but only in 2014 did the thermostable epoprostenol become available for prescription in Portugal. Comprehensibly, patients received only iloprost for the first 10 years of iPCA national implementation and only when epoprostenol became available they could be offered that therapy. Moreover, it is relevant to consider that all patients in the epoprostenol group started their therapy and training with an expert team with 10 years of experience, thereby benefiting not only from the medical experience but also from the accumulated experience in patient education.
- (3)
- Since the introduction of iPCAs in Portugal, new measures have been implemented according to state-of-the-art techniques. Moreover, professionals have gained experience using strategies that can prevent the occurrence of infections, such as the use of a non-return-valve (closed hub) and waterproof connections [19,48]. Similarly, a teaching program and long-distant assistance via cell phone have been developed as an effort to better prepare and support patients to deal with unexpected events and to provide an immediate response to any doubts that might arise during their therapy management.
4. Materials and Methods
4.1. Study Design
4.2. Inclusion and Exclusion Criteria
4.3. Data Collection
4.4. Clinical Outcomes
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galiè, N.; Hoeper, M.; Humbert, M.; Torbicki, A.; Vachiery, J.-L.; Barbera, J.A.; Beghetti, M.; Corris, P.; Gaine, S.; Gibbs, S.; et al. Guidelines on diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology and of the European Respiratory Society. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Vanderpool, R.R.; Gorelova, A.; Ma, Y.; Alhamaydeh, M.; Baust, J.; Shiva, S.; Tofovic, S.P.; Hu, J.; Nouraie, S.M.; Gladwin, M.T.; et al. Reversal of Right Ventricular Hypertrophy and Dysfunction by Prostacyclin in a Rat Model of Severe Pulmonary Arterial Hypertension. Int. J. Mol. Sci. 2022, 23, 5426. [Google Scholar] [CrossRef]
- Ruaro, B.; Salton, F.; Baratella, E.; Confalonieri, P.; Geri, P.; Pozzan, R.; Torregiani, C.; Bulla, R.; Confalonieri, M.; Matucci-Cerinic, M.; et al. An Overview of Different Techniques for Improving the Treatment of Pulmonary Hypertension Secondary in Systemic Sclerosis Patients. Diagnostics 2022, 12, 616. [Google Scholar] [CrossRef] [PubMed]
- Simonneau, G.; Montani, D.; Celermajer, D.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; Williams, P.G.; Souza, R. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801913. [Google Scholar] [CrossRef] [PubMed]
- Barst, R.J.; Rubin, L.J.; Long, W.A.; McGoon, M.D.; Rich, S.; Badesch, D.B.; Groves, B.M.; Tapson, V.F.; Bourge, R.C.; Brundage, B.H.; et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N. Engl. J. Med. 1996, 334, 296–302. [Google Scholar] [CrossRef]
- Humbert, M.; Guignabert, C.; Bonnet, S.; Dorfmüller, P.; Klinger, J.R.; Nicolls, M.R.; Olschewski, A.J.; Pullamsetti, S.S.; Schermuly, R.T.; Stenmark, K.R.; et al. Pathology and pathobiology of pulmonary hypertension: State of the art and research perspectives. Eur. Respir. J. 2019, 53, 1801887. [Google Scholar] [CrossRef] [Green Version]
- LeVarge, B.L. Prostanoid therapies in the management of pulmonary arterial hypertension. Ther. Clin. Risk Manag. 2015, 11, 535–547. [Google Scholar] [CrossRef] [Green Version]
- Kingman, M.; Archer-Chicko, C.; Bartlett, M.; Beckmann, J.; Hohsfield, R.; Lombardi, S. Management of prostacyclin side effects in adult patients with pulmonary arterial hypertension. Pulm. Circ. 2017, 7, 598–608. [Google Scholar] [CrossRef] [Green Version]
- Kitterman, N.; Poms, A.; Miller, D.P.; Lombardi, S.; Farber, H.W.; Barst, R.J. Bloodstream infections in patients with pulmonary arterial hypertension treated with intravenous prostanoids: Insights from the REVEAL REGISTRY®. Mayo. Clin. Proc. 2012, 87, 825–834. [Google Scholar] [CrossRef] [Green Version]
- Sammut, D.; Elliot, C.A.; Kiely, D.G.; Armstrong, I.J.; Martin, L.; Wilkinson, J.; Sephton, P.; Jones, J.; Hamilton, N.; Hurdman, J.; et al. Central venous catheter-related blood stream infections in patients receiving intravenous iloprost for pulmonary hypertension. Eur. J. Clin. Microbiol. Infect. Dis. 2013, 32, 883–889. [Google Scholar] [CrossRef]
- Ivy, D.D.; Calderbank, M.; Wagner, B.; Dolan, S.; Nyquist, A.-C.; Wade, M.; Nickels, W.M.; Doran, A.K. Closed-Hub Systems with Protected Connections and the Reduction of Risk of Catheter-Related Bloodstream Infection in Pediatric Patients Receiving Intravenous Prostanoid Therapy for Pulmonary Hypertension. Infect. Control. Hosp. Epidemiol. 2009, 30, 823–829. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, L.; Schurawlew, A.; Nickel, N.; Tiede, H.; Ghofrani, A.H.; Wilkens, H.; Ewert, R.; Halank, M.; Klose, H.; Bäzner, C.; et al. Long-term effects of intravenous iloprost in patients with idiopathic pulmonary arterial hypertension deteriorating on non-parenteral therapy. BMC Pulm. Med. 2011, 11, 56. [Google Scholar] [CrossRef]
- Keusch, S.; Speich, R.; Treder, U.; Somaini, S.U. Central Venous Catheter Infections in Outpatients with Pulmonary Hypertension Treated with Continuous Iloprost. Respiration 2013, 86, 402–406. [Google Scholar] [CrossRef] [Green Version]
- Athénaïs, B. Infections liées aux cathéters veineux centraux tunnélisés chez les patients ayant une hypertension artérielle pulmonaire traitée par prostacycline intraveineuse. Pressed. Med. 2016, 45, 20–28. [Google Scholar]
- Rubin, L.J.; Mendoza, J.; Hood, M.; McGoon, M.; Barst, R.; Williams, W.B.; Diehl, J.H.; Crow, J.; Long, W. Treatment of primary pulmonary hypertension with continuous intravenous prostacyclin (epoprostenol). Results of a randomized trial. Ann. Intern. Med. 1990, 112, 485–491. [Google Scholar] [CrossRef]
- McLaughlin, V.V.; Genthner, D.E.; Panella, M.M.; Rich, S. Reduction in pulmonary vascular resistance with long-term epoprostenol (prostacyclin) therapy in primary pulmonary hypertension. N. Engl. J. Med. 1998, 338, 273–277. [Google Scholar] [CrossRef]
- Badesch, D.B.; Tapson, V.F.; McGoon, M.D.; Brundage, B.H.; Rubin, L.J.; Wigley, F.M.; Rich, S.; Barst, R.J.; Barrett, P.S.; Kral, K.M.; et al. Continuous intravenous epoprostenol for pulmonary hypertension due to the scleroderma spectrum of disease. A randomized, controlled trial. Ann. Intern. Med. 2000, 132, 425–434. [Google Scholar] [CrossRef]
- Sitbon, O.; Humbert, M.; Nunes, H.; Parent, F.; Garcia, G.; Hervé, P.; Rainisio, M.; Simonneau, G. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension. Prognostic factors and survival. J. Am. Coll. Cardiol. 2002, 40, 780–788. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, V.V. Survival in primary pulmonary hypertension: The impact of epoprostenol therapy. Circulation 2002, 106, 1477–1482. [Google Scholar] [CrossRef] [Green Version]
- Oudiz, R.J.; Widlitz, A.; Beckmann, X.J.; Camanga, D.; Alfie, J.; Brundage, B.H.; Barst, R.J. Micrococcus-associated central venous catheter infection in patients with pulmonary arterial hypertension. Chest 2004, 126, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention (CDC). Bloodstream infections among patients treated with intravenous epoprostenol or intravenous treprostinil for pulmonary arterial hyperhypertension—Seven sites, United States, 2003–2006. MMWR. Morb. Mortal. Wkly. Rep. 2007, 8, 170–172. [Google Scholar]
- Akagi, S.; Matsubara, H.; Ogawa, A.; Kawai, Y.; Hisamatsu, K.; Miyaji, K.; Munemasa, M.; Fujimoto, Y.; Kusano, K.F.; Ohe, T. Prevention of catheter-related infections using a closed hub system in patients with pulmonary arterial hypertension. Circ. J. 2007, 71, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallen, A.J.; Lederman, E.; Balaji, A.; Trevino, I.; Petersen, E.E.; Shoulson, R.; Saiman, L.; Horn, E.M.; Gomberg-Maitland, M.; Barst, R.J.; et al. Bloodstream infections in patients given treatment with intravenous prostanoids. Infect. Control Hosp. Epidemiol. 2008, 29, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Hiremath, J.; Thanikachalam, S.; Parikh, K.; Shanmugasundaram, S.; Bangera, S.; Shapiro, L.; Pott, G.B.; Vnencak-Jones, C.L.; Arneson, C.; Wade, M.; et al. Exercise improvement and plasma biomarker changes with intravenous treprostinil therapy for pulmonary arterial hypertension: A placebo-controlled trial. J. Heart Lung Transpl. 2010, 29, 137–149. [Google Scholar] [CrossRef]
- Rich, J.D.; Glassner, C.; Wade, M.; Coslet, S.; Arneson, C.; Doran, A.; Gomberg-Maitland, M. The effect of diluent ph on bloodstream infection rates in patients receiving intravenous treprostinil for pulmonary arterial hypertension. Chest 2012, 141, 36–42. [Google Scholar] [CrossRef]
- López-Medrano, F.; Fernández-Ruiz, M.; Ruiz-Cano, M.J.; Barrios, E.; Vicente-Hernández, M.; Aguado, J.M.; Escribano, P. High Incidence of Bloodstream Infection Due to Gram-negative Bacilli in Patients With Pulmonary Hypertension Receiving Intravenous Treprostinil. Arch. Bronconeumol. 2012, 48, 443–447. [Google Scholar] [CrossRef]
- Nagai, T. Low incidence of catheter-related complications in patients with advanced pulmonary arterial hypertension undergoing continuous epoprostenol infusion. Chest J. 2012, 141, 272. [Google Scholar] [CrossRef] [Green Version]
- Chin, K.M.; Badesch, D.B.; Robbins, I.M.; Tapson, V.F.; Palevsky, H.I.; Kim, N.H.; Kawut, S.M.; Frost, A.; Benton, W.W.; Lemarie, J.-C.; et al. Two formulations of epoprostenol sodium in the treatment of pulmonary arterial hypertension: EPITOME-1 (epoprostenol for injection in pulmonary arterial hypertension), a phase IV, open-label, randomized study. Am. Heart J. 2014, 167, 218–225. [Google Scholar] [CrossRef]
- Sitbon, O.; Delcroix, M.; Bergot, E.; Boonstra, A.B.; Granton, J.; Langleben, D.; Subías, P.E.; Galiè, N.; Pfister, T.; Lemarié, J.-C.; et al. EPITOME-2: An open-label study assessing the transition to a new formulation of intravenous epoprostenol in patients with pulmonary arterial hypertension. Am. Heart J. 2014, 167, 210–217. [Google Scholar] [CrossRef]
- Frantz, R.P.; Schilz, R.J.; Chakinala, M.M.; Badesch, D.B.; Frost, A.E.; McLaughlin, V.V.; Barst, R.J.; Rosenberg, D.M.; Miller, D.P.; Hartline, B.K.; et al. Hospitalization and survival in patients using epoprostenol for injection in the PROSPECT observational study. Chest 2015, 147, 484–494. [Google Scholar] [CrossRef] [Green Version]
- Marr, C.R.; McSweeney, J.E.; Mullen, M.P.; Kulik, T.J. Central venous line complications with chronic ambulatory infusion of prostacyclin analogues in pediatric patients with pulmonary arterial hypertension. Pulm. Circ. 2015, 5, 322–326. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, E.K. Central line replacement following infection does not improve reinfection rates in pediatric pulmonary hypertension patients receiving intravenous prostanoid therapy. Pulm. Circ. 2018, 8, 2045893218754886. [Google Scholar] [CrossRef] [Green Version]
- Zmantar, T.; Kouidhi, B.; Miladi, H.; Mahdouani, K.; Bakhrouf, A. A Microtiter plate assay for Staphylococcus aureus biofilm quantification at various pH levels and hydrogen peroxide supplementation. New Microbiol. 2010, 33, 137–145. [Google Scholar]
- Nostro, A.; Cellini, L.; Di Giulio, M.; D’Arrigo, M.; Marino, A.; Blanco, A.R.; Favaloro, A.; Cutroneo, G.; Bisignano, G. Effect of alkaline pH on staphylococcal biofilm formation. APMIS 2012, 120, 733–742. [Google Scholar] [CrossRef]
- Zaccardelli, D.; Phares, K.; Jeffs, R.; Doran, A.; Wade, M. Stability and antimicrobial effectiveness of treprostinil sodium in Sterile Diluent for Flolan. Int. J. Clin. Pract. 2010, 64, 885–891. [Google Scholar] [CrossRef]
- Ku, S.-C.; Hsueh, P.-R.; Yang, P.C.; Luh, K.T. Clinical and Microbiological Characteristics of Bacteremia Caused by Acinetobacter. lwoffii. Eur. J. Clin. Microbiol. Infect. Dis. 2000, 19, 501–505. [Google Scholar] [CrossRef]
- Antony, B.; Cherian, E.V.; Boloor, R.; Shenoy, K.V. A sporadic outbreak of Burkholderia cepacia complex bacteremia in pediatric intensive care unit of a tertiary care hospital in coastal Karnataka, South India. Indian J. Pathol. Microbiol. 2016, 59, 197–199. [Google Scholar] [CrossRef]
- Romero-Gómez, M.P.; Quiles-Melero, M.I.; Peña García, P.; Gutiérrez Altes, A.; García de Miguel, M.A.; Jiménez, C.; Valdezate, S.; Sáez Nieto, J.A. Outbreak of Burkholderia cepacia bacteremia caused by contaminated chlorhexidine in a hemodialysis unit. Infect. Control Hosp. Epidemiol. 2008, 29, 377–378. [Google Scholar] [CrossRef] [Green Version]
- Singhal, T.; Shah, S.; Naik, R. Outbreak of Burkholderia cepacia complex bacteremia in a chemotherapy day care unit due to intrinsic contamination of an antiemetic drug. Indian J. Med. Microbiol. 2015, 33, 117–119. [Google Scholar] [CrossRef]
- Liao, C.H.; Chang, H.T.; Lai, C.C.; Huang, Y.T.; Hsu, M.S.; Liu, C.Y.; Yang, C.J.; Hsueh, P.R. Clinical characteristics and outcomes of patients with Burkholderia cepacia bacteremia in an intensive care unit. Diagn. Microbiol. Infect. Dis. 2011, 70, 260–266. [Google Scholar] [CrossRef]
- Ryan, M.P.; Pembroke, J.T.; Adley, C.C. Ralstonia pickettii: A persistent gram-negative nosocomial infectious organism. J. Hosp. Infect. 2006, 62, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Chotikanatis, K.; Bäcker, M.; Rosas-Garcia, G.; Hammerschlag, M.R. Recurrent Intravascular-Catheter-Related Bacteremia Caused by Delftia acidovorans in a Hemodialysis Patient. J. Clin. Microbiol. 2011, 49, 3418–3421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardan, Y.C.; Zarakolu, P.; Altun, B.; Yildirim, A.; Yildirim, G.; Hascelik, G.; Uzun, O. A Cluster of Nosocomial Klebsiella. oxytoca Bloodstream Infections in a University Hospital. Infect. Control. Hosp. Epidemiol. 2004, 25, 878–882. [Google Scholar] [CrossRef] [PubMed]
- De Mauri, A.; Chiarinotti, D.; Andreoni, S.; Molinari, G.L.; Conti, N.; De Leo, M. Leclercia adecarboxylata and catheter-related bacteraemia: Review of the literature and outcome with regard to catheters and patients. J. Med. Microbiol. 2013, 62, 1620–1623. [Google Scholar] [CrossRef]
- Aronoff, D.M.; Peres, C.M.; Serezani, C.H.; Ballinger, M.N.; Carstens, J.K.; Coleman, N.; Peters-Golden, M. Synthetic prostacyclin analogues differentially regulate macrophage function via distinct analogue-receptor binding specificities. J. Immunol. 2007, 178, 1628.e34. [Google Scholar] [CrossRef] [Green Version]
- Coquette, A.; Boeynaems, J.M.; Vray, B. Eicosanoids modulate CR1- and Fc-dependent. Eur. J. Pharmacol. 1992, 226, 1–4. [Google Scholar] [CrossRef]
- Dumble, L.J.; Gibbons, S.; Tejpal, N.; Chou, T.C.; Redgrave, N.G.; Boyle, M.J.; Kahan, B.D. 15 AU81, a prostacyclin analogue, potentiates immunosuppression and mitigates renal injury due to cyclosporine. Transplantation 1993, 55, 1124–1128. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.; Brida, M.; Carlsen, J.; Coats, A.J.; Escribano-Subias, P.; Ferrari, P.; et al. ESC/ERS Scientific Document Group, 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: Developed by the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Endorsed by the International Society for Heart and Lung Transplantation (ISHLT) and the European Reference Network on rare respiratory diseases (ERN-LUNG). Eur. Heart J. 2022, 2022, 3618–3713. [Google Scholar]
- Garner, J.S.; Jarvis, W.R.; Emori, T.G.; Horan, T.C.; Hughes, J.M. CDC definitions for nosocomial infections. Am. J. Infect. Control 1988, 16, 128–140. [Google Scholar] [CrossRef]

| Variables | Total (n = 36) | Iloprost (n = 13) | Epoprostenol (n = 23) | p-Value | |||
|---|---|---|---|---|---|---|---|
| Gender, n (%) | 0.686 | ||||||
| Male | 7 | (19.4) | 3 | (23.1) | 4 | (17.4) | |
| Female | 29 | (80.6) | 10 | (76.9) | 19 | (82.6) | |
| Race, n (%) | 0.525 | ||||||
| Caucasian | 34 | (94.4) | 13 | (100.0) | 21 | (91.3) | |
| African | 2 | (5.6) | 0 | (0.0) | 2 | (8.7) | |
| Age at diagnosis, median (min-max) | 43.0 | (12–81) | 44.0 | (16–77) | 42.0 | (12–81) | 0.820 |
| Comorbidities, n (%) | |||||||
| Yes | 24 | (66.7) | 9 | (69.2) | 15 | (65.2) | 0.806 |
| PH therapy, n (%) | |||||||
| ERA | 27 | (75) | 13 | (100.0) | 14 | (60.9) | 0.014 |
| PDE-5i | 34 | (94.4) | 12 | (92.3) | 22 | (95.7) | 0.674 |
| CCB | 1 | (2.8) | 0 | (0) | 1 | (4.3) | 0.446 |
| PH Aetiology, n (%) | |||
|---|---|---|---|
| 1 PAH | 27 (75.0) | ||
| 1.1 Idiopathic PAH | 14 (38.9) | ||
| 1.2 Heritable PAH | 5 (13.9) | ||
| 1.3 Drug- and toxin-induced PAH | 1 (2.8) | ||
| 1.4 PAH associated with: | |||
| 1.4.1 Connective tissue disease | 3 (8.3) | ||
| 1.4.2 HIV infection | 1 (2.8) | ||
| 1.4.3 Portal hypertension | 1 (2.8) | ||
| 1.4.4 Congenital heart disease | 2 (5.6) | ||
| 1.4.5 Schistosomiasis | 0 (0) | ||
| 1.5 PAH long-term responders to CCB | 0 (0) | ||
| 1.6 PAH with overt features of venous/capillaries (PVOD/PCH) involvement | 0 (0) | ||
| 1.7 Persistent PH of newborn syndrome | 0 (0) | ||
| 2 PH due to left heart disease | 0 (0) | ||
| 3 PH due to lung disease and/or hypoxia | 1 (2.8) | ||
| 4 PH due to pulmonary artery obstructions | 7 (19.4) | ||
| 5 PH with unclear and/or multifactorial mechanisms | 1 (2.8) | ||
| More than one group classification * | 5 (13.9) | ||
| Variables | Total (n = 36) | Iloprost (n = 13) | Epoprostenol (n = 23) | p Value |
|---|---|---|---|---|
| Years of disease until starting iPCA, median (min-max) | 4 (0–29) | 4 (0–9) | 4 (0–29) | 0.987 |
| Days of treatment, median (min-max) | 395.5 (10–2651) | 432 (117–2651) | 329 (10–1638) | 0.267 |
| Days of Hickman, median (min-max) | 306 (3–1904) | 355 (117–1904) | 288 (3–1604) | 0.397 |
| BSI (Hickman), n (%) | 11 (30.6) | 10 (76.9) | 1 (4.3) | <0.001 |
| Multiple infections, n (%) | 7 (19.4) | 7 (53.8) | 0 | <0.001 |
| Deaths during iPCA therapy, n (%) | ||||
| All causes | 13 (36.1) | 4 (30.8) | 9 (39.1) | 0.974 |
| BSI | 3 (8.3) | 3 (23.1) | 0 (0) | 0.04 |
| Variables | Total (n = 36) | No BSI (n = 25) | BSI (n = 11) | p Value |
|---|---|---|---|---|
| Gender, n (%) | 0.559 | |||
| Male | 7 (19.4) | 6 (24.0) | 1 (9.1) | |
| Female | 29 (80.6) | 19 (76.0) | 10 (90.9) | |
| Race, n (%) | 0.861 | |||
| Caucasian | 34 (94.4) | 23 (92.0) | 11 (100) | |
| African | 2 (5.6) | 2 (8.0) | 0 | |
| Comorbidities, n (%) | 24 (66.7) | 16 (64.0) | 8 (72.7) | 0.715 |
| Age at diagnosis (years), median (min-max) | 43 (12–81) | 45 (12–81) | 36 (16–67) | 0.342 |
| Time from diagnosis to iPCA therapy (years), median (min-max) | 4 (0–29) | 4 (0–29) | 4 (0–14) | 0.520 |
| Days of treatment, median (min-max) | 395.5 (10–2651) | 291 (10–2651) | 675 (203–2059) | 0.093 |
| Days of Hickman, median (min-max) | 306 (3–1904) | 281 (3–1604) | 508 (161–1904) | 0.132 |
| Variables | n (%) |
|---|---|
| Total nº of BSIs during iPCA therapy, n = 27 | |
| Multiple BSIs by iPCA cycle | 7 (25.9) |
| 2 | 1 |
| 3 | 4 |
| 4 | 1 |
| 5 | 1 |
| Infections caused by more than one MO | 2 (7.4) |
| Nº of microorganisms identified, n = 29 | |
| Gram-positive | 10 (34.5) |
| Staphylococcus aureus | 5 |
| Staphylococcus epidermidis | 3 |
| Staphylococcus hominis | 2 |
| Gram-negative | 19 (65.5) |
| Pseudomonas aeruginosa | 6 |
| Klebsiella oxytoca | 3 |
| Klebsiella pneumonia | 2 |
| Leclercia adecarboxylata | 2 |
| Acinetobacter iwoffii | 1 |
| Acinetobacter baumannii | 1 |
| Enterobacter cloacae | 1 |
| Burkholderia cepacian | 1 |
| Delftia acidovorans | 1 |
| Ralstonia pickettii | 1 |
| Identification method | |
| Blood cultures | 29 (100) |
| Hickman cateter tip (CR-BSI) | 5 (17.2) |
| Catheter exudate | 2 (6.9) |
| Hospitalization | 25 (92.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camara, R.P.; Coelho, F.d.N.; Cruz-Martins, N.; Marques-Alves, P.; Castro, G.; Baptista, R.; Ferreira, F. Incidence of Bloodstream Infection in Patients with Pulmonary Hypertension under Intravenous Epoprostenol or Iloprost—A Multicentre, Retrospective Study. Int. J. Mol. Sci. 2023, 24, 6434. https://doi.org/10.3390/ijms24076434
Camara RP, Coelho FdN, Cruz-Martins N, Marques-Alves P, Castro G, Baptista R, Ferreira F. Incidence of Bloodstream Infection in Patients with Pulmonary Hypertension under Intravenous Epoprostenol or Iloprost—A Multicentre, Retrospective Study. International Journal of Molecular Sciences. 2023; 24(7):6434. https://doi.org/10.3390/ijms24076434
Chicago/Turabian StyleCamara, Raquel Paulinetti, Francisco das Neves Coelho, Natália Cruz-Martins, Patrícia Marques-Alves, Graça Castro, Rui Baptista, and Filipa Ferreira. 2023. "Incidence of Bloodstream Infection in Patients with Pulmonary Hypertension under Intravenous Epoprostenol or Iloprost—A Multicentre, Retrospective Study" International Journal of Molecular Sciences 24, no. 7: 6434. https://doi.org/10.3390/ijms24076434