
Antibacterial Effects of X-ray and MRI Contrast Media: An In Vitro Pilot Study


Abstract
:1. Introduction
2. Results
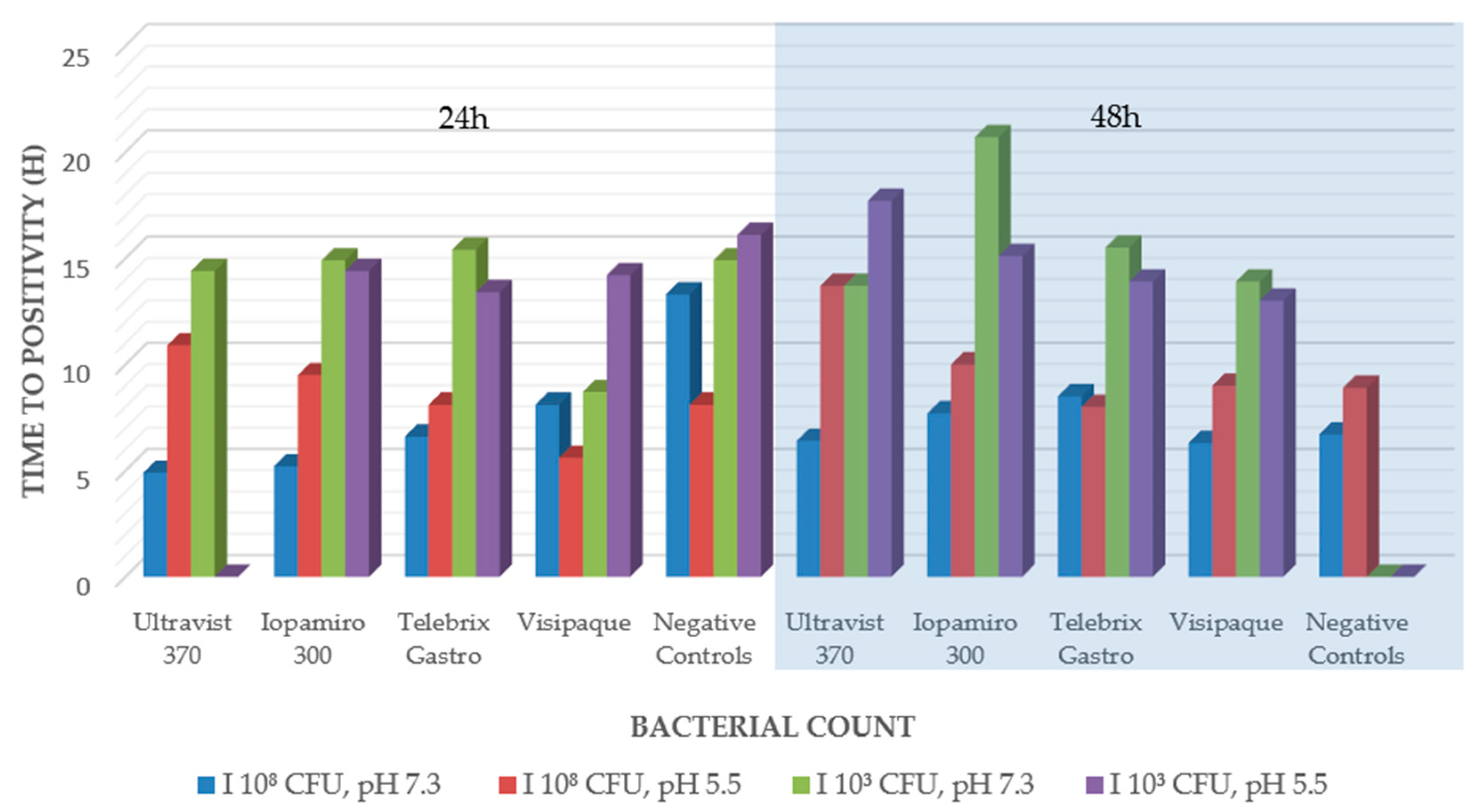
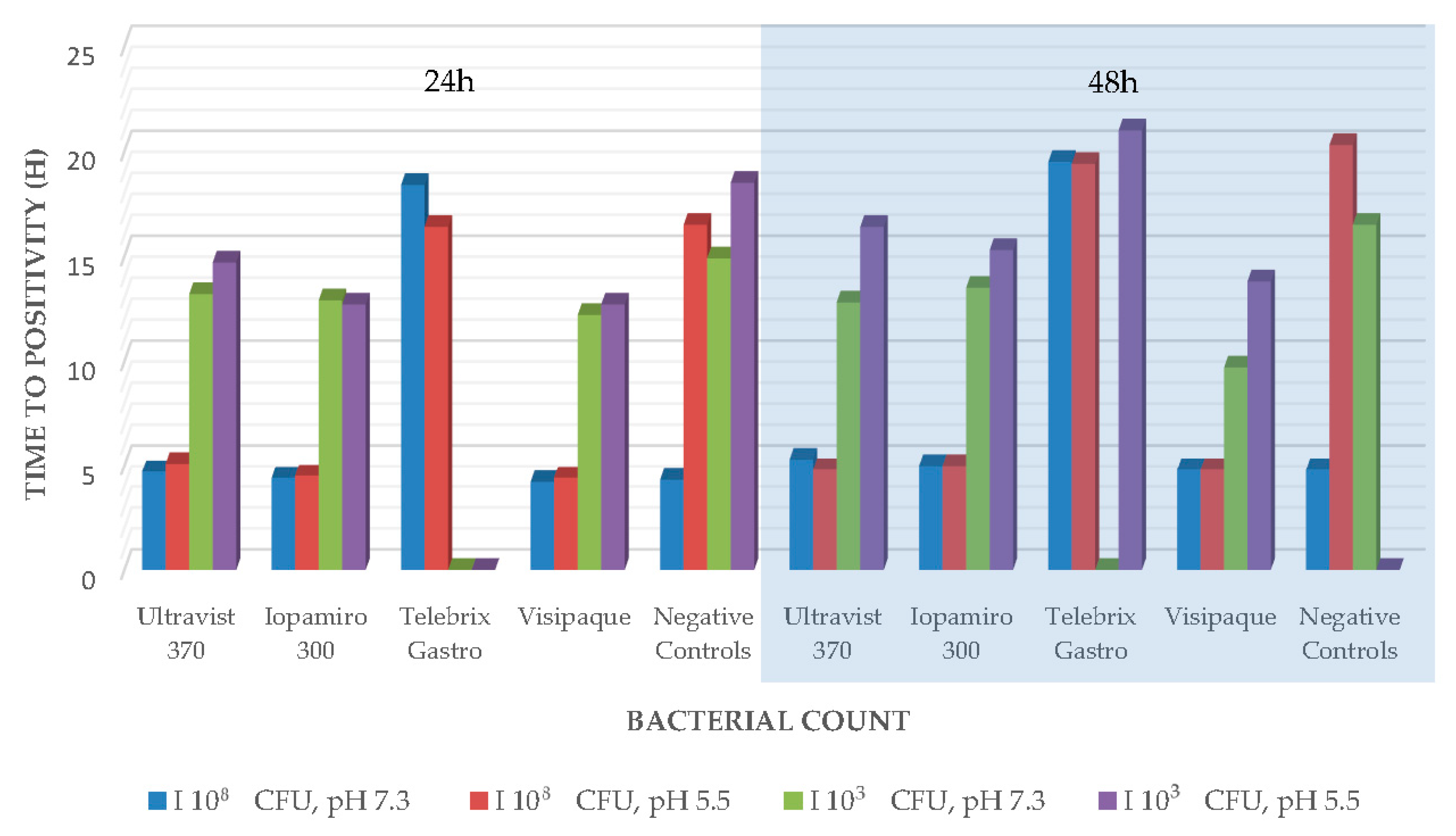
2.1. Antibacterial Efficacy Tests in Blood Culture Bottles
2.2. Agar Disk Diffusion
2.3. Broth Microdilution in Minimal Medium
3. Discussion
Limitations
4. Materials and Methods
4.1. Bacterial Strains
4.2. Antibacterial Efficacy Tests in Blood Culture Bottles
4.3. Agar Disk Diffusion
4.4. Broth Microdilution in Minimal Medium
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, F.C. Iodine in Medicine and Pharmacy Since its Discovery—1811–1961. Proc. R. Soc. Med. 1961, 54, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Haley, T.J.; Raymond, K.; Komesu, N.; Upham, H.C. Toxicological and Pharmacological Effects of Gadolinium and Samarium Chlorides. Br. J. Pharmacol. Chemother. 1961, 17, 526–532. [Google Scholar] [CrossRef] [PubMed]
- Baykara, M.; Ozcan, M.; Bilgen, M.; Kelestimur, H. Effects of gadolinium and gadolinium chelates on intracellular calcium signaling in sensory neurons. Neurosci. Lett. 2019, 707, 134295. [Google Scholar] [CrossRef] [PubMed]
- Blake, M.; Halasz, S. The effects of X-ray contrast media on bacterial growth. Australas. Radiol. 1995, 39, 10–13. [Google Scholar] [CrossRef]
- Kuhns, L.R.; Baublis, J.V.; Gregory, J.; Poznanski, A.K. In Vitro Effect of Cystographic Contrast Media on Urinary Tract Pathogens. Investig. Radiol. 1972, 7, 112–117. [Google Scholar] [CrossRef]
- Narins, D.J.; Chase, R.M. The Effect of Hypaque upon Urine Cultures. J. Urol. 1971, 105, 433–435. [Google Scholar] [CrossRef]
- Speck, U. Kontrastmittel: Übersicht, Anwendung und Pharmazeutische Aspekte; Springer-Verlag: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Green, K.A.; Mustachi, B.; Schoer, K.; Moro, D.; Blend, R.; McGeer, A. Gadolinium-based MR contrast media: Potential for growth of microbial contaminants when single vials are used for multiple patients. Am. J. Roentgenol. 1995, 165, 669–671. [Google Scholar] [CrossRef]
- Beussink, D.R.; Godat, J.F.; Seaton, T. Antimicrobial properties of magnetic resonance imaging contrast media. Am. J. Health Pharm. 2000, 57, 48–50. [Google Scholar] [CrossRef]
- Bruins, M.J.; Zwiers, J.H.; Verheyen, C.C.P.M.; Wolfhagen, M.J.H.M. In vitro study of the antimicrobial effects of radiological contrast agents used in arthrography. J. Bone Jt. Surg. 2011, 93-B, 126–130. [Google Scholar] [CrossRef]
- Dawson, P.; Becker, A.; Holton, J.M. The effect of contrast media on the growth of bacteria. Br. J. Radiol. 1983, 56, 809–815. [Google Scholar] [CrossRef]
- Rendl, J.; Saller, B. Schilddruse und Rontgenkontrastmittel-Pathophysiologie, Haufigkeit und Prophylaxe der jodinduzierten Hyperthyreose. Dtsch. Arztebl-Arztl. Mitt. Ausg. A 2001, 98, 402–406. [Google Scholar]
- Langer, R.; Usmani, A.; van Gorkom, K.; Lorke, D.; Petroianu, G.; Azimullah, S.; Nurulain, S. In vitro assessment of the antibiotic efficacy of contrast media and antibiotics and their combinations at various dilutions. Br. J. Radiol. 2010, 83, 394–400. [Google Scholar] [CrossRef]
- Caravan, P.; Ellison, J.J.; McMurry, T.J.; Lauffer, R.B. Gadolinium (III) chelates as MRI contrast agents: Structure, dynamics, and applications. Chem. Rev. 1999, 99, 2293–2352. [Google Scholar] [CrossRef]
- Black, A.P.; Kinman, R.N.; Keirn, M.A.; Smith, J.J.; Harlan, W.E. The disinfection of swimming pool waters. I. Comparison of iodine and chlorine as swimming pool disinfectants. Am. J. Public Health Nations Heath 1970, 60, 535–545. [Google Scholar] [CrossRef]
- Chang, S.L. The use of active iodine as a water disinfectant. J. Am. Pharm. Assoc. (Sci. Ed.) 1958, 47, 417–423. [Google Scholar] [CrossRef]
- Ellis, K.; Van Vree, H. Iodine used as a water-disinfectant in turbid waters. Water Res. 1989, 23, 671–676. [Google Scholar] [CrossRef]
- World Health Organization. Iodine in Drinking-Water; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Clarke, N.; Berg, G.; Kabler, P.; Chang, S.; TAFT, R.A. Human enteric viruses in water: Source, survival and removability. In Advances in Water Pollution Research; Elsevier: Amsterdam, The Netherlands, 1964; pp. 523–541. [Google Scholar]
- Taylor, G.R.; Butler, M. A comparison of the virucidal properties of chlorine, chlorine dioxide, bromine chloride and iodine. Epidemiol. Infect. 1982, 89, 321–328. [Google Scholar] [CrossRef]
- Pasternak, J.J.; Williamson, E.E. Clinical Pharmacology, Uses, and Adverse Reactions of Iodinated Contrast Agents: A Primer for the Non-radiologist. Mayo Clin. Proc. 2012, 87, 390–402. [Google Scholar] [CrossRef]
- Wahsner, J.; Gale, E.M.; Rodríguez-Rodríguez, A.; Caravan, P. Chemistry of MRI Contrast Agents: Current Challenges and New Frontiers. Chem. Rev. 2018, 119, 957–1057. [Google Scholar] [CrossRef]
- Sheet, P. Berlex Ultravist Imaging Agent Will Be Launched in July; Approved May 10, Two Years after Advisory Committee. Available online: https://scrip.pharmaintelligence.informa.com/PS026177/Berlex-Ultravist-imaging-agent-will-be-launched-in-July-approved-May-10-two-years-after-advisory-committee (accessed on 5 February 2023).
- Dawson, P.; Clauss, W. Contrast Media in Practice: Questions and Answers; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Guerbet. Dotarem® (Gadoteric acid—Gadoterate meglumine). Available online: https://www.guerbet.com/en-in/products-solutions/contrast-agents/dotarem (accessed on 5 February 2023).
- News, I.T. Bracco’s MultiHance to Show Improved MR Visualization. Available online: https://www.itnonline.com/content/braccos-multihance-show-improved-mr-visualization (accessed on 5 February 2023).
- Cleary, K.; Peters, T.M. Image-Guided Interventions: Technology Review and Clinical Applications. Annu. Rev. Biomed. Eng. 2010, 12, 119–142. [Google Scholar] [CrossRef]
- Böhm, I.; Speck, U.; Schild, H. Cell-dependent influence on the phagocytosis induced by non-ionic contrast medium injection. Br. J. Radiol. 2008, 81, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Baert, A.L. Encyclopedia of Imaging; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2008; Volume 2. [Google Scholar]
- Li, H.; Meade, T.J. Molecular Magnetic Resonance Imaging with Gd(III)-Based Contrast Agents: Challenges and Key Advances. J. Am. Chem. Soc. 2019, 141, 17025–17041. [Google Scholar] [CrossRef] [PubMed]
- Bessman, A.N.; Page, J.; Thomas, L.J. In vivo pH of induced soft-tissue abscesses in diabetic and nondiabetic mice. Diabetes 1989, 38, 659–662. [Google Scholar] [CrossRef] [PubMed]
- Huemer, M.; Mairpady Shambat, S.; Bergada-Pijuan, J.; Söderholm, S.; Boumasmoud, M.; Vulin, C.; Gómez-Mejia, A.; Antelo Varela, M.; Tripathi, V.; Götschi, S.; et al. Molecular reprogramming and phenotype switching in Staphylococcus aureus lead to high antibiotic persistence and affect therapy success. Proc. Natl. Acad. Sci. USA 2021, 118, e2014920118. [Google Scholar] [CrossRef]
- Nekoofar, M.H.; Namazikhah, M.S.; Sheykhrezae, M.S.; Mohammadi, M.M.; Kazemi, A.; Aseeley, Z.; Dummer, P. pH of pus collected from periapical abscesses. Int. Endod. J. 2009, 42, 534–538. [Google Scholar] [CrossRef]
- Swissmedic. Dotarem Inj Solution. Available online: https://compendium.ch/product/19763-dotarem-inj-los-2-793-g-10ml (accessed on 22 June 2022).
- Swissmedic. Ultravist Inj Solution 370 mg. Available online: https://compendium.ch/product/23161-ultravist-inj-los-370-mg (accessed on 22 June 2022).



{kind=link}
{kind=link}
| Staphylococcusaureus | Bacillus subtilis | Pseudomonas aeruginosa | ||||||
|---|---|---|---|---|---|---|---|---|
| Contrast Agent | CFU/mL | pH | 24 h | 48 h | 24 h | 48 h | 24 h | 48 h |
| Ultravist 370 | 1.5 × 108–5.0 × 108 | 7.3 | 3.8 | 4.7 | 4.9 | 6.4 | 4.7 | 5.3 |
| 5.5 | 4.3 | 5.8 | 10.9 | 13.7 | 5.1 | 4.8 | ||
| 1.5 × 103–5.0 × 103 | 7.3 | 12.3 | 16 | 14.4 | 13.7 | 13.2 | 12.8 | |
| 5.5 | 11.6 | 13.7 | 17.7 | 14.7 | 16.4 | |||
| Iopamiro 300 | 1.5 × 108–5.0 × 108 | 7 | 3.7 | 4.9 | 5.2 | 7.7 | 4.4 | 5 |
| 5.5 | 4.1 | 5.2 | 9.5 | 10 | 4.5 | 5 | ||
| 1.5 × 103–5.0 × 103 | 7 | 12.8 | 14.4 | 14.9 | 20.7 | 12.9 | 13.5 | |
| 5.5 | 14.9 | 21.5 | 14.4 | 15.1 | 12.7 | 15.3 | ||
| Telebrix Gastro | 1.5 × 108–5.0 × 108 | 7.1 | 6.6 | 9.8 | 6.6 | 8.5 | 18.4 | 19.5 |
| 5.5 | 5.9 | 8 | 8.1 | 8 | 16.4 | 19.4 | ||
| 1.5 × 103–5.0 × 103 | 7.1 | 16.5 | 21.2 | 15.4 | 15.5 | |||
| 5.5 | 11.1 | 15.9 | 13.4 | 13.9 | 21 | |||
| Visipaque | 1.5 × 108–5.0 × 108 | 7.2 | 3.9 | 6.7 | 8.1 | 6.3 | 4.2 | 4.8 |
| 5.5 | 5.4 | 10.7 | 5.6 | 9 | 4.4 | 4.8 | ||
| 1.5 × 103–5.0 × 103 | 7.2 | 13.2 | 20.2 | 8.7 | 13.9 | 12.2 | 9.7 | |
| 5.5 | 15.5 | 23.5 | 14.2 | 13 | 12.7 | 13.8 | ||
| Negative Controls | 1.5 × 108–5.0 × 108 | 7 | 7.5 | 7.8 | 13.3 | 6.7 | 4.3 | 4.8 |
| 5.5 | 9.1 | 18.3 | 8.1 | 8.9 | 16.5 | 20.3 | ||
| 1.5 × 103–5.0 × 103 | 7 | 23.7 | 14.9 | 14.9 | 16.5 | |||
| 5.5 | 16 | 16.1 | 18.5 | |||||
| Bacterium | Ultravist | Iopamiro | Telebrix Gastro | Visipaque | Multihance | Dotarem |
|---|---|---|---|---|---|---|
| M.smegmatis | x | x | x | - | x | x |
| S.aureus | - | - | - | - | - | - |
| E.coli | - | x | - | x | x (1/3) | x (1/3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brönnimann, M.P.; Hirzberger, L.; Keller, P.M.; Gsell-Albert, M. Antibacterial Effects of X-ray and MRI Contrast Media: An In Vitro Pilot Study. Int. J. Mol. Sci. 2023, 24, 3470. https://doi.org/10.3390/ijms24043470
Brönnimann MP, Hirzberger L, Keller PM, Gsell-Albert M. Antibacterial Effects of X-ray and MRI Contrast Media: An In Vitro Pilot Study. International Journal of Molecular Sciences. 2023; 24(4):3470. https://doi.org/10.3390/ijms24043470
Chicago/Turabian StyleBrönnimann, Michael P., Lea Hirzberger, Peter M. Keller, and Monika Gsell-Albert. 2023. "Antibacterial Effects of X-ray and MRI Contrast Media: An In Vitro Pilot Study" International Journal of Molecular Sciences 24, no. 4: 3470. https://doi.org/10.3390/ijms24043470