
Identification of Pre-Renal and Intrinsic Acute Kidney Injury by Anamnestic and Biochemical Criteria: Distinct Association with Urinary Injury Biomarkers
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
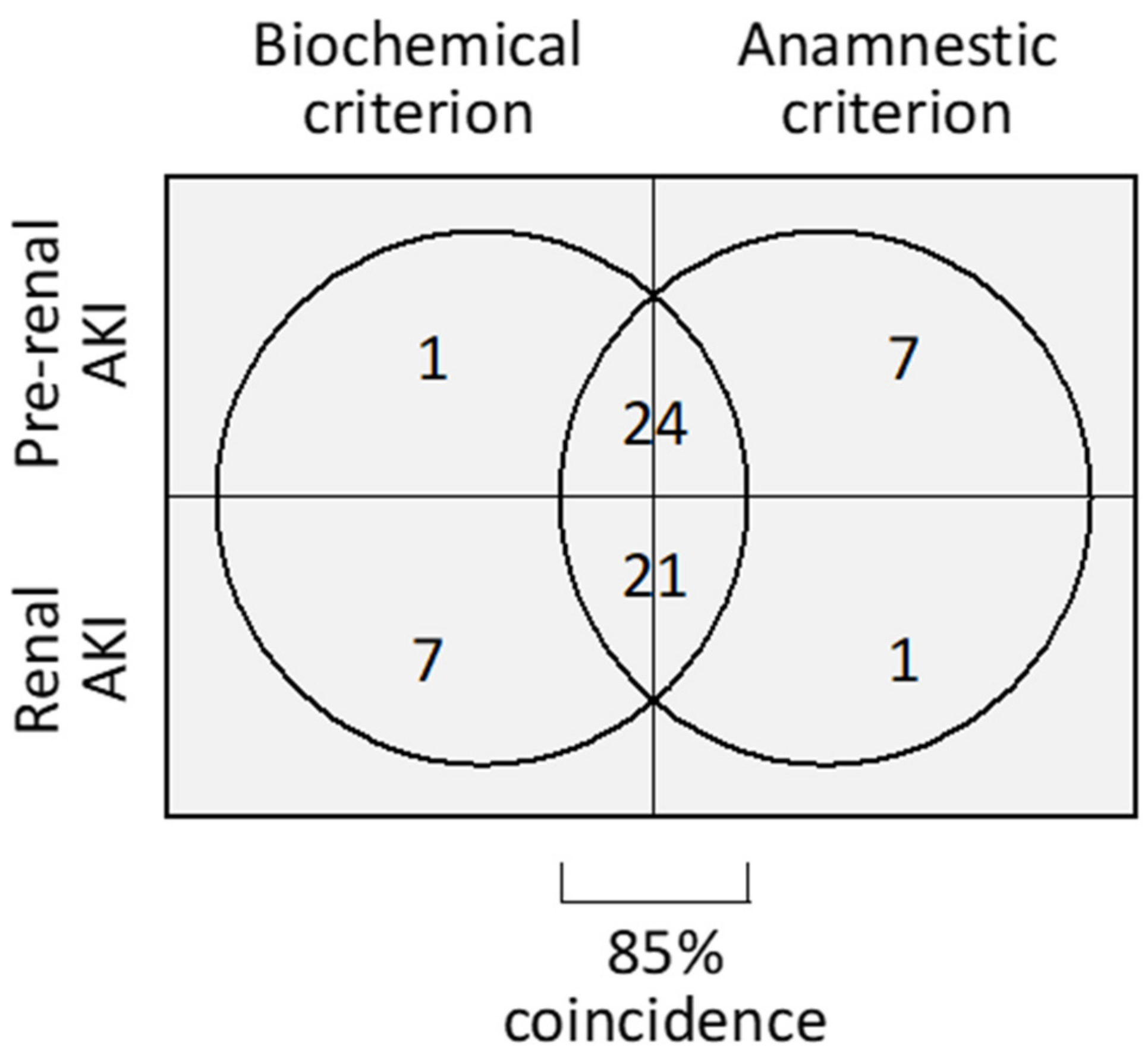
2.1. Patient Description and Etiological Classification
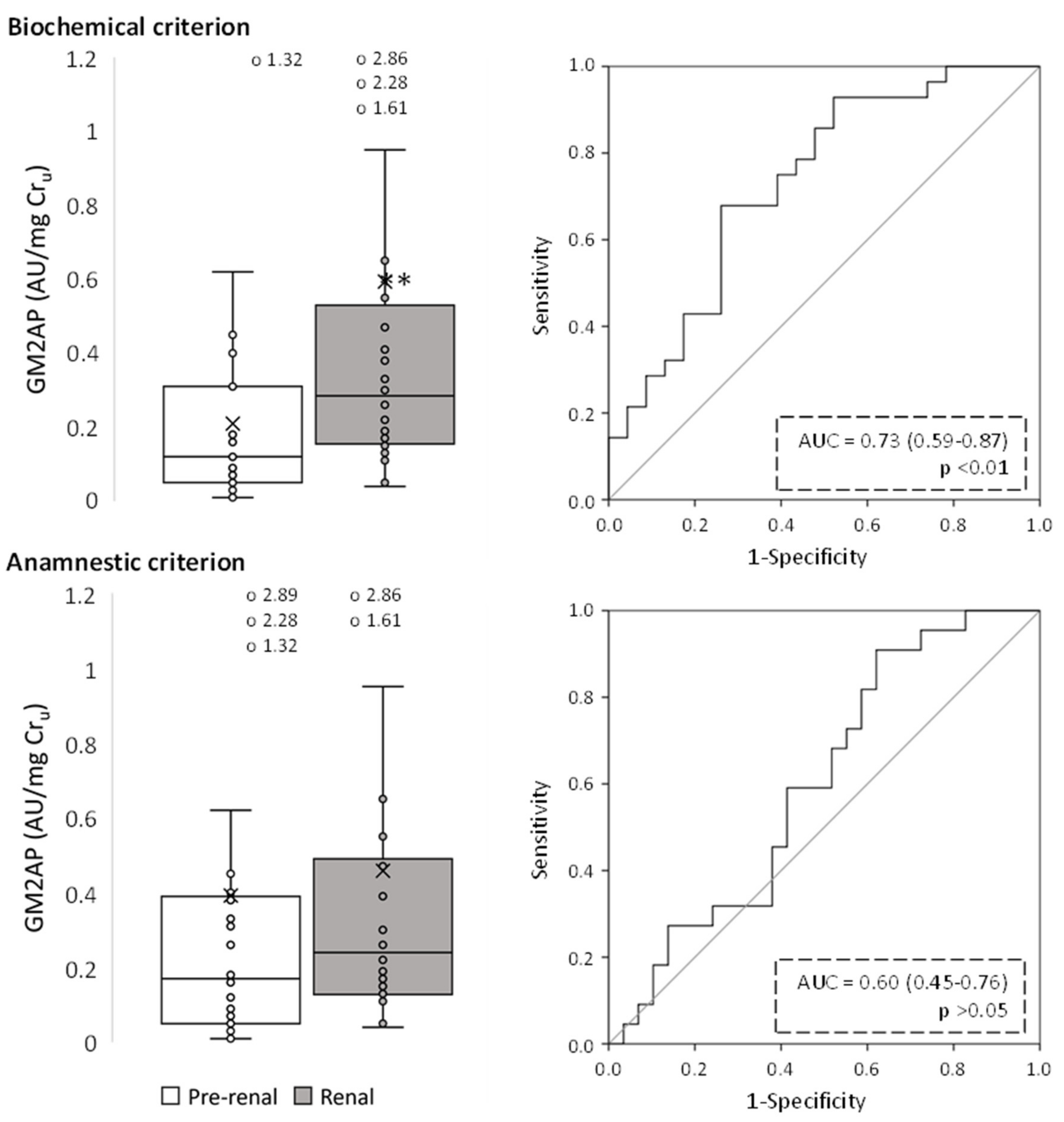
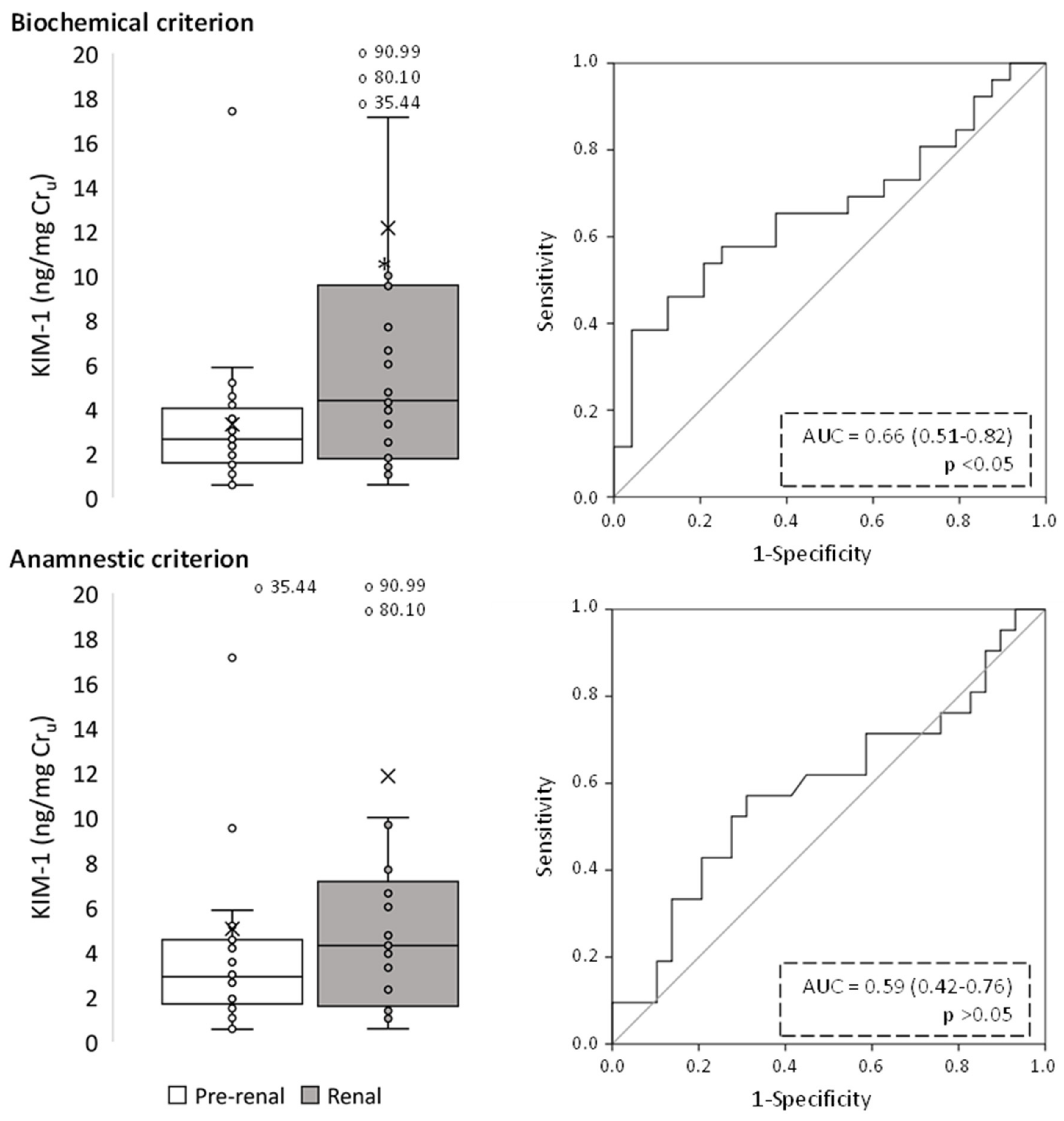
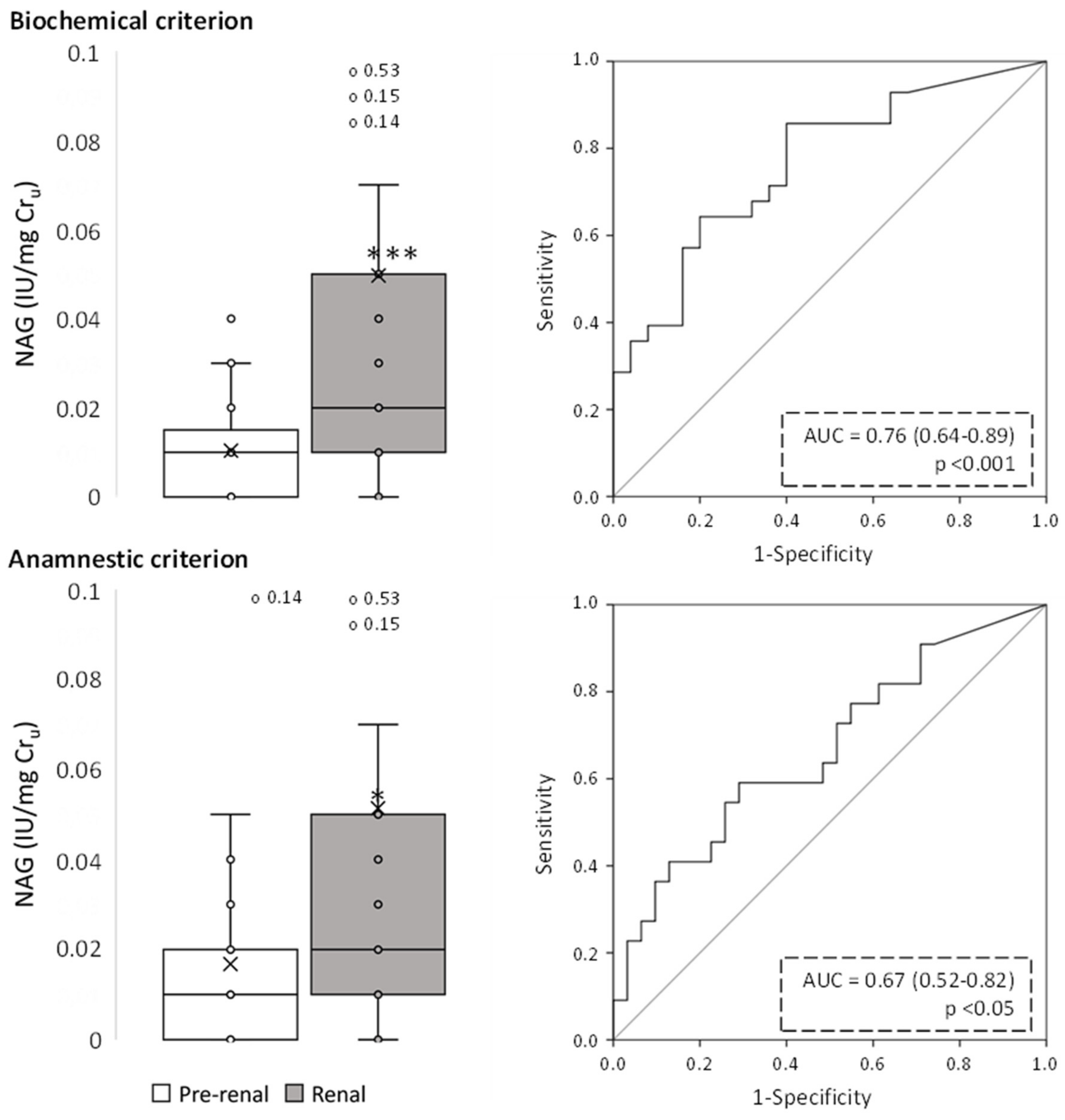
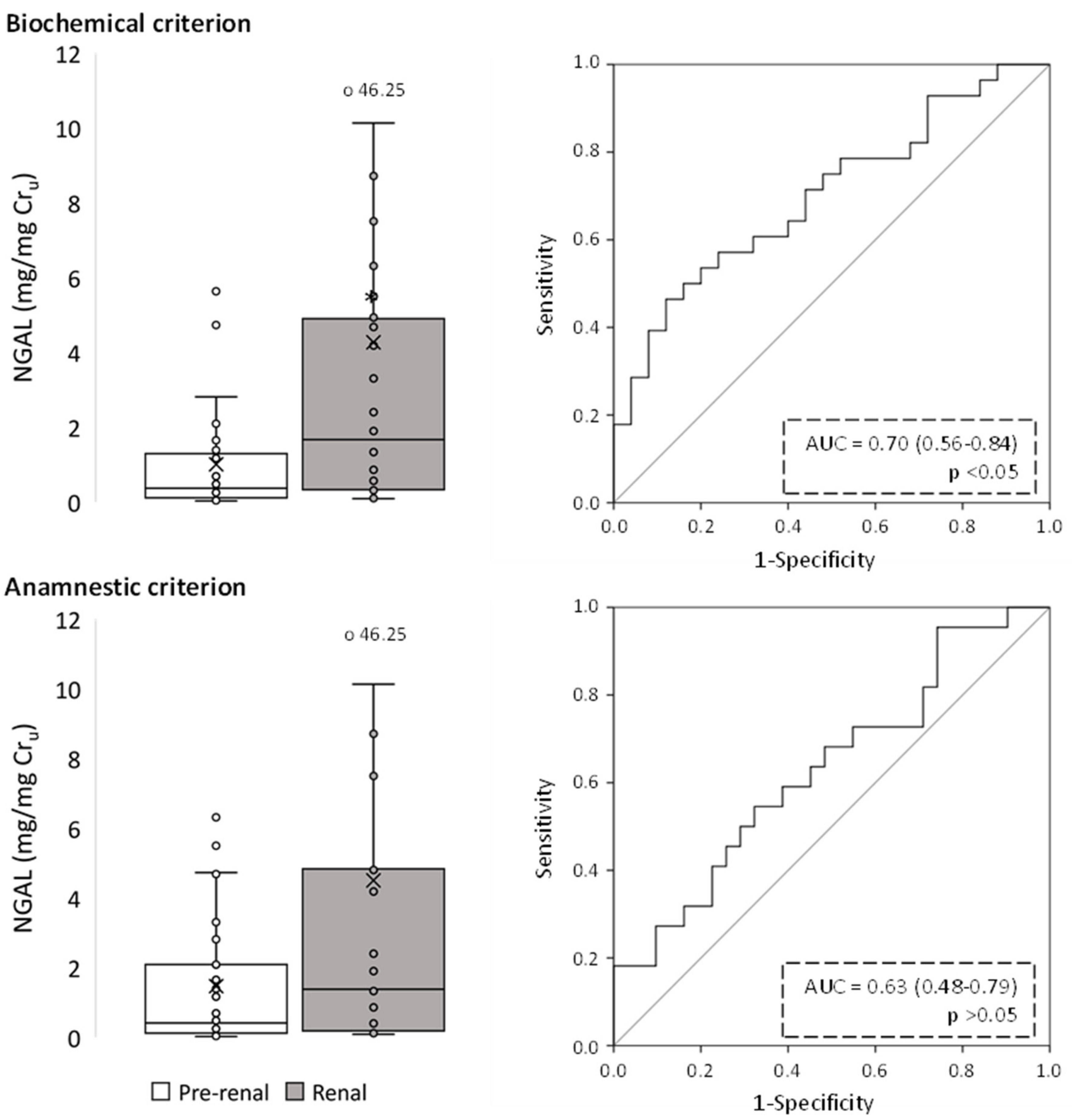
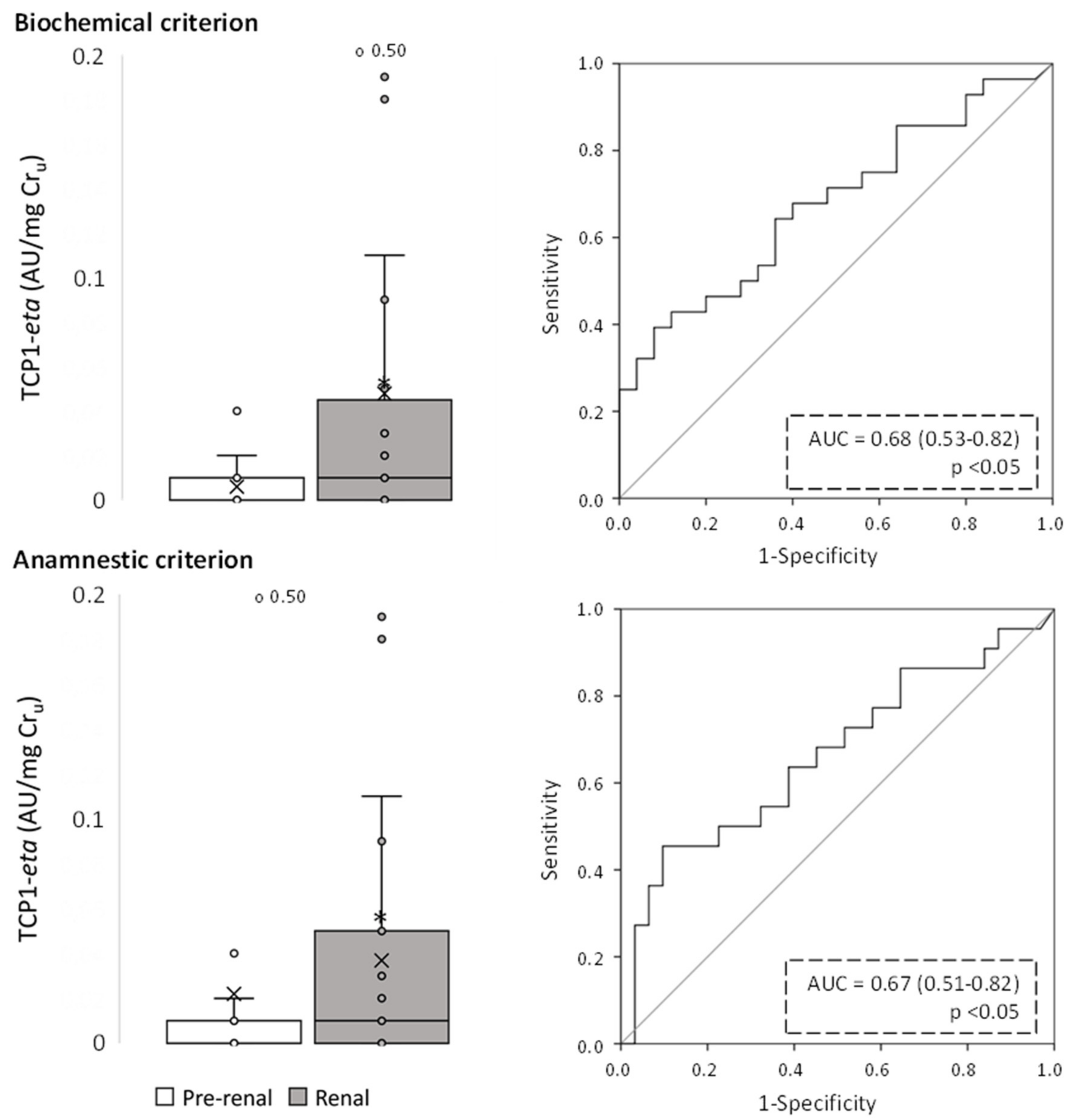
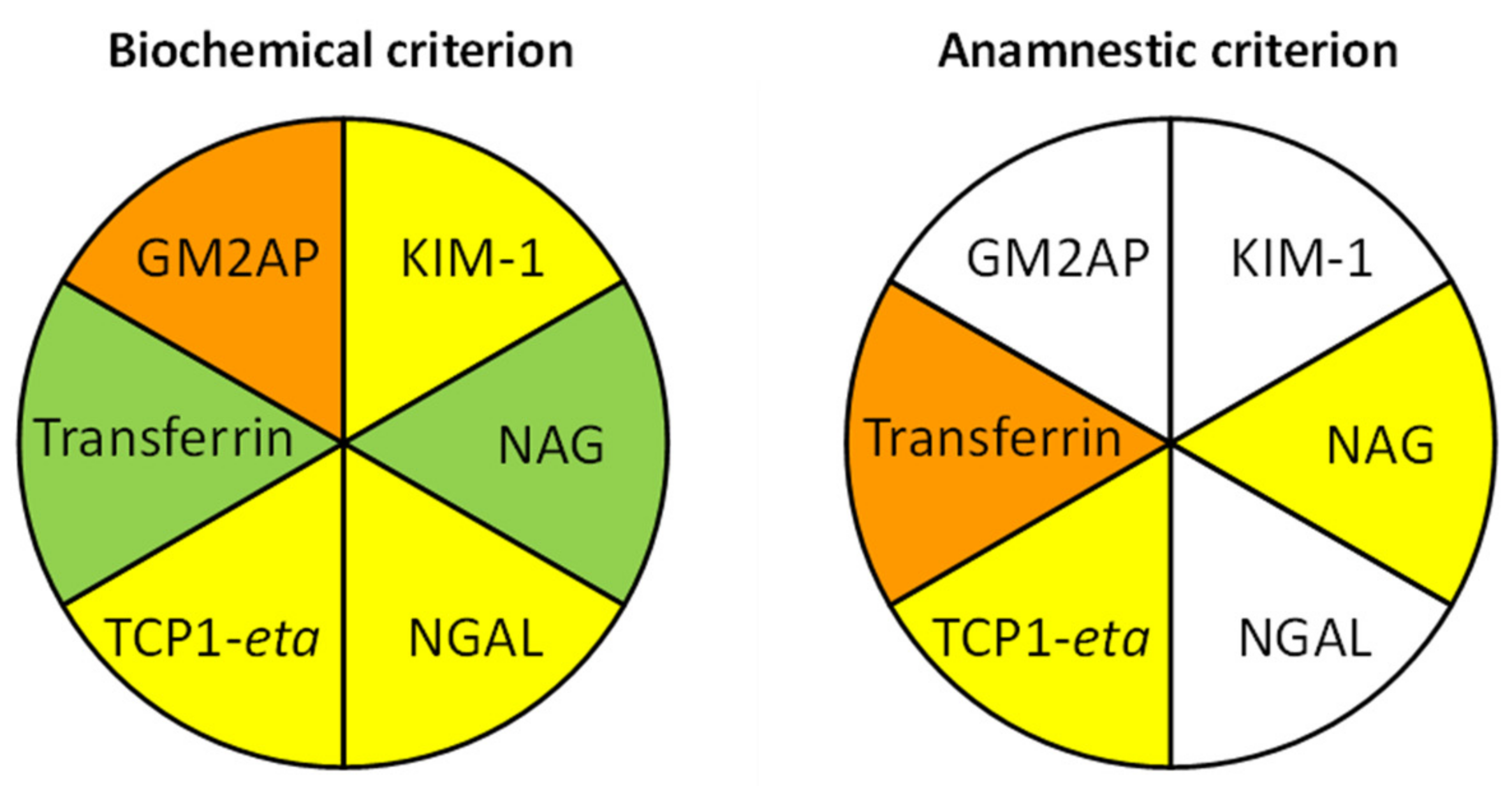
2.2. Evaluation of Urinary Biomarkers
2.3. Evaluation of the Influence of Diuretic Treatment on Patient Classification Mismatch
3. Discussion
4. Materials and Methods
4.1. Patients and Protocols
- The anamnestic criterion classified patients under pre-renal AKI when a decrease in circulating volume was suspected, (i) as per fluid loss following hemorrhage, diarrhea, vomiting, abundant debit by nasogastric tube, diuretics, osmotic diuresis, diabetes insipidus, adrenal insufficiency, fever, burns, tachypnea, etc.; (ii) due to extracellular fluid redistribution, as in edematous states, pancreatitis, peritonitis, intestinal obstruction, crush syndrome, etc.; or (iii) when symptoms of renal hypoperfusion were evident, as in patients with heart failure or shock, suspicion of renal vasoconstriction (as in hepatorenal syndrome, sepsis, use of alpha-adrenergic therapy or hypercalcemia) or drugs altering renal autoregulation (e.g., NSAIDs, calcineurin inhibitors, ACE inhibitors, ARA II, etc.). In these situations, arterial hypotension, orthostatism, and tachycardia may be observed. On examination, mucosal dryness, ocular hypotonicity, decreased central venous pressure or pulmonary capillary pressure, diuretic response to volume expansion and improvement after cause withdrawal also supported pre-renal classification. Renal hypoperfusion, mainly in severe or prolonged forms of ischemia, can condition ATN. Patients with hypotension during surgery, bleeding or sepsis have an increased risk of developing ischemic ATN, especially in the presence of other associated pathologies, such as previous chronic renal failure, diabetes mellitus, arteriosclerosis or malnutrition. Prerenal forms of AKI due to hypovolemia or decreased effective circulating volume due to heart failure or liver disease may also be perpetuated and lead to ischemic ATN. Clinically, it differs from prerenal ARF in that renal hypoperfusion causes damage to the tubular cells, and in that after establishing the appropriate treatment, there is no increase in diuresis nor a decrease in azotemia.
- The biochemical criterion was based on the following ratios: (i) Urinary creatinine/plasma creatinine ratio (Cru/Crp), with values > 20 indicating pre-renal AKI and <20 renal AKI. (ii) Fractional excretion of sodium [FENa = (Nau × Crp)/(Nap × Cru) × 100], with values < 1 indicating pre-renal AKI and >1 renal AKI. (iii) Renal Failure Index (RFI) = (Nau × Crp)/Cru. with values < 1 indicating pre-renal AKI and >1 renal AKI [26,60,61,62,63]. Nap and Nau stand for plasma and urinary Na concentration, respectively, and Crp and Cru for plasma and urinary creatinine concentration. For the biochemical criterion, patients were classified as pre-renal or renal AKI when meeting at least two (of the three) ratios for pre-renal or renal AKI. Renal function and diagnostic data, as well as Nap, Nau and Crp, were obtained from the patients’ medical records. Cru was measured with a Quantichrom Creatinine Assay Kit (BioAssay Systems, Hayward, CA, USA) according to the manufacturer’s instructions.
4.2. Biomarker Measurement
4.3. Data and Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Endre, Z.H.; Kellum, J.A.; Di Somma, S.; Doi, K.; Goldstein, S.L.; Koyner, J.L.; MacEdo, E.; Mehta, R.L.; Murray, P.T. Differential diagnosis of AKI in clinical practice by functional and damage biomarkers: Workgroup statements from the tenth Acute Dialysis Quality Initiative Consensus Conference. Contrib. Nephrol. 2013, 182, 30–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sutherland, S.M.; Byrnes, J.J.; Kothari, M.; Longhurst, C.A.; Dutta, S.; Garcia, P.; Goldstein, S.L. AKI in hospitalized children: Comparing the pRIFLE, AKIN, and KDIGO definitions. Clin. J. Am. Soc. Nephrol. 2015, 10, 554–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, M.; Bedford, M.; Matthews, B.; O’donoghue, D. The economic impact of acute kidney injury in England. Nephrol. Dial. Transplant. 2014, 29, 1362–1368. [Google Scholar] [CrossRef] [Green Version]
- Chertow, G.M.; Burdick, E.; Honour, M.; Bonventre, J.V.; Bates, D.W. Acute kidney injury, mortality, length of stay, and costs in hospitalized patients. J. Am. Soc. Nephrol. 2005, 16, 3365–3370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandijck, D.M.; Oeyen, S.; Decruyenaere, J.M.; Annemans, L.; Hoste, E.A. Acute kidney injury, length of stay, and costs in patients hospitalized in the intensive care unit. Acta Clin. Belg. 2007, 62, 341–345. [Google Scholar] [CrossRef]
- Neild, G.H. Multi-organ renal failure in the elderly. Int. Urol. Nephrol. 2001, 32, 559–565. [Google Scholar] [CrossRef]
- Block, C.A.; Schoolwerth, A.C. The epidemiology and outcome of acute renal failure and the impact on chronic kidney disease. Semin. Dial. 2006, 19, 450–454. [Google Scholar] [CrossRef]
- Kellum, J.A.; Hoste, E.A.J. Acute kidney injury: Epidemiology and assessment. Scand. J. Clin. Lab. Investig. 2008, 68, 6–11. [Google Scholar] [CrossRef]
- Waikar, S.S.; Liu, K.D.; Chertow, G.M. Diagnosis, epidemiology and outcomes of acute kidney injury. Clin. J. Am. Soc. Nephrol. 2008, 3, 844–861. [Google Scholar] [CrossRef] [Green Version]
- Fujii, T.; Uchino, S.; Doi, K.; Sato, T.; Kawamura, T.; JAKID Study Group. Diagnosis, management, and prognosis of patients with acute kidney injury in Japanese intensive care units: The JAKID study. J. Crit. Care 2018, 47, 185–191. [Google Scholar] [CrossRef]
- Pannu, N.; James, M.; Hemmelgarn, B.; Klarenbach, S. Alberta Kidney Disease Network Association between AKI, recovery of renal function, and long-term outcomes after hospital discharge. Clin. J. Am. Soc. Nephrol. 2013, 8, 194–202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, E.; Antonelli, M.; Wittebole, X.; Nanchal, R.; François, B.; Sakr, Y.; Vincent, J.-L.; Pickkers, P. A worldwide multicentre evaluation of the influence of deterioration or improvement of acute kidney injury on clinical outcome in critically ill patients with and without sepsis at ICU admission: Results from The Intensive Care Over Nations audit. Crit. Care 2018, 22, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldberg, R.; Dennen, P. Long-Term Outcomes of Acute Kidney Injury. Adv. Chronic Kidney Dis. 2008, 15, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Palant, C.E.; Amdur, R.L.; Chawla, L.S. The acute kidney injury to chronic kidney disease transition: A potential opportunity to improve care in acute kidney injury. Contrib. Nephrol. 2016, 187, 55–72. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [Green Version]
- Kellum, J.A.; Sileanu, F.E.; Bihorac, A.; Hoste, E.A.J.; Chawla, L.S. Recovery after acute kidney injury. Am. J. Respir. Crit. Care Med. 2017, 195, 784–791. [Google Scholar] [CrossRef] [Green Version]
- Cerdá, J.; Liu, K.D.; Cruz, D.N.; Jaber, B.L.; Koyner, J.L.; Heung, M.; Okusa, M.D.; Faubel, S.; AKI Advisory Group of the American Society of Nephrology. Promoting Kidney Function Recovery in Patients with AKI Requiring RRT. Clin. J. Am. Soc. Nephrol. 2015, 10, 1859–1867. [Google Scholar] [CrossRef] [Green Version]
- Sancho-Martínez, S.M.; Prieto, L.; Blanco-Gozalo, V.; Fontecha-Barriuso, M.; Vicente-Vicente, L.; Casanova, A.G.; Prieto, M.; Pescador, M.; Morales, A.I.; López-Novoa, J.M.; et al. Acute tubular necrosis: An old term in search for a new meaning within the evolving concept of acute kidney injury. New Horiz. Transl. Med. 2015, 2, 110. [Google Scholar] [CrossRef] [Green Version]
- Yang, F.; Zhang, L.; Wu, H.; Zou, H.; Du, Y. Clinical analysis of cause, treatment and prognosis in acute kidney injury patients. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [Green Version]
- Sawhney, S.; Mitchell, M.; Marks, A.; Fluck, N.; Black, C. Long-term prognosis after acute kidney injury (AKI): What is the role of baseline kidney function and recovery? A systematic review. BMJ Open 2015, 5, e006497. [Google Scholar] [CrossRef]
- Kaufman, J.; Dhakal, M.; Patel, B.; Hamburger, R. Community-Acquired Acute Renal Failure. Am. J. Kidney Dis. 1991, 17, 191–198. [Google Scholar] [CrossRef]
- Clarkson, M.R.; Friedewald, J.J.; Eustace, J.A.; Rabb, H. Acute Kidney Injury. In Brenner and Rector’s the Kidney; Saunders: Philadelphia, PA, USA, 2007. [Google Scholar]
- Uchino, S. The meaning of transient azotemia. Contrib. Nephrol. 2010, 165, 337–344. [Google Scholar] [CrossRef]
- Uchino, S.; Bellomo, R.; Bagshaw, S.M.; Goldsmith, D. Transient azotaemia is associated with a high risk of death in hospitalized patients. Nephrol. Dial. Transplant. 2010, 25, 1833–1839. [Google Scholar] [CrossRef] [Green Version]
- Liaño, F.; Pascual, J.; Gámez, C.; Gallego, A.; Bajo, M.A.; Sicilia, L.S.; Junco, E.; Verde, E.; Bernis, C.; Traver, J.A.; et al. Epidemiology of acute renal failure: A prospective, multicenter, community-based study. Kidney Int. 1996, 50, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Esson, M.L.; Schrier, R.W. Diagnosis and treatment of acute tubular necrosis. Ann. Intern. Med. 2002, 137, 744–752. [Google Scholar] [CrossRef]
- Lee, V.W.S.; Harris, D.; Anderson, R.J.; Schrier, R.W. Acute renal failure. In Diseases of the Kidney and Urinary Tract; RW, S., Ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007. [Google Scholar]
- Rachoin, J.-S.; Daher, R.; Moussallem, C.; Milcarek, B.; Hunter, K.; Schorr, C.; Abboud, M.; Henry, P.; Weisberg, L.S. The fallacy of the BUN:creatinine ratio in critically ill patients. Nephrol. Dial. Transplant 2012, 27, 2248–2254. [Google Scholar] [CrossRef]
- Uchino, S.; Bellomo, R.; Goldsmith, D. The meaning of the blood urea nitrogen/creatinine ratio in acute kidney injury. Clin. Kidney J. 2012, 5, 187–191. [Google Scholar] [CrossRef] [Green Version]
- Murray, P.T.; Mehta, R.L.; Shaw, A.; Ronco, C.; Endre, Z.; Kellum, J.A.; Chawla, L.S.; Cruz, D.; Ince, C.; Okusa, M.D. Potential use of biomarkers in acute kidney injury: Report and summary of recommendations from the 10th Acute Dialysis Quality Initiative consensus conference. Kidney Int. 2014, 85, 513–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ronco, C.; Kellum, J.A.; Haase, M. Subclinical AKI is still AKI. Crit. Care 2012, 16, 313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, A.G.; Bellomo, R. Urinalysis and pre-renal acute kidney injury: Time to move on. Crit. Care 2013, 17, 141. [Google Scholar] [CrossRef] [PubMed]
- Nejat, M.; Pickering, J.W.; Devarajan, P.; Bonventre, J.V.; Edelstein, C.L.; Walker, R.J.; Endre, Z.H. Some biomarkers of acute kidney injury are increased in pre-renal acute injury. Kidney Int. 2012, 81, 1254–1262. [Google Scholar] [CrossRef] [Green Version]
- Kanbay, M.; Kasapoglu, B.; Perazella, M.A. Acute tubular necrosis and pre-renal acute kidney injury: Utility of urine microscopy in their evaluation- a systematic review. Int. Urol. Nephrol. 2010, 42, 425–433. [Google Scholar] [CrossRef]
- Cavanaugh, C.; Perazella, M.A. Urine Sediment Examination in the Diagnosis and Management of Kidney Disease: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 73, 258–272. [Google Scholar] [CrossRef] [Green Version]
- Perazella, M.A.; Coca, S.G.; Kanbay, M.; Brewster, U.C.; Parikh, C.R. Diagnostic value of urine microscopy for differential diagnosis of acute kidney injury in hospitalized patients. Clin. J. Am. Soc. Nephrol. 2008, 3, 1615–1619. [Google Scholar] [CrossRef] [Green Version]
- Carvounis, C.P.; Nisar, S.; Guro-Razuman, S. Significance of the fractional excretion of urea in the differential diagnosis of acute renal failure. Kidney Int. 2002, 62, 2223–2229. [Google Scholar] [CrossRef] [Green Version]
- Blanco-Gozalo, V.; Casanova, A.G.; Sancho-Martínez, S.M.; Prieto, M.; Quiros, Y.; Morales, A.I.; Martínez-Salgado, C.; Agüeros-Blanco, C.; Benito-Hernández, A.; Ramos-Barron, M.A.; et al. Combined use of GM2AP and TCP1-eta urinary levels predicts recovery from intrinsic acute kidney injury. Sci. Rep. 2020, 10, 11599. [Google Scholar] [CrossRef]
- Seibert, F.S.; Pagonas, N.; Arndt, R.; Heller, F.; Dragun, D.; Persson, P.; Schmidt-Ott, K.; Zidek, W.; Westhoff, T.H. Calprotectin and neutrophil gelatinase-associated lipocalin in the differentiation of pre-renal and intrinsic acute kidney injury. Acta Physiol. 2013, 207, 700–708. [Google Scholar] [CrossRef]
- Singer, E.; Elger, A.; Elitok, S.; Kettritz, R.; Nickolas, T.L.; Barasch, J.; Luft, F.C.; Schmidt-Ott, K.M. Urinary neutrophil gelatinase-associated lipocalin distinguishes pre-renal from intrinsic renal failure and predicts outcomes. Kidney Int. 2011, 80, 405–414. [Google Scholar] [CrossRef] [Green Version]
- Heller, F.; Frischmann, S.; Grünbaum, M.; Zidek, W.; Westhoff, T.H. Urinary calprotectin and the distinction between prerenal and intrinsic acute kidney injury. Clin. J. Am. Soc. Nephrol. 2011, 6, 2347–2355. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S.; Nakasatomi, M.; Takei, Y.; Ikeuchi, H.; Sakairi, T.; Kaneko, Y.; Hiromura, K.; Nojima, Y.; Maeshima, A. Identification of Urinary Activin A as a Novel Biomarker Reflecting the Severity of Acute Kidney Injury. Sci. Rep. 2018, 8, 5176. [Google Scholar] [CrossRef]
- Kim, A.J.; Ro, H.; Kim, H.; Chang, J.H.; Lee, H.H.; Chung, W.; Jung, J.Y. Klotho and S100A8/A9 as discriminative markers between pre-renal and intrinsic acute kidney injury. PLoS ONE 2016, 11, e0147255. [Google Scholar] [CrossRef] [PubMed]
- Ronco, C.; Bellomo, R.; Kellum, J.A. Acute kidney injury. Lancet 2019, 394, 1949–1964. [Google Scholar] [CrossRef] [PubMed]
- Nickolas, T.L.; Schmidt-Ott, K.M.; Canetta, P.; Forster, C.; Singer, E.; Sise, M.; Elger, A.; Maarouf, O.; Antonio, D.; Valle, S.-D.; et al. Diagnostic and Prognostic Stratification in the Emergency Department Using Urinary Biomarkers of Nephron Damage: A Multicenter Prospective Cohort Study. J. Am. Coll. Cardiol. 2012, 59, 246–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prieto-García, L.; Vicente-Vicente, L.; Blanco-Gozalo, V.; Hidalgo-Thomas, O.; García-Macías, M.C.; Kurtz, A.; Layton, A.T.; Sanz, A.B.; Morales, A.I.; Martínez-Salgado, C.; et al. Pathophysiological mechanisms underlying a rat model of triple whammy acute kidney injury. Lab. Investig. 2020, 100, 1455–1464. [Google Scholar] [CrossRef] [PubMed]
- Sancho-Martínez, S.M.; Herrero, M.; Fontecha-Barriuso, M.; Mercado-Hernández, J.; López-Hernández, F.J. The Urinary Level of Injury Biomarkers Is Not Univocally Reflective of the Extent of Toxic Renal Tubular Injury in Rats. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef]
- Sancho-Martínez, S.M.; Blanco-Gozalo, V.; Quiros, Y.; Prieto-García, L.; Montero-Gómez, M.J.; Docherty, N.G.; Martínez-Salgado, C.; Morales, A.I.; López-Novoa, J.M.; López-Hernández, F.J. Impaired Tubular Reabsorption Is the Main Mechanism Explaining Increases in Urinary NGAL Excretion Following Acute Kidney Injury in Rats. Toxicol. Sci. 2020, 175, 75–86. [Google Scholar] [CrossRef]
- Skrypnyk, N.I.; Gist, K.M.; Okamura, K.; Montford, J.R.; You, Z.; Yang, H.; Moldovan, R.; Bodoni, E.; Blaine, J.T.; Edelstein, C.L.; et al. IL-6-mediated hepatocyte production is the primary source of plasma and urine neutrophil gelatinase–associated lipocalin during acute kidney injury. Kidney Int. 2020, 97, 966–979. [Google Scholar] [CrossRef]
- Johnson, A.C.M.; Zager, R.A. Mechanisms underlying increased TIMP2 and IGFBP7 urinary excretion in experimental AKI. J. Am. Soc. Nephrol. 2018, 29, 2157–2167. [Google Scholar] [CrossRef] [Green Version]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Andreucci, M.; Faga, T.; Pisani, A.; Perticone, M.; Michael, A. The ischemic/nephrotoxic acute kidney injury and the use of renal biomarkers in clinical practice. Eur. J. Intern. Med. 2017, 39, 1–8. [Google Scholar] [CrossRef]
- Menez, S.; Parikh, C.R. Assessing the Health of the Nephron in AKI: Biomarkers of Kidney Function and Injury. Curr. Opin. Nephrol. Hypertens. 2019, 28, 560. [Google Scholar] [CrossRef]
- Sancho-Martínez, S.M.; Sánchez-Juanes, F.; Blanco-Gozalo, V.; Fontecha-Barriuso, M.; Prieto-García, L.; Fuentes-Calvo, I.; González-Buitrago, J.M.; Morales, A.I.; Martínez-Salgado, C.; Ramos-Barron, M.A.; et al. Urinary TCP1-eta: A Cortical Damage Marker for the Pathophysiological Diagnosis and Prognosis of Acute Kidney Injury. Toxicol. Sci. 2020, 174, 3–15. [Google Scholar] [CrossRef]
- Vicente-Vicente, L.; Casanova, A.G.; Hernández-Sánchez, M.T.; Prieto, M.; Martínez-Salgado, C.; López-Hernández, F.J.; Cruz-González, I.; Morales, A.I. Albuminuria Pre-Emptively Identifies Cardiac Patients at Risk of Contrast-Induced Nephropathy. J. Clin. Med. 2021, 10, 4942. [Google Scholar] [CrossRef]
- Quiros, Y.; Ferreira, L.; Sancho-Martínez, S.M.; González-Buitrago, J.M.; López-Novoa, J.M.; López-Hernández, F.J. Sub-nephrotoxic doses of gentamicin predispose animals to developing acute kidney injury and to excrete ganglioside M2 activator protein. Kidney Int. 2010, 78, 1006–1015. [Google Scholar] [CrossRef] [Green Version]
- Casanova, A.G.; Vicente-Vicente, L.; Hernández-Sánchez, M.T.; Prieto, M.; Rihuete, M.I.; Ramis, L.M.; del Barco, E.; Cruz, J.J.; Ortiz, A.; Cruz-González, I.; et al. Urinary transferrin pre-emptively identifies the risk of renal damage posed by subclinical tubular alterations. Biomed. Pharmacother. 2020, 121, 109684. [Google Scholar] [CrossRef]
- Vicente-Vicente, L.; Ferreira, L.; González-Buitrago, J.M.; López-Hernández, F.J.; López-Novoa, J.M.; Morales, A.I. Increased urinary excretion of albumin, hemopexin, transferrin and VDBP correlates with chronic sensitization to gentamicin nephrotoxicity in rats. Toxicology 2013, 304, 83–91. [Google Scholar] [CrossRef]
- Fuentes-Calvo, I.; Cuesta, C.; Sancho-Martínez, S.M.; Hidalgo-Thomas, O.A.; Paniagua-Sancho, M.; López-Hernández, F.J.; Martínez-Salgado, C. Biomarkers of persistent renal vulnerability after acute kidney injury recovery. Sci. Rep. 2021, 11, 21183. [Google Scholar] [CrossRef]
- Espinel, C.H. The FeNa Test: Use in the Differential Diagnosis of Acute Renal Failure. JAMA J. Am. Med. Assoc. 1976, 236, 579–581. [Google Scholar] [CrossRef]
- Miller, T.R.; Anderson, R.J.; Linas, S.L.; Henrich, W.L.; Berns, A.S.; Gabow, P.A.; Schrier, R.W. Urinary diagnostic indices in acute renal failure. A prospective study. Ann. Intern. Med. 1978, 89, 47–50. [Google Scholar] [CrossRef]
- Nally, J.V. Acute renal failure in hospitalized patients. Cleve. Clin. J. Med. 2002, 69, 569–574. [Google Scholar] [CrossRef]
- Lima, C.; Macedo, E. Urinary Biochemistry in the Diagnosis of Acute Kidney Injury. Dis. Markers 2018, 2018, 4907024. [Google Scholar] [CrossRef] [PubMed]
- Hajian-Tilaki, K. Receiver operating characteristic (ROC) curve analysis for medical diagnostic test evaluation. Casp. J. Intern. Med. 2013, 4, 627–635. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Biochemical Criterion | Anamnestic Criterion | ||||
|---|---|---|---|---|---|---|
| Pre-Renal AKI (n = 25) | Renal AKI (n = 28) | p-Value | Pre-Renal AKI (n = 31) | Renal AKI (n = 22) | p-Value | |
| Gender (male/female, %) | 48.0/52.0 | 35.7/64.3 | 0.28 | 45.2/54.8 | 72.7/27.3 | 0.06 |
| Age (years) | 71.0 (27–92) | 75.5 (40–89) | 0.62 | 72.0 (27–92) | 73.5 (40–89) | 0.70 |
| Obesity (no/yes, %) | 66.7/33.3 | 94.1/5.9 | 0.13 | 75.0/25.0 | 88.2/11.8 | 0.62 |
| Diabetes mellitus (no/yes, %) | 72.0/28.0 | 60.7/39.3 | 0.56 | 67.7/32.3 | 63.6/36.4 | 0.78 |
| Hypertension (no/yes, %) | 12.0/88.0 | 25.0/75.0 | 0.30 | 12.9/87.1 | 27.3/72.7 | 0.29 |
| Heart disease (no/yes, %) | 52.0/48.0 | 67.9/32.1 | 0.27 | 58.1/41.9 | 63.6/36.4 | 0.78 |
| Ischemic (no/yes, %) | 60.0/40.0 | 67.9/32.1 | 0.58 | 64.5/35.5 | 63.6/36.4 | 1.00 |
| Valvular (no/yes, %) | 68.0/32.0 | 89.3/10.7 | 0.09 | 71.0/29.0 | 90.9/9.1 | 0.10 |
| Smoking (no/yes, %) | 78.3/21.7 | 76.0/24.0 | 1.00 | 81.5/18.5 | 71.4/28.6 | 0.50 |
| Previous pharmacological treatment: | ||||||
| ACEIs (no/yes, %) | 64.0/36.0 | 71.4/28.6 | 0.77 | 61.3/38.7 | 77.3/22.7 | 0.25 |
| ARBs (no/yes, %) | 60.0/40.0 | 41.4/28.6 | 0.40 | 64.5/35.5 | 68.2/31.8 | 1.00 |
| Diuretics (no/yes, %) | 36.0/64.0 | 42.9/57.1 | 0.78 | 29.0/71.0 | 54.5/45.5 | 0.09 |
| NSAIDs (no/yes, %) | 81.8/18.2 | 73.1/26.9 | 0.51 | 76.9/23.1 | 77.3/22.7 | 1.00 |
| Contrast medium (no/yes, %) | 96.0/4.0 | 100.0/0.0 | 0.48 | 96.8/3.2 | 100.0/0.0 | 1.00 |
| Plasma creatinine (mg/dL) | 5.3 (1.7–12.5) | 4.3 (1.9–13.5) | 0.93 | 5.3 (1.7–13.5) | 4.0 (1.9–9.5) | 0.15 |
| Biochemical Criterion | ||||
|---|---|---|---|---|
| Parameter | B | SD | Wald | p-value |
| Logistic regression analysis (only transferrin) | ||||
| Transferrin (ng/mg Cru) | 0.095 | 0.040 | 5.734 | 0.017 |
| Constant | −1.209 | 0.540 | 5.009 | 0.025 |
| Specificity: 81.8%; Sensitivity: 61.5%; Percentage of success: 70.8% | ||||
| Logistic regression analysis (transferrin and NAG) | ||||
| Transferrin (ng/mg Cru) | 0.095 | 0.040 | 5.510 | 0.019 |
| NAG (IU/mg Cru) | 70.28 | 30.02 | 5.481 | 0.019 |
| Constant | −2.376 | 0.809 | 8.622 | 0.003 |
| Specificity: 77.3%; Sensitivity: 76.9%; Percentage of success: 77.1% | ||||
| Anamnestic Criterion | ||||
| No significant model was obtained for any of the biomarkers analyzed. | ||||
| Presence of Diuretic Treatment | Number of Patients with Coincident Etiological AKI Classification (Pre-Renal/Renal) | p-Value | ||
|---|---|---|---|---|
| Non-Coincident | Coincident | |||
| Any Diuretic | No | 2 | 19 | 0.46 |
| Yes | 6 | 26 | ||
| Thiazides | No | 5 | 26 | 1.00 |
| Yes | 3 | 19 | ||
| Loop diuretics | No | 4 | 35 | 0.19 |
| Yes | 4 | 10 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sancho-Martínez, S.M.; Casanova, A.G.; Düwel, A.G.; Rivero-García, K.; García-Garrido, T.; Morales, A.I.; Martínez-Salgado, C.; López-Hernández, F.J.; Fraile, P. Identification of Pre-Renal and Intrinsic Acute Kidney Injury by Anamnestic and Biochemical Criteria: Distinct Association with Urinary Injury Biomarkers. Int. J. Mol. Sci. 2023, 24, 1826. https://doi.org/10.3390/ijms24031826
Sancho-Martínez SM, Casanova AG, Düwel AG, Rivero-García K, García-Garrido T, Morales AI, Martínez-Salgado C, López-Hernández FJ, Fraile P. Identification of Pre-Renal and Intrinsic Acute Kidney Injury by Anamnestic and Biochemical Criteria: Distinct Association with Urinary Injury Biomarkers. International Journal of Molecular Sciences. 2023; 24(3):1826. https://doi.org/10.3390/ijms24031826
Chicago/Turabian StyleSancho-Martínez, Sandra M., Alfredo G. Casanova, Annette G. Düwel, Karen Rivero-García, Tamara García-Garrido, Ana I. Morales, Carlos Martínez-Salgado, Francisco J. López-Hernández, and Pilar Fraile. 2023. "Identification of Pre-Renal and Intrinsic Acute Kidney Injury by Anamnestic and Biochemical Criteria: Distinct Association with Urinary Injury Biomarkers" International Journal of Molecular Sciences 24, no. 3: 1826. https://doi.org/10.3390/ijms24031826