
Spinal Cord Injury and Complications Related to Neuraxial Anaesthesia Procedures: A Systematic Review

Abstract
:1. Introduction
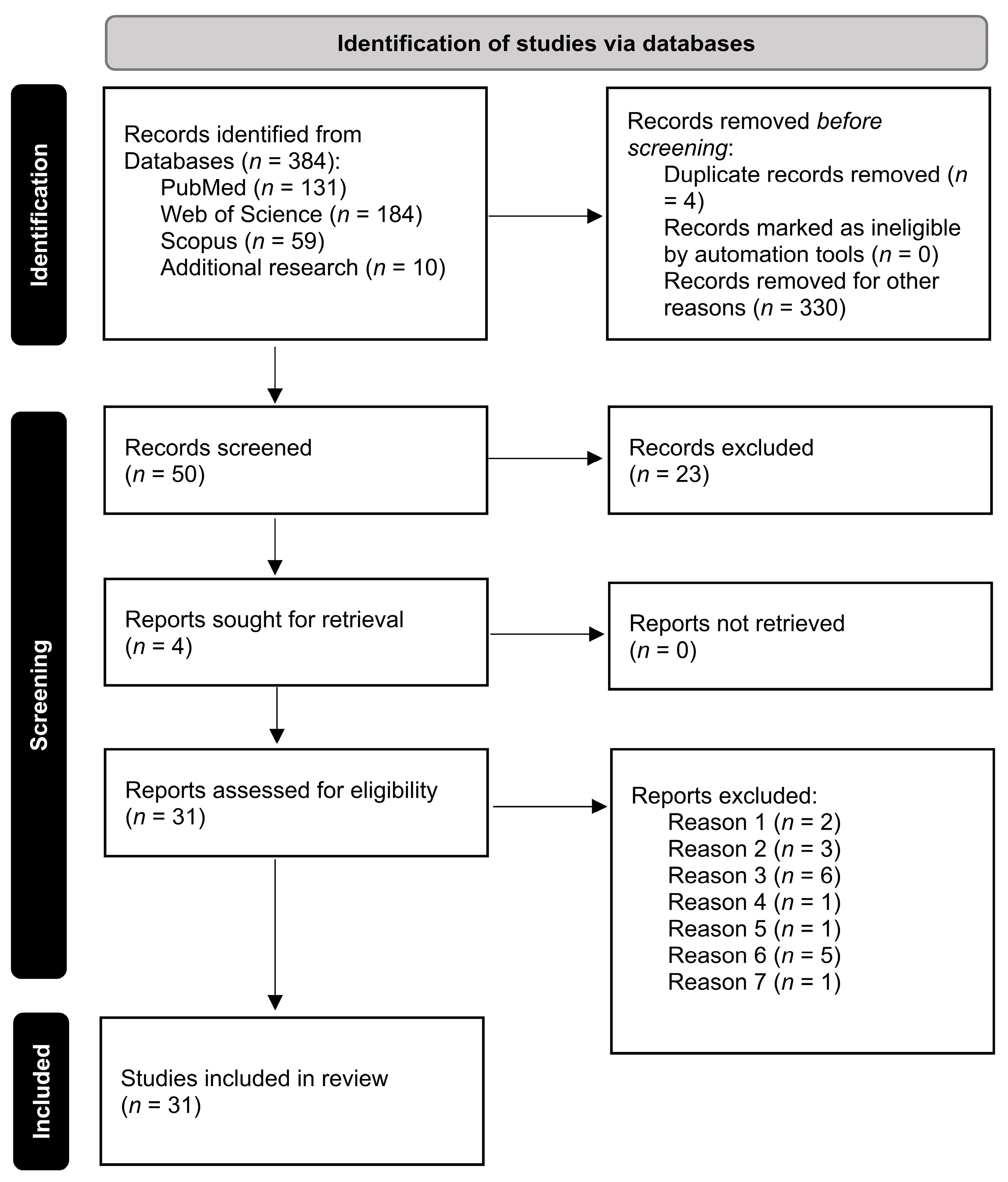
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hewson, D.W.; Bedforth, N.M.; Hardman, J.G. Spinal cord injury arising in anaesthesia practice. Anaesthesia 2018, 73, 43–50. [Google Scholar] [CrossRef] [Green Version]
- Kotoda, M.; Mochizuki, N.; Matsuoka, T.; Kondoh, D.; Matsukawa, T. Successful epidural anesthesia in a patient with an extremely shallow epidural space: A case report. Anaesth. Pain Intensive Care 2018, 22, 224–226. [Google Scholar]
- Drummond, J.C.; Krane, E.J.; Tomatsu, S.; Theroux, M.C.; Lee, R.R. Paraplegia after epidural-general anesthesia in a Morquio patient with moderate thoracic spinal stenosis. Can. J. Anaesth. 2015, 62, 45–49. [Google Scholar] [CrossRef] [Green Version]
- Schildt, E. Low spinal cord injuries following spinal anesthesia. Acta Chir. Scand. 1947, 95, 101–131. [Google Scholar] [CrossRef]
- Vercauteren, M.; Waets, P.; Pitkanen, M.; Forster, J. Neuraxial techniques in patients with pre-existing back impairment or prior spine interventions: A topical review with special reference to obstetrics. Acta Anaesthesiol. Scand. 2011, 55, 910–917. [Google Scholar] [CrossRef]
- Neal, J.M.; Bernards, C.M.; Hadzic, A.; Hebl, J.R.; Hogan, Q.H.; Horlocker, T.T.; Lee, L.A.; Rathmell, J.P.; Sorenson, E.J.; Suresh, S.; et al. ASRA Practice Advisory on Neurologic Complications in Regional Anesthesia and Pain Medicine. Reg. Anesth. Pain Med. 2008, 33, 404–415. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Kishore, K. Complications and controversies of regional anaesthesia: A review. Indian J. Anaesth. 2009, 53, 543–553. [Google Scholar] [PubMed]
- Meyer, M.J.; Krane, E.J.; Goldschneider, K.R.; Klein, N.J. Case report: Neurological complications associated with epidural analgesia in children: A report of 4 cases of ambiguous etiologies. Anesth. Analg. 2012, 115, 1365–1370. [Google Scholar] [CrossRef]
- Stroud, C.C.; Markel, D.; Sidhu, K. Complete paraplegia as a result of regional anesthesia. J. Arthroplast. 2000, 15, 1064–1067. [Google Scholar] [CrossRef]
- Bulow, P.M.; Biering-Sorensen, F. Paraplegia, a severe complication to epidural analgesia. Acta Anaesthesiol. Scand. 1999, 43, 233–235. [Google Scholar] [CrossRef]
- Fabio, C.; Romualdo, D.; Eugenio, A.F.; Vittoradolfo, T.; Massimiliano, V.A.; Giovanna, R. Thoracic Unilateral Spinal Cord Injury After Spinal Anaesthesia for Total Hip Replacement: Fate or Mistake? Turk. J. Anaesthesiol. Reanim. 2017, 45, 116–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagathan, D.S.; Singh, B.P.; Ghatanatti, S.; Sankhwar, S.N. Spinal cord injury: A rare complication following thoracic epidural anesthesia for percutaneous nephrolithotomy. Acta Anaesthesiol. Taiwanica 2012, 50, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Campos, M.G.; Peixoto, A.R.; Fonseca, S.; Santos, F.; Pinho, C.; Leite, D. Assessment of main complications of regional anesthesia recorded in an acute pain unit in a tertiary care university hospital: A retrospective cohort. Braz. J. Anesthesiol. 2022, 72, 605–613. [Google Scholar] [CrossRef] [PubMed]
- Olawin, A.M.; Das, J.M. Spinal Anesthesia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Gadsden, J.; Warlick, A. Regional anesthesia for the trauma patient: Improving patient outcomes. Local Reg. Anesth. 2015, 8, 45–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.P.; Hauerberg, J.; Schmidt, J.F. Incidence of spinal epidural abscess after epidural analgesia: A national 1-year survey. Anesthesiology 1999, 91, 1928–1936. [Google Scholar] [CrossRef]
- Makito, K.; Mouri, H.; Matsui, H.; Michihata, N.; Fushimi, K.; Yasunaga, H. Spinal epidural hematoma and abscess after neuraxial anesthesia: A historical cohort study using the Japanese Diagnosis Procedure Combination database. Can. J. Anaesth. 2021, 68, 42–52. [Google Scholar] [CrossRef]
- Bao, F.-P.; Zhang, H.-G.; Zhu, S.-M. Anesthetic considerations for patients with acute cervical spinal cord injury. Neural Regen. Res. 2017, 12, 499–504. [Google Scholar]
- Neal, J.M. Anatomy and pathophysiology of spinal cord injury associated with regional anesthesia and pain medicine. Reg. Anesth. Pain Med. 2008, 33, 423–434. [Google Scholar] [CrossRef]
- Horlocker, T.T.; Wedel, D.J.; Benzon, H.; Brown, D.L.; Enneking, F.K.; Heit, J.A.; Mulroy, M.F.; Rosenquist, R.W.; Rowlingson, J.; Tryba, M.; et al. Regional anesthesia in the anticoagulated patient: Defining the risks (the second ASRA Consensus Conference on Neuraxial Anesthesia and Anticoagulation). Reg. Anesth. Pain Med. 2003, 28, 172–197. [Google Scholar] [CrossRef]
- Zheng, H.X.; Eric Nyam, T.T.; Liu, C.A.; Lee, Y.L.; Kuo, J.R.; Sung, K.C. Spontaneous Spinal Epidural Hematoma After Normal Spontaneous Delivery with Epidural Analgesia: Case Report and Literature Review. World Neurosurg. 2020, 137, 214–217. [Google Scholar] [CrossRef]
- Sharpe, E.E.; Arendt, K.W.; Jacob, A.K.; Pasternak, J.J. Anesthetic management of parturients with pre-existing paraplegia or tetraplegia: A case series. Int. J. Obstet. Anesth. 2015, 24, 77–84. [Google Scholar] [CrossRef]
- Greaves, J.D. Serious spinal cord injury due to haematomyelia caused by spinal anaesthesia in a patient treated with low-dose heparin. Anaesthesia 1997, 52, 150–154. [Google Scholar] [CrossRef]
- Vogt, L.; Rodermond, B.; Post, P.; Iborra, S.; Stickeler, E.; Schiefer, J.; Alt, J.P.; Rossaint, R.; Röhl, A. Intramedulläre Injektion bei “tethered cord”. Anaesthesist 2018, 67, 131–134. [Google Scholar] [CrossRef]
- Barker, I.; Alderson, J.; Lydon, M.; Franks, C.I. Cardiovascular effects of spinal subarachnoid anesthesia—A study in patients with chronic spinal-cord injuries. Anaesthesia 1985, 40, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Spiro, C.J.; Kamdar, B.B. Labor Epidural Analgesia in a Patient with Brown-Sequard Syndrome: A Case Report. A A Pract. 2020, 14, 3. [Google Scholar] [CrossRef]
- Ciliberti, B.J.; Goldpein, J.; Rovenstine, E.A. HYPERTENSION DURING ANESTHESIA IN PATIENTS WITH SPINAL CORD INJURIES. Anesthesiology 1954, 15, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Rezig, K.; Diar, N.; Benabidallah, D.; Khodja, A.; Saint-Leger, S. Paraplegia and pregnancy: Anaesthesic management. Ann. Fr. D’anesth. Reanim. 2003, 22, 238–241. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, A. Painless epidural haematoma. Anaesth. Intensive Care 1994, 22, 607–610. [Google Scholar] [CrossRef]
- Bartos, A.; Breazu, C.M.; Bartos, D.; Mitre, C.I. Accidental Spinal Cord Injury Following an Attempted Thoracic Epidural for acute Pancreatitis Pain Management. Turk. J. Anaesthesiol. Reanim. 2020, 48, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Mimata, R.; Higashi, M.; Yasui, M.; Hirai, T.; Yamaura, K. Spinal Epidural Hematoma Following Epidural Catheter Removal in a Patient with Postoperative Urgent Coronary Intervention and Intra-Aortic Balloon Pumping (IABP): A Case Report. Am. J. Case Rep. 2019, 20, 1356–1359. [Google Scholar] [CrossRef] [PubMed]
- Kao, M.C.; Tsai, S.K.; Tsou, M.Y.; Lee, H.K.; Guo, W.Y.; Hu, J.S. Paraplegia after delayed detection of inadvertent spinal cord injury during thoracic epidural catheterization in an anesthetized elderly patient. Anesth. Analg. 2004, 99, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Stoll, A.; Sanchez, M. Epidural hematoma after epidural block: Implications for its use in pain management. Surg. Neurol. 2002, 57, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, L.; Harvey, W.R.; Marshall, R.J. Post-operative paraplegia following spinal cord infarction. Acta Anaesthesiol. Scand. 2002, 46, 469–472. [Google Scholar] [CrossRef] [PubMed]
- Mayall, M.F.; Calder, I. Spinal cord injury following an attempted thoracic epidural. Anaesthesia 1999, 54, 990–994. [Google Scholar] [CrossRef]
- Cabitza, P.; Parrini, M. Slow-onset subdural hematoma, evolving into paraplegia, after attempted spinal anesthesia—A case report. Acta Orthop. Scand. 1998, 69, 650–652. [Google Scholar] [CrossRef]
- Barontini, F.; Conti, P.; Marello, G.; Maurri, S. Major neurological sequelae of lumbar epidural anesthesia. Report of three cases. Ital. J. Neurol. Sci. 1996, 17, 333–339. [Google Scholar] [CrossRef]
- Nay, P.G.; Milaszkiewicz, R.; Jothilingam, S. Extradural air as a cause of paraplegia following lumbar analgesia. Anaesthesia 1993, 48, 402–404. [Google Scholar] [CrossRef]
- Adriani, J.; Naragi, M. Paraplegia associated with epidural anesthesia. South Med. J. 1986, 79, 1350–1355. [Google Scholar] [CrossRef] [PubMed]
- Zhu, M.; Zhou, F.; Li, L.; Yin, Q.; Qiu, M.; Zhang, Y. Success with neurotropin in treating pediatric lower extremity pain induced by spinal cord injury after epidural anesthesia. J. Pain Res. 2017, 10, 1391–1394. [Google Scholar] [CrossRef] [Green Version]
- Harsha, K.J.; Parameswaran, K. Permanent spinal cord injury during lumbar spinal anesthesia: A report of two cases. Neurol. India 2016, 64, 808–811. [Google Scholar] [PubMed]
- Netravathi, M.; Taly, A.B.; Sinha, S.; Bindu, P.S.; Goel, G. Accidental spinal cord injury during spinal anesthesia: A report. Ann. Indian Acad. Neurol. 2010, 13, 297–298. [Google Scholar]
- Han, I.S.; Chung, E.Y.; Hahn, Y.J. Spinal epidural hematoma after epidural anesthesia in a patient receiving enoxaparin—A case report. Korean J. Anesthesiol. 2010, 59, 119–122. [Google Scholar] [CrossRef]
- Seidel, R.; Tietke, M.; Heese, O.; Walter, U. Serious Complications After Epidural Catheter Placement: Two Case Reports. Local Reg. Anesth. 2021, 14, 117–124. [Google Scholar] [CrossRef]
- Killeen, T.; Kamat, A.; Walsh, D.; Parker, A.; Aliashkevich, A. Severe adhesive arachnoiditis resulting in progressive paraplegia following obstetric spinal anaesthesia: A case report and review. Anaesthesia 2012, 67, 1386–1394. [Google Scholar] [CrossRef]
- Hirai, T.; Kato, T.; Kawabata, S.; Enomoto, M.; Tomizawa, S.; Yoshii, T.; Sakaki, K.; Shinomiya, K.; Okawa, A. Adhesive arachnoiditis with extensive syringomyelia and giant arachnoid cyst after spinal and epidural anesthesia: A case report. Spine 2012, 37, E195–E198. [Google Scholar] [CrossRef]
- Kang, X.; Zhu, Y.; Lin, K.; Xie, L.; Wen, H.; Geng, W.; Zhu, S. The Incidence of and Risk Factors for Localized Pain at the Epidural Insertion Site After Epidural Anesthesia: A Prospective Survey of More Than 5000 Cases in Nonobstetric Surgery. Risk Manag. Healthc. Policy 2021, 14, 2171–2180. [Google Scholar] [CrossRef]
- Meyer-Bender, A.; Kern, A.; Pollwein, B.; Crispin, A.; Lang, P.M. Incidence and predictors of immediate complications following perioperative non-obstetric epidural punctures. BMC Anesthesiol. 2012, 12, 31. [Google Scholar] [CrossRef] [Green Version]
- Cook, T.M.; Counsell, D.; Wildsmith, J.A.; Royal College of Anaesthetists Third National Audit Project. Major complications of central neuraxial block: Report on the Third National Audit Project of the Royal College of Anaesthetists. Br. J. Anaesth. 2009, 102, 179–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moen, V.; Dahlgren, N.; Irestedt, L. Severe neurological complications after central neuraxial blockades in Sweden 1990–1999. Anesthesiology 2004, 101, 950–959. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Norum, H.; Fenger-Eriksen, C.; Alahuhta, S.; Vigfusson, G.; Thomas, O.; Lagerkranser, M. Reducing risk of spinal haematoma from spinal and epidural pain procedures. Scand. J. Pain 2018, 18, 129–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dupeyrat, A.; Dequire, P.M.; Merouani, A.; Moullier, P.; Eid, G. Subarachnoid hematoma and spinal anesthesia. Ann. Fr. D’anesth. Reanim. 1990, 9, 560–562. [Google Scholar] [CrossRef]
- DeAngelis, J. Hazards of subdural and epidural anesthesia during anticoagulant therapy: A case report and review. Anesth. Analg. 1972, 51, 676–679. [Google Scholar]
- Bent, U.; Gniffke, S.; Reinbold, W.D. Epidural hematoma following single-shot epidural-anesthesia. Anaesthesist 1994, 43, 245–248. [Google Scholar] [CrossRef]
- Otto, C.W.; Wall, C.L. Total spinal anesthesia: A rare complication of intrathoracic intercostal nerve block. Ann. Thorac. Surg. 1976, 22, 289–292. [Google Scholar] [CrossRef]
- Benumof, J.L. Permanent loss of cervical spinal cord function associated with interscalene block performed under general anesthesia. Anesthesiology 2000, 93, 1541–1544. [Google Scholar] [CrossRef]
- Rose, J.B. Spinal Cord Injury in a Child After Single-Shot Epidural Anesthesia. Anesth. Analg. 2003, 96, 3–6. [Google Scholar] [CrossRef]
- Sorenson, E.J. Neurological injuries associated with regional anesthesia. Reg. Anesth. Pain Med. 2008, 33, 442–448. [Google Scholar] [CrossRef]
- Bi, Y.; Zhou, J. Spinal subdural hematoma and subdural anesthesia following combined spinal-epidural anesthesia: A case report. BMC Anesthesiol. 2021, 21, 130. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Ref | Patients/Age, RF | Type of Anaesthesia and Injury | Possible Reasons/Aetiology/ Consequences | Treatments/Conducts/ Recommendations |
|---|---|---|---|---|
| [3] | 1 CR
| L2–3 epidural + GA | Spinal cord infarction leading to complete paraplegia | Epidural discontinued and catheter removal |
| [8] | 4 paediatric CRs
| Epidural + GA:
|
|
|
| [9] | 2 CRs
|
| Complete paraplegia: one spinal cord compression (hematoma) and one subdural hematoma. A patient died in the decompression surgery | Drug discontinued and catheter removed + urgent decompression of the spinal canal |
| [10] | 4 CRs
|
|
| Same treatment for all cases: epidural abscess evacuation + antibiotic treatment + rehabilitation |
| [11] | 1 CR
| L2–L3 spinal
| Severe subacute axonal sciatic damage and S1 root | Not reported |
| [12] | 1 CR
| T12-L1 epidural
| Permanent paraplegia following percutaneous nephrolithotomy | Monitoring to allow early detection of mismanagement and prevention of further neurologic injury |
| [21] | 1 CR
| L3-4 epidural
| Pain, numbness, paraplegia, areflexia sensory loss and anal tone absent. Deep vein thrombosis | Surgical hematoma treatment and rehabilitation with functional recovery. Pharmacologic therapy to prevent further thrombosis |
| [23] | 1 CR
| Spinal anaesthesia with first attempt believed to be at the L3–4 | Intense pain, paralysis, sensory deficit. Autopsy: extensive haematomyelia | Subarachnoid injection withdrawn and moved to GA |
| [34] | 1 CR
| T11-12 epidural + GA
| Fatigue in legs, loss of sensation, motor paralysis. CT + MRI showed a T9-11 spinal epidural hematoma | Emergency laminectomy and rehabilitation with symptoms slightly improved |
| [35] | 1 CR
| T9-10 epidural + GA
| Numbness, weakness, bowel, and bladder incontinence. Sensory loss below T11 and permanent paraplegia | Little improvement after corticoid and rehabilitation |
| [36] | 1 CR
| C5-C6 epidural steroid block for pain control
| Acute cervical myelopathy with pain, weakness | Hemilaminectomy with a near complete recovery |
| [37] | 1 CR
| T10-11 epidural + GA
| Confusion, pyrexia and tachycardia. Systemic inflammatory response syndrome. L3 flaccid paralysis, areflexia, analgesia and impaired sensation | Epidural catheter removed and rehabilitation |
| [38] | 1 CR
| GA + several tentative of thoracic epidural
| Spinal cord damage due to needle puncture and subsequent haematoma | Surgical dura repair with no improvement (paraplegic) |
| [39] | 1 CR
| 3 attempts of L2-L3 spinal anaesthesia
| Mental confusion, fever, permanent paraplegia | Moved to GA.Antibiotic + antinflammatory + hematoma decompression |
| [40] | 3 CRs
|
|
|
|
| [32] | 1 CR
| L1-2 epidural (paraesthesia)
| Limited sensory and motor function, bowel and bladder incontinent. 10 days later: gangrenous stump and septic shock | Urgent spinal cord decompression + rehabilitation |
| [41] | 1 CR
| L2-4 epidural (4 attempts) + GA
| Prolonged paraesthesia and paresis | Corticoids. Patient with no pain or neurological symptoms |
| [42] | 3 CRs
|
|
|
|
| [43] | 1 CR
| T12–L1 epidural + propofol sedationunexpected needle puncture | Myodynamia improved, but progressive pain persisted that was absent after second treatment | Analgesics and corticoids, then neurotropin. Patient reported gradual pain decrease |
| [44] | 2 CRs
|
|
|
|
| [45] | 1 CR
| L1-2 Spinal anaesthesia + T12–L1 interspace second attempt | Pain, persistent numbness, and weakness of her left lower limb with normal bladder and bowel sensations | Corticoids with gradual improvement |
| [46] | 1 CR
| L4-5 epidural + GA + enoxaparin
| 2nd postoperative day reduced sensation of the right and motor weakness of the left leg | Laminectomy with no improvement in neurologic function |
| [47] | 2 CRs
|
|
|
|
| [33] | 1 CR
| Attempted T11-12 epidural for pain management
| Motor deficit on right lower limb. MRI showed a direct spinal cord injury | Pharmacological treatment and laminectomy with slow recovery |
| [32] | 1 CR
| L3–4 spinal–epidural several attempts
| Left leg sensation and motor function completely recovered 3 h later | Hematoma absorption observation |
| [48] | 1 CR
| L4-5 spinal
| Pain, communicating hydrocephalus and syringomyelia. Rapid, progressive paraplegia and sphincter dysfunction | Unsuccessful laminectomy, external drainage of the syrinx and intravenous steroids |
| [49] | 1 CR
| Combined spinal at L3-4 and epidural at L1-2
| Paraplegia, widespread syringomyelia, massive anterior arachnoid spinal cyst | Shunting of the cyst prevented symptoms progression. Numbness and motor weakness remained |
| Ref | Study/Patients | Type of Anaesthesia | Anaes-SCI | Treatments/Conducts/ Recommendations |
|---|---|---|---|---|
| [13] | Retrospective Study: 10,838 referred to Acute Pain Unit |
| 10.1% with side effects/ complications:
| The Acute Pain Units are fundamental in monitoring, following-up and guiding the treatment of patients with complications |
| [16] | Prospective study: 17,372 epidural catheters |
| 9 cases of epidural abscess:
| Main treatments:
|
| [50] | Prospective study: 5083 surgical inpatients |
| Major complications
| Anaesthesiologist’s skills could be improved to reduce the incidence of Anaes-SCI |
| [51] | Retrospective Study: 7958 non-obstetrical |
|
| Increasing anaesthesiologists’ awareness of patients at higher risk for Anaes-SCI will enhance safety |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pozza, D.H.; Tavares, I.; Cruz, C.D.; Fonseca, S. Spinal Cord Injury and Complications Related to Neuraxial Anaesthesia Procedures: A Systematic Review. Int. J. Mol. Sci. 2023, 24, 4665. https://doi.org/10.3390/ijms24054665
Pozza DH, Tavares I, Cruz CD, Fonseca S. Spinal Cord Injury and Complications Related to Neuraxial Anaesthesia Procedures: A Systematic Review. International Journal of Molecular Sciences. 2023; 24(5):4665. https://doi.org/10.3390/ijms24054665
Chicago/Turabian StylePozza, Daniel H., Isaura Tavares, Célia Duarte Cruz, and Sara Fonseca. 2023. "Spinal Cord Injury and Complications Related to Neuraxial Anaesthesia Procedures: A Systematic Review" International Journal of Molecular Sciences 24, no. 5: 4665. https://doi.org/10.3390/ijms24054665