
Interleukin-6 and Macular Edema: A Review of Outcomes with Inhibition

Abstract
:1. Introduction
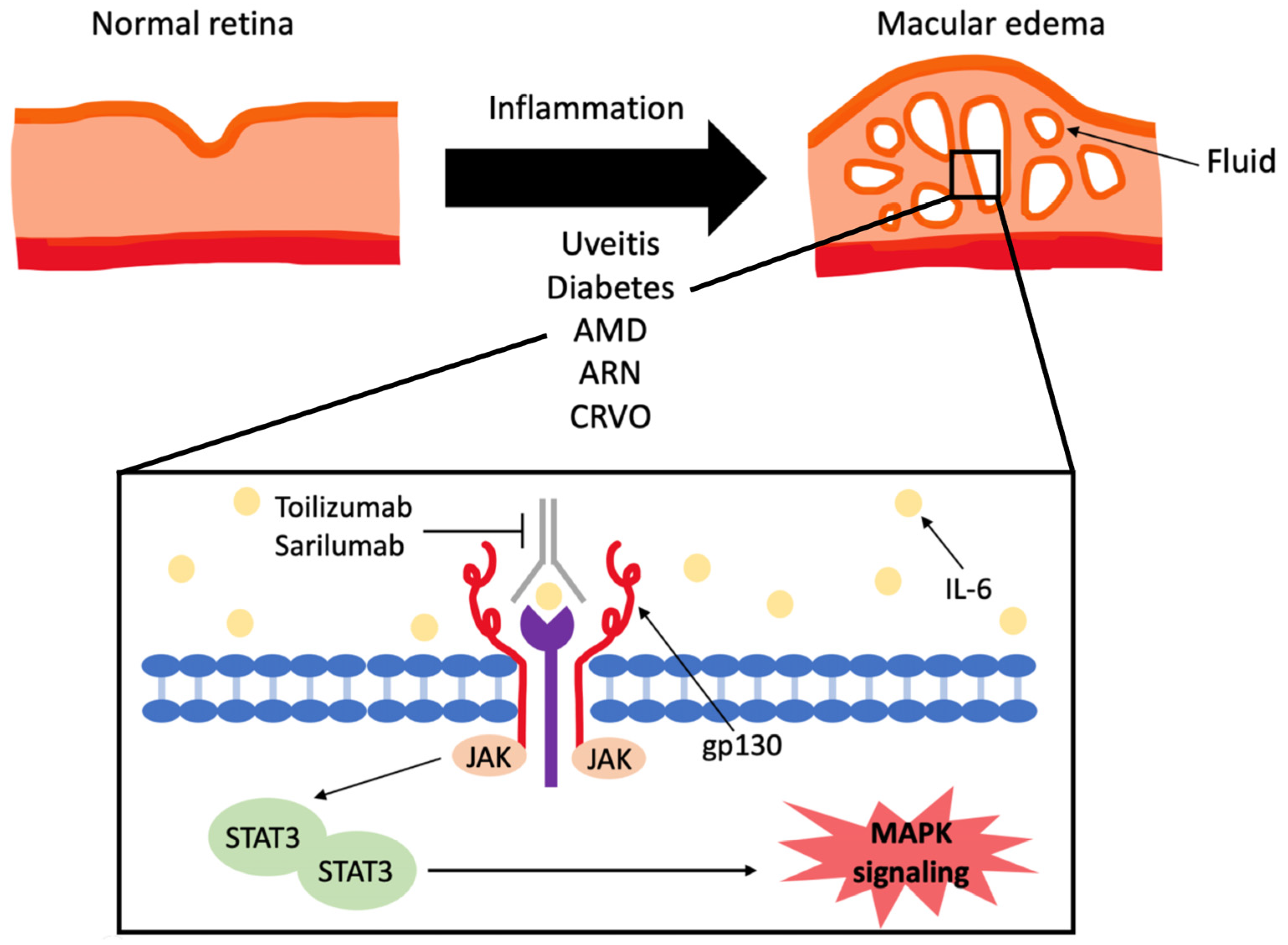
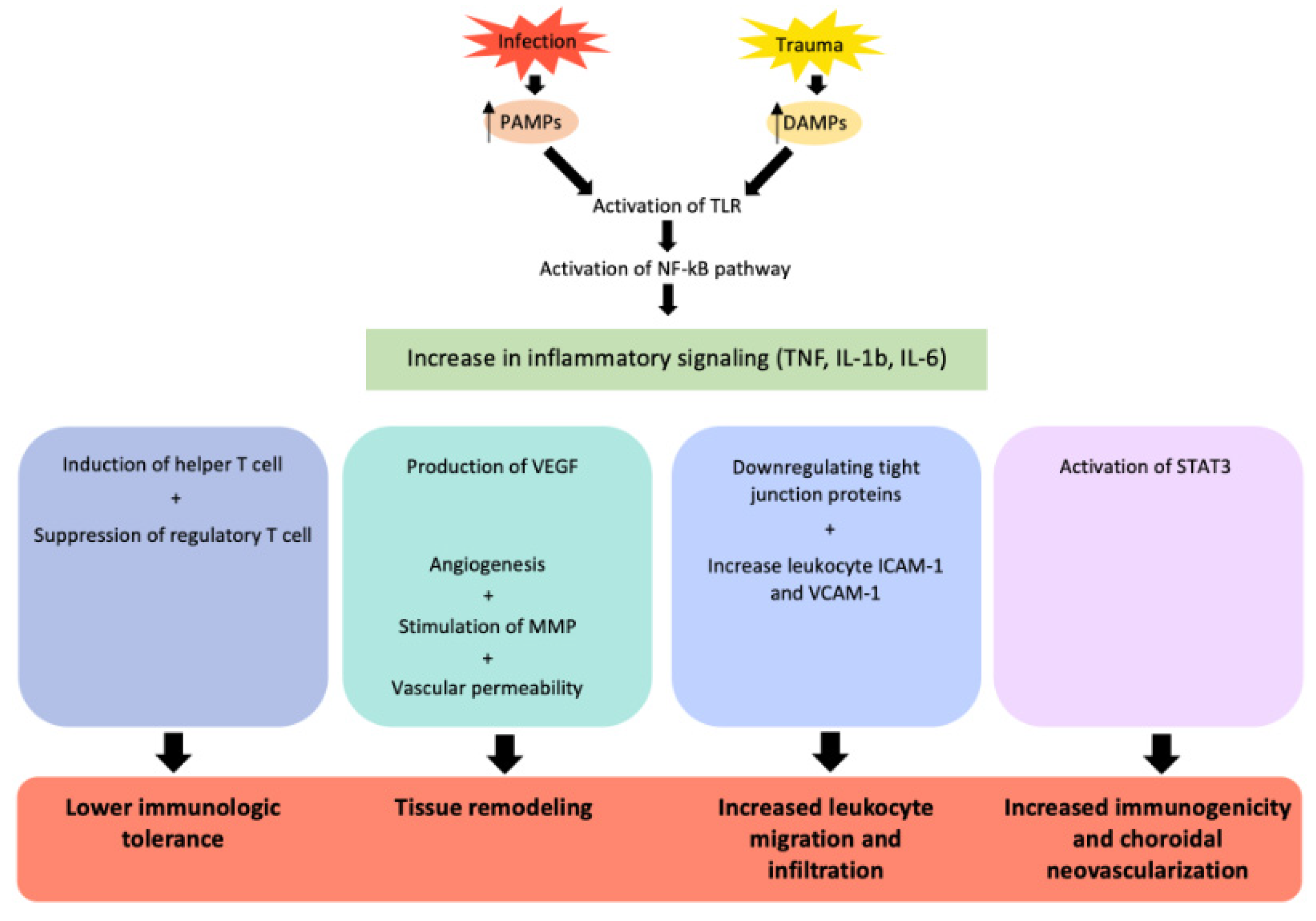
2. The Role of Interleukin-6 in Ocular Pathology
3. Interleukin-6 Blockage in Non-Infectious Uveitis and Its Associated Macular Edema
3.1. Randomized Clinical Trials

{kind=link}
{kind=link}
| First Author | Medication (Administration) | Year | Study Type | Study Objective | # Patients | Type of Uveitis | Follow up Time (Months) | Primary Outcome Measure | % of Primary Efficacy | % of Improvement in ME * | Definition of Improvement in ME * |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Leclercq [17] | TCZ (IV) | 2021 | CS | Efficacy of TNF-alpha agents or TCZ in treating refractory uveitic macular edema | 204 | Idiopathic (97), BD (35), BCR (23), Sarcoidosis (15), JIA (12), VKH (8), spondyloarthritis (5), other (9) | 6 | Composite clinical response (CFT < 300 micrometer, RSU) | 36% | 56% (31/55) | CFT < 300, resolution of cystic spaces |
| Ramanan [8] | TCZ (SUBQ) | 2020 | SAT | Efficacy of TCZ in treating JIA associated NIU refractory to TNF-alpha and MTX | 21 | JIA | 9 | IOI | 34% | 75% (3/4) | N/A |
| Wennink [18] | TCZ (IV) | 2020 | CS | Efficacy of TCZ in treating NIU | 7 | Idiopathic uveitis (5), panuveitis (2) | 18 | CFT | 100% | 100% (7/7) | N/A |
| Vegas-Revenga [6] | TCZ (IV) | 2019 | CS | Efficacy of TCZ in treating refractory uveitic macular edema | 25 | JIA (9), BD (7), BCR (4), idiopathic panuveitis (4), sarcoidosis (1) | 12 | CFT | 100% | 100% (25/25) | CFT < 300, resolution of cystic spaces |
| Ozturk [19] | CS (IV) | 2018 | CS | Efficacy of TCZ in refractory BD | 5 | BD | 10 | CFT | 100% | 80% (4/5) | N/A |
| Heissigerova [16] | SAR (SUBQ) | 2018 | RCT | Efficacy of SAR in treating NIU (SAR vs. placebo) | 58 | Intermediate uveitis (12), posterior uveitis (14), panuveitis (29) | 4 | RSU | 46% | 100% (58/58) | 20% reduction of CFT from baseline |
| Mesquida [20] | TCZ (IV) | 2018 | CS | Efficacy of TCZ in treating refractory uveitic macular edema | 12 | JIA (6), BCR (2), idiopathic panuveitis (2), sympathetic ophthalmia (1), ankylosing spondylitis (1) | 24 | CFT | 100% | 83% (10/12) | CFT < 350, resolution of cystic spaces |
| Sepah [14] | TCZ (IV) | 2017 | RCT | Efficacy of two different doses of TCZ in NIU (4 mg/kg versus 8 mg/kg) | 37 | Idiopathic (28), Sarcoidosis (2), VKH (2), BCR (2), PIC (1), BD (1), TINU (1) | 6 | IOI | 44% | 100% (15/15) | N/A |
| Tappeiner [10] | TCZ (IV) | 2016 | CS | Efficacy of TCZ in treating NIU | 5 | JIA | 12 | IOI | 100% | 100% (5/5) | N/A |
| Deuter [21] | TCZ (IV) | 2016 | CS | Efficacy of TCZ in treating refractory uveitic macular edema | 5 | JIA (2), AS (1), RA (2) | 14 | CFT | 75% | 100% (5/5) | 25% reduction of CFT from baseline |
| Mesquida [20] | TCZ (IV) | 2014 | CS | Efficacy of TCZ in treating refractory uveitic macular edema | 7 | BCR (3), JIA (3), idiopathic panuveitis (1) | 15 | CFT | 100% | 71% (5/7) | CFT < 350 |
| Adan [12] | TCZ (IV) | 2013 | CS | Efficacy of TCZ in treating refractory uveitic macular edema | 5 | BCR (3), JIA (1), idiopathic panuveitis (1) | 8 | CFT | 100% | 100% (5/5) | CFT < 350 |
3.2. Comparative Retrospective Study
3.3. Retrospective Case Series
3.4. Adverse Events
3.5. Limitations of Existing Data
4. Interleukin-6 Blockage in Other Etiologies of Macular Edema
4.1. In the Setting of Acute Retinal Necrosis
4.2. In the Setting of Non-Uveitic Macular Edema
4.3. In the Setting of Retinal Vascular Pathology
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mesquida, M.; Molins, B.; Llorenç, V.; de la Maza, M.S.; Adán, A. Targeting interleukin-6 in autoimmune uveitis. Autoimmun. Rev. 2017, 16, 1079–1089. [Google Scholar] [CrossRef]
- Karkhur, S.; Hasanreisoglu, M.; Vigil, E.; Halim, M.S.; Hassan, M.; Plaza, C.; Nguyen, N.V.; Afridi, R.; Tran, A.T.; Do, D.V.; et al. Interleukin-6 inhibition in the management of non-infectious uveitis and beyond. J. Ophthalmic Inflamm. Infect. 2019, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Zahir-Jouzdani, F.; Atyabi, F.; Mojtabavi, N. Interleukin-6 participation in pathology of ocular diseases. Pathophysiology 2017, 24, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Genentech I. ACTEMRA (Tocilizumab) [Package Insert]. US Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/125276s114lbl.pdf (accessed on 15 November 2022).
- LLC S-A. KEVZARA (Sarilumab) [Package Insert]. US Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/761037s000lbl.pdf (accessed on 15 November 2022).
- Vegas-Revenga, N.; Calvo-Río, V.; Mesquida, M.; Adán, A.; Hernández, M.V.; Beltrán, E.; Pascual, E.V.; Díaz-Valle, D.; Díaz-Cordovés, G.; Hernandez-Garfella, M.; et al. Anti-IL6-Receptor Tocilizumab in Refractory and Noninfectious Uveitic Cystoid Macular Edema: Multicenter Study of 25 Patients. Am. J. Ophthalmol. 2019, 200, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minaker, S.A.; Mason, R.H.; Luna, G.L.; Farahvash, A.; Garg, A.; Bhambra, N.; Bapat, P.; Muni, R.H. Changes in aqueous and vitreous inflammatory cytokine levels in diabetic macular oedema: A systematic review and meta-analysis. Acta Ophthalmol. 2022, 100, e53–e70. [Google Scholar] [CrossRef]
- Sharma, S. Interleukin-6 Trans-signaling: A Pathway with Therapeutic Potential for Diabetic Retinopathy. Front. Physiol. 2021, 12, 689429. [Google Scholar] [CrossRef] [PubMed]
- Urias, E.A.; Urias, G.A.; Monickaraj, F.; McGuire, P.; Das, A. Novel therapeutic targets in diabetic macular edema: Beyond VEGF. Vis. Res. 2017, 139, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Kowluru, R.A.; Zhong, Q.; Santos, J.M. Matrix metalloproteinases in diabetic retinopathy: Potential role of MMP-9. Expert Opin. Investig. Drugs 2012, 21, 797–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Droho, S.; Cuda, C.M.; Perlman, H.; Lavine, J.A. Macrophage-derived interleukin-6 is necessary and sufficient for choroidal angiogenesis. Sci. Rep. 2021, 11, 18084. [Google Scholar] [CrossRef]
- Nahavandipour, A.; Nielsen, M.K.; Sørensen, T.L.; Subhi, Y. Systemic levels of interleukin-6 in patients with age-related macular degeneration: A systematic review and meta-analysis. Acta Ophthalmol. 2020, 98, 434–444. [Google Scholar] [CrossRef]
- Ramanan, A.V.; Dick, A.D.; Guly, C.; McKay, A.; Jones, A.P.; Hardwick, B.; Lee, R.W.J.; Smyth, M.; Jaki, T.; Beresford, M.W.; et al. Tocilizumab in patients with anti-TNF refractory juvenile idiopathic arthritis-associated uveitis (APTITUDE): A multicentre, single-arm, phase 2 trial. Lancet Rheumatol. 2020, 2, e135–e141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maccora, I.; Sen, E.S.; Ramanan, A.V. Update on noninfectious uveitis in children and its treatment. Curr. Opin. Rheumatol. 2020, 32, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Tappeiner, C.; Mesquida, M.; Adán, A.; Anton, J.; Ramanan, A.V.; Carreno, E.; Mackensen, F.; Kotaniemi, K.; de Boer, J.H.; Bou, R.; et al. Evidence for Tocilizumab as a Treatment Option in Refractory Uveitis Associated with Juvenile Idiopathic Arthritis. J. Rheumatol. 2016, 43, 2183–2188. [Google Scholar] [CrossRef] [PubMed]
- Thomas, J.; Kuthyar, S.; Shantha, J.G.; Angeles-Han, S.T.; Yeh, S. Update on biologic therapies for juvenile idiopathic arthritis-associated uveitis. Ann. Eye Sci. 2021, 6, 19. [Google Scholar] [CrossRef]
- Adán, A.; Mesquida, M.; Llorenç, V.; Espinosa, G.; Molins, B.; Hernández, M.V.; Pelegrín, L. Tocilizumab treatment for refractory uveitis-related cystoid macular edema. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 2627–2632. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Río, V.; Santos-Gómez, M.; Calvo, I.; González-Fernández, M.I.; López-Montesinos, B.; Mesquida, M.; Adán, A.; Hernández, M.V.; Maíz, O.; Atanes, A.; et al. Anti-Interleukin-6 Receptor Tocilizumab for Severe Juvenile Idiopathic Arthritis-Associated Uveitis Refractory to Anti-Tumor Necrosis Factor Therapy: A Multicenter Study of Twenty-Five Patients. Arthritis Rheumatol. 2017, 69, 668–675. [Google Scholar] [CrossRef]
- Sepah, Y.J.; Sadiq, M.A.; Chu, D.S.; Dacey, M.; Gallemore, R.; Dayani, P.; Hanout, M.; Hassan, M.; Afridi, R.; Agarwal, A.; et al. Primary (Month-6) Outcomes of the STOP-Uveitis Study: Evaluating the Safety, Tolerability, and Efficacy of Tocilizumab in Patients with Noninfectious Uveitis. Am. J. Ophthalmol. 2017, 183, 71–80. [Google Scholar] [CrossRef]
- Gómez-Gómez, A.; Loza, E.; Rosario, M.P.; Espinosa, G.; de Morales, J.M.G.R.; Herrera, J.M.; Muñoz-Fernández, S.; Rodríguez-Rodríguez, L.; Cordero-Coma, M. Efficacy and safety of immunomodulatory drugs in patients with non-infectious intermediate and posterior uveitis, panuveitis and macular edema: A systematic literature review. Semin. Arthritis Rheum. 2020, 50, 1299–1306. [Google Scholar] [CrossRef]
- Heissigerová, J.; Callanan, D.; de Smet, M.D.; Srivastava, S.K.; Karkanová, M.; Garcia-Garcia, O.; Kadayifcilar, S.; Ozyazgan, Y.; Vitti, R.; Erickson, K.; et al. Efficacy and Safety of Sarilumab for the Treatment of Posterior Segment Noninfectious Uveitis (SARIL-NIU): The Phase 2 SATURN Study. Ophthalmology 2019, 126, 428–437. [Google Scholar] [CrossRef]
- Leclercq, M.; Andrillon, A.; Maalouf, G.; Sève, P.; Bielefeld, P.; Gueudry, J.; Sené, T.; Moulinet, T.; Rouvière, B.; Sène, D.; et al. Anti-Tumor Necrosis Factor alpha versus Tocilizumab in the Treatment of Refractory Uveitic Macular Edema: A Multicenter Study from the French Uveitis Network. Ophthalmology 2022, 129, 520–529. [Google Scholar] [CrossRef]
- Wennink, R.A.W.; Ayuso, V.K.; de Vries, L.A.; Vastert, S.J.; de Boer, J.H. Tocilizumab as an Effective Treatment Option in Children with Refractory Intermediate and Panuveitis. Ocul. Immunol. Inflamm. 2021, 29, 21–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eser-Ozturk, H.; Oray, M.; Tugal-Tutkun, I. Tocilizumab for the Treatment of Behçet Uveitis that Failed Interferon Alpha and Anti-Tumor Necrosis Factor-Alpha Therapy. Ocul. Immunol. Inflamm. 2018, 26, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Mesquida, M.; Molins, B.; Llorenç, V.; Hernández, M.V.; Espinosa, G.; De La Maza, M.S.; Adán, A. Twenty-Four Month Follow-up of Tocilizumab Therapy for Refractory Uveitis-Related Macular Edema. Retina 2018, 38, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Deuter, C.M.E.; Zierhut, M.; Igney-Oertel, A.; Xenitidis, T.; Feidt, A.; Sobolewska, B.; Stuebiger, N.; Doycheva, D. Tocilizumab in Uveitic Macular Edema Refractory to Previous Immunomodulatory Treatment. Ocul. Immunol. Inflamm. 2017, 25, 215–220. [Google Scholar] [CrossRef]
- Bograd, A.; Villiger, P.M.; Munk, M.R.; Bolt, I.; Tappeiner, C. Tocilizumab and Aflibercept as a Treatment Option for Refractory Macular Edema after Acute Retinal Necrosis. Ocul. Immunol. Inflamm. 2022, 31, 242–245. [Google Scholar] [CrossRef] [PubMed]
- Pham, B.; Hien, D.L.; Matsumiya, W.; Ngoc, T.T.T.; Doan, H.L.; Akhavanrezayat, A.; Yaşar, Ç.; Nguyen, H.V.; Halim, M.S.; Nguyen, Q.D. Anti-interleukin-6 receptor therapy with tocilizumab for refractory pseudophakic cystoid macular edema. Am. J. Ophthalmol. Case Rep. 2020, 20, 100881. [Google Scholar] [CrossRef]
- Deaner, J.D.; Jaffe, G.J.; Keenan, R.T.; Carnago, L.; Grewal, D.S. Anti–Interleukin-6 Antibodies for Autoimmune Retinopathy with Macular Edema. Ophthalmol. Retin. 2022, 6, 91–93. [Google Scholar] [CrossRef]
- Grewal, D.S.; Jaffe, G.J.; Keenan, R.T. Sarilumab for Recalcitrant Cystoid Macular Edema in Non-Paraneoplastic Autoimmune Retinopathy. Retin. Cases Brief Rep. 2021, 15, 504–508. [Google Scholar] [CrossRef]
- Finn, A.P.; Keenan, R.T.; Jaffe, G.J. Reconstitution of the Ellipsoid Zone with Tocilizumab in Autoimmune Retinopathy. Retin. Cases Brief Rep. 2020, 14, 297–300. [Google Scholar] [CrossRef]
- Ranibizumab for Edema of the mAcula in Diabetes: Protocol 4 with Tocilizumab: The READ-4 Study (READ-4). US National Library of Medicine. Available online: https://clinicaltrials.gov/ct2/show/NCT02511067?term=read+4&draw=2&rank=1 (accessed on 15 November 2022).
- Noma, H.; Yasuda, K.; Shimura, M. Cytokines and the Pathogenesis of Macular Edema in Branch Retinal Vein Occlusion. J. Ophthalmol. 2019, 2019, 5185128. [Google Scholar] [CrossRef]
- Noma, H.; Yasuda, K.; Shimura, M. Cytokines and Pathogenesis of Central Retinal Vein Occlusion. J. Clin. Med. 2020, 9, 3457. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.Y.; Goldberg, D.; Sobrin, L. Interleukin-6 and Macular Edema: A Review of Outcomes with Inhibition. Int. J. Mol. Sci. 2023, 24, 4676. https://doi.org/10.3390/ijms24054676
Yang JY, Goldberg D, Sobrin L. Interleukin-6 and Macular Edema: A Review of Outcomes with Inhibition. International Journal of Molecular Sciences. 2023; 24(5):4676. https://doi.org/10.3390/ijms24054676
Chicago/Turabian StyleYang, Janine Yunfan, David Goldberg, and Lucia Sobrin. 2023. "Interleukin-6 and Macular Edema: A Review of Outcomes with Inhibition" International Journal of Molecular Sciences 24, no. 5: 4676. https://doi.org/10.3390/ijms24054676