
The APSANTICO Study: A Prospective Observational Study to Evaluate Antiphospholipid Antibody Profiles in Patients with Thromboembolic Antiphospholipid Syndrome (APS) after COVID-19 Infection and/or Vaccination


Abstract
:1. Introduction
2. Results
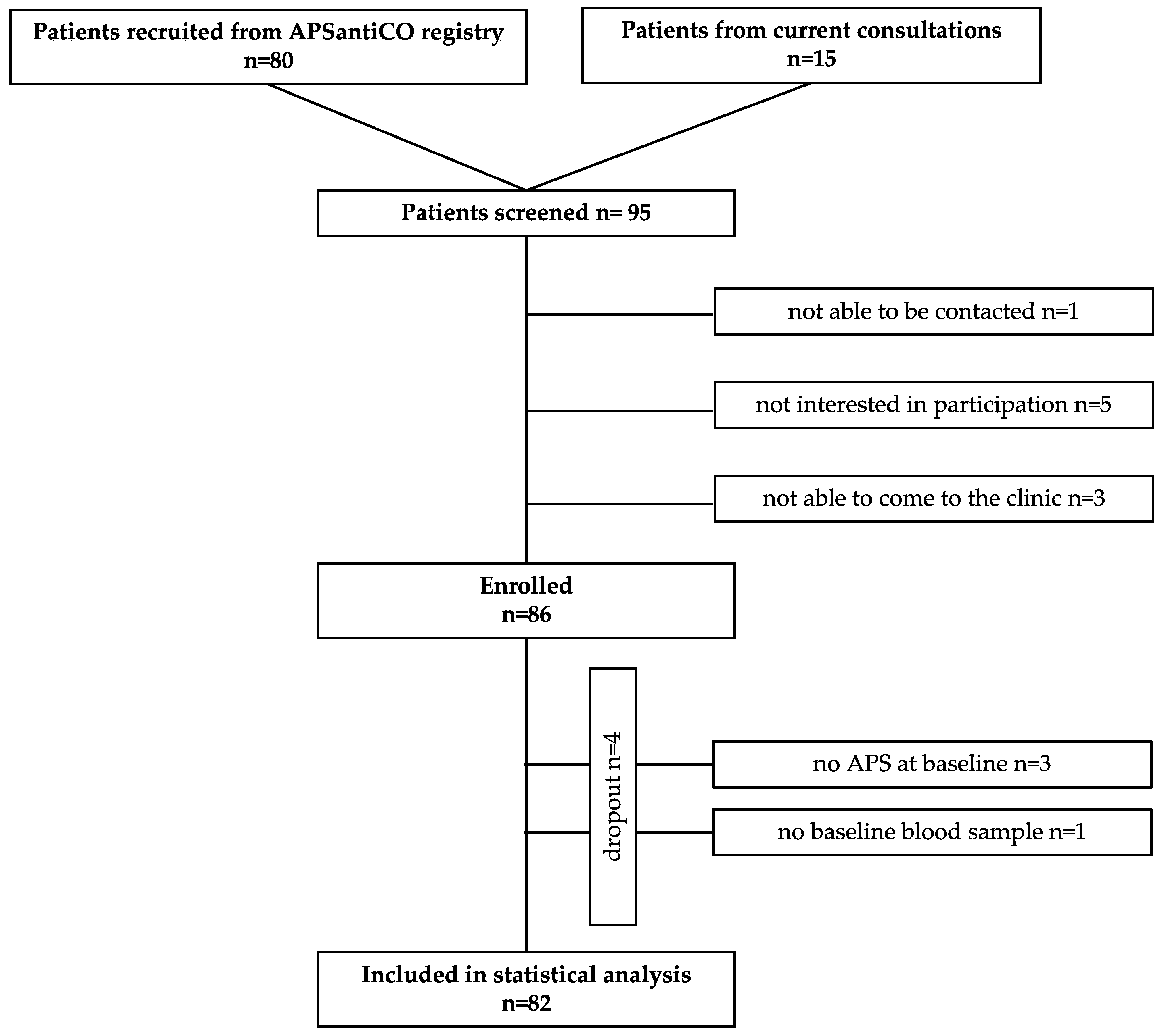
2.1. Patient Characteristics
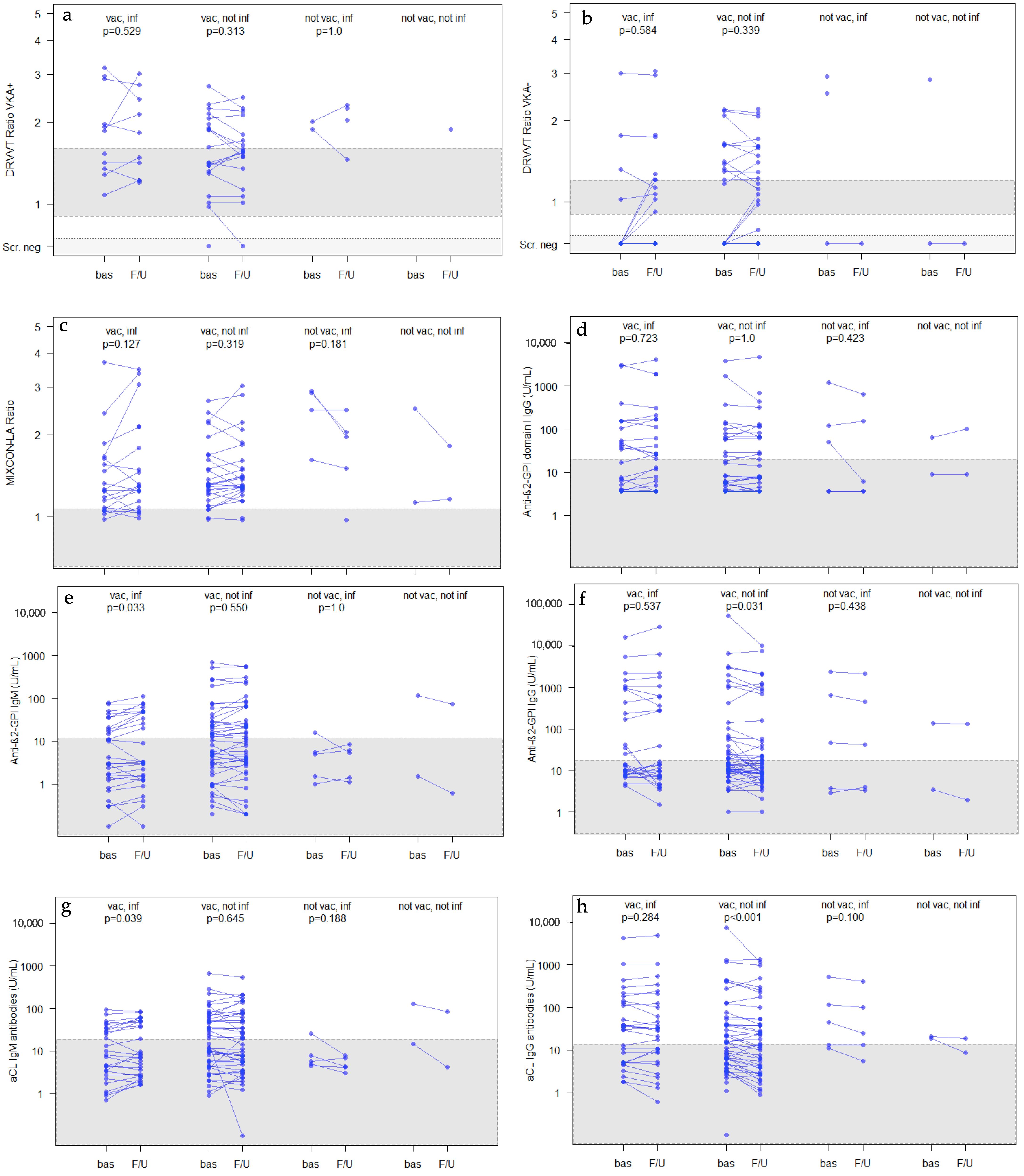
2.2. Antiphospholipid-Antibodies and Platelet Counts at Baseline and at Follow-Up (after COVID-19 Infection and/or Vaccination)
2.3. Hospital Admissions Due to COVID-19 Infection or COVID-19 Vaccination
2.3.1. Hospital Admissions Due to COVID-19 Infection (see Table 5)
2.3.2. Hospital Admissions Due to COVID-19 Vaccination (see Table 5)
2.4. INR Variations Due to COVID-19 Infection or COVID-19 Vaccination
3. Discussion
3.1. aPL and COVID-19 Vaccination/Infection
3.2. Thrombocytopenia and COVID-19 Vaccination/Infection
3.3. The Immune System and COVID-19 Vaccination/Infection
3.4. COVID-19 Infections and COVID-19 Vaccinations and Their Association with Thromboembolic Complications
3.5. Strengths and Limitations
3.5.1. Strengths of the Study
3.5.2. Limitations of the Study
4. Materials and Methods
- Minimum age of 18 years;
- Presence of any APS antibody risk profile (single-/double-/triple-positivity);
- Arterial and/or venous thromboembolism in their medical history.
Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Linnemann, B. Antiphospholipid syndrome-an update. Vasa 2018, 47, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Miyakis, S.; Lockshin, M.D.; Atsumi, T.; Branch, D.W.; Brey, R.L.; Cervera, R.; Derksen, R.H.; PG, D.E.G.; Koike, T.; Meroni, P.L.; et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J. Thromb. Haemost. 2006, 4, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gkrouzman, E.; Andrade, D.C.O.; Andreoli, L.; Barbhaiya, M.; Belmont, H.M.; Branch, D.W.; de Jesus, G.R.; Efthymiou, M.; Rios-Garces, R.; et al. COVID-19 and antiphospholipid antibodies: A position statement and management guidance from AntiPhospholipid Syndrome Alliance for Clinical Trials and InternatiOnal Networking (APS ACTION). Lupus 2021, 30, 2276–2285. [Google Scholar] [CrossRef] [PubMed]
- Paul-Ehrlich-Institut. COVID-19-Impfstoffe. Available online: https://www.pei.de/DE/arzneimittel/impfstoffe/covid-19/covid-19-node.html (accessed on 17 January 2023).
- Gendron, N.; Dragon-Durey, M.A.; Chocron, R.; Darnige, L.; Jourdi, G.; Philippe, A.; Chenevier-Gobeaux, C.; Hadjadj, J.; Duchemin, J.; Khider, L.; et al. Lupus Anticoagulant Single Positivity During the Acute Phase of COVID-19 Is Not Associated With Venous Thromboembolism or In-Hospital Mortality. Arthritis Rheumatol. 2021, 73, 1976–1985. [Google Scholar] [CrossRef] [PubMed]
- Uthman, I.W.; Gharavi, A.E. Viral infections and antiphospholipid antibodies. Semin Arthritis Rheum 2002, 31, 256–263. [Google Scholar] [CrossRef]
- Devreese, K.M.J.; Linskens, E.A.; Benoit, D.; Peperstraete, H. Antiphospholipid antibodies in patients with COVID-19: A relevant observation? J. Thromb. Haemost. 2020, 18, 2191–2201. [Google Scholar] [CrossRef]
- Galeano-Valle, F.; Oblitas, C.M.; Ferreiro-Mazon, M.M.; Alonso-Munoz, J.; Del Toro-Cervera, J.; di Natale, M.; Demelo-Rodriguez, P. Antiphospholipid antibodies are not elevated in patients with severe COVID-19 pneumonia and venous thromboembolism. Thromb. Res. 2020, 192, 113–115. [Google Scholar] [CrossRef]
- Borghi, M.O.; Beltagy, A.; Garrafa, E.; Curreli, D.; Cecchini, G.; Bodio, C.; Grossi, C.; Blengino, S.; Tincani, A.; Franceschini, F.; et al. Anti-Phospholipid Antibodies in COVID-19 Are Different From Those Detectable in the Anti-Phospholipid Syndrome. Front. Immunol. 2020, 11, 584241. [Google Scholar] [CrossRef]
- Espinosa, G.; Zamora-Martinez, C.; Perez-Isidro, A.; Neto, D.; Bravo-Gallego, L.Y.; Prieto-Gonzalez, S.; Vinas, O.; Moreno-Castano, A.B.; Ruiz-Ortiz, E.; Cervera, R. Persistent Antiphospholipid Antibodies Are Not Associated With Worse Clinical Outcomes in a Prospective Cohort of Hospitalised Patients With SARS-CoV-2 Infection. Front. Immunol. 2022, 13, 911979. [Google Scholar] [CrossRef]
- Zuo, Y.; Estes, S.K.; Ali, R.A.; Gandhi, A.A.; Yalavarthi, S.; Shi, H.; Sule, G.; Gockman, K.; Madison, J.A.; Zuo, M.; et al. Prothrombotic autoantibodies in serum from patients hospitalized with COVID-19. Sci. Transl. Med. 2020, 12, eabd3876. [Google Scholar] [CrossRef]
- Gan, G.; Liu, H.; Liang, Z.; Zhang, G.; Liu, X.; Ma, L. Vaccine-associated thrombocytopenia. Thromb. Res. 2022, 220, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H. Thrombosis and thrombocytopenia in COVID-19 and after COVID-19 vaccination. Trends Cardiovasc. Med. 2022, 32, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Pontara, E.; Banzato, A.; Bison, E.; Cattini, M.G.; Baroni, G.; Denas, G.; Calligaro, A.; Marson, P.; Tison, T.; Ruffatti, A.; et al. Thrombocytopenia in high-risk patients with antiphospholipid syndrome. J. Thromb. Haemost. 2018, 16, 529–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaefers, C.; Paulsen, F.O.; Frenzel, C.; Weisel, K.; Bokemeyer, C.; Seidel, C. Increased incidence of immune thrombocytopenia (ITP) in 2021 correlating with the ongoing vaccination campaign against COVID-19 in a tertiary center-A monocentric analysis. Br. J. Haematol. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infections: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef]
- Yang, M.; Ng, M.H.; Li, C.K. Thrombocytopenia in patients with severe acute respiratory syndrome (review). Hematology 2005, 10, 101–105. [Google Scholar] [CrossRef] [Green Version]
- Franchini, M.; Veneri, D.; Lippi, G. Thrombocytopenia and infections. Expert Rev. Hematol. 2017, 10, 99–106. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.M.; Shuai, Z.W.; Ye, D.Q.; Pan, H.F. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef]
- Yazdanpanah, N.; Rezaei, N. Autoimmune complications of COVID-19. J. Med. Virol. 2022, 94, 54–62. [Google Scholar] [CrossRef]
- Pascolini, S.; Vannini, A.; Deleonardi, G.; Ciordinik, M.; Sensoli, A.; Carletti, I.; Veronesi, L.; Ricci, C.; Pronesti, A.; Mazzanti, L.; et al. COVID-19 and Immunological Dysregulation: Can Autoantibodies be Useful? Clin. Transl. Sci. 2021, 14, 502–508. [Google Scholar] [CrossRef]
- Gomez-Puerta, J.A.; Martin, H.; Amigo, M.C.; Aguirre, M.A.; Camps, M.T.; Cuadrado, M.J.; Hughes, G.R.V.; Khamashta, M.A. Long-term follow-up in 128 patients with primary antiphospholipid syndrome: Do they develop lupus? Medicine (Baltimore) 2005, 84, 225–230. [Google Scholar] [CrossRef]
- Zou, Y.; Guo, H.; Zhang, Y.; Zhang, Z.; Liu, Y.; Wang, J.; Lu, H.; Qian, Z. Analysis of coagulation parameters in patients with COVID-19 in Shanghai, China. Biosci. Trends 2020, 14, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Fiolet, T.; Kherabi, Y.; MacDonald, C.J.; Ghosn, J.; Peiffer-Smadja, N. Comparing COVID-19 vaccines for their characteristics, efficacy and effectiveness against SARS-CoV-2 and variants of concern: A narrative review. Clin. Microbiol. Infect. 2022, 28, 202–221. [Google Scholar] [CrossRef] [PubMed]
- Agency, U.H.S. COVID-19 Vaccine Surveillance Report Week 44. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1115385/Vaccine_surveillance_report___week-44.pdf (accessed on 17 January 2023).
- Statista. Verteilung Besorgniserregender Coronavirusvarianten (VOC) in Deutschland 2021. Available online: https://de.statista.com/statistik/daten/studie/1208627/umfrage/ausbreitung-von-corona-mutationen-in-deutschland/ (accessed on 17 January 2023).
- Robert Koch Institut. SARS-CoV-2: Virologische Basisdaten Sowie Virusvarianten. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Virologische_Basisdaten.html;jsessionid=CBB1C1C394B7CDCE980B01F79385A939.internet062?nn=13490888#doc14716546bodyText8 (accessed on 17 January 2023).
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emerg. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef]
- Schulz, A.; Herrmann, E.; Ott, O.; Lindhoff-Last, E. Thromboembolic Antiphospholipid Syndrome (APS): Efficacy and Safety of Different Anticoagulants-Results of the APSantiCO Registry. J. Clin. Med. 2022, 11, 4845. [Google Scholar] [CrossRef]
- Institut, R.K. Gesamtübersicht der pro Tag ans RKI Übermittelten Fälle und Todesfälle. Available online: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Fallzahlen_Gesamtuebersicht.html (accessed on 17 January 2023).
- Kaatz, S.; Ahmad, D.; Spyropoulos, A.C.; Schulman, S.; For the Subcommittee on Control of Anticoagulation. Definition of clinically relevant non-major bleeding in studies of anticoagulants in atrial fibrillation and venous thromboembolic disease in non-surgical patients: Communication from the SSC of the ISTH. J. Thromb. Haemost. 2015, 13, 2119–2126. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Study Population (n = 82) | COVID-19 vac. only (n = 47/82) | COVID-19 vac. and inf. * (n = 28/82) | COVID-19 inf. only (n = 5/82) | Neither COVID-19 inf. nor vac. (n = 2/82) | |
|---|---|---|---|---|---|
| Number of patients (n) | 82 | 47 | 28 | 5 | 2 |
| Female, % (counts/n) | 53.7 (44/82) | 40.4 (19/45) | 75.0 (21/28) | 60.0 (3/5) | 50.0 (1/2) |
| Age (years) median (25–75% percentiles) | 52 (39.5–62.8) | 57 (48.5–69.0) | 43 (32.8–54.0) | 52 (39.0–53.0) | 26 (26.0–26.0) |
| BMI (kg/m2) median (25–75% percentiles) | 26.3 (24.1–30.1) | 26.2 (24.7–29.3) | 27.3 (21.9–30.6) | 25.5 (24.2–28) | 26.6 (23.9–29.3) |
| Cardiovascular risk factors % (counts/n) | 74.4 (61/82) | 85.1 (40/47) | 60.7 (17/28) | 80.0 (4/5) | 0 (0/2) |
| None % (counts/n) | 25.6 (21/82) | 14.9 (7/47) | 39.3 (11/28) | 20.0 (1/5) | 100 (2/2) |
| Hypertension % (counts/n) | 53.7 (44/82) | 70.2 (33/47) | 32.1 (9/28) | 40.0 (2/5) | 0 (0/2) |
| Diabetes % (counts/n) | 8.5 (7/82) | 10.6 (5/47) | 7.1 (2/28) | 0 (0/5) | 0 (0/2) |
| Smoking % (counts/n) | 8.5 (7/82) | 10.6 (5/47) | 7.1 (2/28) | 0 (0/5) | 0 (0/2) |
| Hypercholesterolaemia % (counts/n) | 48.8 (40/82) | 59.6 (28/47) | 35.7 (10/28) | 20.0 (2/5) | 0 (0/2) |
| elevated Lipoprotein a % (counts/n) | 11.0 (9/82) | 10.6 (5/47) | 14.3 (4/28) | 0 (0/5) | 0 (0/2) |
| Atrial fibrillation % (counts/n) | 6.1 (5/82) | 8.5 (4/47) | 3.6 (1/28) | 0 (0/5) | 0 (0/2) |
| Primary APS % (counts/n) | 76.8 (63/82) | 85.1 (40/47) | 67.9 (19/28) | 20.0 (2/5) | 100 (2/2) |
| Female % (counts/n) | 50.8 (32/63) | 40.0 (16/40) | 73.7 (14/19) | 50.0 (1/2) | 50.0 (1/2) |
| Secondary APS % (counts/n) | 23.2 (19/82) | 14.9 (7/47) | 32.1 (9/28) | 60.0 (3/5) | 0 (0/2) |
| Female % (counts/n) | 63.2 (12/19) | 42.9 (3/7) | 77.8 (7/9) | 66.7 (2/3) | 0 (0/0) |
| Autoimmune disease ** % (counts/n) | 35.4 (29/82) | 25.5 (12/47) | 46.4 (13/28) | 60.0 (3/5) | 50.0 (1/2) |
| Female % (counts/n) | 69.0 (20/29) | 50.0 (6/12) | 84.6 (11/13) | 66.7 (2/3) | 100 (1/1) |
| SLE % (counts/n) | 13.4 (11/82) | 6.4 (3/47) | 17.9 (5/28) | 60.0 (3/5) | 0 (0/2) |
| Female % (counts/n) | 72.7 (8/11) | 33.3 (1/3) | 100.0 (5/5) | 66.7 (2/3) | 0 (0/0) |
| Immunosuppressive drugs | 20.7 (17/82) | 12.8 (6/47) | 28.6 (8/28) | 60.0 (3/5) | 0 (0/2) |
| VTE in medical history % (counts/n) | 79.3 (65/82) | 68.1 (32/47) | 92.8 (26/28) | 100 (5/5) | 100 (2/2) |
| ATE in medical history % (counts/n) | 39.0 (32/82) | 51.1 (24/47) | 21.4 (6/28) | 20.0 (2/5) | 0 (0/2) |
| Antiphospholipid antibodies | |||||
| Lupus anticoagulants % (counts/n) | 58.5 (48/82) | 57.4 (27/47) | 53.6 (15/28) | 80.0 (4/5) | 100 (2/2) |
| Elevated Mixcon LA Ratio % (counts/n) | 53.7 (44/82) | 51.1 (24/47) | 50.0 (14/28) | 80.0 (4/5) | 100 (2/2) |
| Elevated DRVVT Ratio % (counts/n) | 42.7 (35/82) | 44.7 (21/47) | 32.1 (9/28) | 80.0 (4/5) | 50 (1/2) |
| Elevated aCL % (counts/n) | 80.5 (66/82) | 80.9 (38/47) | 82.1 (23/28) | 60.0 (3/5) | 100 (2/2) |
| Elevated aCL IgM % (counts/n) | 43.9 (36/82) | 48.9 (23/47) | 39.3 (11/28) | 20.0 (1/5) | 50 (1/2) |
| Elevated aCL IgG % (counts/n) | 54.9 (45/82) | 51.1 (24/47) | 57.1 (16/28) | 60.0 (3/5) | 100 (2/2) |
| Elevated anti-2-GPI % (counts/n) | 69.5 (57/82) | 70.2 (33/47) | 71.4 (20/28) | 60.0 (3/5) | 50 (1/2) |
| Elevated anti-2-GPI IgM % (counts/n) | 41.5 (34/82) | 46.8 (22/47) | 35.7 (10/28) | 20.0 (1/5) | 50 (1/2) |
| Elevated anti-2-GPI IgG % (counts/n) | 46.3 (38/82) | 44.7 (21/47) | 46.4 (13/28) | 60.0 (3/5) | 50 (1/2) |
| Elevated anti-2-GPI domain I IgG % (counts/n) | 34.2 (28/82) | 25.5 (12/47) | 42.9 (12/28) | 60.0 (3/5) | 50 (1/2) |
| aPL status | |||||
| Single-positive % (counts/n) | 37.8 (31/82) | 38.3 (18/47) | 35.7 (10/28) | 20.0 (2/5) | 50 (1/2) |
| Double-positive % (counts/n) | 23.2 (19/82) | 23.4 (11/47) | 25.0 (7/28) | 20.0 (1/5) | 0 (0/2) |
| Triple-positive % (counts/n) | 39.0 (32/82) | 38.3 (18/47) | 39.3 (11/28) | 20.0 (2/5) | 50 (1/2) |
| Medication | Baseline | Follow-Up |
|---|---|---|
| VKA only % (counts/n) | 34.1 (28/82) | 34.1 (28/82) |
| DOAC only % (counts/n) | 32.9 (27/82) | 32.9 (27/82) |
| LMWH only % (counts/n) | 8.5 (7/82) | 6.1 (5/82) |
| Fondaparinux only % (counts/n) | 1.2 (1/82) | 2.4 (2/82) |
| PI only % (counts/n) | 7.3 (6/82) | 7.3 (6/82) |
| VKA + PI % (counts/n) | 7.3 (6/82) | 7.3 (6/82) |
| DOAC + PI % (counts/n) | 4.9 (4/82) | 6.1 (5/82) |
| LMWH + PI % (counts/n) | 2.4 (2/82) | 1.2 (1/82) |
| none | 1.2 (1/82) | 2.4 (2/82) |
| Total Study Population (n = 82) | COVID-19 vac. only (n = 47/82) | COVID-19 vac. and inf. ** (n = 28/82) | COVID-19 inf. only (n = 5/82) | Neither COVID-19 inf. nor vac. (n = 2/82) | |
|---|---|---|---|---|---|
| Time between baseline and Follow-up blood sampling (days) median (25–75% percentiles) | 617 (486.5–783) | 624 (518.5–814.5) | 634 (494.8–747.8) | 329 (253–334) | 306 (241.3–369.8) |
| Time between baseline blood sampling and first COVID-19 vac. or inf. (days) median (25–75% percentiles) | 200 (102.5–354.0) | 218 (116–402) | 194 (55.8–351.5) | 93 (72.3–113.5) | 305.5 ### (n.a.) |
| Time between last COVID-19 vac. or inf. and Follow-up blood sampling (days) median (25–75% percentiles) | 142 (88.5–199) | 155 (114–208.5) | 120 (56.3–159.8) | 169 (155.3–205.5) | 305.5 ### (n.a.) |
| ≥1 COVID-19 vac. % (counts/n) | 91.5 (75/82) | 100 (47/47) | 100 (28/28) | n.a. | n.a. |
| Hospitalization after COVID-19 vac. % (counts/n) | 5.3 (4/75) | 8.5 (4/47) | 0 (0/28) | n.a. | n.a. |
| ≥1 SARS-CoV-2 inf. * % (counts/n) | 40.2 (33/82) | n.a. | 100 (28/28) | 100 (5/5) | n.a. |
| Hospitalization after COVID-19 inf. % (counts/n) | 9.1 (3/33) | n.a. | 7.1 (2/28) | 20 (1/5) | n.a. |
| of whom % were not vaccinated (counts/n) | 33.3 (1/3) | n.a. | n.a. | 100 (1/1) | n.a. |
| Infection in 2020 % (counts/n) | 2.9 (1/35 #) | n.a. | 3.3 (1/30 ##) | 0 (0/5) | n.a. |
| Infection in 2021 % (counts/n) | 22.9 (8/35 #) | n.a. | 20.0 (6/30 ##) | 40 (2/5) | n.a. |
| Infection in 2022 % (counts/n) | 74.3 (26/35 #) | n.a. | 76.7 (23/30 ##) | 60 (3/5) | n.a. |
| COVID-19 inf. on immunosuppressive drugs % (counts/n) | 27.3 (9/33) | n.a. | 21.4 (6/28) | 60 (3/5) | n.a. |
| Immunosuppressive drugs | 18.3 (15/82) | 12.8 (6/47) | 21.4 (6/28) | 60.0 (3/5) | 0 (0/2) |
| of whom % (counts/n) were infected with COVID-19 | 60.0 (9/15) | n.a. | 100 (6/6) | 100 (3/3) | n.a. |
| VTE during observation % (counts/n) | 0.0 (0/82) | 0.0 (0/47) | 0.0 (0/28) | 0 (0/5) | 0 (0/2) |
| ATE during observation % (counts/n) | 1.2 (1/82) | 2.1 (1/47) | 0.0 (0/28) | 0 (0/5) | 0 (0/2) |
| Major bleeding during observation % (counts/n) | 1.2 (1/82) | 2.1 (1/47) | 0.0 (0/28) | 0 (0/5) | 0 (0/2) |
| Antiphospholipid antibodies | |||||
| Lupus anticoagulants % (counts/n) | 61 (50/82) | 57.4 (27/47) | 60.7 (17/28) | 80 (4/5) | 100 (2/2) |
| Elevated Mixcon LA Ratio % (counts/n) | 57.3 (47/82) | 53.2 (25/47) | 57.1 (16/28) | 80 (4/5) | 100 (2/2) |
| Elevated DRVVT Ratio % (counts/n) | 42.7 (35/82) | 38.3 (18/47) | 46.4 (13/28) | 60 (3/5) | 50 (1/2) |
| Elevated aCL % (counts/n) | 81.7 (67/82) | 80.9 (38/47) | 89.3 (25/28) | 60 (3/5) | 50 (1/2) |
| Elevated aCL IgM % (counts/n) | 42.7 (35/82) | 48.9 23/47) | 39.3 (11/28) | 0 (0/5) | 50 (1/2) |
| Elevated aCL IgG %(counts/n) | 51.2 (42/82) | 44.7 (21/47) | 60.7 (17/28) | 60 (3/5) | 50 (1/2) |
| Elevated anti-2-GPI % (counts/n) | 63.4 (52/82) | 61.7 (29/47) | 67.9 (19/28) | 60 (3/5) | 50 (1/2) |
| Elevated anti-2-GPI IgM % (counts/n) | 40.2 (33/82) | 44.7 (21/47) | 39.3 (11/28) | 0 (0/5) | 50 (1/2) |
| Elevated anti-2-GPI IgG % (counts/n) | 41.5 (34/82) | 40.4 (19/47) | 39.3 (11/28) | 60 (3/5) | 50 (1/2) |
| Elevated anti-2-GPI domain I IgG % (counts/n) | 37.8 (31/82) | 29.8 (14/47) | 50.0 (14/28) | 40 (2/5) | 50 (1/2) |
| aPL status | |||||
| Single-positive % (counts/n) | 36.6 (30/82) | 38.3 (18/47) | 32.1 (9/28) | 40 (2/5) | 50 (1/2) |
| Double-positive % (counts/n) | 18.3 (15/82) | 17.0 (8/47) | 21.4 (6/28) | 20 (1/5) | 0 (0/2) |
| Triple-positive % (counts/n) | 40.2 (33/82) | 38.3 (18/47) | 42.9 (12/28) | 40 (2/5) | 50 (1/2) |
| Loss of aPL % (counts/n) | 4.9 (4/82) | 6.4 (3/47) | 3.6 (1/28) | 0 (0/5) | 0 (0/2) |
| Increase + in aPL positivity % (counts/n) | 7.3 (6/82) | 4.3 (2/47) | 14.3 (4/28) | 0 (0/5) | 0 (0/2) |
| Decrease ++ in aPL positivity % (counts/n) | 14.6 (12/82) | 17.0 (8/47) | 14.3 (4/28) | 0 (0/5) | 0 (0/2) |
| Total Study Population | COVID-19 vac. only | COVID-19 vac. and inf. ** | COVID-19 inf. only | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (25–75% Percentiles) | Median (25–75% Percentiles) | Median (25–75% Percentiles) | Median (25–75% Percentiles) | |||||||||
| Baseline | Follow-Up | p | Baseline | Follow-Up | p | Baseline | Follow-Up | p | Baseline | Follow-Up | p | |
| Lupus anticoagulants | ||||||||||||
| DRVVT Ratio VKA+ * (Normal range: 0.9–1.6) | 1.9 (1.4–2.0) | 1.6 (1.4–2.1) | 0.494 | 1.5 (1.3–2.0) | 1.6 (1.4–1.8) | 0.313 | 1.9 (1.4–2.0) | 1.8 (1.4–2.4) | 0.529 | 1.9 (1.9–2.0) | 1.9 (1.7–2.1) | 1.0 |
| DRVVT Ratio VKA- * (Normal range: 0.9–1.2) | 1.6 (1.3–1.9) | 1.6 (1.3–1.7) | 0.135 | 1.5 (1.3–1.8) | 1.5 (1.3–1.6) | 0.339 | 1.8 (1.5–2.4) | 1.7 (1.4–2.3) | 0.584 | n.a. | n.a. | n.a. |
| Mixcon LA Ratio (Normal range 0.8-1.07) | 1.3 (1.2–1.7) | 1.3 (1.2–1.8) | 0.398 | 1.3 (1.2–1.7) | 1.3 (1.3–1.6) | 0.319 | 1.3 (1.1–1.6) | 1.3 (1.1–1.6) | 0.127 | 2.7 (2.3–2.9) | 2.0 (1.8–2.1) | 0.181 |
| anti-2-GPI | ||||||||||||
| anti-ß2-GPI domain I IgG (U/mL) (Normal range: 0–20) | 5.6 (3.6–55.4) | 6.3 (3.6–61.5) | 0.858 | 3.8 (3.6–22.2) | 3.6 (3.6–24.7) | 1.0 | 12.2 (3.7–91.2) | 16.9 (3.6–99.1) | 0.723 | 49.0 (3.6–121.0) | 6.0 (3.6–152.2) | 0.423 |
| anti-2-GPI IgM (U/mL) (Normal range 0–12) | 5.5 (1.5–22.5) | 5.5 (1.4–33.3) | 0.129 | 8.0 (2.2–26.6) | 9.1 (2.3–28.4) | 0.550 | 3.6 (1.4–19.5) | 3.1 (1.3–47.4) | 0.033 | 5.0 (1.5–5.4) | 5.3 (1.4–6.2) | 1.0 |
| anti-2-GPI IgG (U/mL) (Normal range 0–17.4) | 14.6 (8.6–167.3) | 12.5 (6.6–249.3) | 0.021 | 14.9 (9.7–66.3) | 12.0 (7.4–45.0) | 0.031 | 18.3 (8.7–558.3) | 12.5 (6.9–424.4) | 0.537 | 47.1 (3.7–665.7) | 41.9 (4.0–451.4) | 0.438 |
| aCL | ||||||||||||
| aCL IgM (U/mL) (Normal range: 0–18.7) | 10.8 (4.2–43.8) | 8.1 (3.5–51.1) | 0.901 | 14.8 (4.4–55.0) | 14.3 (4.1–56.9) | 0.645 | 7.8 (2.6–30.3) | 7.6 (2.7–48.7) | 0.039 | 5.6 (4.9–7.7) | 4.3 (4.2–6.7) | 0.188 |
| aCL IgG (U/mL) (Normal range: 0–13.6) | 17.3 (5.1–72.4) | 15.8 (4.0–53.7) | <10−3 | 14.8 (4.6–48.0) | 11.1 (2.7–39.0) | <10−3 | 32.8 (5.2–133.3) | 29.5 (7.9–106.8) | 0.284 | 44.4 (13.2–113.7) | 24.7 (13.2–101.0) | 0.100 |
| Platelet count (103/µL) (Normal range 150–400) | 212.5 (174.0–249.0) | 221.5 (176.8–267.3) | 0.608 | 203.5 (174.8–242.0) | 207.0 (170.3–254.8) | 0.645 | 221.0 (177.5–258.5) | 236.0 (209.5–283.5) | 0.546 | 231.0 (145.0–243.0) | 237.0 (182.0–257.0) | 0.313 |
| Patient | Age (Years) | Sex | Hospitalization after vac. or inf. | Time from vac. or inf. to Hospitalization (Days) | Diagnosis/Symptoms Leading to Hospitalization | Duration of Hospitalization (Days) | Outcome |
|---|---|---|---|---|---|---|---|
| Mild Cases | |||||||
| 1 | 77 | female | inf. * | 12 | nausea, vomiting, headache | 5 | fully recovered |
| 2 | 38 | female | inf. * | 11 | esophagitis | 1 | fully recovered |
| 3 | 45 | female | vac. | 37 | spinning vertigo, periods of aphasia, vomiting | 3 | fully recovered |
| 4 | 71 | male | vac. | 2 | acute hearing loss | n.a. | hearing 75% restored after 3 weeks |
| Severe cases | |||||||
| 5 | 60 | female | inf. ** | 1 | acute general distress, later respiratory insufficiency | 51 | stable but impaired general condition |
| 6 | 85 | male | vac. | 5 | arm paresis left side due to paramedian pons infarction | 19 | stable but impaired general condition |
| 7 | 54 | male | vac. | 33 | dysaesthesia right hand and aphasia due to spontaneous subdural hematoma | 19 | symptoms have improved, not fully recovered |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ott, O.; Herrmann, E.; Schulz, A.; Lindhoff-Last, E. The APSANTICO Study: A Prospective Observational Study to Evaluate Antiphospholipid Antibody Profiles in Patients with Thromboembolic Antiphospholipid Syndrome (APS) after COVID-19 Infection and/or Vaccination. Int. J. Mol. Sci. 2023, 24, 5644. https://doi.org/10.3390/ijms24065644
Ott O, Herrmann E, Schulz A, Lindhoff-Last E. The APSANTICO Study: A Prospective Observational Study to Evaluate Antiphospholipid Antibody Profiles in Patients with Thromboembolic Antiphospholipid Syndrome (APS) after COVID-19 Infection and/or Vaccination. International Journal of Molecular Sciences. 2023; 24(6):5644. https://doi.org/10.3390/ijms24065644
Chicago/Turabian StyleOtt, Olivia, Eva Herrmann, Annabel Schulz, and Edelgard Lindhoff-Last. 2023. "The APSANTICO Study: A Prospective Observational Study to Evaluate Antiphospholipid Antibody Profiles in Patients with Thromboembolic Antiphospholipid Syndrome (APS) after COVID-19 Infection and/or Vaccination" International Journal of Molecular Sciences 24, no. 6: 5644. https://doi.org/10.3390/ijms24065644