
Evaluation of the Synovial Effects of Biological and Targeted Synthetic DMARDs in Patients with Psoriatic Arthritis: A Systematic Literature Review and Meta-Analysis
 , , , , , ,
, , , , , ,  , , , , , , and
, , , , , , and
Abstract
:1. Introduction
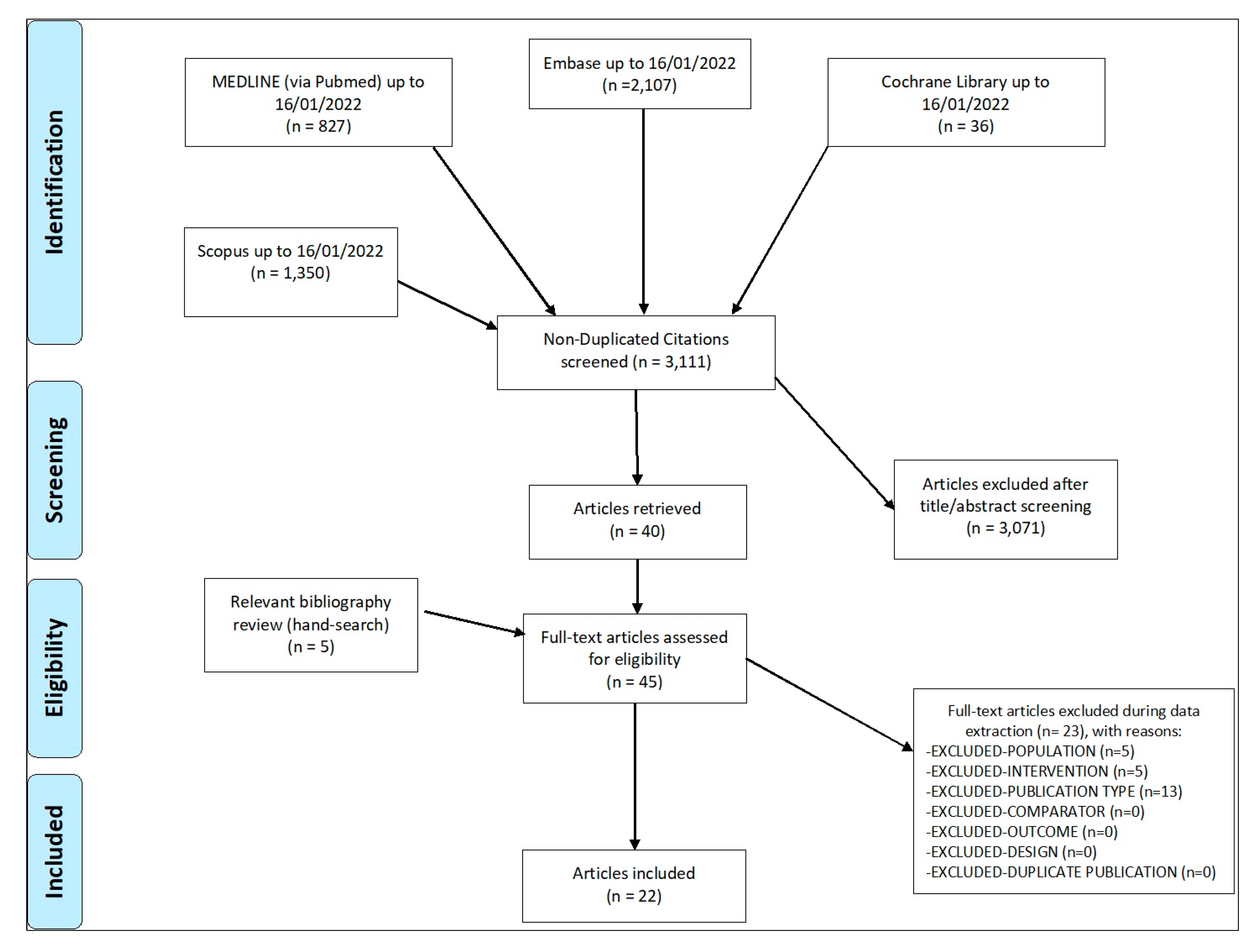
2. Materials and Methods
3. Results and Discussion
3.1. Descriptive Results
3.2. Longitudinal Studies of TNF Inhibitors (Immunohistochemistry—IHC)
3.3. Longitudinal Studies of TNF Inhibitors (Other Techniques)
3.4. Longitudinal Studies of Non-TNF Inhibitors
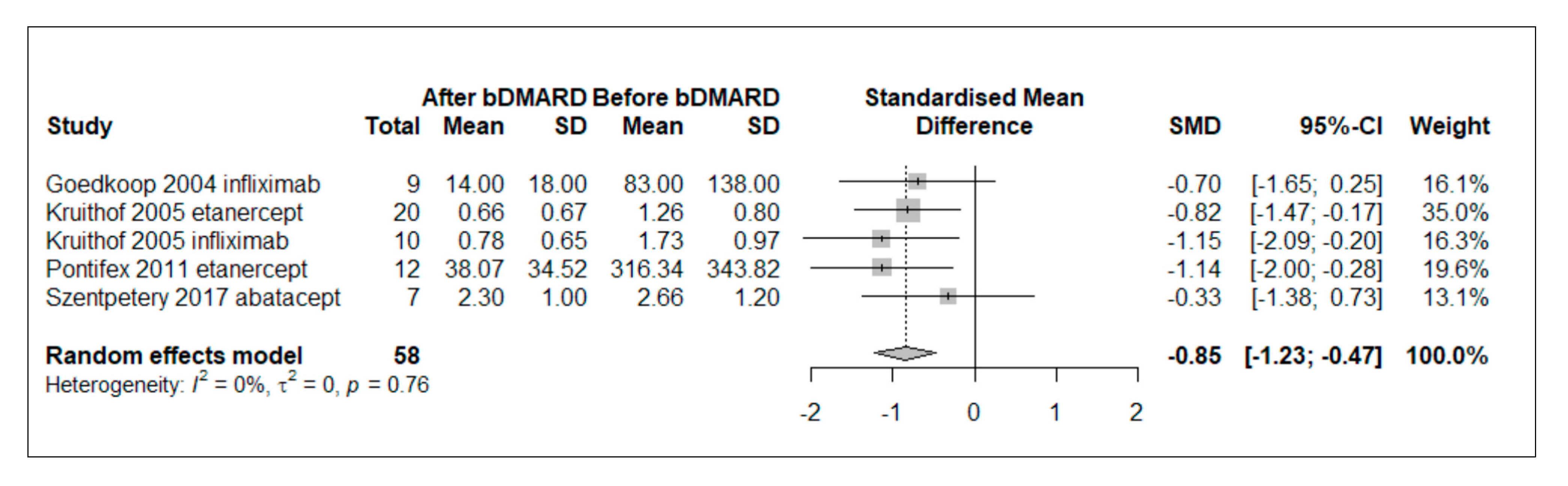
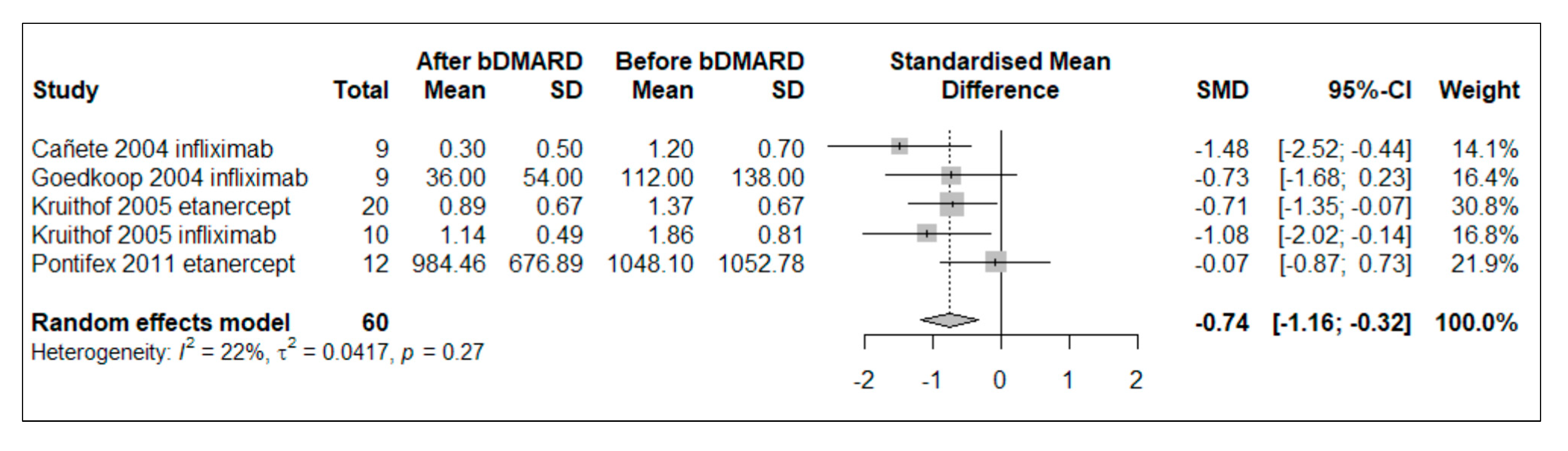
3.5. Meta-Analysis of bDMARD Effect in Longitudinal Studies
3.6. In Vitro Studies
3.7. Biomarkers of Response to Therapy
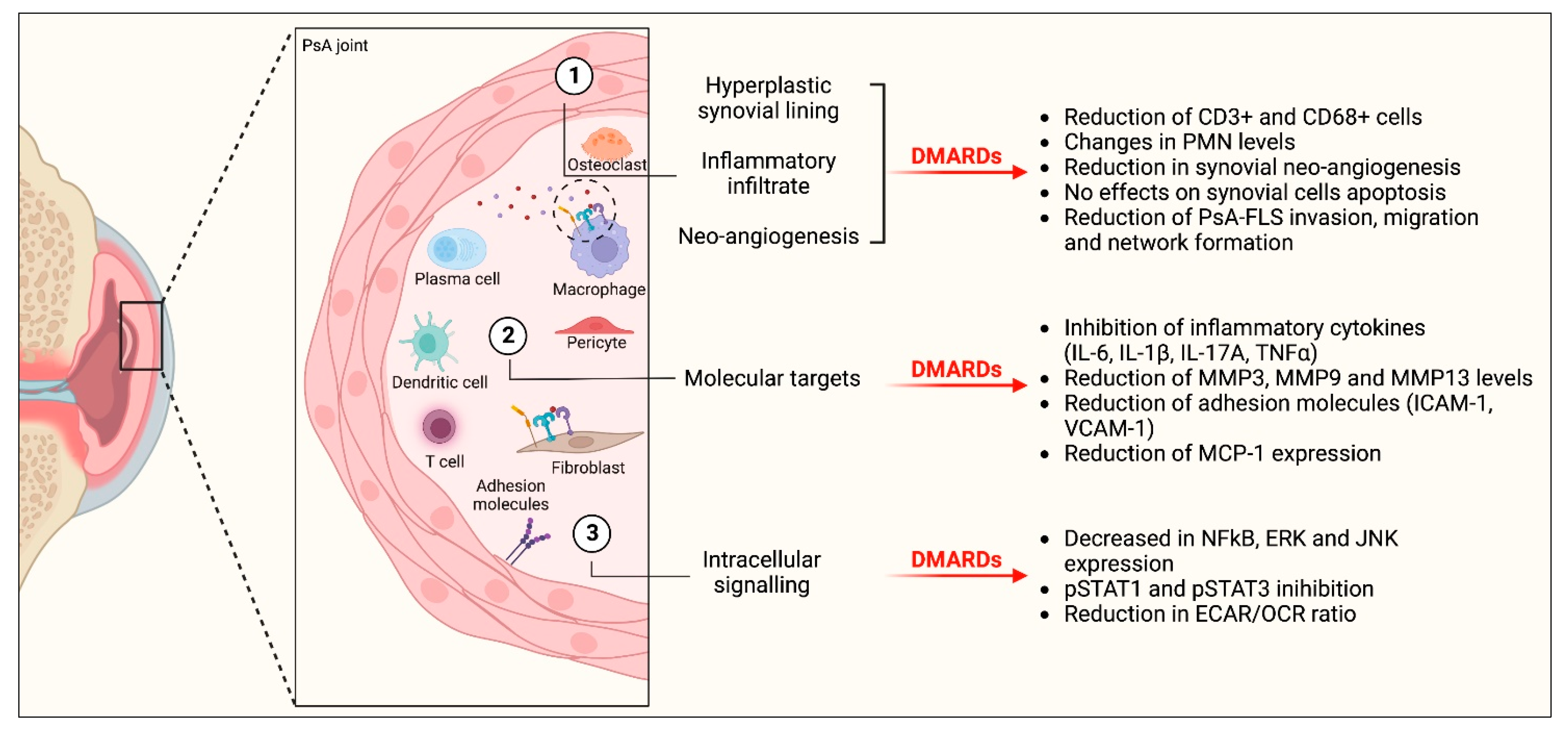
3.8. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Menter, A.; Korman, N.J.; Elmets, C.A.; Feldman, S.R.; Gelfand, J.M.; Gordon, K.B.; Gottlieb, A.; Koo, J.Y.; Lebwohl, M.; Leonardi, C.L.; et al. Guidelines of care for the management of psoriasis and psoriatic arthritis. J. Am. Acad. Dermatol. 2011, 65, 137–174. [Google Scholar] [CrossRef] [PubMed]
- Veale, D.J.; Fearon, U. The pathogenesis of psoriatic arthritis. Lancet 2018, 391, 2273–2284. [Google Scholar] [CrossRef]
- Russel, C.; Hu, R.; Bigler, J.; Boedigheimer, M.; Sullivan, B.; Kricorian, G.; Klekotka, P.; Chung, J.; Newhall, K.; Martin, D. Dissection of Inflammatory Pathways and Molecular Trajectories of Multiple Therapeutics. Exp. Dermatol. 2014, 23, 2. [Google Scholar] [CrossRef] [Green Version]
- Schnell, A.; Littman, D.R.; Kuchroo, V.K. TH17 cell heterogeneity and its role in tissue inflammation. Nat. Immunol. 2023, 24, 19–29. [Google Scholar] [CrossRef] [PubMed]
- Silvagni, E.; Missiroli, S.; Perrone, M.; Patergnani, S.; Boncompagni, C.; Bortoluzzi, A.; Govoni, M.; Giorgi, C.; Alivernini, S.; Pinton, P.; et al. From Bed to Bench and Back: TNF-α, IL-23/IL-17A, and JAK-Dependent Inflammation in the Pathogenesis of Psoriatic Synovitis. Front. Pharmacol. 2021, 12, 672515. [Google Scholar] [CrossRef] [PubMed]
- Silvagni, E.; Bortoluzzi, A.; Ciancio, G.; Govoni, M. Biological and synthetic target DMARDs in psoriatic arthritis. Pharmacol. Res. 2019, 149, 104473. [Google Scholar] [CrossRef]
- Hutton, J.; Mease, P.; Jadon, D. Horizon scan: State-of-the-art therapeutics for psoriatic arthritis. Best Pract. Res. Clin. Rheumatol. 2022, 101809. [Google Scholar] [CrossRef]
- Gossec, L.; Baraliakos, X.; Kerschbaumer, A.; de Wit, M.; McInnes, I.; Dougados, M.; Primdahl, J.; McGonagle, D.G.; Aletaha, D.; Balanescu, A.; et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann. Rheum. Dis. 2020, 79, 700–712. [Google Scholar] [CrossRef] [PubMed]
- Coates, L.C.; Corp, N.; van der Windt, D.A.; O’Sullivan, D.; Soriano, E.R.; Kavanaugh, A. GRAPPA Treatment Recommendations: 2021 Update. J. Rheumatol. 2022, 49, 52–54. [Google Scholar] [CrossRef]
- Magee, C.; Jethwa, H.; FitzGerald, O.M.; Jadon, D.R. Biomarkers predictive of treatment response in psoriasis and psoriatic arthritis: A systematic review. Ther. Adv. Musculoskelet. Dis. 2021, 13, 1759720X2110140. [Google Scholar] [CrossRef]
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Primers 2018, 4, 18001. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.B.M.; Bergstra, S.A.; Kerschbaumer, A.; Sepriano, A.; Aletaha, D.; Caporali, R.; Edwards, C.J.; Hyrich, K.L.; E. Pope, J.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann. Rheum. Dis. 2022, 82, 3–18. [Google Scholar] [CrossRef]
- Garaffoni, C.; Adinolfi, A.; Bortoluzzi, A.; Filippou, G.; Giollo, A.; Sakellariou, G.; Sirotti, S.; Ughi, N.; Scirè, C.A.; Silvagni, E. Novel insights into the management of rheumatoid arthritis: One year in review 2022. Ann. Rheum. Dis. 2022, 40, 1247–1257. [Google Scholar] [CrossRef] [PubMed]
- Generali, E.; Scirè, C.A.; Favalli, E.G.; Selmi, C. Biomarkers in psoriatic arthritis: A systematic literature review. Expert Rev. Clin. Immunol. 2016, 12, 651–660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najm, A.; Goodyear, C.S.; McInnes, I.B.; Siebert, S. Phenotypic heterogeneity in psoriatic arthritis: Towards tissue pathology-based therapy. Nat. Rev. Rheumatol. 2023, 19, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Veale, D.J. Synovial Tissue Biopsy Research. Front. Med. 2019, 6, 72. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- FDA-NIH Biomarker Working Group BEST (Biomarkers, EndpointS, and Other Tools) Resource; Food and Drug Administration (US): Silver Spring, MD, USA, 2021.
- Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 11 September 2021).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res. Methodol. 2014, 14, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Van Kuijk, A.W.R.; Gerlag, D.M.; Vos, K.; Wolbink, G.J.; De Groot, M.; De Rie, M.A.; Zwinderman, A.H.; Dijkmans, B.A.C.; Tak, P.P. A prospective, randomised, placebo-controlled study to identify biomarkers associated with active treatment in psoriatic arthritis: Effects of adalimumab treatment on synovial tissue. Ann. Rheum. Dis. 2008, 68, 1303–1309. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- R: The R Project for Statistical Computing. Available online: https://www.r-project.org/ (accessed on 16 August 2022).
- Cañete, J.D.; Pablos, J.L.; Sanmartí, R.; Mallofré, C.; Marsal, S.; Maymó, J.; Gratacós, J.; Mezquita, J.; Mezquita, C.; Cid, M.C. Antiangiogenic effects of anti-tumor necrosis factor α therapy with infliximab in psoriatic arthritis. Arthritis Rheum. 2004, 50, 1636–1641. [Google Scholar] [CrossRef] [PubMed]
- Bolt, J.; Van Kuijk, A.W.R.; Teunissen, M.B.; De Hair, M.J.H.; Van Der Coelen, D.; Aarrass, S.; Gerlag, D.M.; Tak, P.P.; Van De Sande, M.; Lebre, M.C.; et al. Adalimumab Has No Significant Effect on Interleukin-17 and Interleukin-17 Receptor Expression in Skin and Synovium of Psoriatic Arthritis Patients with Mild Psoriasis. J. Psoriasis Psoriatic Arthritis 2021, 6, 207. [Google Scholar] [CrossRef]
- Pontifex, E.K.; Gerlag, D.M.; Gogarty, M.; Vinkenoog, M.; Gibbs, A.; Burgman, I.; Fearon, U.; Bresnihan, B.; Tak, P.P.; Gibney, R.G.; et al. Change in CD3 Positive T-Cell Expression in Psoriatic Arthritis Synovium Correlates with Change in DAS28 and Magnetic Resonance Imaging Synovitis Scores Following Initiation of Biologic Therapy—A Single Centre, Open-Label Study. Arthritis Res. Ther. 2011, 13, R7. [Google Scholar] [CrossRef] [Green Version]
- Vandooren, B.; Cantaert, T.; Noordenbos, T.; Tak, P.P.; Baeten, D. The abundant synovial expression of the RANK/RANKL/Osteoprotegerin system in peripheral spondylarthritis is partially disconnected from inflammation. Arthritis Rheum. 2008, 58, 718–729. [Google Scholar] [CrossRef]
- Goedkoop, A.Y.; Kraan, M.C.; Teunissen, M.B.M.; Picavet, D.I.; De Rie, M.A.; Bos, J.D.; Tak, P.P. Early Effects of Tumour Necrosis Factor α Blockade on Skin and Synovial Tissue in Patients with Active Psoriasis and Psoriatic Arthritis. Ann. Rheum. Dis. 2004, 63, 769–773. [Google Scholar] [CrossRef] [Green Version]
- Goedkoop, A.Y.; Kraan, M.C.; Picavet, D.I.; de Rie, M.A.; Teunissen, M.B.M.; Bos, J.D.; Tak, P.P. Deactivation of Endothelium and Reduction in Angiogenesis in Psoriatic Skin and Synovium by Low Dose Infliximab Therapy in Combination with Stable Methotrexate Therapy: A Prospective Single-Centre Study. Arthritis Res. Ther. 2004, 6, R326–R334. [Google Scholar] [CrossRef] [Green Version]
- Kruithof, E.; Baeten, D.; van den Bosch, F.; Mielants, H.; Veys, E.M.; De Keyser, F. Histological evidence that infliximab treatment leads to downregulation of inflammation and tissue remodelling of the synovial membrane in spondyloarthropathy. Ann. Rheum. Dis. 2005, 64, 529–536. [Google Scholar] [CrossRef] [Green Version]
- Kruithof, E.; De Rycke, L.; Roth, J.; Mielants, H.; Bosch, F.V.D.; De Keyser, F.; Veys, E.M.; Baeten, D. Immunomodulatory effects of etanercept on peripheral joint synovitis in the spondylarthropathies. Arthritis Rheum. 2005, 52, 3898–3909. [Google Scholar] [CrossRef] [PubMed]
- Kruithof, E.; De Rycke, L.; Vandooren, B.; De Keyser, F.; FitzGerald, O.; McInnes, I.; Tak, P.P.; Bresnihan, B.; Veys, E.M.; Baeten, D.; et al. Identification of synovial biomarkers of response to experimental treatment in early-phase clinical trials in spondylarthritis. Arthritis Rheum. 2006, 54, 1795–1804. [Google Scholar] [CrossRef] [PubMed]
- De Rycke, L.; Baeten, D.; Foell, D.; Kruithof, E.; Veys, E.M.; Roth, J.; De Keyser, F. Differential expression and response to anti-TNFα treatment of infiltrating versus resident tissue macrophage subsets in autoimmune arthritis. J. Pathol. 2005, 206, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Lories, R.J.U.; Derese, I.; Luyten, F.P.; De Vlam, K. Activation of nuclear factor kappa B and mitogen activated protein kinases in psoriatic arthritis before and after etanercept treatment. Ann. Rheum. Dis. 2008, 26, 96–102. [Google Scholar]
- Cañete, J.D.; Santiago, B.; Cantaert, T.; Sanmartí, R.; Palacin, A.; Celis, R.; Graell, E.; Gil-Torregrosa, B.; Baeten, D.; Pablos, J.L. Ectopic lymphoid neogenesis in psoriatic arthritis. Ann. Rheum. Dis. 2007, 66, 720–726. [Google Scholar] [CrossRef] [Green Version]
- Ramos, M.I.; Teunissen, M.B.M.; Helder, B.; Aarrass, S.; De Hair, M.J.H.; Van Kuijk, A.W.; Gerlag, D.M.; Tak, P.P.; Lebre, M.C. Reduced CLEC9A expression in synovial tissue of psoriatic arthritis patients after adalimumab therapy. Rheumatology 2016, 55, 1575–1584. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, E.S.; Butt, A.Q.; Gibson, D.S.; Dunn, M.J.; Fearon, U.; van Kuijk, A.W.; Gerlag, D.M.; Pontifex, E.; Veale, D.J.; Tak, P.P.; et al. A clinically based protein discovery strategy to identify potential biomarkers of response to anti-TNF-α treatment of psoriatic arthritis. Proteom.—Clin. Appl. 2015, 10, 645–662. [Google Scholar] [CrossRef]
- Szentpetery, A.; Heffernan, E.; Gogarty, M.; Mellerick, L.; McCormack, J.; Haroon, M.; Elmamoun, M.; Gallagher, P.; Kelly, G.; Fabre, A.; et al. Abatacept Reduces Synovial Regulatory T-Cell Expression in Patients with Psoriatic Arthritis. Arthritis. Res. Ther. 2017, 19, 1–11. [Google Scholar] [CrossRef]
- Fiechter, R.H.; de Jong, H.M.; van Mens, L.J.J.; Fluri, I.A.; Tas, S.W.; Baeten, D.L.P.; Yeremenko, N.G.; van de Sande, M.G.H. IL-12p40/IL-23p40 Blockade With Ustekinumab Decreases the Synovial Inflammatory Infiltrate Through Modulation of Multiple Signaling Pathways Including MAPK-ERK and Wnt. Front. Immunol. 2021, 12, 611656. [Google Scholar] [CrossRef]
- Mens, L.J.J.; Sande, M.G.H.; Menegatti, S.; Chen, S.; Blijdorp, I.C.J.; Jong, H.M.; Fluri, I.A.; Latuhihin, T.E.; Kuijk, A.W.R.; Rogge, L.; et al. Brief Report: Interleukin-17 Blockade With Secukinumab in Peripheral Spondyloarthritis Impacts Synovial Immunopathology Without Compromising Systemic Immune Responses. Arthritis Rheumatol. 2018, 70, 1994–2002. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.; Noordenbos, T.; Blijdorp, I.; Van Mens, L.; Ambarus, C.A.; Vogels, E.; Velde, A.T.; Alsina, M.; Cañete, J.D.; Yeremenko, N.; et al. Histologic evidence that mast cells contribute to local tissue inflammation in peripheral spondyloarthritis by regulating interleukin-17A content. Rheumatology 2018, 58, 617–627. [Google Scholar] [CrossRef]
- Gao, W.; McGarry, T.; Orr, C.; McCormick, J.; Veale, D.J.; Fearon, U. Tofacitinib regulates synovial inflammation in psoriatic arthritis, inhibiting STAT activation and induction of negative feedback inhibitors. Ann. Rheum. Dis. 2015, 75, 311–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Brien, A.; Hanlon, M.M.; Marzaioli, V.; Wade, S.C.; Flynn, K.; Fearon, U.; Veale, D.J. Targeting JAK-STAT Signalling Alters PsA Synovial Fibroblast Pro-Inflammatory and Metabolic Function. Front. Immunol. 2021, 12, 672461. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Davelaar, N.; Mus, A.; Asmawidjaja, P.S.; Hazes, J.M.W.; Baeten, D.L.P.; Vis, M.; Bisoendial, R.J.; Prens, E.P.; Lubberts, E. Interleukin-17A Is Produced by CD4+ but Not CD8+ T Cells in Synovial Fluid Following T Cell Receptor Activation and Regulates Different Inflammatory Mediators Compared to Tumor Necrosis Factor in a Model of Psoriatic Arthritis Synovitis. Arthritis Rheumatol. 2020, 72, 1303–1313. [Google Scholar] [CrossRef] [Green Version]
- Sancho, D.; Joffre, O.P.; Keller, A.M.; Rogers, N.C.; Martínez, D.; Hernanz-Falcón, P.; Rosewell, I.; Reis, E.; Sousa, C. Identification of a dendritic cell receptor that couples sensing of necrosis to immunity. Nature 2009, 458, 899–903. [Google Scholar] [CrossRef] [Green Version]
- Sweeney, S.E.; Firestein, G.S. Signal Transduction in Rheumatoid Arthritis. Curr. Opin. Rheumatol. 2004, 16, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Schöls, M.; Braun, J.; Dougados, M.; FitzGerald, O.; Gladman, D.D.; Kavanaugh, A.; Landewé, R.; Mease, P.; Sieper, J.; et al. Treating axial spondyloarthritis and peripheral spondyloarthritis, especially psoriatic arthritis, to target: 2017 update of recommendations by an international task force. Ann. Rheum. Dis. 2017, 77, 3–17. [Google Scholar] [CrossRef] [Green Version]
- Najm, A.; Orr, C.; Heymann, M.-F.; Bart, G.; Veale, D.; Le Goff, B. Success Rate and Utility of Ultrasound-guided Synovial Biopsies in Clinical Practice. J. Rheumatol. 2016, 43, 2113–2119. [Google Scholar] [CrossRef]
- Humby, F.; Kelly, S.; Bugatti, S.; Manzo, A.; Filer, A.; Mahto, A.; Fonseca, J.E.; Lauwerys, B.; D’Agostino, M.-A.; Naredo, E.; et al. Evaluation of Minimally Invasive, Ultrasound-guided Synovial Biopsy Techniques by the OMERACT Filter—Determining Validation Requirements. J. Rheumatol. 2015, 43, 208–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lazarou, I.; D’Agostino, M.-A.; Naredo, E.; Humby, F.; Filer, A.; Kelly, S.G. Ultrasound-guided synovial biopsy: A systematic review according to the OMERACT filter and recommendations for minimal reporting standards in clinical studies. Rheumatology 2015, 54, 1867–1875. [Google Scholar] [CrossRef] [Green Version]
- Nerviani, A.; Di Cicco, M.; Mahto, A.; Lliso-Ribera, G.; Rivellese, F.; Thorborn, G.; Hands, R.; Bellan, M.; Mauro, D.; Boutet, M.-A.; et al. A Pauci-Immune Synovial Pathotype Predicts Inadequate Response to TNFα-Blockade in Rheumatoid Arthritis Patients. Front. Immunol. 2020, 11, 845. [Google Scholar] [CrossRef]
- Wang, J.; Conlon, D.; Rivellese, F.; Nerviani, A.; Lewis, M.J.; Housley, W.; Levesque, M.C.; Cao, X.; Cuff, C.; Long, A.; et al. Synovial Inflammatory Pathways Characterize Anti-TNF –Responsive Rheumatoid Arthritis Patients. Arthritis Rheumatol. 2022, 74, 1916–1927. [Google Scholar] [CrossRef]
- Haringman, J.J.; Gerlag, D.M.; Zwinderman, A.H.; Smeets, T.J.M.; Kraan, M.C.; Baeten, D.; McInnes, I.; Bresnihan, B.; Tak, P.P. Synovial tissue macrophages: A sensitive biomarker for response to treatment in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2005, 64, 834–838. [Google Scholar] [CrossRef]
- Taylor, P.C.; Peters, A.M.; Paleolog, E.; Chapman, P.T.; Elliott, M.J.; McCloskey, R.; Feldmann, M.; Maini, R.N. Reduction of Chemokine Levels and Leukocyte Traffic to Joints by Tumor Necrosis Factor Alpha Blockade in Patients with Rheumatoid Arthritis. Arthritis Rheum. 2000, 43, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Vordenbäumen, S.; Sewerin, P.; Lögters, T.; Miese, F.; Schleich, C.; Bleck, E.; Philippski, P.; Schädel-Höpfner, M.; Pauly, T.; Schneider, M.; et al. Inflammation and vascularisation markers of arthroscopically-guided finger joint synovial biospies reflect global disease activity in rheumatoid arthritis. Ann. Rheum. Dis. 2014, 32, 117–120. [Google Scholar]
- Orr, C.; Vieira-Sousa, E.; Boyle, D.L.; Buch, M.; Buckley, C.D.; Cañete, J.D.; Catrina, A.I.; Choy, E.H.S.; Emery, P.; Fearon, U.; et al. Synovial tissue research: A state-of-the-art review. Nat. Rev. Rheumatol. 2017, 13, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Pitzalis, C. Can Pathobiology Inform Disease Outcome and Response to Therapy? Rheumatology 2011, 50, iii22. [Google Scholar]
- Pitzalis, C.; Choy, E.H.S.; Buch, M.H. Transforming clinical trials in rheumatology: Towards patient-centric precision medicine. Nat. Rev. Rheumatol. 2020, 16, 590–599. [Google Scholar] [CrossRef] [PubMed]
- Alivernini, S.; MacDonald, L.; Elmesmari, A.; Finlay, S.; Tolusso, B.; Gigante, M.R.; Petricca, L.; Di Mario, C.; Bui, L.; Perniola, S.; et al. Distinct synovial tissue macrophage subsets regulate inflammation and remission in rheumatoid arthritis. Nat. Med. 2020, 26, 1295–1306. [Google Scholar] [CrossRef] [PubMed]
- Rivellese, F.; Pitzalis, C. Cellular and molecular diversity in Rheumatoid Arthritis. Semin. Immunol. 2021, 58, 101519. [Google Scholar] [CrossRef]
- Najm, A.; Le Goff, B.; Orr, C.; Thurlings, R.; Canete, J.D.; Humby, F.; Alivernini, S.; Manzo, A.; Just, S.A.; Romao, V.C.; et al. Standardisation of synovial biopsy analyses in rheumatic diseases: A consensus of the EULAR Synovitis and OMERACT Synovial Tissue Biopsy Groups. Arthritis Res. Ther. 2018, 20, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najm, A.; Costantino, F.; Alivernini, S.; Alunno, A.; Bianchi, E.; Bignall, J.; Boyce, B.; Cañete, J.D.; Carubbi, F.; Durez, P.; et al. EULAR points to consider for minimal reporting requirements in synovial tissue research in rheumatology. Ann. Rheum. Dis. 2022, 81, 1640–1646. [Google Scholar] [CrossRef]
- Krenn, V.; Morawietz, L.; Burmester, G.-R.; Kinne, R.W.; Mueller-Ladner, U.; Muller, B.; Haupl, T. Synovitis score: Discrimination between chronic low-grade and high-grade synovitis. Histopathology 2006, 49, 358–364. [Google Scholar] [CrossRef]
- Alivernini, S.; Tolusso, B.; Petricca, L.; Bui, L.; Di Sante, G.; Peluso, G.; Benvenuto, R.; Fedele, A.L.; Federico, F.; Ferraccioli, G.; et al. Synovial features of patients with rheumatoid arthritis and psoriatic arthritis in clinical and ultrasound remission differ under anti-TNF therapy: A clue to interpret different chances of relapse after clinical remission? Ann. Rheum. Dis. 2017, 76, 1228–1236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuret, T.; Sodin-Šemrl, S.; Leskošek, B.; Ferk, P. Single Cell RNA Sequencing in Autoimmune Inflammatory Rheumatic Diseases: Current Applications, Challenges and a Step Toward Precision Medicine. Front. Med. 2022, 8, 3067. [Google Scholar] [CrossRef] [PubMed]
- McGarry, T.; Orr, C.; Wade, S.; Biniecka, M.; Wade, S.; Gallagher, L.; Low, C.; Veale, D.; Fearon, U. JAK/STATBlockade Alters Synovial Bioenergetics, Mitochondrial Function, and Proinflammatory Mediators in Rheumatoid Arthritis. Arthritis Rheumatol. 2018, 70, 1959–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humby, F.; Durez, P.; Buch, M.H.; Lewis, M.J.; Rizvi, H.; Rivellese, F.; Nerviani, A.; Giorli, G.; Mahto, A.; Montecucco, C.; et al. Rituximab versus tocilizumab in anti-TNF inadequate responder patients with rheumatoid arthritis (R4RA): 16-week outcomes of a stratified, biopsy-driven, multicentre, open-label, phase 4 randomised controlled trial. Lancet 2021, 397, 305–317. [Google Scholar] [CrossRef] [PubMed]
- Rivellese, F.; Surace, A.E.A.; Goldmann, K.; Sciacca, E.; Çubuk, C.; Giorli, G.; John, C.R.; Nerviani, A.; Fossati-Jimack, L.; Thorborn, G.; et al. Rituximab versus tocilizumab in rheumatoid arthritis: Synovial biopsy-based biomarker analysis of the phase 4 R4RA randomized trial. Nat. Med. 2022, 28, 1256–1268. [Google Scholar] [CrossRef] [PubMed]
- Bolt, J.W.; van Kuijk, A.W.; Teunissen, M.B.M.; van der Coelen, D.; Aarrass, S.; Gerlag, D.M.; Tak, P.P.; van de Sande, M.G.; Lebre, M.C.; van Baarsen, L.G.M. Impact of Adalimumab Treatment on Interleukin-17 and Interleukin-17 Receptor Expression in Skin and Synovium of Psoriatic Arthritis Patients with Mild Psoriasis. Biomedicines 2022, 10, 324. [Google Scholar] [CrossRef]
- Fiocco, U.; Sfriso, P.; Oliviero, F.; Roux-Lombard, P.; Lunardi, F.; Calabrese, F.; Nardacchione, R. Synovial Fluid and Synovial Tissue Biomarkers of the Response to Intra-Articular TNF-Blockade in Psoriatic Arthritis. Arthritis Rheum. 2009, 60, 1346. [Google Scholar] [CrossRef]
- Fiocco, U.; Oliviero, F.; Sfriso, P.; Calabrese, F.; Lunardi, F.; Scagliori, E.; Rubaltelli, L.; Stramare, R.; Di Maggio, A.; Nardacchione, R.; et al. Synovial Biomarkers in Psoriatic Arthritis. J. Rheumatol. 2012, 89, 61–64. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Frequency |
|---|---|
| Study type | |
| In vitro studies, N (%) | 3 (13.6) |
| Longitudinal studies, N (%) | 19 (86.4) |
| Characteristics of population and disease | |
| Number of participants, mean (SD) | 17.2 (10.5) |
| Number of female participants, mean (SD) | 8.3 (5.5) |
| Age, mean (SD) | 45.8 (4.3) |
| PsA disease duration in months, mean (SD) | 88.0 (40.8) |
| PsO disease duration in months, mean (SD) | 234 (25.5) |
| Duration of follow-up in weeks, mean (SD) | 11.0 (6.4) |
| Drug tested | |
| Infliximab, N (%) | 8 (36.4) |
| Etanercept, N (%) | 7 (31.8) |
| Adalimumab, N (%) | 5 (22.7) |
| Secukinumab, N (%) | 3 (13.6) |
| Ustekinumab, N (%) | 1 (4.6) |
| Tofacitinib, N (%) | 1 (4.6) |
| Upadacitinib, N (%) | 1 (4.6) |
| Abatacept, N (%) | 1 (4.6) |
| Synovial biopsy | |
| Site of biopsy: Knee, N (%) | 17 (77.3) |
| Site of biopsy: Wrist, N (%) | 5 (22.7) |
| Site of biopsy: Ankle, N (%) | 5 (22.7) |
| Technique: Arthroscopic synovial biopsy, N (%) | 20 (90.9) |
| Technique: Blind needle biopsy, N (%) | 1 (4.6) |
| Technique: US-guided, N (%) | 0 |
| Technique: Arthrotomy, N (%) | 0 |
| Type of laboratory technique assessed | |
| Immunohistochemistry, N (%) | 17 (77.3) |
| mRNA extraction and RT-PCR, N (%) | 6 (27.3) |
| ELISA, N (%) | 5 (22.7) |
| Optical microscopy analysis, N (%) | 7 (31.8) |
| Immunofluorescence staining, N (%) | 3 (13.6) |
| Western blot, N (%) | 2 (9.1) |
| TUNEL assay, N (%) | 1 (4.6) |
| Migration, invasion, Matrigel network, N (%) | 2 (9.1) |
| Cellular bioenergetic function analysis, N (%) | 1 (4.6) |
| Gene ontology analysis, N (%) | 1 (4.6) |
| Mass spectrometry, N (%) | 1 (4.6) |
| Cellular population assessed | |
| FLS or subpopulations, N (%) | 4 (18.2) |
| T cells or subpopulations, N (%) | 13 (59.1) |
| B cells or subpopulations, N (%) | 8 (36.4) |
| Macrophages or subpopulations, N (%) | 11 (50.0) |
| Mast cells or subpopulations, N (%) | 2 (9.1) |
| Endothelial cells or subpopulations, N (%) | 5 (22.7) |
| Synovial explants, N (%) | 1 (4.6) |
| Article | Year | Study Design | Number of Participants | PsA Disease Duration (Mean Months) | Drug Adopted | Mean Duration of the Follow-Up (Main Outcome–Weeks) | Type of Laboratory Technique Assessed | Main Results |
|---|---|---|---|---|---|---|---|---|
| van Kuijk A [23] | 2009 | RCT | 24 | 66 | adalimumab | 12 | IHC | ↓ CD3+-positive T cell infiltration and expression of MMP13. |
| Cañete [27] | 2004 | Cohort | 9 | 120 | infliximab | 8 | IHC Histologic evaluation mRNA extraction/RT-PCR | ↓ CD68 + sl macrophages ↓ SDF-1 in vessels, neovessels and VEGF, VEGFR-2 ↓ vascular score in sequential biopsies ↓ VEGF and VEGFR2 mRNA expression and increase in Ang-2 |
| Bolt [28] | 2021 | Cohort | 12 | 106 | adalimumab | 4 | IHC | no change in IL- 17A, IL-17F, IL-17RA and IL-17RC |
| Pontifex [29] | 2011 | Cohort | 15 | 90 | etanercept | 12 | IHC | ↓ CD3+ T cells in responders to etanercept |
| Vandooren [30] | 2008 | Cohort | 11 | 60 (median) | etanercept, adalimumab | 12 | IHC | no changes in synovial RANKL, OPG, and RANK expression |
| Goedkoop [31] | 2004 | RCT | 12 | - | infliximab | 0.2 | IHC TUNEL assay | ↓ total number of T cells and CD68 no effect of TNFis on synovial cell apoptosis |
| Goedkoop [32] | 2004 | Cohort | 11 | 108 | infliximab | 4 | IHC | ↓ CD3+ T cells and CD68+ macrophages in synovial tissue ↓ synovial neo-angiogenesis (downregulation of both vWF and αvβ3-positive vessels, VEGF) ↓ adhesion molecules (ICAM-1) |
| Kruithof [33] | 2005 | RCT | 13 for study population I; 20 for study pop. II | 168 for study population I; 222 for study population II | infliximab | 12 | IHC Histologic evaluation | ↓ neutrophils, macrophages, and T cells, but not B cells ↓ synovial lining layer thickness, endothelial activation and number of blood vessels, downregulation of follicular structures organization |
| Kruithof [34] | 2005 | Cohort | 20 | 60 | etanercept | 52 | IHC Histologic evaluation | ↓ global cellular infiltration, T lymphocytes, macrophages subsets (CD68+, CD163, MRP-8, and MRP-14) ↓ lining layer hyperplasia, moderate reduction in vascularity ↓ synovial expression of MMP3 and MMP9 |
| Kruithof [35] | 2006 | Cohort | 20 treated with infliximab 20 treated with etanercept 12 controls | 52 | infliximab and etanercept | 12 | IHC Histologic evaluation | changes in synovial macrophage subsets, PMN levels, and MMP3 expression in responders to treatment vs. non-responders no significant difference between responders and non-responders regarding synovial histology modification |
| de Rycke [36] | 2005 | Cohort | 40 with SpA | 78 | infliximab | 12 | IHC Histologic evaluation | ↓ infiltrating macrophages as demonstrated by the change in the expression of myeloid-related protein in both the lining layer and the sublining layer (MRP-4, MRP-8) |
| Lories [37] | 2008 | Case-series | 9 | 109.3 | etanercept | 26 | Histologic evaluation Immunofluorescence staining | ↓ lining layer hyperplasia and normalization of sublining vascularity. ↓ cell infiltration and lymphoid follicles ↓ NFkB, ERK, JNK but no variation in p38 |
| Canete [38] | 2007 | Cohort | 27 | 82.6 | infliximab | 12 | Histologic evaluation IHC | ↓ ectopic lymphoid neogenesis |
| Ramos [39] | 2016 | RCT | 24 | - | adalimumab | 4 | ICH, mRNA extraction/RT-PCR | ↓ CLEC9A expression in PsA synovial tissue in the adalimumab treated group compared with placebo after 4 weeks |
| Collins [40] | 2016 | Cohort | 12 | - | etanercept, adalimumab | 12 | Mass spectrometry | 119 different protein spots changed significantly (etanercept treatment) including haptoglobin, annexin A2, serum amyloid P, peroxiredoxin 6, serum albumin, Ig kappa chain C, fibrinogen beta chain 91 different protein spots changed significantly (adalimumab treatment) including haptoglobin, serum albumin, ubiquitin conjugating enzyme E2, annexin A1, A2 and A6, serum amyloid P, heat shock cognate 71 kDa protein, fibrinogen beta chain, pyruvate kinase isozymes M1/M2, collagen alpha 3 and cathepsin B |
| Szentpetery [41] | 2017 | RCT | 15 | 120 | abatacept | 8 | IHC Dual IF staining | ↓ FOXP3+ T-cells in the synovium = CD4+, CD3+, CD31+, CD8+ |
| Fiechter [42] | 2021 | Cohort | 11 | - | ustekinumab | 24 | IHC mRNA extraction RT-PCR Gene ontology analysis | ↓ CD68 + sl at 12 weeks, but not at 24 weeks ↓ expression of IL23A mRNA at 12 weeks but not at 24 weeks ↓ MMP3 levels at 12 weeks interference with chemotaxis and neo-angiogenesis pathways, wnt-signaling and PI3K-Akt-mTOR and MAPK-ERK pathways |
| van Mens [43] | 2018 | Cohort | 20 | 66 (median) | secukinumab | 12 | IHC mRNA extraction/RT-PCR | ↓ CD15+ neutrophils and CD68 + sl macrophages ↓ synovial mRNA expression of IL-6, MMP3, CCL20 and IL-17A; = synovial mRNA expression of TNF |
| Chen [44] | 2019 | Cohort | 15 | -- | secukinumab | 12 | IHC | ↑ IL-17A-positive mast cells ↓ all IL-17A-positive cells (non-mast cells) |
| Article | Year | Study Design | Number of Participants | PsA Disease Duration (Mean Months) | Drug Adopted | Type of Laboratory Technique Assessed | Main Results |
|---|---|---|---|---|---|---|---|
| Gao [45] | 2016 | Cohort | 11 | - | tofacitinib | Western blot ELISA Invasion, migration and Matrigel network formation assays | ↓ pSTAT1, pSTAT3 (FLS), NFkBp65 (FLS, synovial explants) ↑ SOCS3 and PIAS3 (FLS) ↓ IL-6, IL-8, MCP-1, MMP3, MMP2/9 (synovial explants) ↓ PsA-FLS invasion, migration, network formation. |
| O’Brien [46] | 2021 | Cohort | 14 | 11.7 | upadacitinib | ELISA mRNA extraction and RT-PCR Invasion, migration assays Cellular bioenergetic function analysis | ↓ expression of IL-6, MCP-1, and ICAM-1 (FLS) ↓ migration capacity of PsA FLS ↓ ECAR/OCR ratio |
| Xu [47] | 2020 | Cohort | 20 | - | secukinumab, adalimumab | ELISA and RT-PCR (co-cultures of CD4+ T cells and FLS) | ↓ IL- 6 and IL- 1β after secukinumab/adalimumab ↓ TNF, MMP3 and MMP13 after adalimumab ↓ IL-17A and IL-6 after secukinumab. |
| Selection | Comparability | Exposure/Outcome | Total | |
|---|---|---|---|---|
| Bolt, 2021 [28] | ★★ | - | - | 2 |
| Cañete, 2007 [38] | ★★ | ★ | ★★ | 5 |
| Cañete, 2004 [27] | ★★★★ | ★★ | ★★★ | 9 |
| Chen, 2019 [44] | ★ | - | ★★ | 3 |
| Collins, 2016 [40] | ★★ | - | ★★ | 4 |
| de Rycke, 2005 [36] | ★★ | ★★ | ★ | 5 |
| Fiechter, 2021 [42] | ★★★★ | ★ | ★★★ | 8 |
| Gao, 2016 [45] | ★★★★ | ★★ | ★★★ | 9 |
| Goedkoop, 2004 [32] | ★★★ | - | ★★★ | 6 |
| Kruithof, 2005 [34] | ★ | - | ★★ | 3 |
| Kruithof, 2006 [35] | ★★★ | - | ★★ | 5 |
| Lories, 2008 [37] | ★★★ | - | ★★★ | 6 |
| O’Brien, 2021 [46] | ★★ | ★ | ★★ | 5 |
| Pontifex, 2011 [29] | ★★★ | - | ★★★ | 6 |
| van Mens, 2018 [43] | ★★ | - | ★★ | 4 |
| Vandooren, 2008 [30] | ★★ | - | ★ | 3 |
| Xu, 2020 [47] | ★ | - | ★★ | 3 |
| Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | |
|---|---|---|---|---|---|
| Goedkoop, 2004 [31] |  | | | |  |
| Kruithof, 2005 [33] | | | | | |
| Ramos, 2016 [39] | | | | | |
| Szentpetery, 2017 [41] | | | | | |
| van Kuijk, 2009 [23] | | | | | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciliento, M.S.; Venturelli, V.; Schettini, N.; Bertola, R.; Garaffoni, C.; Lanza, G.; Gafà, R.; Borghi, A.; Corazza, M.; Zabotti, A.; et al. Evaluation of the Synovial Effects of Biological and Targeted Synthetic DMARDs in Patients with Psoriatic Arthritis: A Systematic Literature Review and Meta-Analysis. Int. J. Mol. Sci. 2023, 24, 5006. https://doi.org/10.3390/ijms24055006
Ciliento MS, Venturelli V, Schettini N, Bertola R, Garaffoni C, Lanza G, Gafà R, Borghi A, Corazza M, Zabotti A, et al. Evaluation of the Synovial Effects of Biological and Targeted Synthetic DMARDs in Patients with Psoriatic Arthritis: A Systematic Literature Review and Meta-Analysis. International Journal of Molecular Sciences. 2023; 24(5):5006. https://doi.org/10.3390/ijms24055006
Chicago/Turabian StyleCiliento, Maria Sofia, Veronica Venturelli, Natale Schettini, Riccardo Bertola, Carlo Garaffoni, Giovanni Lanza, Roberta Gafà, Alessandro Borghi, Monica Corazza, Alen Zabotti, and et al. 2023. "Evaluation of the Synovial Effects of Biological and Targeted Synthetic DMARDs in Patients with Psoriatic Arthritis: A Systematic Literature Review and Meta-Analysis" International Journal of Molecular Sciences 24, no. 5: 5006. https://doi.org/10.3390/ijms24055006