

Decreased Gas6 and sAxl Plasma Levels Are Associated with Hair Loss in COVID-19 Survivors
 , , , , , , ,
, , , , , , ,  , , ,
, , ,  , , , , , , , , and
on behalf of the No-More COVID Groupadd
Show full author list
, , , , , , , , and
on behalf of the No-More COVID Groupadd
Show full author list
Abstract
:1. Introduction
2. Results
2.1. Study Population
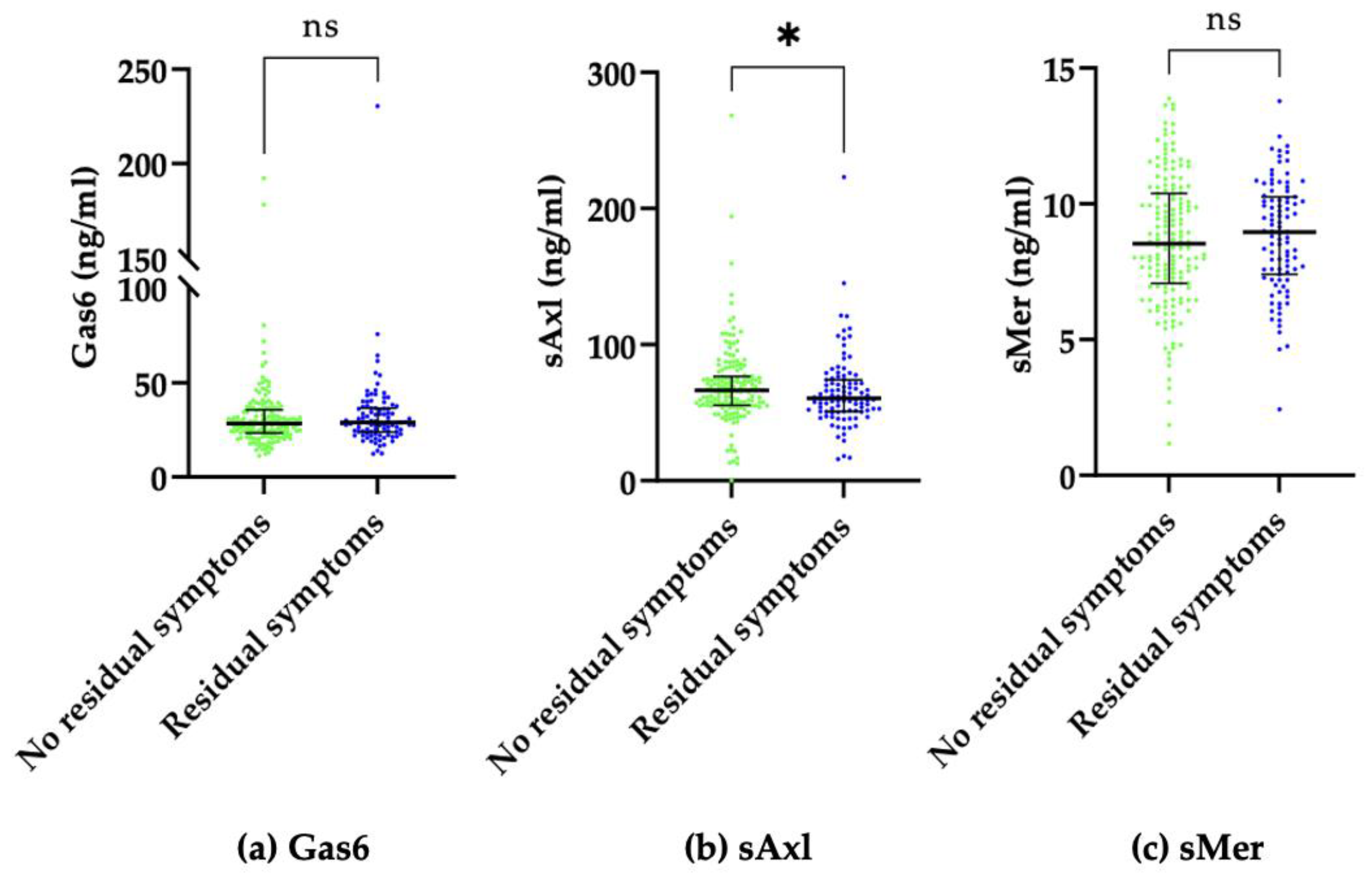
2.2. Residual Symptoms
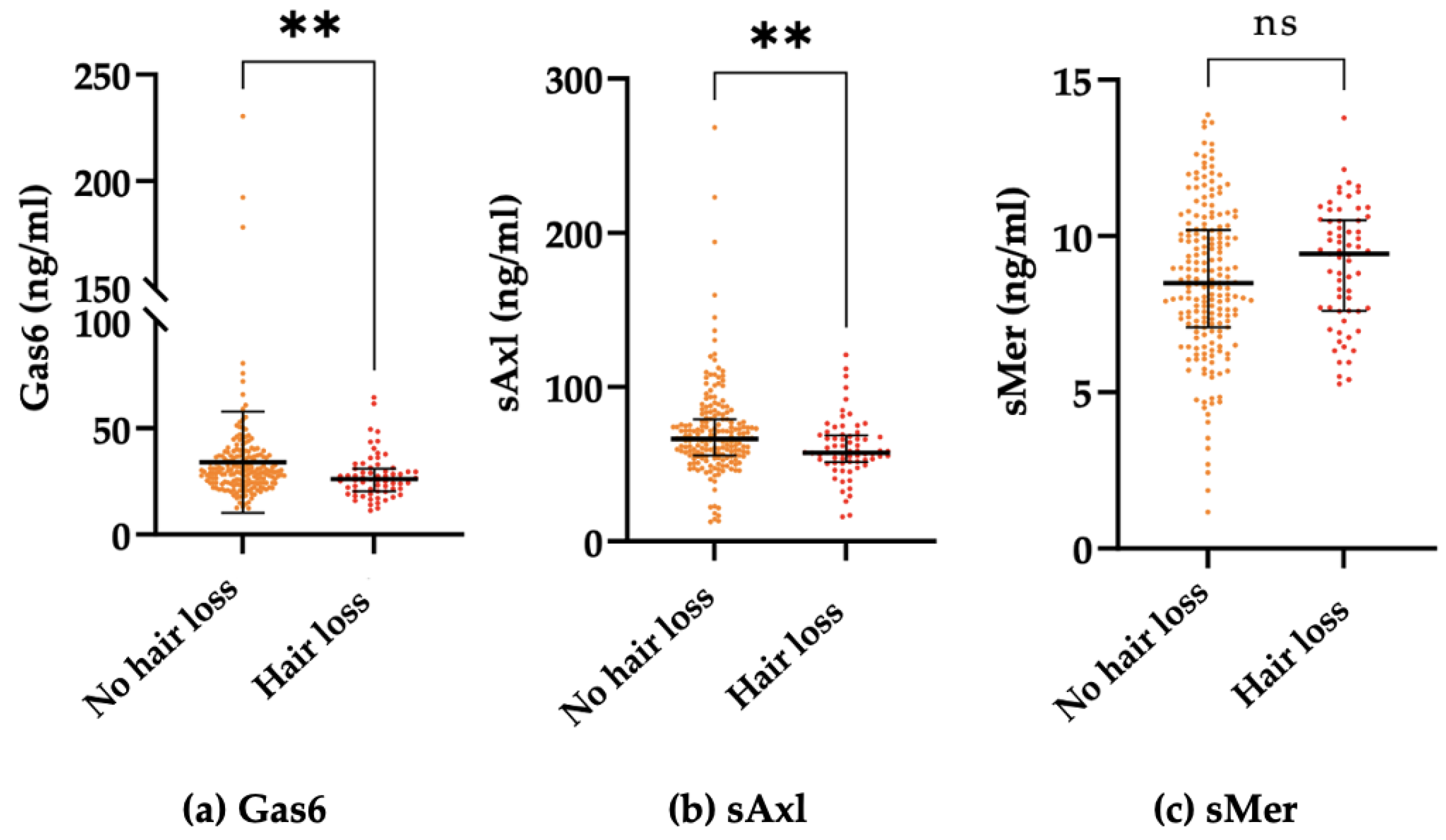
2.3. Hair Loss
3. Discussion
4. Methods and Materials
4.1. Patients
4.2. Clinical Evaluation
4.3. Blood Sample Collection
4.4. Circulating Gas6 Levels Determination
4.5. Soluble Axl (sAxl) Levels Determination
4.6. Soluble Mer (sMer) Levels Determination
4.7. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat. Immunol. 2022, 23, 210–216. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Bellan, M.; Soddu, D.; Balbo, P.E.; Baricich, A.; Zeppegno, P.; Avanzi, G.C.; Baldon, G.; Bartolomei, G.; Battaglia, M.; Battistini, S.; et al. Respiratory and Psychophysical Sequelae among Patients with COVID-19 Four Months after Hospital Discharge. JAMA Netw. Open 2021, 4, e2036142. [Google Scholar] [CrossRef] [PubMed]
- Baricich, A.; Borg, M.B.; Cuneo, D.; Cadario, E.; Azzolina, D.; Balbo, P.E.; Bellan, M.; Zeppegno, P.; Pirisi, M.; Cisari, C.; et al. Midterm functional sequelae and implications in rehabilitation after COVID-19. A cross-sectional study. Eur. J. Phys. Rehabil. Med. 2021, 57, 199–207. [Google Scholar] [CrossRef]
- Bellan, M.; Baricich, A.; Patrucco, F.; Zeppegno, P.; Gramaglia, C.; Balbo, P.E.; Carriero, A.; Amico, C.S.; Avanzi, G.C.; Barini, M.; et al. Long-term sequelae are highly prevalent one year after hospitalization for severe COVID-19. Sci. Rep. 2021, 11, 22666. [Google Scholar] [CrossRef] [PubMed]
- Kessel, S.A.M.v.; Hartman, T.C.O.; Lucassen, P.L.B.J.; van Jaarsveld, C.H.M. Post-acute and long-COVID-19 symptoms in patients with mild diseases: A systematic review. Fam. Pract. 2021, 39, 159–167. [Google Scholar] [CrossRef]
- Crook, H.; Raza, S.; Nowell, J.; Young, M.; Edison, P. Long Covid—Mechanisms, Risk Factors, and Management. BMJ 2021, 374. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.D.; Lavelle, M.; Boursiquot, B.C.; Wan, E.Y. Long-term complications of COVID-19. Am. J. Physiol. Cell. Physiol. 2022, 322, C1–C11. [Google Scholar] [CrossRef] [PubMed]
- Stefanou, M.-I.; Palaiodimou, L.; Bakola, E.; Smyrnis, N.; Papadopoulou, M.; Paraskevas, G.P.; Rizos, E.; Boutati, E.; Grigoriadis, N.; Krogias, C.; et al. Neurological manifestations of long-COVID syndrome: A narrative review. Ther. Adv. Chronic Dis. 2022, 13, 20406223221076890. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- McElvaney, O.J.; McEvoy, N.L.; McElvaney, O.F.; Carroll, T.P.; Murphy, M.P.; Dunlea, D.M.; Ni Choileain, O.; Clarke, J.; O’Connor, E.; Hogan, G.; et al. Characterization of the Inflammatory Response to Severe COVID-19 Illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal Coagulation Parameters Are Associated with Poor Prognosis in Patients with Novel Coronavirus Pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellan, M.; Apostolo, D.; Albè, A.; Crevola, M.; Errica, N.; Ratano, G.; Tonello, S.; Minisini, R.; D’Onghia, D.; Baricich, A.; et al. Determinants of long COVID among adults hospitalized for SARS-CoV-2 infection: A prospective cohort study. Front. Immunol. 2022, 13, 1038227. [Google Scholar] [CrossRef] [PubMed]
- Bellan, M.; Cittone, M.G.; Tonello, S.; Rigamonti, C.; Castello, L.M.; Gavelli, F.; Pirisi, M.; Sainaghi, P.P. Gas6/TAM System: A Key Modulator of the Interplay between Inflammation and Fibrosis. Int. J. Mol. Sci. 2019, 20, 5070. [Google Scholar] [CrossRef] [Green Version]
- Lemke, G. Biology of the TAM Receptors. Cold Spring Harb. Perspect. Biol. 2013, 5, a009076. [Google Scholar] [CrossRef] [PubMed]
- Sainaghi, P.P.; Bellan, M.; Nerviani, A. Role of the Gas6/TAM System as a Disease Marker and Potential Drug Target. Dis. Mark. 2021, 2021, 2854925. [Google Scholar] [CrossRef]
- Law, L.A.; Graham, D.K.; di Paola, J.; Branchford, B.R. GAS6/TAM Pathway Signaling in Hemostasis and Thrombosis. Front. Med. 2018, 5, 137. [Google Scholar] [CrossRef] [Green Version]
- Zhu, C.; Wei, Y.; Wei, X. AXL receptor tyrosine kinase as a promising anti-cancer approach: Functions, molecular mechanisms and clinical applications. Mol. Cancer 2019, 18, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Ekman, C.; Stenhoff, J.; Dahlbäck, B. Gas6 is complexed to the soluble tyrosine kinase receptor Axl in human blood. J. Thromb. Haemost. 2010, 8, 838–844. [Google Scholar] [CrossRef]
- Hafizi, S.; Dahlbäck, B. Gas6 and Protein S: Vitamin K-Dependent Ligands for the Axl Receptor Tyrosine Kinase Subfamily. FEBS J. 2006, 273, 5231–5244. [Google Scholar] [CrossRef]
- Bellan, M.; Pogliani, G.; Marconi, C.; Minisini, R.; Franzosi, L.; Alciato, F.; Magri, A.; Avanzi, G.C.; Pirisi, M.; Sainaghi, P.P. Gas6 as a putative noninvasive biomarker of hepatic fibrosis. Biomar. Med. 2016, 10, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.; Ma, Z.; Hu, W.; Wang, D.; Gong, B.; Fan, C.; Jiang, S.; Li, T.; Gao, J.; Yang, Y. Molecular insights of Gas6/TAM in cancer development and therapy. Cell Death Dis. 2017, 8, e2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinelli, E.; Martini, G.; Cardone, C.; Troiani, T.; Liguori, G.; Vitagliano, D.; Napolitano, S.; Morgillo, F.; Rinaldi, B.; Melillo, R.M.; et al. AXL is an oncotarget in human colorectal cancer. Oncotarget 2015, 6, 23281–23296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- May, C.D.; Garnett, J.; Ma, X.; Landers, S.M.; Ingram, D.R.; Demicco, E.G.; Al Sannaa, G.A.; Vu, T.; Han, L.; Zhang, Y.; et al. AXL is a potential therapeutic target in dedifferentiated and pleomorphic liposarcomas. BMC Cancer 2015, 15, 901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rankin, E.B.; Giaccia, A.J. The Receptor Tyrosine Kinase AXL in Cancer Progression. Cancers 2016, 8, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, G.; Ma, Z.; Cheng, Y.; Hu, W.; Deng, C.; Jiang, S.; Li, T.; Chen, F.; Yang, Y. Targeting Gas6/TAM in Cancer Cells and Tumor Microenvironment. Mol. Cancer 2018, 17, 20. [Google Scholar] [CrossRef] [Green Version]
- Paolino, M.; Penninger, J.M. The Role of TAM Family Receptors in Immune Cell Function: Implications for Cancer Therapy. Cancers 2016, 8, 97. [Google Scholar] [CrossRef] [Green Version]
- Pagani, S.; Bellan, M.; Mauro, D.; Castello, L.M.; Avanzi, G.C.; Lewis, M.J.; Sainaghi, P.P.; Pitzalis, C.; Nerviani, A. New Insights into the Role of Tyro3, Axl, and Mer Receptors in Rheumatoid Arthritis. Dis. Markers 2020, 2020, 1614627. [Google Scholar] [CrossRef] [Green Version]
- Gavelli, F.; Molinari, L.; Baldrighi, M.; Salmi, L.; Mearelli, F.; Fiotti, N.; Patrucco, F.; Airoldi, C.; Bellan, M.; Sainaghi, P.P.; et al. Are Baseline Levels of Gas6 and Soluble Mer Predictors of Mortality and Organ Damage in Patients with Sepsis? The Need-Speed Trial Database. Biomedicines 2022, 10, 198. [Google Scholar] [CrossRef]
- Sainaghi, P.P.; Bellan, M.; Lombino, F.; Alciato, F.; Carecchio, M.; Galimberti, D.; Fenoglio, C.; Scarpini, E.; Cantello, R.; Pirisi, M.; et al. Growth Arrest Specific 6 Concentration is Increased in the Cerebrospinal Fluid of Patients with Alzheimer’s Disease. J. Alzheimer’s Dis. 2016, 55, 59–65. [Google Scholar] [CrossRef]
- Smirne, C.; Rigamonti, C.; de Benedittis, C.; Sainaghi, P.P.; Bellan, M.; Burlone, M.E.; Castello, L.M.; Avanzi, G.C. Gas6/TAM Signaling Components as Novel Biomarkers of Liver Fibrosis. Dis. Mark. 2019, 2019, 2304931. [Google Scholar] [CrossRef] [PubMed]
- Cohen, P.L.; Shao, W.H.; Sainaghi, P.P. Gas6/TAM Receptors in Systemic Lupus Erythematosus. Dis. Mark. 2019, 2019, 7838195. [Google Scholar] [CrossRef] [Green Version]
- Salmi, L.; Gavelli, F.; Patrucco, F.; Bellan, M.; Sainaghi, P.P.; Avanzi, G.C.; Castello, L.M. Growth Arrest-Specific Gene 6 Administration Ameliorates Sepsis-Induced Organ Damage in Mice and Reduces ROS Formation In Vitro. Cells 2021, 10, 602. [Google Scholar] [CrossRef] [PubMed]
- Sainaghi, P.P.; Collimedaglia, L.; Alciato, F.; Molinari, R.; Sola, D.; Ranza, E.; Naldi, P.; Monaco, F.; Leone, M.; Pirisi, M.; et al. Growth Arrest Specific Gene 6 Protein Concentration in Cerebrospinal Fluid Correlates with Relapse Severity in Multiple Sclerosis. Mediat. Inflamm. 2013, 2013, 406483. [Google Scholar] [CrossRef] [Green Version]
- Tonello, S.; Rizzi, M.; Matino, E.; Costanzo, M.; Casciaro, G.F.; Croce, A.; Rizzi, E.; Zecca, E.; Pedrinelli, A.; Vassia, V.; et al. Baseline Plasma Gas6 Protein Elevation Predicts Adverse Outcomes in Hospitalized COVID-19 Patients. Dis. Mark. 2022, 2022, 1568352. [Google Scholar] [CrossRef]
- Morales, A.; Rello, S.R.; Cristóbal, H.; Fiz-López, A.; Arribas, E.; Marí, M.; Tutusaus, A.; de la Cal-Sabater, P.; Nicolaes, G.; Ortiz-Pérez, J.; et al. Growth Arrest-Specific Factor 6 (GAS6) Is Increased in COVID-19 Patients and Predicts Clinical Outcome. Biomedicines 2021, 9, 335. [Google Scholar] [CrossRef] [PubMed]
- Alhiyari, M.A.; Ata, F.; Alghizzawi, M.I.; Bilal, A.B.I.; Abdulhadi, A.S.; Yousaf, Z. Post COVID-19 fibrosis, an emerging complicationof SARS-CoV-2 infection. Idcases 2021, 23, e01041. [Google Scholar] [CrossRef]
- Tutusaus, A.; Marí, M.; Ortiz-Pérez, J.T.; Nicolaes, G.A.F.; Morales, A.; García de Frutos, P. Role of Vitamin K-Dependent Factors Protein S and GAS6 and TAM Receptors in SARS-CoV-2 Infection and COVID-19-Associated Immunothrombosis. Cells 2020, 9, 2186. [Google Scholar] [CrossRef] [PubMed]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 16144. [Google Scholar] [CrossRef]
- Olds, H.; Liu, J.; Luk, K.; Lim, H.W.; Ozog, D.; Rambhatla, P.V. Telogen effluvium associated with COVID-19 infection. Dermatol. Ther. 2021, 34, e14761. [Google Scholar] [CrossRef]
- Quist, S.R.; Quist, J. Keep quiet—How stress regulates hair follicle stem cells. Signal Transduct. Target. Ther. 2021, 6, 364. [Google Scholar] [CrossRef]
- Yi, R. Relax to grow more hair. Nature 2021, 592, 356–357. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Zhang, B.; Ma, S.; Gonzalez-Celeiro, M.; Stein, D.; Jin, X.; Kim, S.T.; Kang, Y.-L.; Besnard, A.; Rezza, A.; et al. Corticosterone inhibits GAS6 to govern hair follicle stem-cell quiescence. Nature 2021, 592, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.; Tosti, A. Alopecia in patients with COVID-19: A systematic review and meta-analysis. JAAD Int. 2022, 7, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.E.; Jafferany, M. Association between alopecia areata and COVID-19: A systematic review. JAAD Int. 2022, 7, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Schultheiß, C.; Willscher, E.; Paschold, L.; Gottschick, C.; Klee, B.; Henkes, S.-S.; Bosurgi, L.; Dutzmann, J.; Sedding, D.; Frese, T.; et al. The IL-1β, IL-6, and TNF cytokine triad is associated with post-acute sequelae of COVID-19. Cell Rep. Med. 2022, 3, 100663. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of COVID-19—Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Class of Severity | Frequency (%) |
|---|---|
| 3 | 40 (15.2) |
| 4 | 5 (1.9) |
| 5 | 86 (32.7) |
| 6 | 115 (43.7) |
| 7 | 17 (6.5) |
| Predictors | Coefficient | p-Value | OR (95%CI) |
|---|---|---|---|
| Sex (female) | 0.91 | 0.001 | 2.49 (1.45–4.28) |
| DLCO, % | −0.02 | 0.007 | 0.98 (0.96–0.99) |
| sAxl (ng/mL) | −0.006 | 0.24 | 0.99 (0.98–1.0) |
| Variables | No Hair Loss (n = 194) | Hair Loss (n = 69) | p-Value | |
|---|---|---|---|---|
| CIRS | 2.0 (1–4) | 2.0 (1–3) | 0.10 | |
| DLCO, % | 82.0 (70–93) | 76.0 (68–85) | 0.017 | |
| Age, years | 59 (51–68) | 61 (50–70) | 0.38 | |
| Gas6 (ng/mL) | 29.39 (24.2–36.8) | 26.01 (20.3–30.9) | 0.0012 | |
| sAxl (ng/mL) | 66.5 (55.6–79.1) | 57.3 (51.6–68.1) | 0.0011 | |
| sMer (ng/mL) | 8,49 (7.09–10.18) | 9.43 (7.61–10.49) | 0.12 | |
| Sex (male/female) | 141 (72.7)/53 (27.3) | 21 (30.4)/48 (69.6) | 0.0001 | |
| Class of severity | 3 | 29 (15) | 11 (15.9) | 0.78 |
| 4 | 4 (2) | 1 (1.5) | ||
| 5 | 62 (32) | 24 (34.8) | ||
| 6 | 91 (46.9) | 24 (34.8) | ||
| 7 | 8 (4.1) | 9 (13) | ||
| Predictors | Coefficient | p-Value | OR (95%CI) |
|---|---|---|---|
| Sex (female) | 1.88 | 0.0001 | 6.58 (3.39–12.78) |
| DLCO, % | −0.01 | 0.35 | 0.99 (0.97–1.01) |
| Gas6 (ng/mL) | −0.04 | 0.015 | 0.96 (0.92–0.99) |
| sAxl (ng/mL) | −0.02 | 0.014 | 0.98 (0.97–1.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Apostolo, D.; D’Onghia, D.; Tonello, S.; Minisini, R.; Baricich, A.; Gramaglia, C.; Patrucco, F.; Zeppegno, P.; Acquaviva, A.; Balbo, P.E.; et al. Decreased Gas6 and sAxl Plasma Levels Are Associated with Hair Loss in COVID-19 Survivors. Int. J. Mol. Sci. 2023, 24, 6257. https://doi.org/10.3390/ijms24076257
Apostolo D, D’Onghia D, Tonello S, Minisini R, Baricich A, Gramaglia C, Patrucco F, Zeppegno P, Acquaviva A, Balbo PE, et al. Decreased Gas6 and sAxl Plasma Levels Are Associated with Hair Loss in COVID-19 Survivors. International Journal of Molecular Sciences. 2023; 24(7):6257. https://doi.org/10.3390/ijms24076257
Chicago/Turabian StyleApostolo, Daria, Davide D’Onghia, Stelvio Tonello, Rosalba Minisini, Alessio Baricich, Carla Gramaglia, Filippo Patrucco, Patrizia Zeppegno, Antonio Acquaviva, Piero Emilio Balbo, and et al. 2023. "Decreased Gas6 and sAxl Plasma Levels Are Associated with Hair Loss in COVID-19 Survivors" International Journal of Molecular Sciences 24, no. 7: 6257. https://doi.org/10.3390/ijms24076257