
A Histologic, Histomorphometric, and Immunohistochemical Evaluation of Anorganic Bovine Bone and Injectable Biphasic Calcium Phosphate in Humans: A Randomized Clinical Trial

 ,
, 
 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Demographic Data
2.2. Quantitative Analysis of the Histological Bone Biopsy Samples
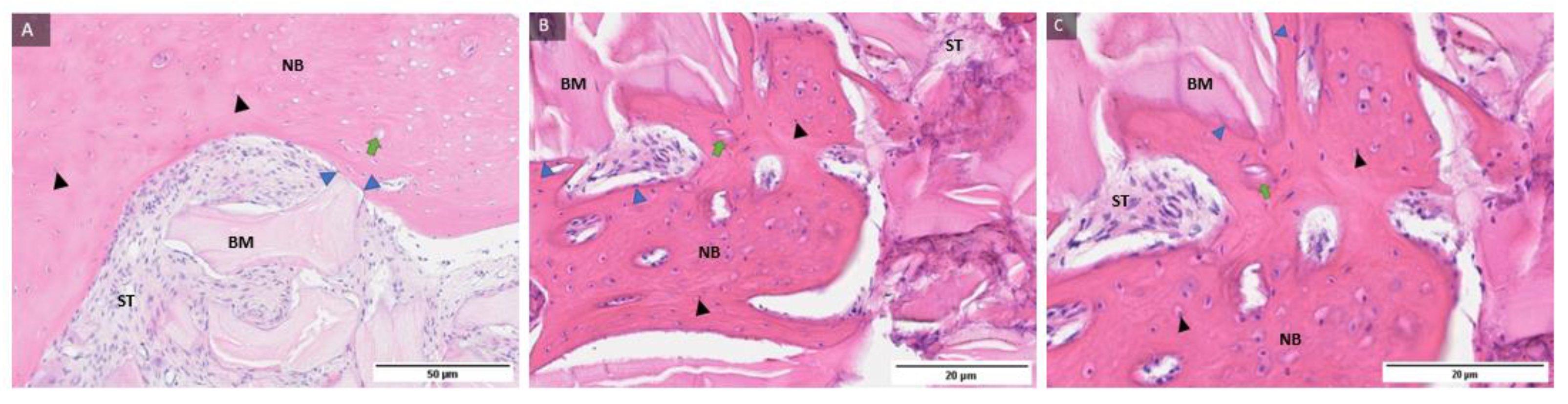
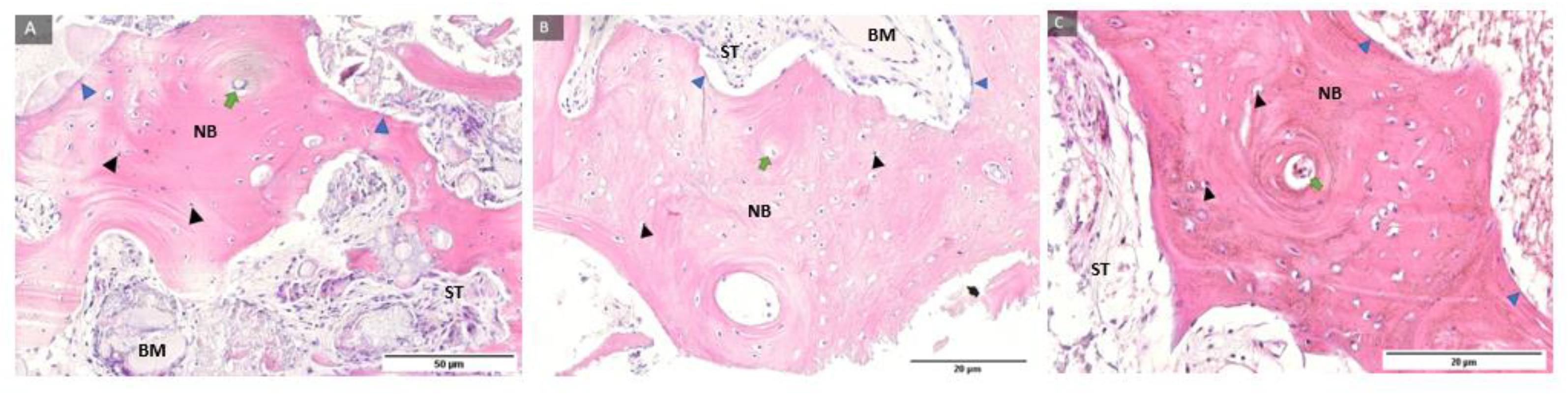
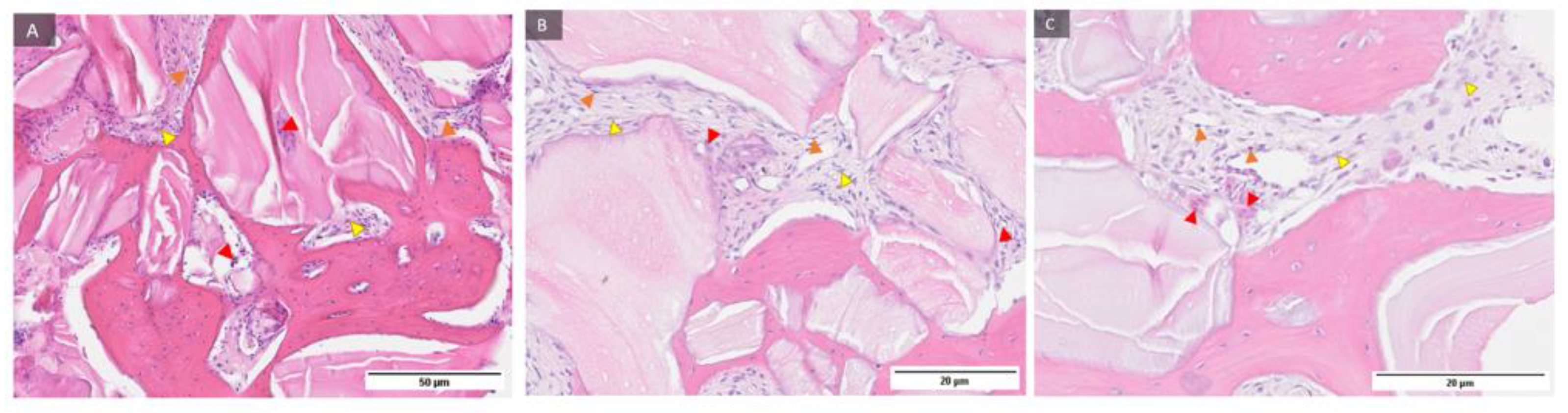
2.3. Qualitative Histological Analysis
HE histological Staining
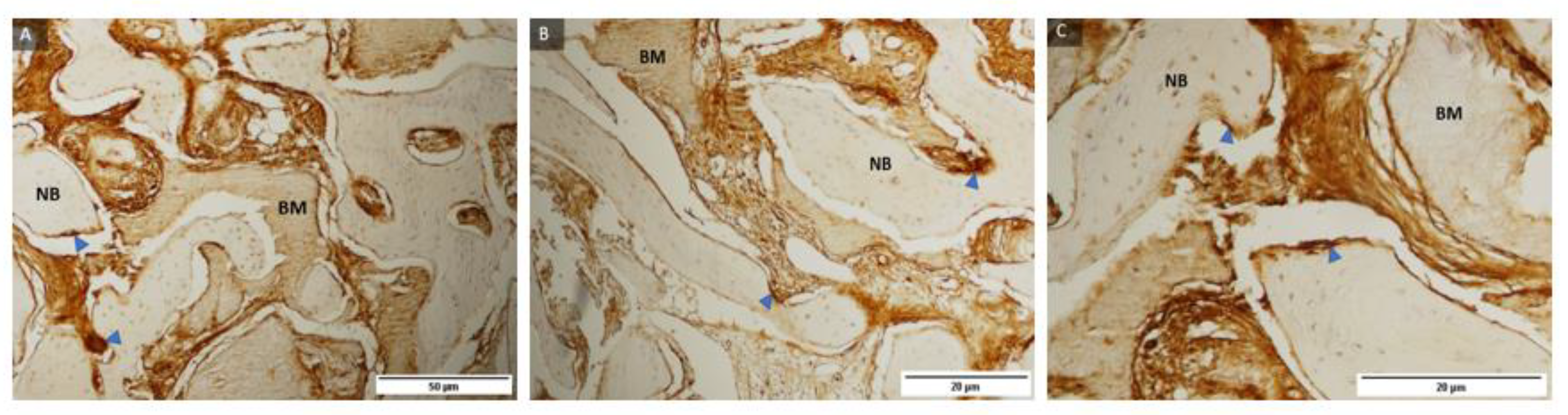
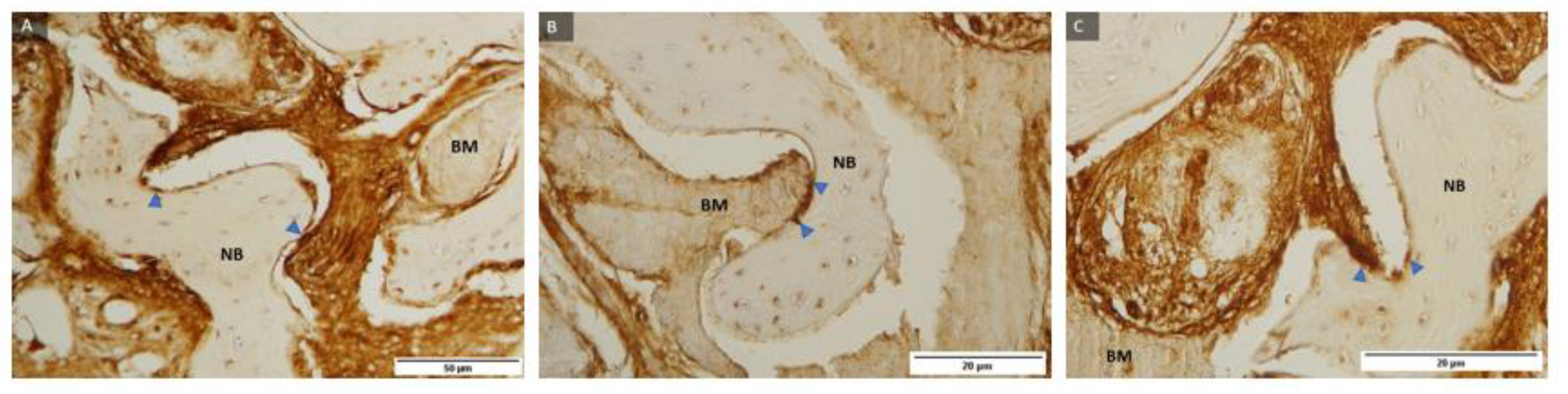
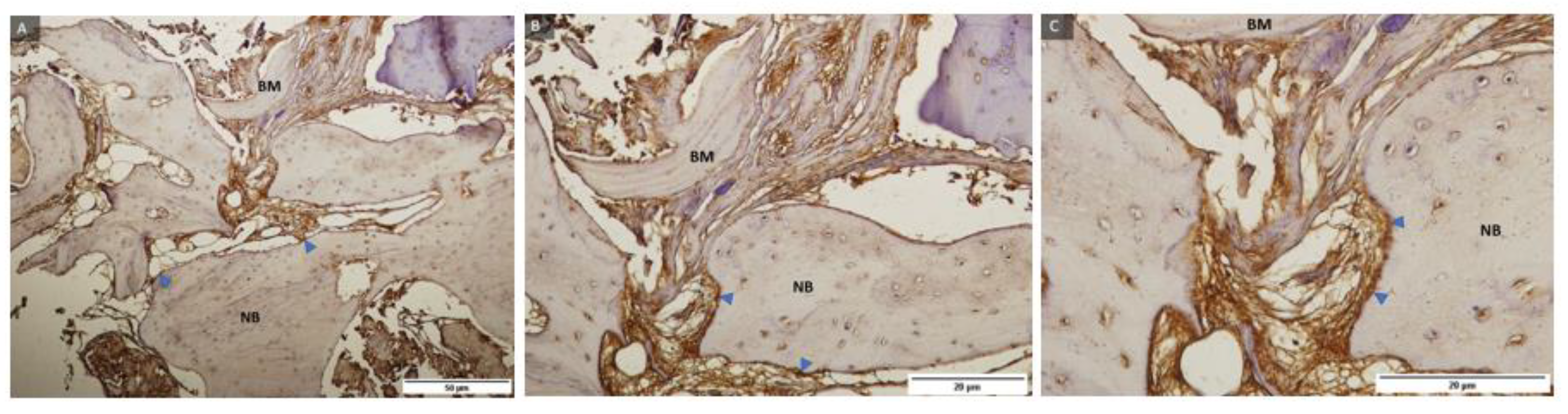
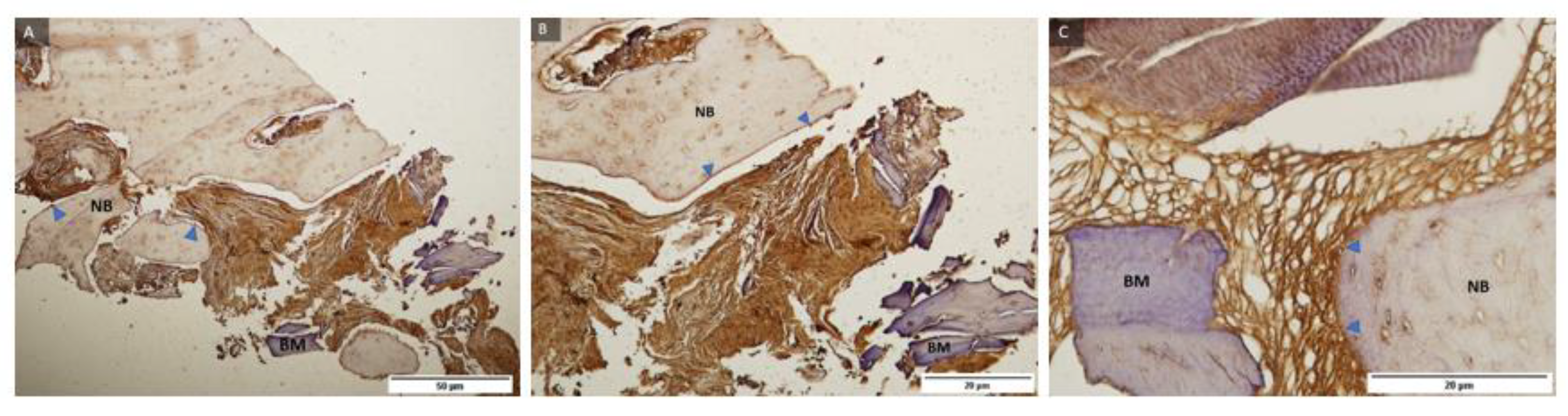
2.4. Immunohistochemical Analysis
3. Discussion
4. Materials and Methods
4.1. Subjects
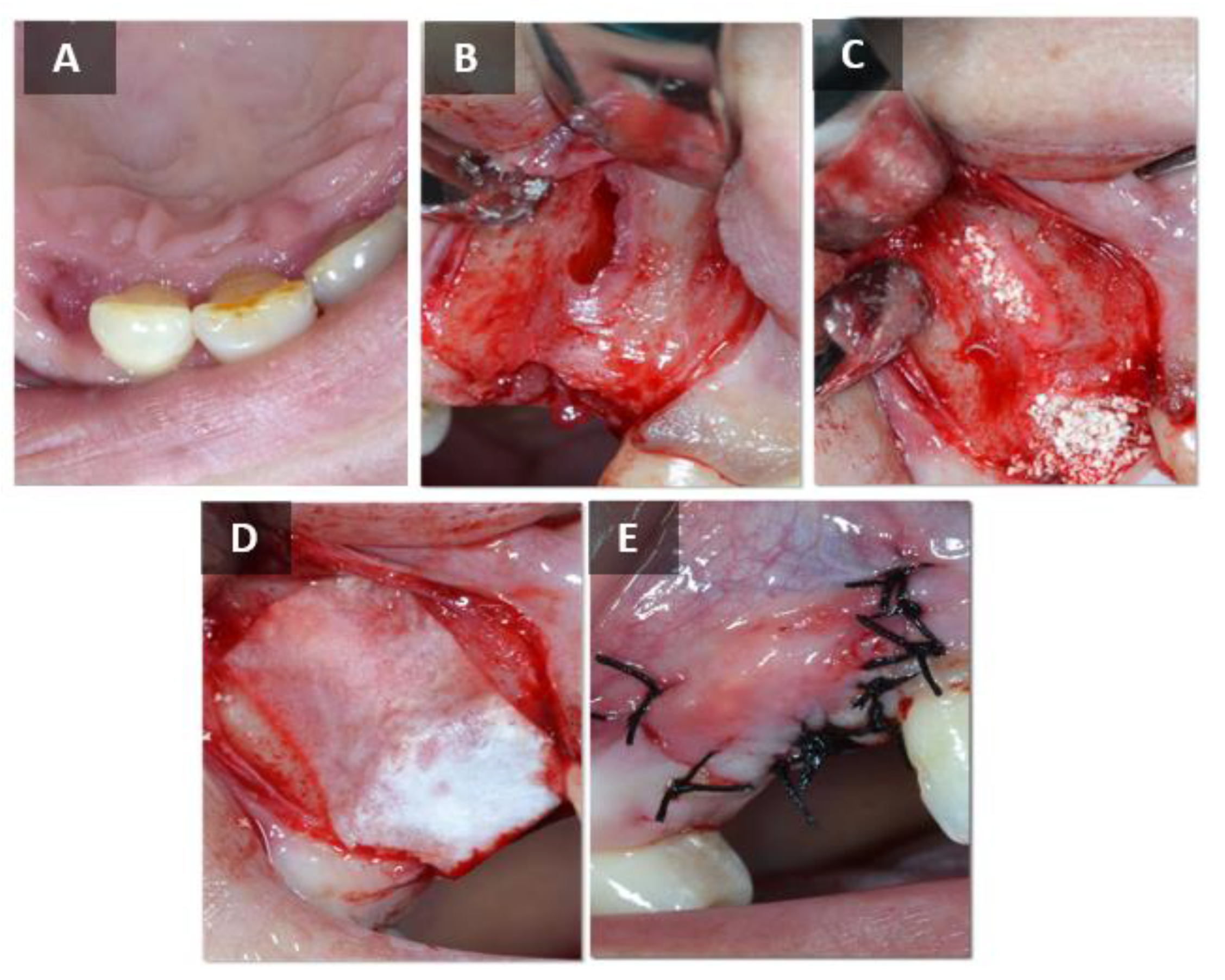
4.2. Surgical Phase
4.3. Qualitative Analysis of the Histological Bone Biopsy Samples Was Performed
4.4. Quantitative Analysis of Histological Bone Biopsy Samples
4.5. Immunohistochemical Analysis of Bone Biopsy Samples
4.6. Statistical Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ono, T.; Nakashima, T. Oral Bone Biology. J. Oral Biosci. 2022, 64, 8–17. [Google Scholar] [CrossRef]
- Devlin, H.; Hoyland, J.; Newall, J.F.; Ayad, S. Trabecular Bone Formation in the Healing of the Rodent Molar Tooth Extraction Socket. J. Bone Miner. Res. 1997, 12, 2061–2067. [Google Scholar] [CrossRef] [PubMed]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone Healing and Soft Tissue Contour Changes Following Single-Tooth Extraction: A Clinical and Radiographic 12-Month Prospective Study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Irinakis, T.; Tabesh, M. Preserving the Socket Dimensions with Bone Grafting in Single Sites: An Esthetic Surgical Approach When Planning Delayed Implant Placement. J. Oral Implant. 2006, 33, 917–922. [Google Scholar] [CrossRef] [PubMed]
- Araújo, M.G.; Lindhe, J. Dimensional Ridge Alterations Following Tooth Extraction. An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Araújo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Ridge Alterations Following Implant Placement in Fresh Extraction Sockets: An Experimental Study in the Dog. J. Clin. Periodontol. 2005, 32, 645–652. [Google Scholar] [CrossRef]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-Tissue Alterations Following Immediate Implant Placement in Extraction Sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Shenoy, V.K. Single Tooth Implants: Pretreatment Considerations and Pretreatment Evaluation. J. Interdiscip. Dent. 2012, 2, 149. [Google Scholar] [CrossRef]
- Darby, I.; Chen, S.; De Poi, R. Ridge Preservation: What Is It and When Should It Be Considered. Aust. Dent. J. 2008, 53, 11–21. [Google Scholar] [CrossRef]
- Nevins, M.; Mellonig, J.T.; Clem, D.S.; Reiser, G.M.; Buser, D.A. Implants in Regenerated Bone: Long-Term Survival. Int. J. Periodontics Restor. Dent. 1998, 18, 34–45. [Google Scholar]
- Sassano, P.; Gennaro, P.; Chisci, G.; Gabriele, G.; Aboh, I.V.; Mitro, V.; Di Curzio, P. Calvarial Onlay Graft and Submental Incision in Treatment of Atrophic Edentulous Mandibles: An Approach to Reduce Postoperative Complications. J. Craniofac. Surg. 2014, 25, 693–697. [Google Scholar] [CrossRef]
- Crespi, R.; Toti, P.; Covani, U.; Crespi, G.; Menchini-Fabris, G.-B. Changes in Alveolar Bone Width Following Immediate Implant and Fresh Socket Preservation with Xenogeneic Gap-Filling Material Versus Guided Tissue Healing with Anatomical Tooth-Shaped Caps: A 3-Year Retrospective Case-Control Study. Int. J. Periodontics Restor. Dent. 2023, 43, 75–83. [Google Scholar] [CrossRef]
- Chisci, G.; Fredianelli, L. Therapeutic Efficacy of Bromelain in Alveolar Ridge Preservation. Antibiotics 2022, 11, 1542. [Google Scholar] [CrossRef]
- Bhatt, R.A.; Rozental, T.D. Bone Graft Substitutes. Hand Clin. 2012, 28, 457–468. [Google Scholar] [CrossRef]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign Body Reaction to Biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [Green Version]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing Esthetics for Implant Restorations in the Anterior Maxilla: Anatomic and Surgical Considerations. Int. J. Oral Maxillofac. Implant. 2004, 19, 43–61. [Google Scholar]
- Buser, D.; Chen, S.T.; Weber, H.; Belser, U. Early Implant Placement Following Single-Tooth Extraction in the Esthetic Zone: Biologic Rationale and Surgical Procedures. Int. J. Periodontics Restor. Dent. 2008, 28, 441–451. [Google Scholar]
- Hämmerle, C.H.F.; Chiantella, G.C.; Karring, T.; Lang, N.P. The Effect of a Deproteinized Bovine Bone Mineral on Bone Regeneration around Titanium Dental Implants. Clin. Oral Implant. Res. 1998, 9, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Byun, H.; Madhurakkat Perikamana, S.K.; Lee, S.; Shin, H. Current Advances in Immunomodulatory Biomaterials for Bone Regeneration. Adv. Healthcare Mater. 2019, 8, e1801106. [Google Scholar] [CrossRef] [PubMed]
- Kolk, A.; Handschel, J.; Drescher, W.; Rothamel, D.; Kloss, F.; Blessmann, M.; Heiland, M.; Wolff, K.D.; Smeets, R. Current Trends and Future Perspectives of Bone Substitute Materials—From Space Holders to Innovative Biomaterials. J. Craniomaxillofac. Surg. 2012, 40, 706–718. [Google Scholar] [CrossRef]
- Horch, H.H.; Sader, R.; Pautke, C.; Neff, A.; Deppe, H.; Kolk, A. Synthetic, Pure-Phase Beta-Tricalcium Phosphate Ceramic Granules (Cerasorb) for Bone Regeneration in the Reconstructive Surgery of the Jaws. Int. J. Oral Maxillofac. Surg. 2006, 35, 708–713. [Google Scholar] [CrossRef]
- Buser, D.; Hoffmann, B.; Bernard, J.P.; Lussi, A.; Mettler, D.; Schenk, R.K. Evaluation of Filling Materials in Membrane--Protected Bone Defects. A Comparative Histomorphometric Study in the Mandible of Miniature Pigs. Clin. Oral Implant. Res. 1998, 9, 137–150. [Google Scholar] [CrossRef] [PubMed]
- Haugen, H.J.; Lyngstadaas, S.P.; Rossi, F.; Perale, G. Bone Grafts: Which Is the Ideal Biomaterial? J. Clin. Periodontol. 2019, 46, 92–102. [Google Scholar] [CrossRef] [PubMed]
- Pikos, M.A. Block Autografts for Localized Ridge Augmentation: Part II. The Posterior Mandible. Implant. Dent. 2000, 9, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, S.; Deshmukh, J.; Deshpande, S.; Khatri, R.; Deshpande, S. Vertical and Horizontal Ridge Augmentation in Anterior Maxilla Using Autograft, Xenograft and Titanium Mesh with Simultaneous Placement of Endosseous Implants. J. Indian Soc. Periodontol. 2014, 18, 661–665. [Google Scholar] [CrossRef] [PubMed]
- Johansson, B.; Grepe, A.; Wannfors, K.; Hirsch, J.M. A Clinical Study of Changes in the Volume of Bone Grafts in the Atrophic Maxilla. Dentomaxillofacial Radiol. 2001, 30, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Cecchinato, D.; Donati, M.; Tomasi, C.; Liljenberg, B. Ridge Preservation with the Use of Deproteinized Bovine Bone Mineral. Clin. Oral Implant. Res. 2014, 25, 786–790. [Google Scholar] [CrossRef]
- Helder, M.N.; van Esterik, F.A.S.; Kwehandjaja, M.D.; ten Bruggenkate, C.M.; Klein-Nulend, J.; Schulten, E.A.J.M. Evaluation of a New Biphasic Calcium Phosphate for Maxillary Sinus Floor Elevation: Micro-CT and Histomorphometrical Analyses. Clin. Oral Implant. Res. 2018, 29, 488–498. [Google Scholar] [CrossRef] [Green Version]
- Ohayon, L. Maxillary Sinus Floor Augmentation Using Biphasic Calcium Phosphate: A Histologic and Histomorphometric Study. Int. J. Oral Maxillofac. Implant. 2014, 29, 1143–1148. [Google Scholar] [CrossRef] [Green Version]
- Von Arx, T.; Buser, D. Horizontal Ridge Augmentation Using Autogenous Block Grafts and the Guided Bone Regeneration Technique with Collagen Membranes: A Clinical Study with 42 Patients. Clin. Oral Implant. Res. 2006, 17, 359–366. [Google Scholar] [CrossRef]
- Martinez, A.; Balboa, O.; Gasamans, I.; Otero-Cepeda, X.L.; Guitian, F. Deproteinated Bovine Bone vs. Beta-Tricalcium Phosphate as Bone Graft Substitutes: Histomorphometric Longitudinal Study in the Rabbit Cranial Vault. Clin. Oral Implant. Res. 2015, 26, 623–632. [Google Scholar] [CrossRef]
- Jensen, S.S.; Broggini, N.; Hjørting-Hansen, E.; Schenk, R.; Buser, D. Bone Healing and Graft Resorption of Autograft, Anorganic Bovine Bone and Beta-Tricalcium Phosphate. A Histologic and Histomorphometric Study in the Mandibles of Minipigs. Clin. Oral Implant. Res. 2006, 17, 237–243. [Google Scholar] [CrossRef]
- Franco, M.; Viscioni, A.; Rigo, L.; Guidi, R.; Strohmenger, L.; Zollino, I.; Avantaggiato, A.; Carinci, F. Wide Diameter Implants Inserted in Jaws Grafted with Homologue Bone. Acta Stomatol. Croat. 2008, 42, 273–282. [Google Scholar]
- Chiapasco, M.; Zaniboni, M.; Boisco, M. Augmentation Procedures for the Rehabilitation of Deficient Edentulous Ridges with Oral Implants. Clin. Oral Implant. Res. 2006, 17, 136–159. [Google Scholar] [CrossRef]
- Kao, S.T.; Scott, D.D. A Review of Bone Substitutes. Oral Maxillofac. Surg. Clin. N. Am. 2007, 19, 513–521. [Google Scholar] [CrossRef]
- Fernandez de Grado, G.; Keller, L.; Idoux-Gillet, Y.; Wagner, Q.; Musset, A.M.; Benkirane-Jessel, N.; Bornert, F.; Offner, D. Bone Substitutes: A Review of Their Characteristics, Clinical Use, and Perspectives for Large Bone Defects Management. J. Tissue Eng. 2018, 9, 2041731418776819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Aql, Z.S.; Alagl, A.S.; Graves, D.T.; Gerstenfeld, L.C.; Einhorn, T.A. Molecular Mechanisms Controlling Bone Formation during Fracture Healing and Distraction Osteogenesis. J. Dent. Res. 2008, 87, 107–118. [Google Scholar] [CrossRef]
- Kim, Y.; Nowzari, H.; Rich, S.K. Risk of Prion Disease Transmission through Bovine-Derived Bone Substitutes: A Systematic Review. Clin. Implant. Dent. Relat. Res. 2013, 15, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Wenz, B.; Oesch, B.; Horst, M. Analysis of the Risk of Transmitting Bovine Spongiform Encephalopathy through Bone Grafts Derived from Bovine Bone. Biomaterials 2001, 22, 1599–1606. [Google Scholar] [CrossRef]
- Berglundh, T.; Lindhe, J. Healing around Implants Placed in Bone Defects Treated with Bio-Oss. An Experimental Study in the Dog. Clin. Oral Implant. Res. 1997, 8, 117–124. [Google Scholar] [CrossRef]
- Urban, I.A.; Ravidà, A.; Saleh, M.H.A.; Galli, M.; Lozada, J.; Farkasdi, S.; Wang, H.L. Long-Term Crestal Bone Changes in Implants Placed in Augmented Sinuses with Minimal or Moderate Remaining Alveolar Bone: A 10-Year Retrospective Case-Series Study. Clin. Oral Implant. Res. 2021, 32, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Galindo-Moreno, P.; Abril-García, D.; Carrillo-Galvez, A.B.; Zurita, F.; Martín-Morales, N.; O’Valle, F.; Padial-Molina, M. Maxillary Sinus Floor Augmentation Comparing Bovine versus Porcine Bone Xenografts Mixed with Autogenous Bone Graft. A Split-Mouth Randomized Controlled Trial. Clin. Oral Implant. Res. 2022, 33, 524–536. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, M.; Favero, G.; Scarano, A.; Orsini, G.; Piattelli, A. Bone Reactions to Anorganic Bovine Bone (Bio-Oss) Used in Sinus Augmentation Procedures: A Histologic Long-Term Report of 20 Cases in Humans. Int. J. Oral Maxillofac. Implant. 1999, 14, 835–840. [Google Scholar]
- Kumar, P.; Vinitha, B.; Fathima, G. Bone Grafts in Dentistry. J. Pharm. Bioallied Sci. 2013, 5, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.; Barbeck, M.; Kirkpatrick, C.; Sader, R.; Lerner, H.; Ghanaati, S. Injectable Bone Substitute Material on the Basis of?—TCP and Hyaluronan Achieves Complete Bone Regeneration While Undergoing Nearly Complete Degradation. Int. J. Oral Maxillofac. Implant. 2018, 33, 636–644. [Google Scholar] [CrossRef]
- Barbeck, M.; Jung, O.; Smeets, R.; Gosau, M.; Schnettler, R.; Rider, P.; Houshmand, A.; Korzinskas, T. Implantation of an Injectable Bone Substitute Material Enables Integration Following the Principles of Guided Bone Regeneration. In Vivo 2020, 34, 557–568. [Google Scholar] [CrossRef] [Green Version]
- Ku, J.K.; Hong, I.; Lee, B.K.; Yun, P.Y.; Lee, J.K. Dental Alloplastic Bone Substitutes Currently Available in Korea. J. Korean Assoc. Oral Maxillofac. Surg. 2019, 45, 51–67. [Google Scholar] [CrossRef] [Green Version]
- Al-Nawas, B.; Schiegnitz, E. Augmentation Procedures Using Bone Substitute Materials or Autogenous Bone—A Systematic Review and Meta-Analysis. Eur. J. Oral Implantol. 2014, 7, 219–234. [Google Scholar]
- Onişor-Gligor, F.; Juncar, M.; Câmpian, R.S.; Băciuţ, G.; Bran, S.; Băciuţ, M.F. Subantral Bone Grafts, a Comparative Study of the Degree of Resorption of Alloplastic versus Autologous Grafts. Rom. J. Morphol. Embryol. 2015, 56, 1003–1009. [Google Scholar]
- Kakar, A.; Rao, B.H.S.; Hegde, S.; Deshpande, N.; Lindner, A.; Nagursky, H.; Patney, A.; Mahajan, H. Ridge Preservation Using an in Situ Hardening Biphasic Calcium Phosphate (β-TCP/HA) Bone Graft Substitute—A Clinical, Radiological, and Histological Study. Int. J. Implant. Dent. 2017, 3, 25. [Google Scholar] [CrossRef] [Green Version]
- Annibali, S.; Iezzi, G.; Sfasciotti, G.L.; Cristalli, M.P.; Vozza, I.; Mangano, C.; La Monaca, G.; Polimeni, A. Histological and Histomorphometric Human Results of HA-Beta-TCP 30/70 Compared to Three Different Biomaterials in Maxillary Sinus Augmentation at 6 Months: A Preliminary Report. BioMed Res. Int. 2015, 2015, 156850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, T.; Takayanagi, H. Osteoimmunology in Bone Fracture Healing. Curr. Osteoporos. Rep. 2017, 15, 367–375. [Google Scholar] [CrossRef]
- Schlundt, C.; Schell, H.; Goodman, S.B.; Vunjak-Novakovic, G.; Duda, G.N.; Schmidt-Bleek, K. Immune Modulation as a Therapeutic Strategy in Bone Regeneration. J. Exp. Orthop. 2015, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Einhorn, T.A.; Gerstenfeld, L.C. Fracture Healing: Mechanisms and Interventions. Nat. Rev. Rheumatol. 2015, 11, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mountziaris, P.M.; Mikos, A.G. Modulation of the Inflammatory Response for Enhanced Bone Tissue Regeneration. Tissue Eng. Part. B Rev. 2008, 14, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.E.; Salhotra, A.; Robertson, K.S.; Ransom, R.C.; Foster, D.S.; Shah, H.N.; Quarto, N.; Wan, D.C.; Longaker, M.T. Skeletal Stem Cell-Schwann Cell Circuitry in Mandibular Repair. Cell Rep. 2019, 28, 2757–2766.e5. [Google Scholar] [CrossRef]
- Gerstenfeld, L.C.; Cullinane, D.M.; Barnes, G.L.; Graves, D.T.; Einhorn, T.A. Fracture Healing as a Post-Natal Developmental Process: Molecular, Spatial, and Temporal Aspects of Its Regulation. J. Cell. Biochem. 2003, 88, 873–884. [Google Scholar] [CrossRef]
- Cameron, J.A.; Milner, D.J.; Lee, J.S.; Cheng, J.; Fang, N.X.; Jasiuk, I.M. Employing the Biology of Successful Fracture Repair to Heal Critical Size Bone Defects. Curr. Top. Microbiol. Immunol. 2013, 367, 113–132. [Google Scholar] [CrossRef]
- Dimitriou, R.; Tsiridis, E.; Giannoudis, P.V. Current Concepts of Molecular Aspects of Bone Healing. Injury 2005, 36, 1392–1404. [Google Scholar] [CrossRef]
- Nakashima, K.; Zhou, X.; Kunkel, G.; Zhang, Z.; Deng, J.M.; Behringer, R.R.; de Crombrugghe, B. The Novel Zinc Finger-Containing Transcription Factor Osterix Is Required for Osteoblast Differentiation and Bone Formation. Cell 2002, 108, 17–29. [Google Scholar] [CrossRef] [Green Version]
- Hojo, H.; Ohba, S.; He, X.; Lai, L.P.; McMahon, A.P. Sp7/Osterix Is Restricted to Bone-Forming Vertebrates Where It Acts as a Dlx Co-Factor in Osteoblast Specification. Dev. Cell 2016, 37, 238–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; Li, M.; Wang, S.; Xiao, Z.; Xiong, Y.; Wang, G. Recent Advances of Osterix Transcription Factor in Osteoblast Differentiation and Bone Formation. Front. Cell Dev. Biol. 2020, 8, 601224. [Google Scholar] [CrossRef] [PubMed]
- Čandrlić, M.; Tomas, M.; Karl, M.; Malešić, L.; Včev, A.; Perić Kačarević, Ž.; Matijević, M. Comparison of Injectable Biphasic Calcium Phosphate and a Bovine Xenograft in Socket Preservation: Qualitative and Quantitative Histologic Study in Humans. Int. J. Mol. Sci. 2022, 23, 2539. [Google Scholar] [CrossRef] [PubMed]
- Jelusic, D.; Zirk, M.L.; Fienitz, T.; Plancak, D.; Puhar, I.; Rothamel, D. Monophasic ß-TCP vs. Biphasic HA/ß-TCP in Two-Stage Sinus Floor Augmentation Procedures—A Prospective Randomized Clinical Trial. Clin. Oral Implant. Res. 2017, 28, e175–e183. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, L.; Bosshardt, D.D.; Palattella, P.; Rao, W.; Serino, G.; Chiapasco, M. Maxillary Sinus Grafting with Bio-Oss® or Straumann® Bone Ceramic: Histomorphometric Results from a Randomized Controlled Multicenter Clinical Trial. Clin. Oral Implant. Res. 2008, 19, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Menezes, J.D.; Pereira, R.D.S.; Bonardi, J.P.; Griza, G.L.; Okamoto, R.; Hochuli-Vieira, E. Bioactive Glass Added to Autogenous Bone Graft in Maxillary Sinus Augmentation: A Prospective Histomorphometric, Immunohistochemical, and Bone Graft Resorption Assessment. J. Appl. Oral Sci. 2018, 26, e20170296. [Google Scholar] [CrossRef]
- Nizam, N.; Eren, G.; Akcalı, A.; Donos, N. Maxillary Sinus Augmentation with Leukocyte and Platelet-Rich Fibrin and Deproteinized Bovine Bone Mineral: A Split-Mouth Histological and Histomorphometric Study. Clin. Oral Implant. Res. 2018, 29, 67–75. [Google Scholar] [CrossRef]
- Cömert Kılıç, S.; Güngörmüş, M.; Parlak, S.N. Histologic and Histomorphometric Assessment of Sinus-Floor Augmentation with Beta-Tricalcium Phosphate Alone or in Combination with Pure-Platelet-Rich Plasma or Platelet-Rich Fibrin: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 959–967. [Google Scholar] [CrossRef]
- Artzi, Z.; Nemcovsky, C.E.; Tal, H.; Dayan, D. Histopathological Morphometric Evaluation of 2 Different Hydroxyapatite-Bone Derivatives in Sinus Augmentation Procedures: A Comparative Study in Humans. J. Periodontol. 2001, 72, 911–920. [Google Scholar] [CrossRef] [Green Version]
- Dos Anjos, T.L.M.R.; De Molon, R.S.; Paim, P.R.F.; Marcantonio, E.; Marcantonio, E.; Faeda, R.S. Implant Stability after Sinus Floor Augmentation with Deproteinized Bovine Bone Mineral Particles of Different Sizes: A Prospective, Randomized and Controlled Split-Mouth Clinical Trial. Int. J. Oral Maxillofac. Surg. 2016, 45, 1556–1563. [Google Scholar] [CrossRef] [Green Version]
- Jensen, S.; Aaboe, M.; Pinholt, E.; Hjørting-Hansen, E.; Melsen, F.; Ruyter, I.E. Tissue Reaction and Material Characteristics of Four Bone Substitutes. Int. J. Oral Maxillofac. Implant. 1996, 11, 55–66. [Google Scholar]
- McAllister, B.; Margolin, M.; Cogan, A.; Taylor, M.; Wollins, J. Residual Lateral Wall Defects Following Sinus Grafting with Recombinant Human Osteogenic Protein-1 or Bio-Oss in the Chimpanzee. Int. J. Periodontics Restor. Dent. 1998, 18, 227–239. [Google Scholar]
- McAllister, B.; Margolin, M.; Cogan, A.; Buck, D.; Hollinger, J.; Lynch, S. Eighteen-Month Radiographic and Histologic Evaluation of Sinus Grafting with Anorganic Bovine Bone in the Chimpanzee. Int. J. Oral Maxillofac. Implant. 1999, 14, 361–368. [Google Scholar]
- Mah, J.; Hung, J.; Wang, J.; Salih, E. The Efficacy of Various Alloplastic Bone Grafts on the Healing of Rat Calvarial Defects. Eur. J. Orthod. 2004, 26, 475–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Piattelli, A.; Pecora, G.; Petrizzi, L.; Valbonetti, L.; Varasano, V.; Iezzi, G. A Histomorphometric Comparison of Anorganic Bovine Bone (ABB) and Calcium Sulfate (CaS) Used in Sinus Augmentation Procedures: A Study in Sheep. J. Osseointegration 2009, 2, 75–81. [Google Scholar] [CrossRef]
- Aludden, H.; Mordenfeld, A.; Dahlin, C.; Hallman, M.; Starch-Jensen, T. Histological and Histomorphometrical Outcome after Lateral Guided Bone Regeneration Augmentation of the Mandible with Different Ratios of Deproteinized Bovine Bone Mineral and Autogenous Bone. A Preclinical in Vivo Study. Clin. Oral Implant. Res. 2020, 31, 1025–1036. [Google Scholar] [CrossRef]
- Zitzmann, N.U.; Schärer, P.; Marinello, C.P.; Schüpbach, P.; Berglundh, T. Alveolar Ridge Augmentation with Bio-Oss: A Histologic Study in Humans. Int. J. Periodontics Restor. Dent. 2001, 21, 288–295. [Google Scholar]
- Amoian, B.; Moudi, E.; Majidi, M.S.; Ali Tabatabaei, S.M. A Histologic, Histomorphometric, and Radiographic Comparison between Two Complexes of CenoBoen/CenoMembrane and Bio-Oss/Bio-Gide in Lateral Ridge Augmentation: A Clinical Trial. Dent. Res. J. 2016, 13, 446–453. [Google Scholar] [CrossRef]
- Scarano, A.; Degidi, M.; Iezzi, G.; Pecora, G.; Piattelli, M.; Orsini, G.; Caputi, S.; Perrotti, V.; Mangano, C.; Piattelli, A. Maxillary Sinus Augmentation with Different Biomaterials: A Comparative Histologic and Histomorphometric Study in Man. Implant. Dent. 2006, 15, 197–207. [Google Scholar] [CrossRef]
- Wei, Y.; Xu, T.; Hu, W.; Zhao, L.; Wang, C.; Chung, K.-H. Socket Preservation Following Extraction of Molars with Severe Periodontitis. Int. J. Periodontics Restor. Dent. 2021, 41, 269–275. [Google Scholar] [CrossRef]
- Froum, S.; Wallace, S.; Cho, S.-C.; Elian, N.; Tarnow, D. Histomorphometric Comparison of a Biphasic Bone Ceramic to Anorganic Bovine Bone for Sinus Augmentation: 6- to 8-Month Postsurgical Assessment of Vital Bone Formation. A Pilot Study. Int. J. Periodontics Restor. Dent. 2008, 28, 273–281. [Google Scholar]
- Schmitt, C.M.; Doering, H.; Schmidt, T.; Lutz, R.; Neukam, F.W.; Schlegel, K.A. Histological Results after Maxillary Sinus Augmentation with Straumann® BoneCeramic, Bio-Oss®, Puros®, and Autologous Bone. A Randomized Controlled Clinical Trial. Clin. Oral Implant. Res. 2013, 24, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, J.; Kubesch, A.; Korzinskas, T.; Barbeck, M.; Landes, C.; Sader, R.A.; Kirkpatrick, C.J.; Ghanaati, S. TRAP-Positive Multinucleated Giant Cells Are Foreign Body Giant Cells Rather Than Osteoclasts: Results From a Split-Mouth Study in Humans. J. Oral Implantol. 2015, 41, e257–e266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fienitz, T.; Moses, O.; Klemm, C.; Happe, A.; Ferrari, D.; Kreppel, M.; Ormianer, Z.; Gal, M.; Rothamel, D. Histological and Radiological Evaluation of Sintered and Non-Sintered Deproteinized Bovine Bone Substitute Materials in Sinus Augmentation Procedures. A Prospective, Randomized-Controlled, Clinical Multicenter Study. Clin. Oral Investig. 2017, 21, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Sivolella, S.; Botticelli, D.; Prasad, S.; Ricci, S.; Bressan, E.; Prasad, H. Evaluation and Comparison of Histologic Changes and Implant Survival in Extraction Sites Immediately Grafted with Two Different Xenografts: A Randomized Clinical Pilot Study. Clin. Oral Implant. Res. 2020, 31, 825–835. [Google Scholar] [CrossRef]
- Pignaton, T.B.; Spin-Neto, R.; de Ferreira, C.E.A.; Martinelli, C.B.; de Oliveira, G.J.P.L.; Marcantonio, E. Remodelling of Sinus Bone Grafts According to the Distance from the Native Bone: A Histomorphometric Analysis. Clin. Oral Implant. Res. 2020, 31, 959–967. [Google Scholar] [CrossRef]
- Santos, A.; Botelho, J.; Machado, V.; Borrecho, G.; Proença, L.; Mendes, J.J.; Mascarenhas, P.; Alcoforado, G. Autogenous Mineralized Dentin versus Xenograft Granules in Ridge Preservation for Delayed Implantation in Post-Extraction Sites: A Randomized Controlled Clinical Trial with an 18 Months Follow-Up. Clin. Oral Implant. Res. 2021, 32, 905–915. [Google Scholar] [CrossRef]
- Jensen, T.; Schou, S.; Stavropoulos, A.; Terheyden, H.; Holmstrup, P. Maxillary Sinus Floor Augmentation with Bio-Oss or Bio-Oss Mixed with Autogenous Bone as Graft in Animals: A Systematic Review. Int. J. Oral Maxillofac. Surg. 2012, 41, 114–120. [Google Scholar] [CrossRef]
- Calasans-Maia, M.D.; de Mourão, C.F.A.B.; Alves, A.T.N.N.; Sartoretto, S.C.; de Uzeda, M.J.P.G.; Granjeiro, J.M. Maxillary Sinus Augmentation with a New Xenograft: A Randomized Controlled Clinical Trial. Clin. Implant. Dent. Relat. Res. 2015, 17, 586–593. [Google Scholar] [CrossRef]
- Uzbek, U.H.; Rahman, S.A.B.; Alam, M.K.; Gillani, S.W. Bone Forming Potential of An-Organic Bovine Bone Graft: A Cone Beam CT Study. J. Clin. Diagn. Res. 2014, 8, 73–76. [Google Scholar] [CrossRef]
- Gauthier, O.; Boix, D.; Grimandi, G.; Aguado, E.; Bouler, J.-M.; Weiss, P.; Daculsi, G. A New Injectable Calcium Phosphate Biomaterial for Immediate Bone Filling of Extraction Sockets: A Preliminary Study in Dogs. J. Periodontol. 1999, 70, 375–383. [Google Scholar] [CrossRef]
- Boix, D.; Gauthier, O.; Guicheux, J.; Pilet, P.; Weiss, P.; Grimandi, G.; Daculsi, G. Alveolar Bone Regeneration for Immediate Implant Placement Using an Injectable Bone Substitute: An Experimental Study in Dogs. J. Periodontol. 2004, 75, 663–671. [Google Scholar] [CrossRef]
- Aral, A.; Yalçn, S.; Karabuda, Z.C.; Anl, A.; Jansen, J.A.; Mutlu, Z. Injectable Calcium Phosphate Cement as a Graft Material for Maxillary Sinus Augmentation: An Experimental Pilot Study. Clin. Oral Implant. Res. 2008, 19, 612–617. [Google Scholar] [CrossRef]
- Struillou, X.; Boutigny, H.; Badran, Z.; Fellah, B.H.; Gauthier, O.; Sourice, S.; Pilet, P.; Rouillon, T.; Layrolle, P.; Weiss, P.; et al. Treatment of Periodontal Defects in Dogs Using an Injectable Composite Hydrogel/Biphasic Calcium Phosphate. J. Mater. Sci. Mater. Med. 2011, 22, 1707–1717. [Google Scholar] [CrossRef]
- Papanchev, G.; Georgiev, T.; Peev, S.; Arnautska, H.; Zgurova, N.; Borisova-Papancheva, T.; Dzhongova, E. Comparison of the Rates of Bone Regeneration in Sinus Lift Grafting with a Calcium-Phosphate Paste between the 6th and the 9th Month—A Clinical Case. Scr. Sci. Med. Dent. 2015, 1, 41. [Google Scholar] [CrossRef] [Green Version]
- Ricci, L.; Perrotti, V.; Ravera, L.; Scarano, A.; Piattelli, A.; Iezzi, G. Rehabilitation of Deficient Alveolar Ridges Using Titanium Grids before and Simultaneously with Implant Placement: A Systematic Review. J. Periodontol. 2013, 84, 1234–1242. [Google Scholar] [CrossRef]
- Nery, J.C.; Pereira, L.A.V.D.; Guimarães, G.F.; Scardueli, C.R.; França, F.M.G.; Spin-Neto, R.; Stavropoulos, A. β-TCP/HA with or without Enamel Matrix Proteins for Maxillary Sinus Floor Augmentation: A Histomorphometric Analysis of Human Biopsies. Int. J. Implant. Dent. 2017, 3, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flichy-Fernández, A.J.; Blaya-Tárraga, J.A.; O’Valle, F.; Padial-Molina, M.; Peñarrocha-Diago, M.; Galindo-Moreno, P. Sinus Floor Elevation Using Particulate PLGA-Coated Biphasic Calcium Phosphate Bone Graft Substitutes: A Prospective Histological and Radiological Study. Clin. Implant. Dent. Relat. Res. 2019, 21, 895–902. [Google Scholar] [CrossRef] [PubMed]
- Tetè, S.; Mastrangelo, F.; Carone, L.; Nargi, E.; Costanzo, G.; Vinci, R.; Burruano, F.; Tortorici, S.; Dadorante, V.; Caciagli, F.; et al. Morphostructural Analysis of Human Follicular Stem Cells on Highly Porous Bone Hydroxyapatite Scaffold. Int. J. Immunopathol. Pharmacol. 2007, 20, 819–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mastrangelo, F.; Nargi, E.; Carone, L.; Dolci, M.; Caciagli, F.; Ciccarelli, R.; de Lutiis, M.A.; Karapanou, V.; Shaik, B.Y.; Conti, P.; et al. Tridimensional Response of Human Dental Follicular Stem Cells onto a Synthetic Hydroxyapatite Scaffold. J. Health Sci. 2008, 54, 154–161. [Google Scholar] [CrossRef] [Green Version]
- Stevens, B.; Yang, Y.; Mohandas, A.; Stucker, B.; Nguyen, K.T. A Review of Materials, Fabrication Methods, and Strategies Used to Enhance Bone Regeneration in Engineered Bone Tissues. J. Biomed. Mater. Res. B Appl. Biomater. 2008, 85, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Khaled, H.; Atef, M.; Hakam, M. Maxillary Sinus Floor Elevation Using Hydroxyapatite Nano Particles vs Tenting Technique with Simultaneous Implant Placement: A Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2019, 21, 1241–1252. [Google Scholar] [CrossRef]
- Georgiev, T.; Peev, S.; Arnautska, H.; Gencheva, A.; Gerdzhikov, I. An Evaluation of Three-Dimensional Scans of the Time-Dependent Volume Changes in Bone Grafting Materials. Int. J. Sci. Res. (IJSR) 2017, 6, 562–571. [Google Scholar] [CrossRef]
- Götz, W.; Gerber, T.; Michel, B.; Lossdörfer, S.; Henkel, K.O.; Heinemann, F. Immunohistochemical Characterization of Nanocrystalline Hydroxyapatite Silica Gel (NanoBone®) Osteogenesis: A Study on Biopsies from Human Jaws. Clin. Oral Implant. Res. 2008, 19, 1016–1026. [Google Scholar] [CrossRef] [PubMed]
- Ortuño, M.J.; Susperregui, A.R.G.; Artigas, N.; Rosa, J.L.; Ventura, F. Osterix Induces Col1a1 Gene Expression through Binding to Sp1 Sites in the Bone Enhancer and Proximal Promoter Regions. Bone 2013, 52, 548–556. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Huang, Y.; Zhang, L.; Zhang, C. Transcriptional Regulation of Bone Sialoprotein Gene Expression by Osx. Biochem. Biophys. Res. Commun. 2016, 476, 574–579. [Google Scholar] [CrossRef]
- Friedmann, A.; Gissel, K.; Konermann, A.; Götz, W. Tissue Reactions after Simultaneous Alveolar Ridge Augmentation with Biphasic Calcium Phosphate and Implant Insertion—Histological and Immunohistochemical Evaluation in Humans. Clin. Oral Investig. 2015, 19, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Wang, H.L. Medical Contraindications to Implant Therapy: Part I: Absolute Contraindications. Implant. Dent. 2006, 15, 353–360. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | |
|---|---|---|
| Control group 1 | 33.54 ± 10.08 | 35.58 ± 7.48 |
| Test group 2 | 32.60 ± 13.10 | 38.11 ± 4.60 |
| Total | 33.00 ± 11.61 | 36.67 ± 6.39 |
| NB 1 | BM 2 | ST 3 | ||||
|---|---|---|---|---|---|---|
| Min | Max | Min | Max | Min | Max | |
| Control group | 15.05% | 68.61% | 7.58% | 65.62% | 12.76% | 38.86% |
| Test group | 24.70% | 51.77% | 4.66% | 50.04% | 19.24% | 55.00% |
| NB 1 | BM 2 | ST 3 | |
|---|---|---|---|
| Control group 1 | 41.73 ± 13.99% | 31.72 ± 15.52% | 26.54 ± 7.25% |
| Test group 2 | 39.91 ± 8.49% | 28.61 ± 11.38% | 31.49 ± 11.09% |
| p-value * | p = 0.629 | p = 0.485 | p = 0.113 |
| Antibody | Isotype | Manufacturer | Incubation |
|---|---|---|---|
| Anti-Sp7/Osx 1 | Rabbit polyclonal | Abcam, Cambridge, UK | 1:200, overnight, 4° |
| Anti-BMP-2 2 | Rabbit polyclonal | Abcam, Cambridge, UK | 1:200, overnight, 4° |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomas, M.; Karl, M.; Čandrlić, M.; Matijević, M.; Juzbašić, M.; Peloza, O.C.; Radetić, A.T.J.; Kuiš, D.; Vidaković, B.; Ivanišević, Z.; et al. A Histologic, Histomorphometric, and Immunohistochemical Evaluation of Anorganic Bovine Bone and Injectable Biphasic Calcium Phosphate in Humans: A Randomized Clinical Trial. Int. J. Mol. Sci. 2023, 24, 5539. https://doi.org/10.3390/ijms24065539
Tomas M, Karl M, Čandrlić M, Matijević M, Juzbašić M, Peloza OC, Radetić ATJ, Kuiš D, Vidaković B, Ivanišević Z, et al. A Histologic, Histomorphometric, and Immunohistochemical Evaluation of Anorganic Bovine Bone and Injectable Biphasic Calcium Phosphate in Humans: A Randomized Clinical Trial. International Journal of Molecular Sciences. 2023; 24(6):5539. https://doi.org/10.3390/ijms24065539
Chicago/Turabian StyleTomas, Matej, Matej Karl, Marija Čandrlić, Marko Matijević, Martina Juzbašić, Olga Cvijanović Peloza, Ana Terezija Jerbić Radetić, Davor Kuiš, Bruno Vidaković, Zrinka Ivanišević, and et al. 2023. "A Histologic, Histomorphometric, and Immunohistochemical Evaluation of Anorganic Bovine Bone and Injectable Biphasic Calcium Phosphate in Humans: A Randomized Clinical Trial" International Journal of Molecular Sciences 24, no. 6: 5539. https://doi.org/10.3390/ijms24065539