
Clinical and Functional Characteristics of the E92K CFTR Gene Variant in the Russian and Turkish Population of People with Cystic Fibrosis
 , , , , , , , , , , and
, , , , , , , , , , and
Abstract
:1. Introduction
2. Results
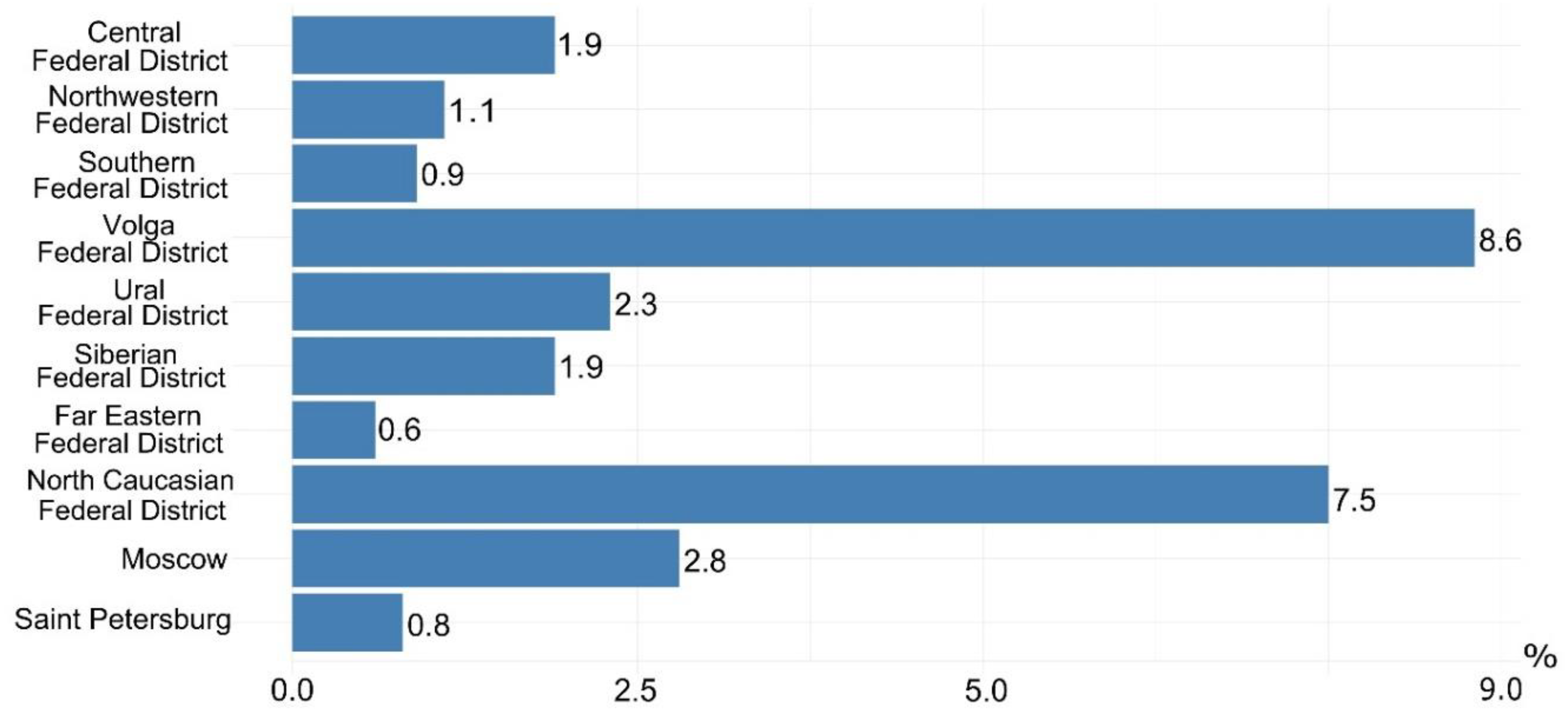
2.1. Assessment of the Frequency of the Genetic Variant of E92K in Different Regions of the Russian Federation and in Turkey
2.2. Characteristics of the Clinical Picture of Patients with the Genetic Variant E92K
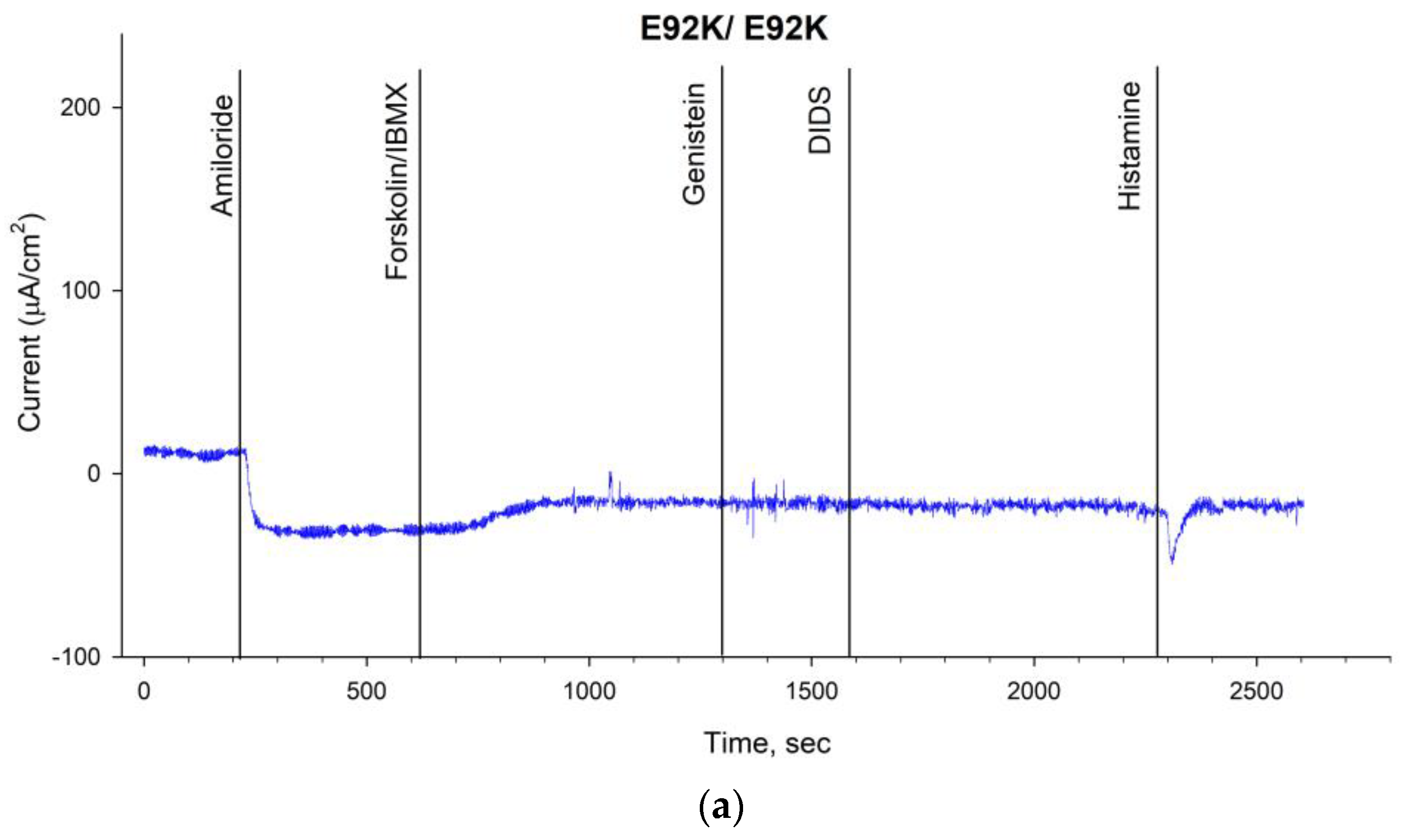
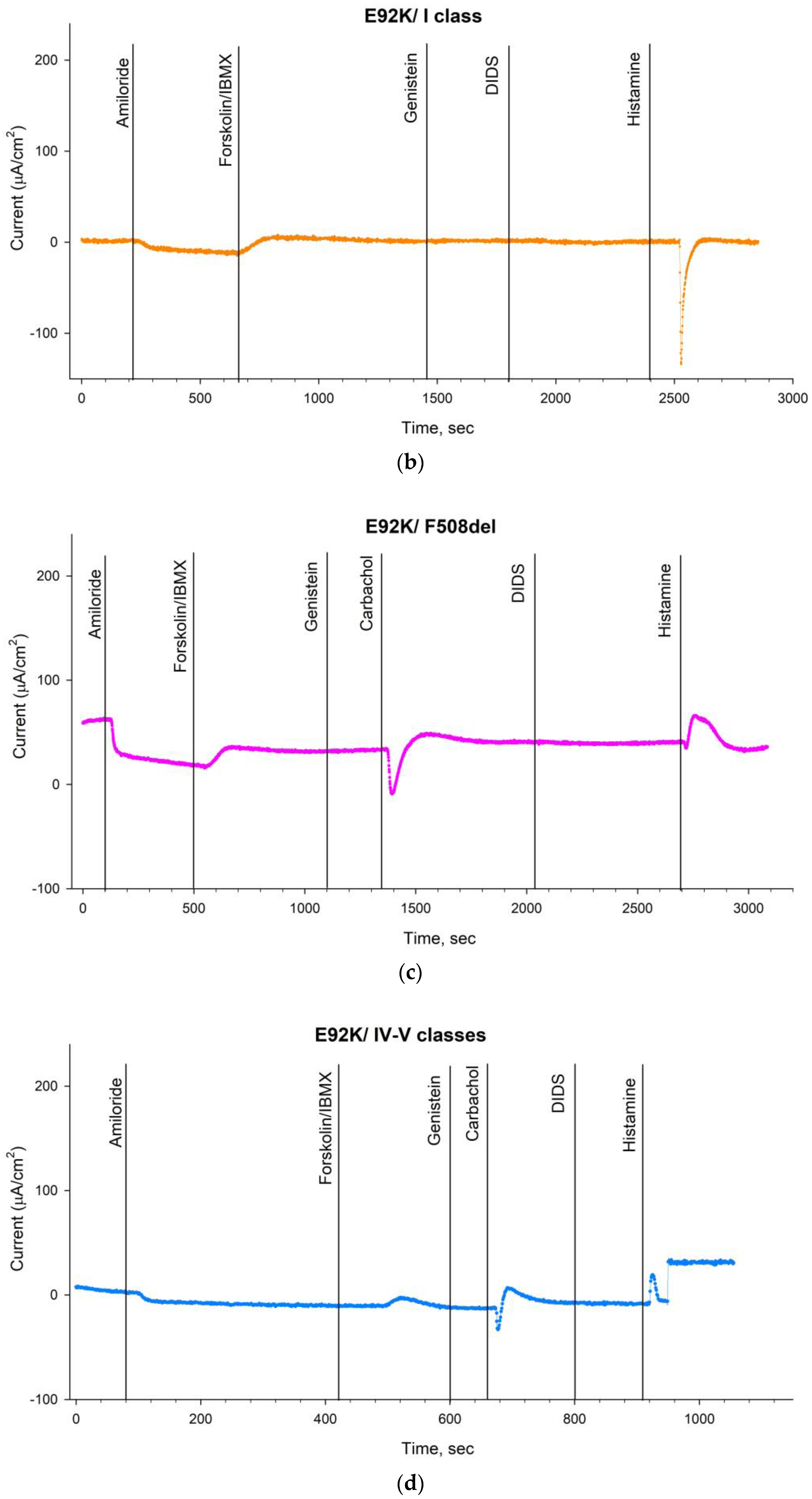
2.3. Evaluation of the Functional Activity of Ion Channels on the Surface of the Intestinal Epithelium by the Intestinal Current Measurements (ICM) Method
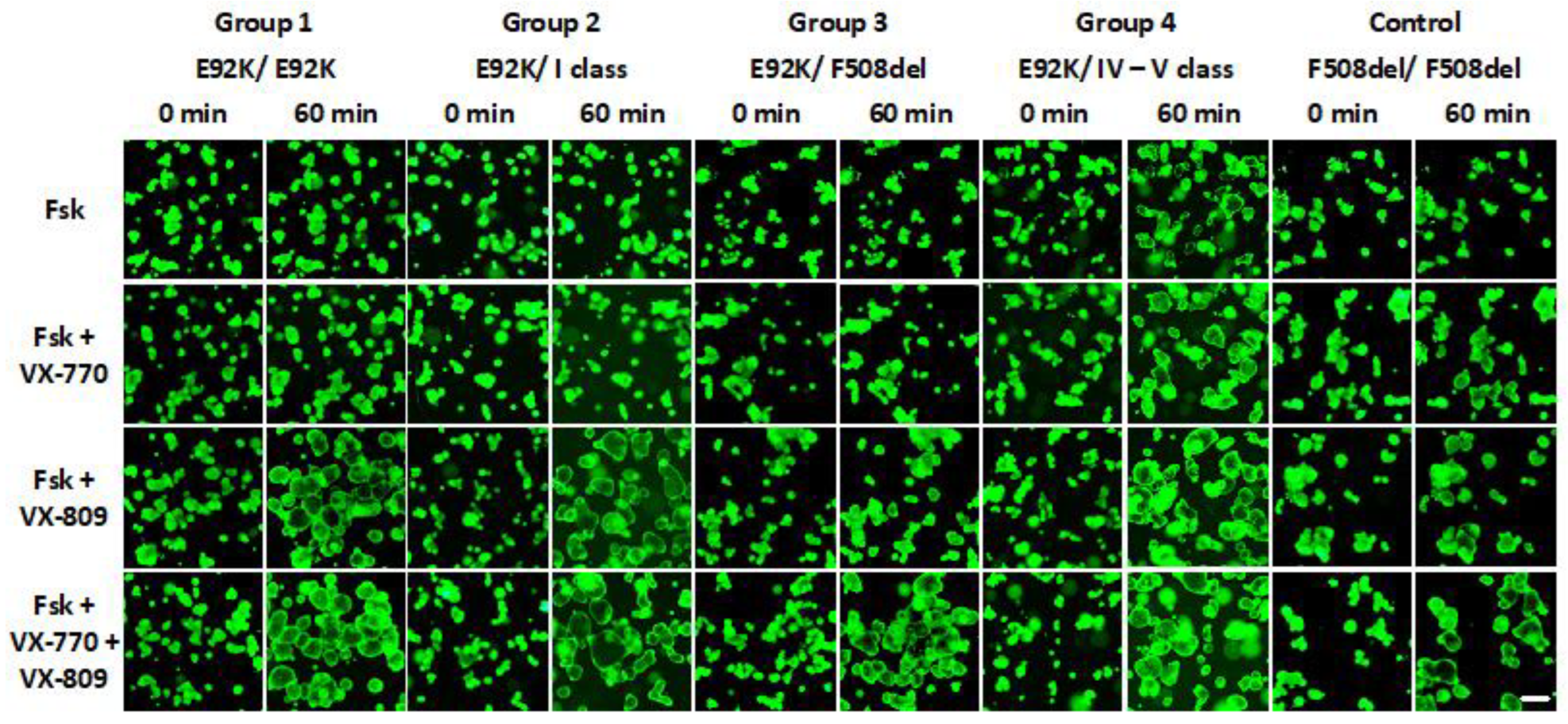
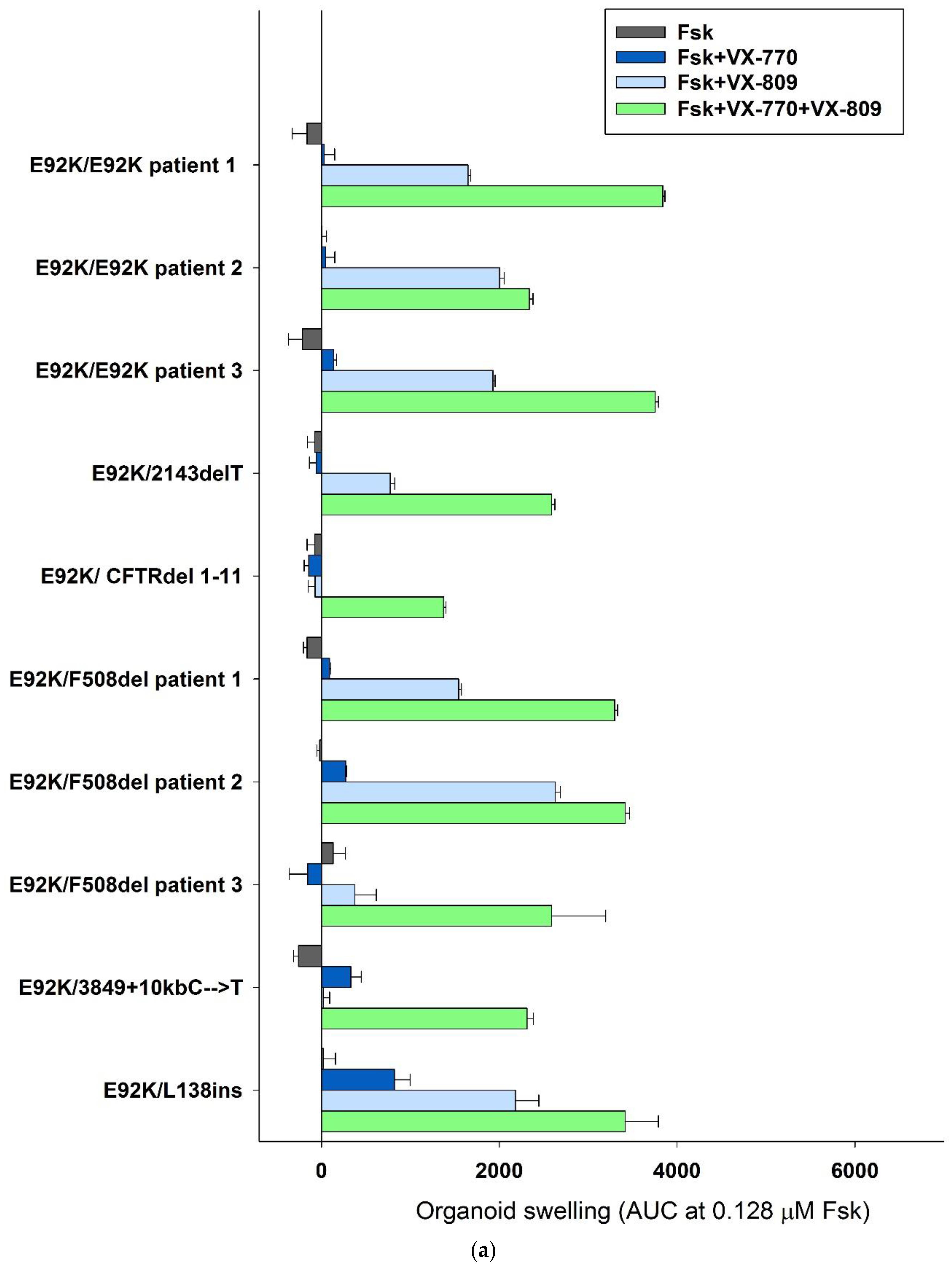
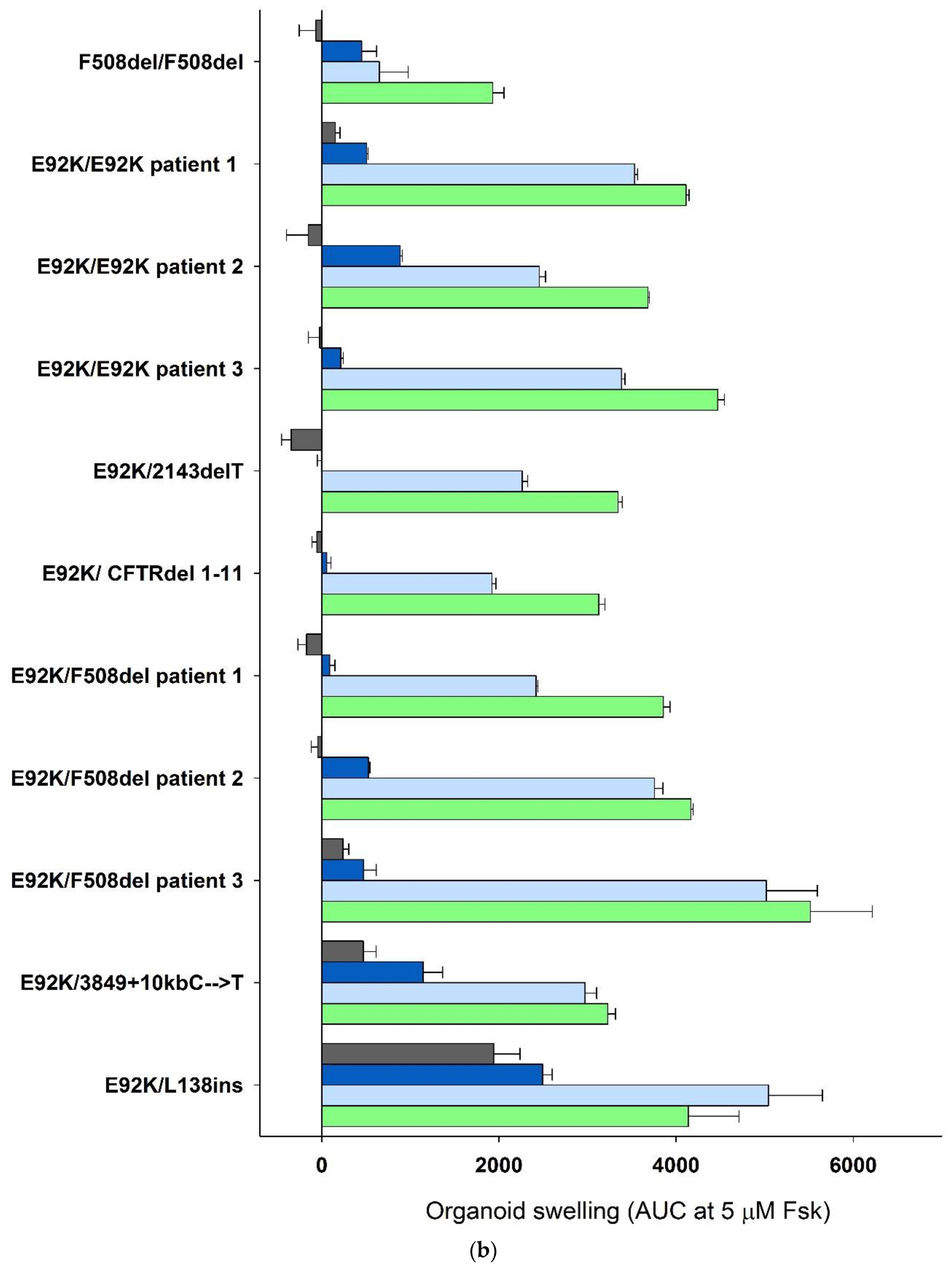
2.4. Evaluation of the Effect of Targeted Drugs on the Functional Activity of the CFTR Channel on Models of Intestinal Organoids
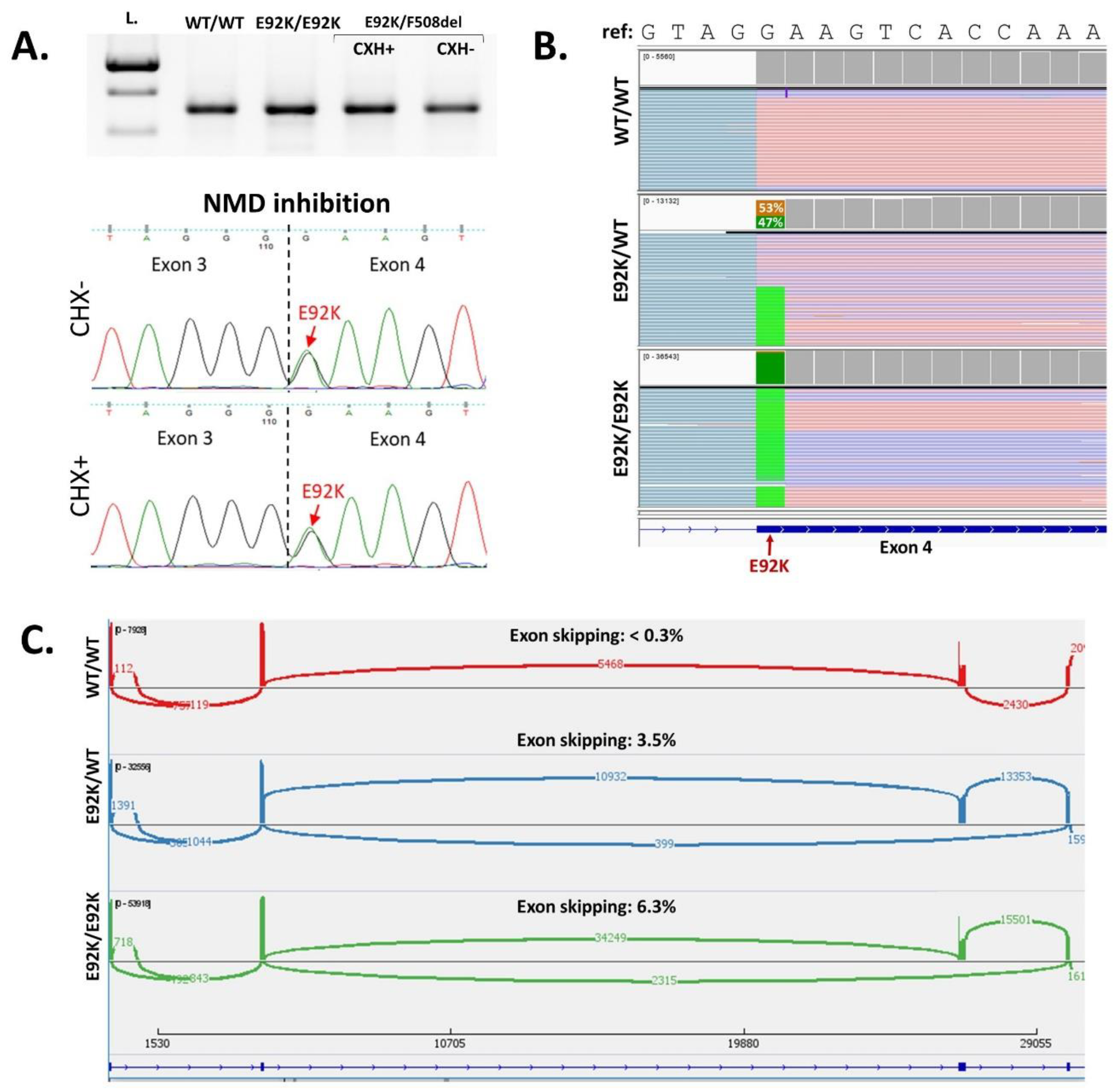
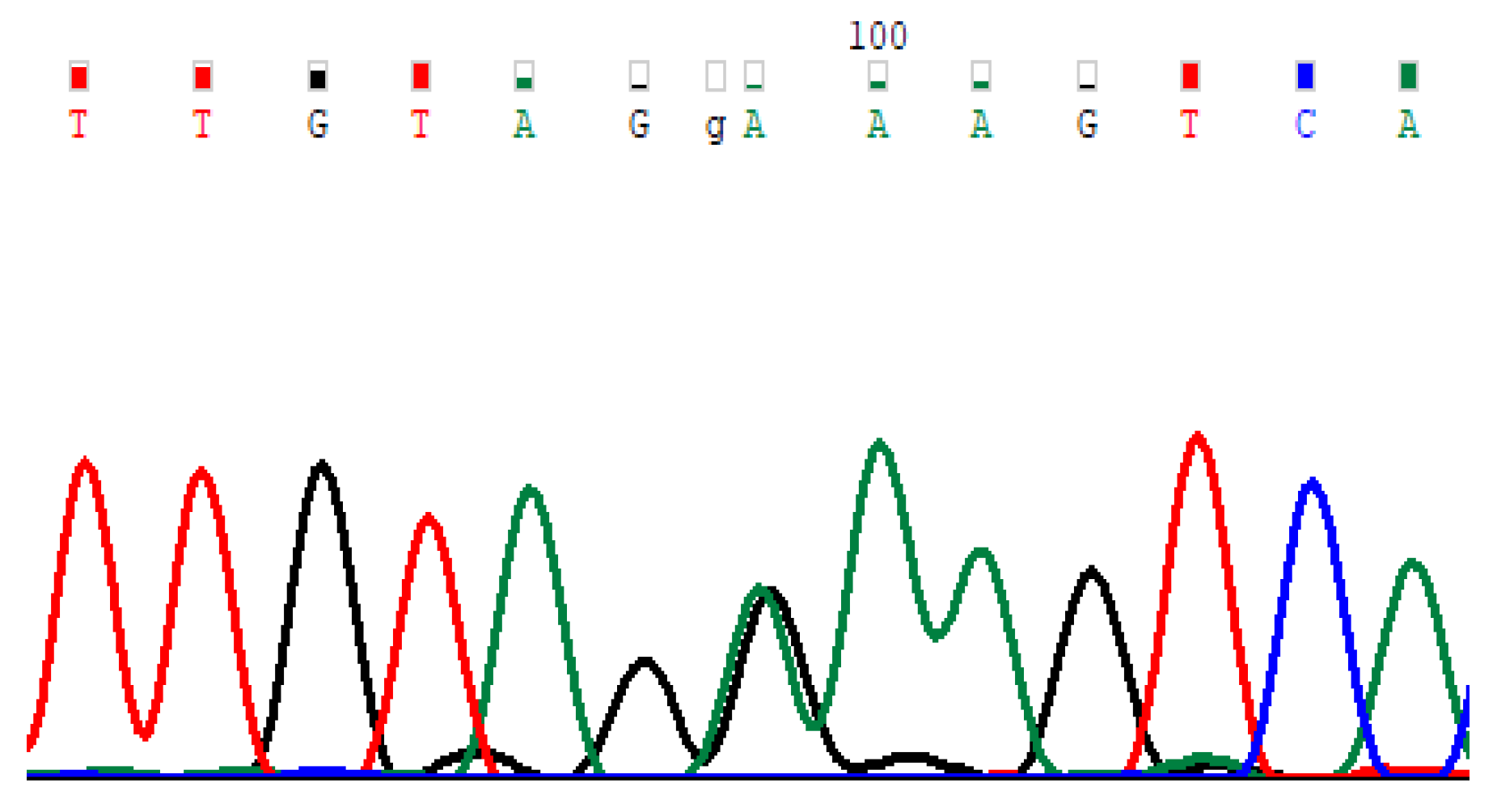
2.5. Functional Assessment of the Effect of E92K Variant on Splicing
3. Discussion
4. Materials and Methods
4.1. Criteria for Inclusion of Patients in the Study. Description of the Clinical Picture
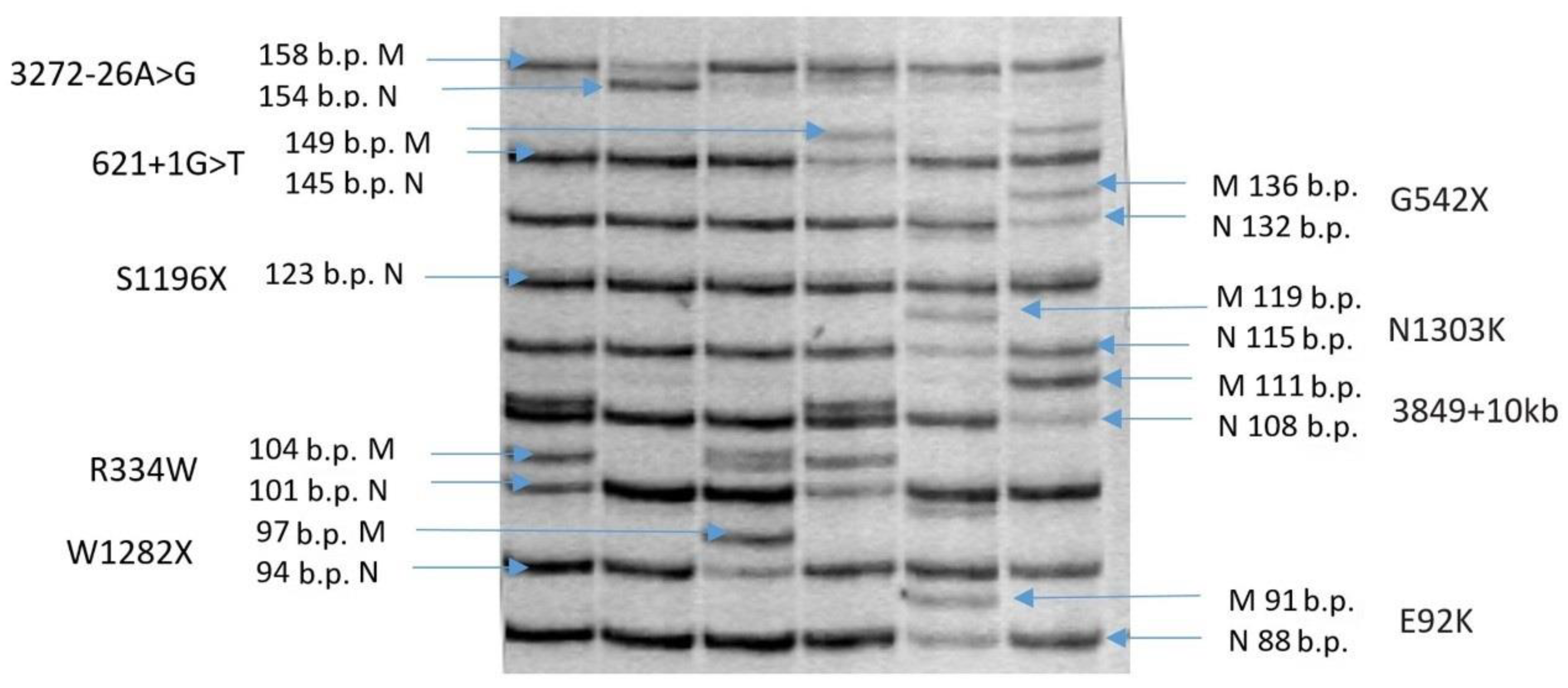
4.2. Determination of the E92K Genetic Variant
4.3. Methods for Evaluating the Functional Activity of the CFTR Channel
4.3.1. Intestinal Current Measurements (ICM)
4.3.2. Human Intestinal Organoids Culture
4.3.3. Forskolin-Induced Swelling (FIS) Assay
4.4. RT-PCR Analysis
4.5. NMD Inhibition
4.6. Targeted Next-Generation Sequencing of PCR-Product
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hangül, M.; Pekcan, S.; Köse, M.; Acıcan, D.; Şahlar, T.E.; Erdoğan, M.; Kendirci, M.; Güney, D.; Öznavruz, H.; Demir, O.; et al. The Incidence of Cystic Fibrosis in the Central Region of Anatolia in Turkey between 2015 and 2016. Balkan Med. J. 2019, 36, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Kashirskaya, N.Y.; Kapranova, N.I.; Kondratyeva, E.I. Cystic Fibrosi, 2nd ed.; Medpraktika-M: Moscow, Russia, 2021. [Google Scholar]
- Berger, H.A.; Travis, S.M.; Welsh, M.J. Regulation of the Cystic Fibrosis Transmembrane Conductance Regulator Cl- Channel by Specific Protein Kinases and Protein Phosphatases. J. Biol. Chem. 1993, 268, 2037–2047. [Google Scholar] [CrossRef] [PubMed]
- Kondratyeva, E.I.; Kashirskaya, N.Y.; Kapranov, N.I. National Consensus “Cystic fibrosis: Definition, Diagnostic Criteria, Therapy”; Borges Company: Moscow, Russia, 2019; p. 356. [Google Scholar]
- Kondratyeva, E.I.; Krasovsky, S.A.; Starinova, M.A.; Voronkova, A.Y.; Amelina, E.L.; Kashirskaya, N.Y.; Avdeev, S.N.; Kutsev, S.I. (Eds.) Register of Patients with Cystic Fibrosis in the Russian Federation, 2020 Year; Medpraktika-M: Moscow, Russia, 2022; p. 68. [Google Scholar]
- Bell, S.C.; De Boeck, K.; Amaral, M.D. New Pharmacological Approaches for Cystic Fibrosis: Promises, Progress, Pitfalls. Pharmacol. Ther. 2015, 145, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Cystic Fibrosis Variant Database. Available online: http://www.genet.sickkids.on.ca/ (accessed on 20 September 2022).
- Orenti, A.; Zolin, A.; Jung, A.; van Rens, J.; Fox, A.; Krasnyk, M.; Daneau, G.; Hatziagorou, E.; Mei-Zahav, M.; Naehrlich, L.; et al. ECFSPR Annual Report 2020. 2022. Available online: https://www.ecfs.eu/sites/default/files/ECFSPR_Report_2020_v1.0%20%2807Jun2022%29_website.pdf (accessed on 27 September 2022).
- Bienvenu, T.; Lopez, M.; Girodon, E. Molecular Diagnosis and Genetic Counseling of Cystic Fibrosis and Related Disorders: New Challenges. Genes 2020, 11, 619. [Google Scholar] [CrossRef]
- Ulusal Kistik Fibrozis Kayıt Sistemi Verileri. Yılı Verileri Database. Available online: https://www.kistikfibrozisturkiye.org (accessed on 27 September 2022).
- Genome Aggregation Database (GnomAD v.2.1.1). Available online: https://gnomad.broadinstitute.org (accessed on 14 September 2022).
- National Center for Biotechnology Information. Available online: https://www.ncbi.nlm.nih.gov/clinvar (accessed on 13 May 2022).
- Clinical and Functional Translation of CFTR. Available online: https://cftr2.org/ (accessed on 29 April 2022).
- Beekman, J.M. Individualized Medicine Using Intestinal Responses to CFTR Potentiators and Correctors. Pediatr. Pulmonol. 2016, 51, S23–S34. [Google Scholar] [CrossRef]
- Dekkers, J.F.; van der Ent, C.K.; Beekman, J.M. Novel Opportunities for CFTR-Targeting Drug Development Using Organoids. Rare Dis. 2013, 1, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Dekkers, J.F.; Berkers, G.; Kruisselbrink, E.; Vonk, A.; De Jonge, H.R.; Janssens, H.M.; Bronsveld, I.; Van De Graaf, E.A.; Nieuwenhuis, E.E.S.; Houwen, R.H.J.; et al. Characterizing Responses to CFTR-Modulating Drugs Using Rectal Organoids Derived from Subjects with Cystic Fibrosis. Sci. Transl. Med. 2016, 8, 344ra84. [Google Scholar] [CrossRef]
- Boj, S.F.; Vonk, A.M.; Statia, M.; Su, J.; Vries, R.R.G.; Beekman, J.M.; Clevers, H. Forskolin-Induced Swelling in Intestinal Organoids: An In Vitro Assay for Assessing Drug Response in Cystic Fibrosis Patients. J. Vis. Exp. 2017, 120, 55159. [Google Scholar] [CrossRef]
- Kondratyeva, E.; Bukharova, T.; Efremova, A.; Melyanovskaya, Y.; Bulatenko, N.; Davydenko, K.; Filatova, A.; Skoblov, M.; Krasovsky, S.; Petrova, N.; et al. Health Characteristics of Patients with Cystic Fibrosis Whose Genotype Includes a Variant of the Nucleotide Sequence c.3140-16T>A and Functional Analysis of This Variant. Genes 2021, 12, 837. [Google Scholar] [CrossRef]
- Nunes, V.; Chillón, M.; Dörk, T.; Tümmler, B.; Casals, T.; Estivill, X. A New Missense Variant (E92K) in the First Transmembrane Domain of the CFTR Gene Causes a Benign Cystic Fibrosis Phenotype. Hum. Mol. Genet. 1993, 2, 79–80. [Google Scholar] [CrossRef]
- Stanke, F.; Ballmann, M.; Bronsveld, I.; Dork, T.; Gallati, S.; Laabs, U.; Derichs, N.; Ritzka, M.; Posselt, H.-G.; Harms, H.K.; et al. Diversity of the Basic Defect of Homozygous CFTR Variant Genotypes in Humans. J. Med. Genet. 2007, 45, 47–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrova, N.V. Molecular Genetic and Clinical Genotypic Peculiarities of Mucoviscidosis in the Russian Populations. Ph.D. Thesis, Research Centre for Medical Genetics, Moscow, Russia, 2009; p. 42, Synopsis of Thesis for the Degree of Doctor of Medical Science. [Google Scholar]
- Register of Patients with Cystic Fibrosis in the Russian Federation 2011. Available online: https://mukoviscidoz.org/doc/registr/Registr_end_2011.pdf (accessed on 20 September 2022).
- Stepanova, A.A.; Abrukova, A.V.; Savaskina, E.N.; Polyakov, A.V. Variant p.E92K is the Main Cause of Cystic Fibrosis in Chuvashs. Genetics 2012, 48, 863–871. [Google Scholar]
- Golubtsova, O.I.; Krasovskiy, S.A.; Kozhevnikova, S.L.; Kapranov, N.I. Clinical Features of the Lesions of the Respiratory Organs in Children with Cystic Fibrosis in the Chuvash Republic. Vopr. Sovrem. Pediatr. 2012, 11, 55–58. [Google Scholar]
- Gené, G.G.; Llobet, A.; Larriba, S.; de Semir, D.; Martínez, I.; Escalada, A.; Solsona, C.; Casals, T.; Aran, J.M. N-Terminal CFTR Missense Variants Severely Affect the Behavior of the CFTR Chloride Channel. Hum. Mutat. 2008, 29, 738–749. [Google Scholar] [CrossRef] [PubMed]
- Van Goor, F.; Yu, H.; Burton, B.; Hoffman, B.J. Effect of Ivacaftor on CFTR Forms with Missense Variants Associated with Defects in Protein Processing or Function. J. Cyst. Fibros. 2014, 13, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, H.Y.; Grove, D.E.; De La Rosa, O.; Houck, S.A.; Sopha, P.; Van Goor, F.; Hoffman, B.J.; Cyr, D.M. VX-809 Corrects Folding Defects in Cystic Fibrosis Transmembrane Conductance Regulator Protein through Action on Membrane-Spanning Domain 1. Mol. Biol. Cell 2013, 24, 3016–3024. [Google Scholar] [CrossRef] [PubMed]
- Castellani, C.; Cuppens, H.; Macek, M.; Cassiman, J.J.; Kerem, E.; Durie, P.; Tullis, E.; Assael, B.M.; Bombieri, C.; Brown, A.; et al. Consensus on the Use and Interpretation of Cystic Fibrosis Variant Analysis in Clinical Practice. J. Cyst. Fibros. 2008, 7, 179–196. [Google Scholar] [CrossRef] [Green Version]
- Golubtsova, O.I.; Krasnov, M.V.; Krasovsky, S.A.; Nikolaev, L.A. Genetic features of cystic fibrosis in patients of the chuvash republic. Mod. Probl. Sci. Educ. 2015, 1, 133. [Google Scholar]
- Ramalho, A.S.; Förstová, E.; Vonk, A.M.; Ferrante, M.; Verfailli, C.; Dupont, L.; Boon, M.; Proesmans, M.; Beekma, J.M.; Sarouk, I.; et al. Correction of CFTR Function in Intestinal Organoids to Guide Treatment of Cystic Fibrosis. Eur. Respir. J. 2021, 57, 1902426. [Google Scholar] [CrossRef]
- Awatade, N.T.; Ramalho, S.; Silva, I.A.L.; Felício, V.; Botelho, H.M.; de Poel, E.; Vonk, A.; Beekman, J.M.; Farinha, C.M.; Amaral, M.D. R560S: A Class II CFTR Variant That Is Not Rescued by Current Modulators. J. Cyst. Fibros. 2019, 18, 182–189. [Google Scholar] [CrossRef]
- Kondratyeva, E.I.; Melianovskaya, Y.L.; Efremova, A.S.; Bulatenko, N.V.; Bukharova, T.B.; Goldshtein, D.V.; Zodbinova, A.E.; Nikonova, V.S.; Zhekaite, E.K.; Kashirskaya, N.Y.; et al. Experience of evaluating functionality of anionic cftr channel methods application in patients with cystic fibrosis diagnosed and supposed. Sib. Med. Rev. 2019, 2, 60–69. [Google Scholar] [CrossRef]
- Joynt, A.T.; Evans, T.A.; Pellicore, M.J.; Davis-Marcisak, E.F.; Aksit, M.A.; Eastman, A.C.; Patel, S.U.; Paul, K.C.; Osorio, D.L.; Bowling, A.D.; et al. Evaluation of Both Exonic and Intronic Variants for Effects on RNA Splicing Allows for Accurate Assessment of the Effectiveness of Precision Therapies. PLoS Genet. 2020, 16, e1009100. [Google Scholar] [CrossRef] [PubMed]
- Graeber, S.Y.; Dopfer, C.; Naehrlich, L.; Gyulumyan, L.; Scheuermann, H.; Hirtz, S.; Wege, S.; Mairbäurl, H.; Dorda, M.; Hyde, R.; et al. Effects of Lumacaftor-Ivacaftor Therapy on Cystic Fibrosis Transmembrane Conductance Regulator Function in Phe508del Homozygous Patients with Cystic Fibrosis. Am. J. Respir. Crit. Care Med. 2018, 197, 1433–1442. [Google Scholar] [CrossRef] [PubMed]
- Veit, G.; Avramescu, R.G.; Chiang, A.N.; Houck, S.A.; Cai, Z.; Peters, K.W.; Hong, J.S.; Pollard, H.B.; Guggino, W.B.; Balch, W.E.; et al. From CFTR Biology toward Combinatorial Pharmacotherapy: Expanded Classification of Cystic Fibrosis Variants. Mol. Biol. Cell 2016, 27, 424–433. [Google Scholar] [CrossRef] [Green Version]
- Zolin, A.; Naehrlich, L.; van Rens, J.; Fox, A.; Iansa, P.; Gulmans, V.; Jung, A.; Cosgriff, R.; Pypops, U.; Naehrlich, L. ECFSPR Annual Report 2015. 2017. Available online: https://www.ecfs.eu/news/ecfs-patient-registry-2015-annual-report (accessed on 27 September 2022).
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of Spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Sinaasappel, M.; Stern, M.; Littlewood, J.; Wolfe, S.; Steinkamp, G.; Heijerman, H.G.M.; Robberecht, E.; Döring, G. Nutrition in Patients with Cystic Fibrosis: A European Consensus. J. Cyst. Fibros. 2002, 1, 51–75. [Google Scholar] [CrossRef] [Green Version]
- WHO. Child Growth Standards. Available online: http://www.who.int/childgrowth/software/en/ (accessed on 15 September 2022).
- Castellani, C.; Duff, A.J.A.; Bell, S.C.; Heijerman, H.G.M.; Munck, A.; Ratjen, F.; Sermet-Gaudelus, I.; Southern, K.W.; Barben, J.; Flume, P.A.; et al. ECFS Best Practice Guidelines: The 2018 Revision. J. Cyst. Fibros. 2018, 17, 153–178. [Google Scholar] [CrossRef] [Green Version]
- WHO. Expert Committee; WHO: Geneva, Switzerland, 1995. [Google Scholar]
- Petrova, N.V.; Kashirskaya, N.Y.; Vasilyeva, T.A.; Timkovskaya, E.E.; Voronkova, A.Y.; Shabalova, L.A.; Kondratyeva, E.I.; Sherman, V.D.; Novoselova, O.G.; Kapranov, N.I.; et al. High Prevalence of W1282X Variant in Cystic Fibrosis Patients from Karachay-Cherkessia. J. Cyst. Fibros. 2016, 15, e28–e32. [Google Scholar] [CrossRef] [Green Version]
- Farrell, P.M.; White, T.B.; Ren, C.L.; Hempstead, S.E.; Accurso, F.; Derichs, N.; Howenstine, M.; McColley, S.A.; Rock, M.; Rosenfeld, M.; et al. Diagnosis of Cystic Fibrosis: Consensus Guidelines from the Cystic Fibrosis Foundation. J. Pediatr. 2017, 181, S4–S15. [Google Scholar] [CrossRef] [Green Version]
- Derichs, N.; Sanz, J.; Von Kanel, T.; Stolpe, C.; Zapf, A.; Tümmler, B.; Gallati, S.; Ballmann, M. Intestinal Current Measurement for Diagnostic Classification of Patients with Questionable Cystic Fibrosis: Validation and Reference Data. Thorax 2010, 65, 594–599. [Google Scholar] [CrossRef] [Green Version]
- Vonk, A.M.; van Mourik, P.; Ramalho, A.S.; Silva, I.A.L.; Statia, M.; Kruisselbrink, E.; Suen, S.W.F.; Dekkers, J.F.; Vleggaar, F.P.; Houwen, R.H.J.; et al. Protocol for Application, Standardization and Validation of the Forskolin-Induced Swelling Assay in Cystic Fibrosis Human Colon Organoids. STAR Protoc. 2020, 1, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Kondratyeva, E.; Efremova, A.; Melyanovskaya, Y.; Petrova, N.; Satsuk, N.; Bulatenko, N.; Bukharova, T.; Zodbinova, A.; Sherman, V.; Kashirskaya, N.; et al. Clinical and Genetic Characterization of Patients with Cystic Fibrosis and Functional Assessment of the Chloride Channel with the Pathogenic Variant c.831G>A (p.Trp277*), Described for the First Time. Gene 2020, 761, 145023. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| E92K/ E92K Group 1 | E92K/ I Class Group 2 | E92K/ F508del Group 3 | E92K/IV-VI Classes Group 4 | F508del/ F508del Group 5 | p | p | |||
|---|---|---|---|---|---|---|---|---|---|
| Number of patients | 33 | 36 | 82 | 8 | 881 | ||||
| Age at the time of the study, years | Me (Q25;Q75) | 12.1 (7.4; 22.5) | 9.0 (4.7; 19.2) | 13.6 (6.8; 22.7) | 14.2 (11.1; 25.3) | 9.7 (5.2; 15.6) | p = 0.004 | P3–5 = 0.014 | |
| Age of diagnosis, years | Me (Q25;Q75) | 0.8 (0.4; 11.4) | 0.6 (0.2; 7.4) | 2.7 (0.3; 9.5) | 6.5 (4.2; 14.0) | 0.3 (0.1; 1.3) | p < 0.001 | P1–5 < 0.001 P2–5 = 0.028 P3–5 < 0.001 P4–5 = 0.001 | |
| Sweat test Conductivity, mmol/L | 100.0 (90.5; 102.0) | 105.8 (97.5; 114.5) | 108.5 (93.0; 120.0) | 92.0 (88.5; 111.0) | 112.0 (101.0; 121.0) | p = 0.016 | P1–5 = 0.019 | ||
| Fecal elastase | ≥200 ng/g | 12 (75.0%) | 12 (60.0%) | 29 (76.3%) | 4 (80.0%) | 44 (9.8%) | p < 0.001 | P1–5 < 0.001 P2–5 < 0.001 P3–5 < 0.001 P4–5 = 0.001 | |
| Diagnosis by newborn screening | Yes, positive,% | 11 (34.4%) | 11 (39.3%) | 29 (36.3%) | 1 (14.3%) | 467 (54.7%) | p = 0.008 | ||
| Yes, negative, % | 0 (0.0%) | 2 (7.1%) | 2 (2.5%) | 0 (0.0%) | 15 (1.8%) | - | |||
| Microbiological examination | Chronic Ps. aeruginosa | 9 (27.3%) | 9 (25.7%) | 30 (36.6%) | 3 (37.5%) | 295 (33.9%) | p = 0.738 | - | |
| Intermittent Ps. aeruginosa | 2 (6.1%) | 7 (20.0%) | 15 (18.5%) | 1 (14.3%) | 133 (15.7%) | p = 0.509 | - | ||
| Chronic Staph. aureus | 20 (60.6%) | 17 (48.6%) | 41 (50.0%) | 2 (25.0%) | 526 (60.8%) | p = 0.053 | - | ||
| Chronic Burkholderia cepacia complex | 2 (6.1%) | 2 (5.7%) | 9 (11.0%) | 1 (12.5%) | 59 (6.8%) | p = 0.502 | - | ||
| H. influenzae | 1 (3.1%) | 1 (2.9%) | 1 (1.30%) | 0 (0.0%) | 52 (6.2%) | p = 0.405 | - | ||
| Achromobacter | 1 (3.1%) | 2 (5.6%) | 4 (4.9%) | 0 (0.0%) | 48 (5.6%) | p > 0.99 | - | ||
| MRSA | 3 (9.4%) | 0 (0.0%) | 6 (7.3%) | 2 (25.0%) | 30 (3.5%) | p = 0.010 | P4–5 = 0.008 | ||
| Respiratory function | FEV1, % | 80.3 ± 31.3 | 73.6 ± 33.7 | 71.2 ± 30.0 | 72.8 ± 21.6 | 79.3 ± 24.9 | p = 0.271 | ||
| FVC, % | 83.8 ± 30.1 | 79.3 ± 28.4 | 77.7 ± 24.2 | 87.0 ± 8.3 | 86.8 ± 20.7 | p = 0.153 | |||
| BMI, kg/m2 Me (Q25;Q75)) | 16.0 (14.4; 19.5) | 17.0 (15.1; 18.8) | 17.2 (14.9; 19.8) | 18.0 (14.5; 19.3) | 15.8 (14.6; 17.8) | p = 0.004 | P3–5 = 0.011 | ||
| Complications | ABPA | 0 (0.0%) | 2 (5.7%) | 3 (3.7%) | 0 (0.0%) | 14 (1.6%) | p = 0.176 | ||
| Diabetes (insulin treatment) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 30 (3.4%) | p = 0.363 | |||
| Hemoptysis | 1 (3.0%) | 0 (0.0%) | 4 (4.9%) | 0 (0.0%) | 8 (0.9%) | p = 0.046 | P3–5 = 0.006 | ||
| Occur malignancy | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (0.1%) | p > 0.99 | |||
| Osteoporosis | 1 (5.9%) | 1 (3.6%) | 4 (6.8%) | 0 (0.0%) | 46 (7.7%) | p = 0.976 | |||
| Polyposis of the upper respiratory tract | 4 (12.1%) | 7 (20.0%) | 25 (30.5%) | 1 (12.5%) | 253 (30.7%) | p = 0.090 | |||
| Liver damage | Cirrhosis of the liver with hypertension | 0 (0.0%) | 1 (100%) | 2 (33.3%) | 0 (0.0%) | 44 (21.4%) | p = 0.566 | ||
| Cirrhosis of the liver without hypertension | 0 (0.0%) | 0 (0.0%) | 1 (16.7%) | 0 (0.0%) | 24 (11.7%) | ||||
| Liver damage without cirrhosis | 1 (100%) | 0 (0.0%) | 3 (50.0%) | 0 (0.0%) | 138 (67.0%) | ||||
| Therapy | NaCl | 15 (45.5%) | 18 (51.4%) | 53 (64.6%) | 3 (37.5%) | 627 (72.0%) | p < 0.001 | P1–5 = 0.010 | |
| Antibiotic | 7 (21.2%) | 12 (33.3%) | 37 (45.1%) | 4 (50.0%) | 417 (47.7%) | p = 0.021 | P1–5 = 0.028 | ||
| Antibiotic Intravenous | 8 (25.0%) | 12 (33.3%) | 27 (32.9%) | 2 (25.0%) | 342 (39.3%) | p = 0.321 | |||
| Antibiotic tablets | 11 (33.3%) | 17 (47.2%) | 45 (54.9%) | 5 (62.5%) | 540 (61.8%) | p = 0.006 | P1–5 = 0.010 | ||
| Bronchodilator | 9 (27.3%) | 16 (44.4%) | 39 (47.6%) | 5 (62.5%) | 444 (50.8%) | p = 0.087 | |||
| Oxygen | 0 (0.0%) | 3 (8.3%) | 6 (7.3%) | 0 (0.0%) | 28 (3.2%) | p = 0.112 | |||
| rhDNase | 31 (93.9%) | 35 (97.2%) | 81 (98.8%) | 8 (100%) | 852 (97.1%) | p = 0.529 | |||
| Azithromycin | 4 (12.1%) | 6 (16.7%) | 14 (17.1%) | 3 (37.5%) | 287 (33.2%) | p = 0.001 | P3–5 = 0.028 | ||
| Ursodeoxycholic acid | 24 (75%) | 30 (83.3%) | 66 (80.5%) | 5 (62.5%) | 820 (93.5%) | p < 0.001 | P1–5 = 0.001 P3–5 < 0.001 P4–5 = 0.005 | ||
| Pancreatic enzymes | 24 (75%) | 24 (66.7%) | 63 (76.8%) | 5 (62.5%) | 869 (99.2%) | p < 0.001 | P1–5 < 0.001 P2–5 < 0.001 P3–5 < 0.001 P4–5 < 0.001 | ||
| PPI | 2 (6.1%) | 4 (11.8%) | 17 (20.7%) | 0 (0.0%) | 175 (20.1%) | p = 0.118 | |||
| Vitamin | 21 (65.6%) | 34 (94.4%) | 61 (76.3%) | 7 (87.5%) | 827 (95.1%) | p < 0.001 | P1–2 = 0.026 P1–5 < 0.001 P3–5 < 0.001 | ||
| CF physiotherapy | 23 (71.9%) | 23 (63.9%) | 60 (74.1%) | 7 (87.5%) | 741 (85.7%) | p < 0.001 | P2–5 = 0.004 | ||
| E92K/E92K (Group 1) | ||||||
| patient | ΔISC, µA/cm2 | amiloride | forskolin/IBMX | genistein | DIDS | histamine |
| 1 | M ± m CF | −23.5 | 8.75 ± 3.89 | 1.5 ± 0.71 | 1.5 ± 0.71 | 18.25 ± 5.3 |
| 2 | M ± m CF | −0.5 | 7.83 ± 2.13 | 0.5 | 0.5 | 12.5 ± 3.37 |
| 3 | M ± m CF | −4.67 ± 3.01 | 5.33 ± 1.02 | 0.5 | 0.5 | 6.33 ± 0.82 |
| M ± m total Me | −7.81 ± 3.83 2.5 | 7.13 ± 1.05 6.5 | 0.75 ± 0.2 0.5 | 0.75 ± 0.2 0.5 | 11.63 ± 2.26 10.75 | |
| E92K/CFTRdele1-11 и E92K/2143delT (Group 2) | ||||||
| ΔISC, µA/cm2 | amiloride | forskolin/IBMX | genistein | DIDS | histamine | |
| 1 | M ± m CF | −5.5 ± 1.87 | 6.67 ± 2.68 | 1 | 0.5 | 53.83 ± 10.51 |
| 2 | M ± m CF | −6.33 | 4.67 ± 1.02 | 1.17 ± 0.2 | 1.17 ± 0.2 | 13.17 ± 6.42 |
| M ± m total Me | −5.92 ± 1.01 −5.75 | 5.67 ± 1.25 5.25 | 1.08 ± 0.09 1 | 0.83 ± 0.18 0.75 | 33.5 ± 11.11 30.75 | |
| E92K/F508del (Group 3) | ||||||
| ΔISC, µA/cm2 | amiloride | forskolin/IBMX | genistein | DIDS | histamine | |
| 1 | M ± m CF | −8 ± 0.71 | 17.75 ± 3.89 | 0.75 ± 0.35 | 1 | 7.25 ± 1.77 |
| 2 | M ± m CF | −4.5 ± 2.12 | 17.75 ± 3.18 | 1.75 ± 0.35 | 1.75 ± 0.35 | 2.25 ± 0.35 |
| 3 | M ± m CF | −38.83 ± 4.32 | 17.17 ± 1.43 | 1 | 1 | 17.33 ± 2.68 |
| M ± m total | −20.21 ± 7.29 | 17.5 ± 0.97 | 1.14 ± 0.19 | 1.21 ± 0.16 | 10.14 ± 3.02 | |
| E92K/L138ins и E92K/3849 + 10kbC > T (Group 4) | ||||||
| ΔISC, µA/cm2 | amiloride | forskolin/IBMX | genistein | DIDS | histamine | |
| 1 | M ± m CF | −5 ± 0.61 | 14.5 ± 1.87 | 2.5 | 2.5 | 37.33 ± 3.56 |
| 2 | M ± m CF | −4.67 ± 0.74 | 5.83 ± 1.63 | 2.5 | 2.5 | 14.83 ± 2.35 |
| M ± m total | −4.83 ± 0.39 | 10.17 ± 2.34 | 2.5 | 2.5 | 26.08 ± 5.77 | |
| M ± m F508del/F508del | −18.39 ± 5.62 | 3.06 ± 0.89 | 1.83 ± 0.35 | 1.83 ± 0.35 | 21.5 ± 5.46 | |
| M ± m PI-CF * | −23.67 ± 4.36 | 2.97 ± 0.61 | 1.4 ± 0.25 | 1.67 ± 0.28 | 19.07 ± 3.69 | |
| Healthy M ± m | −8.98 ± 2.23 | 25.78 ± 3.37 | 2 ± 0.2 | 1.8 ± 0.18 | 101.68 ± 9.78 | |
| Reference value according to European SOP * | −8.5 ± 10.7 | 19.5 ± 13.4 | - | - | 32.4 ± 19.7 | |
| Genotypes (Legacy Name) | Genotypes (c. DNA Name) | Genotypes (Protein Name) | Gender | Total | Russian | Turkish | ||
|---|---|---|---|---|---|---|---|---|
| Male | Female | |||||||
| E92K/E92K (Group 1) | (c.[274G > A];[274G > A] | p.[Glu92Lys];[Glu92Lys] | N | 14 | 19 | 33 | 25 | 8 |
| % | 42.4 | 57.6 | 100.0 | |||||
| E92K/I class (Group 2) | c.[274G > A];[I class] | p.[Glu92Lys];[I class] | N | 21 | 15 | 36 | 33 | 3 |
| % | 58.3 | 41.7 | 100.0 | |||||
| E92K/F508del (Group 3) | c.[274G > A];[1521_1523delCTT] | p.[Glu92Lys];[Phe508del] | N | 37 | 45 | 82 | 81 | 1 |
| % | 45.1 | 54.9 | 100 | |||||
| E92K/IV-VI classes (Group 4) | c.[274G > A];[IV-V classes] | p.[Glu92Lys];[IV-V classes] | N | 3 | 5 | 8 | 6 | 2 |
| % | 37.5 | 62.5 | 100.0 | |||||
| F508del/F508del (Group 5, control) | c.[1521_1523delCTT];[1521_1523delCTT] | p.[Phe508del];[Phe508del] | N | 442 | 439 | 881 | 787 | 94 |
| % | 50.2 | 49.8 | 100.0 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kondratyeva, E.; Melyanovskaya, Y.; Bulatenko, N.; Davydenko, K.; Filatova, A.; Efremova, A.; Skoblov, M.; Bukharova, T.; Sherman, V.; Voronkova, A.; et al. Clinical and Functional Characteristics of the E92K CFTR Gene Variant in the Russian and Turkish Population of People with Cystic Fibrosis. Int. J. Mol. Sci. 2023, 24, 6351. https://doi.org/10.3390/ijms24076351
Kondratyeva E, Melyanovskaya Y, Bulatenko N, Davydenko K, Filatova A, Efremova A, Skoblov M, Bukharova T, Sherman V, Voronkova A, et al. Clinical and Functional Characteristics of the E92K CFTR Gene Variant in the Russian and Turkish Population of People with Cystic Fibrosis. International Journal of Molecular Sciences. 2023; 24(7):6351. https://doi.org/10.3390/ijms24076351
Chicago/Turabian StyleKondratyeva, Elena, Yuliya Melyanovskaya, Nataliya Bulatenko, Ksenia Davydenko, Alexandra Filatova, Anna Efremova, Mikhail Skoblov, Tatiana Bukharova, Viktoriya Sherman, Anna Voronkova, and et al. 2023. "Clinical and Functional Characteristics of the E92K CFTR Gene Variant in the Russian and Turkish Population of People with Cystic Fibrosis" International Journal of Molecular Sciences 24, no. 7: 6351. https://doi.org/10.3390/ijms24076351