


Influence of Occlusal Hypofunction on Alveolar Bone Healing in Rats
 , , , and
, , , and 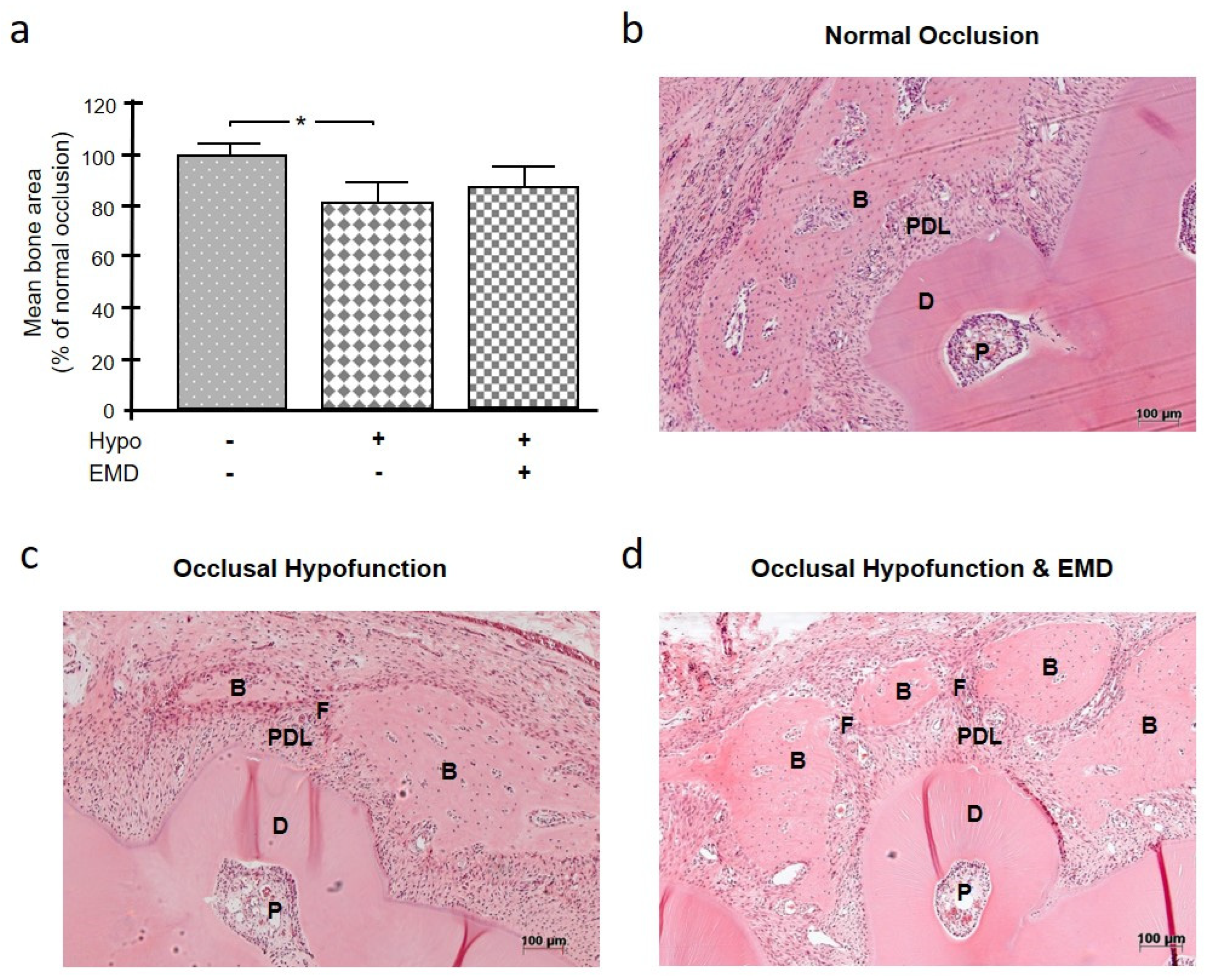{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Effect of Occlusal Hypofunction on Alveolar Bone Healing
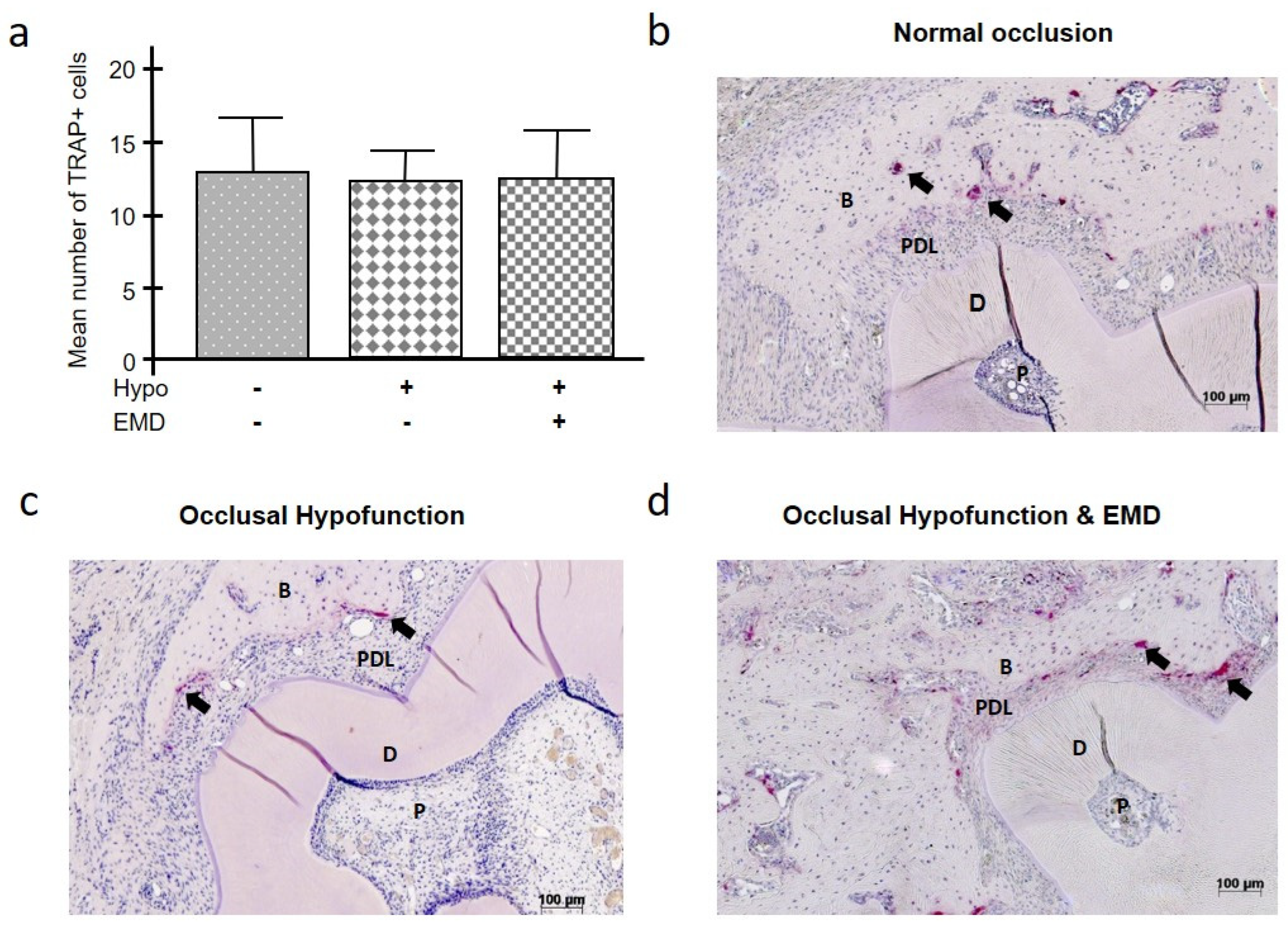
2.2. Influence of Occlusal Hypofunction on the Number of TRAP+ Cells
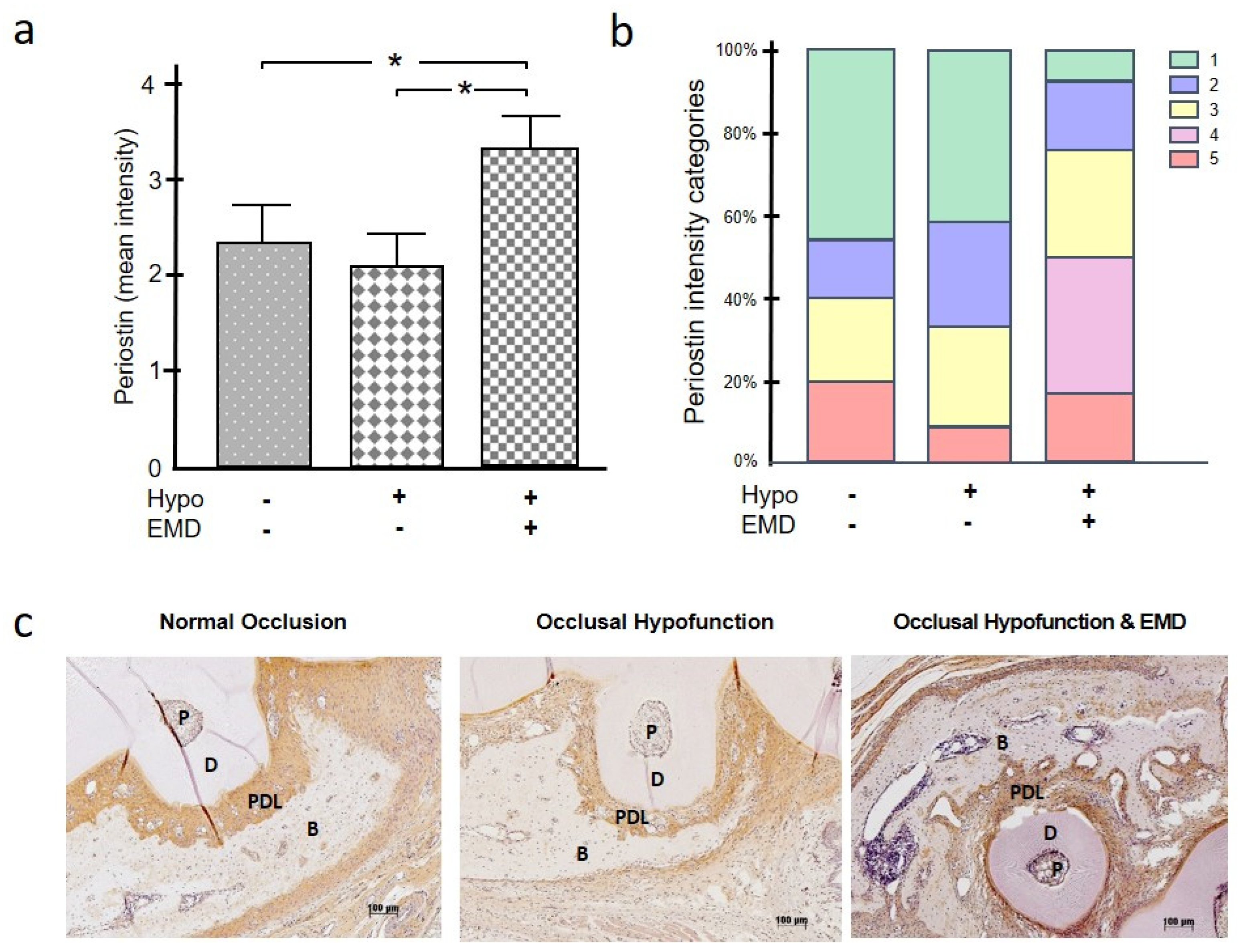
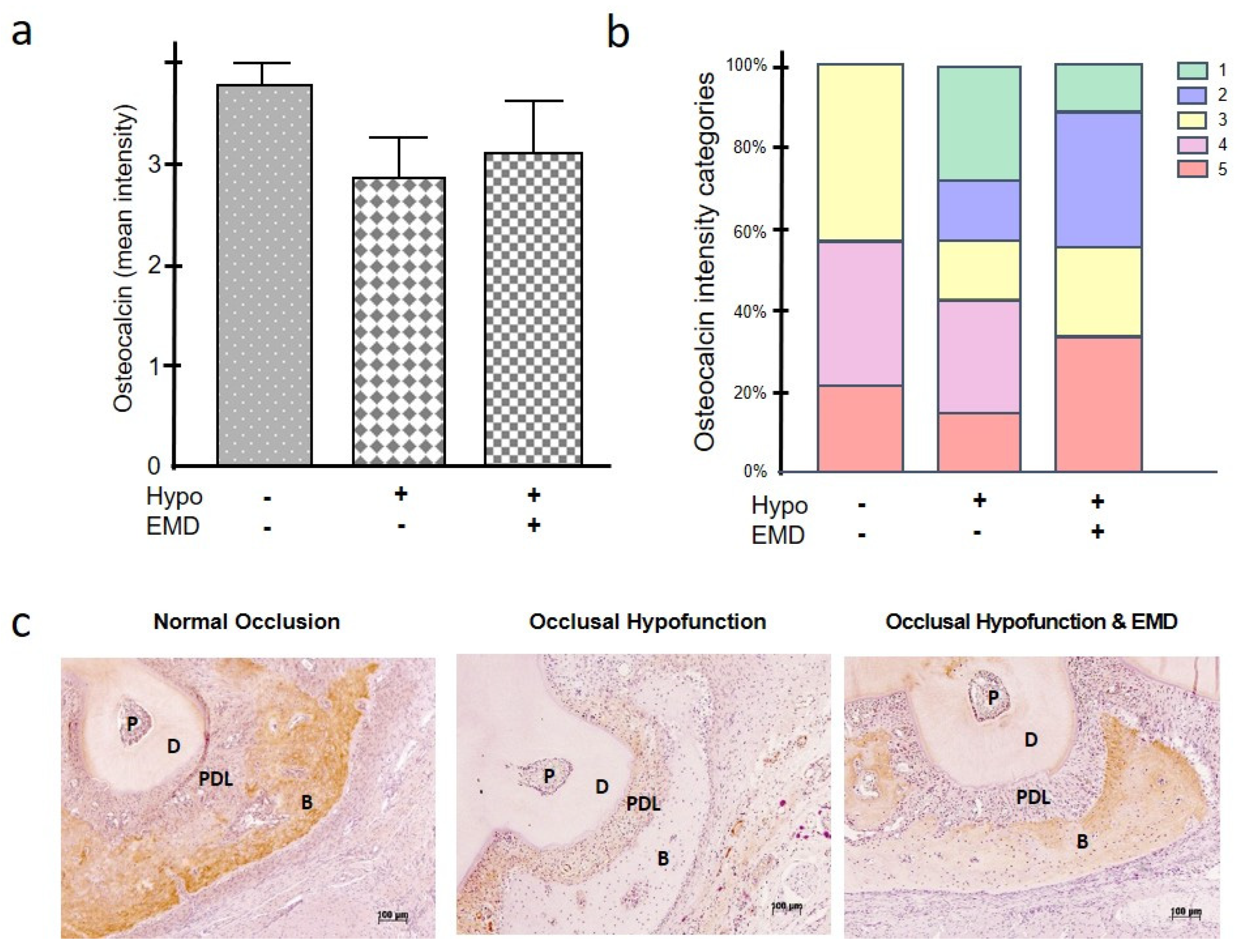
2.3. Effect of Occlusal Hypofunction on Periostin, Osteopontin, and Osteocalcin
3. Discussion
4. Materials and Methods
4.1. Animal Model
4.2. Surgical Procedures
4.3. Histological Preparation and Staining
4.4. Immunohistochemical Staining
4.5. Histomorphometric Evaluation
4.6. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| B | bone |
| BMP-2 | bone morphogenetic protein 2 |
| D | dentin |
| EDTA | ethylenediaminetetraacetic acid |
| EMD | enamel matrix derivative |
| H&E | hematoxylin and eosin |
| OPG | osteoprotegerin |
| P | pulp |
| PDL | periodontal ligament |
| RANKL | receptor activator of nuclear factor-kappa B ligand |
| ROI | region of interest |
| TRAP | tartrate-resistant acid phosphate |
References
- Hajishengallis, G.; Chavakis, T.; Lambris, J.D. Current understanding of periodontal disease pathogenesis and targets for host-modulation therapy. Periodontology 2020, 84, 14–34. [Google Scholar] [CrossRef] [PubMed]
- Fragkioudakis, I.; Riggio, M.P.; Apatzidou, D.A. Understanding the microbial components of periodontal diseases and periodontal treatment-induced microbiological shifts. J. Med. Microbiol. 2021, 70, 001247. [Google Scholar] [CrossRef] [PubMed]
- Ramseier, C.A.; Anerud, A.; Dulac, M.; Lulic, M.; Cullinan, M.P.; Seymour, G.J.; Faddy, M.J.; Bürgin, W.; Schätzle, M.; Lang, N.P. Natural history of periodontitis: Disease progression and tooth loss over 40 years. J. Clin. Periodontol. 2017, 44, 1182–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stöhr, J.; Barbaresko, J.; Neuenschwander, M.; Schlesinger, S. Bidirectional association between periodontal disease and diabetes mellitus: A systematic review and meta-analysis of cohort studies. Sci. Rep. 2021, 1, 13686. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.Z.; Yuan, Y.H.; Liu, H.H.; Li, S.S.; Zhang, B.W.; Chen, W.; An, Z.J.; Chen, S.Y.; Wu, Y.Z.; Han, B.; et al. Epidemiologic relationship between periodontitis and type 2 diabetes mellitus. BMC Oral. Health 2020, 11, 204. [Google Scholar] [CrossRef]
- Dicembrini, I.; Serni, L.; Monami, M.; Caliri, M.; Barbato, L.; Cairo, F.; Mannucci, E. Type 1 diabetes and periodontitis: Prevalence and periodontal destruction-a systematic review. Acta Diabetol. 2020, 57, 1405–1412. [Google Scholar] [CrossRef]
- Nascimento, G.G.; Leite, F.R.M.; Vestergaard, P.; Scheutz, F.; López, R. Does diabetes increase the risk of periodontitis? A systematic review and meta-regression analysis of longitudinal prospective studies. Acta Diabetol. 2018, 55, 653–667. [Google Scholar] [CrossRef]
- Loos, B.G.; Van Dyke, T.E. The role of inflammation and genetics in periodontal disease. Periodontology 2020, 83, 26–39. [Google Scholar] [CrossRef]
- Genco, R.J.; Borgnakke, W.S. Risk factors for periodontal disease. Periodontology 2013, 62, 59–94. [Google Scholar] [CrossRef]
- Available online: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed on 26 January 2023).
- Broers, D.L.M.; Dubois, L.; de Lange, J.; Su, N.; de Jongh, A. Reasons for Tooth Removal in Adults: A Systematic Review. Int. Dent. J. 2022, 72, 52–57. [Google Scholar] [CrossRef]
- Wu, L.; Zhang, S.Q.; Zhao, L.; Ren, Z.H.; Hu, C.Y. Global, regional, and national burden of periodontitis from 1990 to 2019: Results from the Global Burden of Disease study 2019. J. Periodontol. 2022, 93, 1445–1454. [Google Scholar] [CrossRef] [PubMed]
- Kanasi, E.; Ayilavarapu, S.; Jones, J. The aging population: Demographics and the biology of aging. Periodontology 2016, 72, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Jepsen, S.; Jin, L.; Otomo-Corgel, J. Impact of the global burden of periodontal diseases on health, nutrition and wellbeing of mankind: A call for global action. J. Clin. Periodontol. 2017, 44, 456–462. [Google Scholar] [CrossRef] [Green Version]
- Baniasadi, K.; Armoon, B.; Higgs, P.; Bayat, A.H.; Mohammadi Gharehghani, M.A.; Hemmat, M.; Fakhri, Y.; Mohammadi, R.; Fattah Moghaddam, L.; Schroth, R.J. The Association of Oral Health Status and socio-economic determinants with Oral Health-Related Quality of Life among the elderly: A systematic review and meta-analysis. Int. J. Dent. Hyg. 2021, 19, 153–165. [Google Scholar] [CrossRef]
- Chapple, I.L.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingstrom, P.; et al. Interaction of lifestyle, behaviour or systemic diseases with dental caries and periodontal diseases: Consensus report of group 2 of the joint EFP/ORCA workshop on the boundaries between caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Cianetti, S.; Valenti, C.; Orso, M.; Lomurno, G.; Nardone, M.; Lomurno, A.P.; Pagano, S.; Lombardo, G. Systematic Review of the Literature on Dental Caries and Periodontal Disease in Socio-Economically Disadvantaged Individuals. Int. J. Environ. Res. Public Health 2021, 24, 12360. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Periodontol. 2018, 89, 159–172. [Google Scholar] [CrossRef] [Green Version]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S. EFP Workshop Participants and Methodological Consultant. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49, 4–71. [Google Scholar] [CrossRef]
- Suvan, J.; Leira, Y.; Moreno Sancho, F.M.; Graziani, F.; Derks, J.; Tomasi, C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J. Clin. Periodontol. 2020, 47, 155–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakubovics, N.S.; Goodman, S.D.; Mashburn-Warren, L.; Stafford, G.P.; Cieplik, F. The dental plaque biofilm matrix. Periodontology 2021, 86, 32–56. [Google Scholar] [CrossRef]
- Graziani, F.; Karapetsa, D.; Alonso, B.; Herrera, D. Nonsurgical and surgical treatment of periodontitis: How many options for one disease? Periodontolpgy 2017, 75, 152–188. [Google Scholar] [CrossRef]
- Kwon, T.; Lamster, I.B.; Levin, L. Current Concepts in the Management of Periodontitis. Int. Dent. J. 2021, 71, 462–476. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Sculean, A.; Cochran, D.L.; Froum, S.; Zucchelli, G.; Nemcovsky, C.; Donos, N.; Lyngstadaas, S.P.; Deschner, J.; Dard, M.; et al. Twenty years of enamel matrix derivative: The past, the present and the future. J. Clin. Periodontol. 2016, 43, 668–683. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Gennai, S.; Hirschfeld, J.; Kalemaj, Z.; Buti, J.; Graziani, F. Regenerative surgical treatment of furcation defects: A systematic review and Bayesian network meta-analysis of randomized clinical trials. J. Clin. Periodontol. 2020, 47, 352–374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tu, Y.K.; Needleman, I.; Chambrone, L.; Lu, H.K.; Faggion, C.M., Jr. A Bayesian network meta-analysis on comparisons of enamel matrix derivatives, guided tissue regeneration and their combination therapies. J. Clin. Periodontol. 2012, 39, 303–314. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Bertl, K.; Spineli, L.M.; Sculean, A.; Cortellini, P.; Tonetti, M. Medium- and long-term clinical benefits of periodontal regenerative/reconstructive procedures in intrabony defects: Systematic review and network meta-analysis of randomized controlled clinical studies. J. Clin. Periodontol. 2021, 48, 410–430. [Google Scholar] [CrossRef]
- Yukna, R.A.; Mellonig, J.T. Histologic evaluation of periodontal healing in humans following regenerative therapy with enamel matrix derivative. A 10-case series. J. Periodontol. 2000, 71, 752–759. [Google Scholar] [CrossRef]
- McGuire, M.K.; Cochran, D.L. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 2: Histological evaluation. J. Periodontol. 2003, 74, 1126–1135. [Google Scholar] [CrossRef]
- Sculean, A.; Junker, R.; Donos, N.; Windisch, P.; Brecx, M.; Dünker, N. Immunohistochemical evaluation of matrix molecules associated with wound healing following treatment with an enamel matrix protein derivative in humans. Clin. Oral. Investig. 2003, 7, 167–174. [Google Scholar] [CrossRef]
- Nokhbehsaim, M.; Winter, J.; Rath, B.; Jäger, A.; Jepsen, S.; Deschner, J. Effects of enamel matrix derivative on periodontal wound healing in an inflammatory environment in vitro. J. Clin. Periodontol. 2011, 38, 479–490. [Google Scholar] [CrossRef]
- Inaba, H.; Kawai, S.; Nakayama, K.; Okahashi, N.; Amano, A. Effect of enamel matrix derivative on periodontal ligament cells in vitro is diminished by Porphyromonas gingivalis. J. Periodontol. 2004, 75, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, M.G.; Campos, M.L.; Benatti, B.B.; Marques, M.R.; Casati, M.Z.; Nociti, F.H., Jr.; Sallum, E.A. The impact of cigarette smoke inhalation on the outcome of enamel matrix derivative treatment in rats: Histometric analysis. J. Periodontol. 2010, 81, 1820–1828. [Google Scholar] [CrossRef]
- Deschner, J.; Nokhbehsaim, M. Regulatory effects of inflammatory and biomechanical signals on regenerative periodontal healing. Int. J. Oral. Maxillofac. Implants 2013, 28, 472–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laaksonen, M.; Salo, T.; Vardar-Sengul, S.; Atilla, G.; Saygan, B.H.; Simmer, J.P.; Baylas, H.; Sorsa, T. Gingival crevicular fluid can degrade Emdogain and inhibit Emdogain-induced proliferation of periodontal ligament fibroblasts. J. Periodontal. Res. 2010, 45, 353–360. [Google Scholar] [CrossRef] [PubMed]
- De Ry, S.P.; Pagnamenta, M.; Ramseier, C.A.; Roccuzzo, A.; Salvi, G.E.; Sculean, A. Five-year results following regenerative periodontal surgery with an enamel matrix derivative in patients with different smoking status. Quintessence Int. 2022, 21, 832–838. [Google Scholar]
- Takeda, K.; Mizutani, K.; Matsuura, T.; Kido, D.; Mikami, R.; Noda, M.; Buranasin, P.; Sasaki, Y.; Izumi, Y. Periodontal regenerative effect of enamel matrix derivative in diabetes. PLoS ONE 2018, 15, 0207201. [Google Scholar] [CrossRef]
- Deschner, J.; Eick, S.; Damanaki, A.; Nokhbehsaim, M. The role of adipokines in periodontal infection and healing. Mol. Oral. Microbiol. 2014, 29, 258–269. [Google Scholar] [CrossRef]
- Nokhbehsaim, M.; Deschner, B.; Winter, J.; Bourauel, C.; Jäger, A.; Jepsen, S.; Deschner, J. Anti-inflammatory effects of EMD in the presence of biomechanical loading and interleukin-1β in vitro. Clin. Oral. Investig. 2012, 16, 275–283. [Google Scholar] [CrossRef]
- Nokhbehsaim, M.; Deschner, B.; Winter, J.; Bourauel, C.; Rath, B.; Jäger, A.; Jepsen, S.; Deschner, J. Interactions of regenerative, inflammatory and biomechanical signals on bone morphogenetic protein-2 in periodontal ligament cells. J. Periodontal. Res. 2011, 46, 374–381. [Google Scholar] [CrossRef]
- Nokhbehsaim, M.; Deschner, B.; Bourauel, C.; Reimann, S.; Winter, J.; Rath, B.; Jäger, A.; Jepsen, S.; Deschner, J. Interactions of enamel matrix derivative and biomechanical loading in periodontal regenerative healing. J. Periodontol. 2011, 82, 1725–1734. [Google Scholar] [CrossRef]
- Heng, N.H.; N’Guessan, P.D.; Kleber, B.M.; Bernimoulin, J.P.; Pischon, N. Enamel matrix derivative induces connective tissue growth factor expression in human osteoblastic cells. J. Periodontol. 2007, 78, 2369–2379. [Google Scholar] [CrossRef] [PubMed]
- Eggers, B.; Marciniak, J.; Deschner, J.; Stope, M.B.; Mustea, A.; Kramer, F.J.; Nokhbehsaim, M. Cold Atmospheric Plasma Promotes Regeneration-Associated Cell Functions of Murine Cementoblasts In Vitro. Int. J. Mol. Sci. 2021, 22, 5280. [Google Scholar] [CrossRef] [PubMed]
- Zeldich, E.; Koren, R.; Nemcovsky, C.; Weinreb, M. Enamel matrix derivative stimulates human gingival fibroblast proliferation via ERK. J. Dent. Res. 2007, 86, 41–46. [Google Scholar] [CrossRef]
- Kawase, T.; Okuda, K.; Momose, M.; Kato, Y.; Yoshie, H.; Burns, D.M. Enamel matrix derivative (EMDOGAIN) rapidly stimulates phosphorylation of the MAP kinase family and nuclear accumulation of smad2 in both oral epithelial and fibroblastic human cells. J. Periodontal Res. 2001, 36, 367–376. [Google Scholar] [CrossRef]
- Itoh, N.; Kasai, H.; Ariyoshi, W.; Harada, E.; Yokota, M.; Nishihara, T. Mechanisms involved in the enhancement of osteoclast formation by enamel matrix derivative. J. Periodontal Res. 2006, 41, 273–279. [Google Scholar] [CrossRef]
- Saito, K.; Konishi, I.; Nishiguchi, M.; Hoshino, T.; Fujiwara, T. Amelogenin binds to both heparan sulfate and bone morphogenetic protein 2 and pharmacologically suppresses the effect of noggin. Bone 2008, 43, 371–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sculean, A.; Auschill, T.M.; Donos, N.; Brecx, M.; Arweiler, N.B. Effect of an enamel matrix protein derivative (Emdogain) on ex vivo dental plaque vitality. J. Clin. Periodontol. 2001, 28, 1074–1078. [Google Scholar] [CrossRef]
- Spahr, A.; Lyngstadaas, S.P.; Boeckh, C.; Andersson, C.; Podbielski, A.; Haller, B. Effect of the enamel matrix derivative Emdogain on the growth of periodontal pathogens in vitro. J. Clin. Periodontol. 2002, 29, 62–72. [Google Scholar] [CrossRef]
- Shimomoto, Y.; Chung, C.J.; Iwasaki-Hayashi, Y.; Muramoto, T.; Soma, K. Effects of occlusal stimuli on alveolar/jaw bone formation. J. Dent. Res. 2007, 86, 47–51. [Google Scholar] [CrossRef]
- Oddie, G.W.; Schenk, G.; Angel, N.Z.; Walsh, N.; Guddat, L.W.; de Jersey, J.; Cassady, A.I.; Hamilton, S.E.; Hume, D.A. Structure, function, and regulation of tartrate-resistant acid phosphatase. Bone 2000, 27, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Ling, J.; Jiang, Q. Inflammasomes in Alveolar Bone Loss. Front. Immunol. 2021, 12, 691013. [Google Scholar] [CrossRef] [PubMed]
- Iezzi, G.; Mangano, C.; Barone, A.; Tirone, F.; Baggi, L.; Tromba, G.; Piattelli, A.; Giuliani, A. Jawbone remodeling: A conceptual study based on Synchrotron High-resolution Tomography. Sci. Rep. 2020, 10, 3777. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arita, Y.; Yoshinaga, Y.; Kaneko, T.; Kawahara, Y.; Nakamura, K.; Ohgi, K.; Arita, S.; Ryu, T.; Takase, M.; Sakagami, R. Glyburide inhibits the bone resorption induced by traumatic occlusion in rats. J. Periodontal Res. 2020, 55, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, Y.; Minagawa, T.; Okui, T.; Yamazaki, K. Resveratrol suppresses the alveolar bone resorption induced by artificial trauma from occlusion in mice. Oral. Dis. 2018, 24, 412–421. [Google Scholar] [CrossRef] [PubMed]
- Walker, C.G.; Ito, Y.; Dangaria, S.; Luan, X.; Diekwisch, T.G. RANKL, osteopontin, and osteoclast homeostasis in a hyperocclusion mouse model. Eur. J. Oral Sci. 2008, 116, 312–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, J.; Li, M. Functions of Periostin in Dental Tissues and Its Role in Periodontal Tissue Regeneration. Adv. Exp. Med. Biol. 2019, 1132, 63–72. [Google Scholar]
- Rodan, G.A. Osteopontin overview. Ann. N. Y. Acad. Sci. 1995, 21, 1–5. [Google Scholar] [CrossRef]
- Zoch, M.L.; Clemens, T.L.; Riddle, R.C. New insights into the biology of osteocalcin. Bone 2016, 82, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Bonnet, N.; Garnero, P.; Ferrari, S. Periostin action in bone. Mol. Cell Endocrinol. 2016, 5, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Yang, D.; Liu, R.; Liu, L.; Liao, H.; Wang, C.; Cao, Z. Involvement of CD147 in alveolar bone remodeling and soft tissue degradation in experimental periodontitis. J. Periodontal Res. 2017, 52, 704–712. [Google Scholar] [CrossRef]
- Terai, K.; Takano-Yamamoto, T.; Ohba, Y.; Hiura, K.; Sugimoto, M.; Sato, M.; Kawahata, H.; Inaguma, N.; Kitamura, Y.; Nomura, S. Role of osteopontin in bone remodeling caused by mechanical stress. J. Bone Miner. Res. 1999, 14, 839–849. [Google Scholar] [CrossRef] [PubMed]
- King, G.N.; Hughes, F.J. Effects of occlusal loading on ankylosis, bone, and cementum formation during bone morphogenetic protein-2-stimulated periodontal regeneration in vivo. J. Periodontol. 1999, 70, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Damanaki, A.; Memmert, S.; Nokhbehsaim, M.; Abedi, A.; Rath-Deschner, B.; Nogueira, A.; Deschner, J. Effects of Obesity on Bone Healing in Rats. Int. J. Mol. Sci. 2021, 11, 13339. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Kanno, Z.; Soma, K. Occlusal hypofunction induces atrophic changes in rat gingiva. Angle Orthod. 2008, 78, 1015–1022. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, Y.; Hosomichi, J.; Nakamura, S.; Ono, T. Micro-computed tomography analysis of changes in the periodontal ligament and alveolar bone proper induced by occlusal hypofunction of rat molars. Korean J. Orthod. 2014, 44, 263–267. [Google Scholar] [CrossRef] [Green Version]
- Kasahara, Y.; Usumi-Fujita, R.; Hosomichi, J.; Kaneko, S.; Ishida, Y.; Shibutani, N.; Shimizu, Y.; Okito, A.; Oishi, S.; Kuma, Y.; et al. Low-intensity pulsed ultrasound reduces periodontal atrophy in occlusal hypofunctional teeth. Angle Orthod. 2017, 87, 709–716. [Google Scholar] [CrossRef] [Green Version]
- Kunii, R.; Yamaguchi, M.; Aoki, Y.; Watanabe, A.; Kasai, K. Effects of experimental occlusal hypofunction, and its recovery, on mandibular bone mineral density in rats. Eur. J. Orthod. 2008, 30, 52–56. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; Dai, W.; Wang, P.; Zhang, X.; Tang, Y.; Liu, L.; Wang, Q.; Li, M.; Tang, C. Periostin promotes migration, proliferation, and differentiation of human periodontal ligament mesenchymal stem cells. Connect. Tissue Res. 2018, 59, 108–119. [Google Scholar] [CrossRef]
- Choi, J.W.; Arai, C.; Ishikawa, M.; Shimoda, S.; Nakamura, Y. Fiber system degradation, and periostin and connective tissue growth factor level reduction, in the periodontal ligament of teeth in the absence of masticatory load. J. Periodontal Res. 2011, 46, 513–521. [Google Scholar] [CrossRef]
- Ivanovski, S.; Li, H.; Haase, H.R.; Bartold, P.M. Expression of bone associated macromolecules by gingival and periodontal ligament fibroblasts. J. Periodontal Res. 2001, 36, 131–141. [Google Scholar] [CrossRef]
- Hassumi, J.S.; Mulinari-Santos, G.; Fabris, A.L.D.S.; Jacob, R.G.M.; Gonçalves, A.; Rossi, A.C.; Freire, A.R.; Faverani, L.P.; Okamoto, R. Alveolar bone healing in rats: Micro-CT, immunohistochemical and molecular analysis. J. Appl. Oral. Sci. 2018, 18, 20170326. [Google Scholar] [CrossRef]
- Lekic, P.; Sodek, J.; McCulloch, C.A. Osteopontin and bone sialoprotein expression in regenerating rat periodontal ligament and alveolar bone. Anat. Rec. 1996, 244, 50–58. [Google Scholar] [CrossRef]
- Galli, C.; Macaluso, G.M.; Guizzardi, S.; Vescovini, R.; Passeri, M.; Passeri, G. Osteoprotegerin and receptor activator of nuclear factor-kappa B ligand modulation by enamel matrix derivative in human alveolar osteoblasts. J. Periodontol. 2006, 77, 1223–1228. [Google Scholar] [CrossRef] [PubMed]
- Selvig, K.A.; Sorensen, R.G.; Wozney, J.M.; Wikesjö, U.M. Bone repair following recombinant human bone morphogenetic protein-2 stimulated periodontal regeneration. J. Periodontol. 2002, 73, 1020–1029. [Google Scholar] [CrossRef] [PubMed]
- Hammarström, L. Enamel matrix, cementum development and regeneration. J. Clin. Periodontol. 1997, 24, 658–668. [Google Scholar] [CrossRef]
- Bosshardt, D.D. Biological mediators and periodontal regeneration: A review of enamel matrix proteins at the cellular and molecular levels. J. Clin. Periodontol. 2008, 35, 87–105. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Wei, L.; Bosshardt, D.D.; Buser, D.; Sculean, A.; Zhang, Y. Effects of enamel matrix proteins in combination with a bovine-derived natural bone mineral for the repair of bone defects. Clin. Oral. Investig. 2014, 18, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Shibui, T.; Yajima, T.; Irie, K.; Ochi, M.; Sakakura, Y. Architecture of connective tissue regenerated by enamel matrix derivative around hydroxyapatite implanted into tooth extraction sockets in the rat maxilla. Anat. Sci. Int. 2020, 95, 334–341. [Google Scholar] [CrossRef]
- Walter, C.; Jawor, P.; Bernimoulin, J.P.; Hägewald, S. Moderate effect of enamel matrix derivative (Emdogain Gel) on Porphyromonas gingivalis growth in vitro. Arch. Oral. Biol. 2006, 51, 171–176. [Google Scholar] [CrossRef]
- Tsai, S.J.; Ding, Y.W.; Shih, M.C.; Tu, Y.K. Systematic review and sequential network meta-analysis on the efficacy of periodontal regenerative therapies. J. Clin. Periodontol. 2020, 47, 1108–1120. [Google Scholar] [CrossRef]
- Wu, Y.C.; Lin, L.K.; Song, C.J.; Su, Y.X.; Tu, Y.K. Comparisons of periodontal regenerative therapies: A meta-analysis on the long-term efficacy. J. Clin. Periodontol. 2017, 44, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Susin, C.; Fiorini, T.; Lee, J.; De Stefano, J.A.; Dickinson, D.P.; Wikesjö, U.M. Wound healing following surgical and regenerative periodontal therapy. Periodontology 2015, 68, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Nagata, M.J.; de Campos, N.; Messora, M.R.; Pola, N.M.; Santinoni, C.S.; Bomfim, S.R.; Fucini, S.E.; Ervolino, E.; de Almeida, J.M.; Theodoro, L.H.; et al. Platelet-rich plasma, low-level laser therapy, or their combination promotes periodontal regeneration in fenestration defects: A preliminary in vivo study. J. Periodontol. 2014, 85, 770–778. [Google Scholar] [CrossRef]
- Corrêa, M.G.; Gomes Campos, M.L.; Marques, M.R.; Bovi Ambrosano, G.M.; Casati, M.Z.; Nociti, F.H., Jr.; Sallum, E.A. Outcome of enamel matrix derivative treatment in the presence of chronic stress: Histometric study in rats. J. Periodontol. 2014, 85, 259–267. [Google Scholar] [CrossRef]
- Miron, R.J.; Wei, L.; Yang, S.; Caluseru, O.M.; Sculean, A.; Zhang, Y. Effect of enamel matrix derivative on periodontal wound healing and regeneration in an osteoporotic model. J. Periodontol. 2014, 85, 1603–1611. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.K.; Shen, C.; Chiang, C.Y.; Hsieh, Y.D.; Fu, E. Effects of bone morphogenetic protein-6 on periodontal wound healing in a fenestration defect of rats. J. Periodontal Res. 2005, 40, 1–10. [Google Scholar] [CrossRef]
- Fischer, A.H.; Jacobson, K.A.; Rose, J.; Zeller, R. Hematoxylin and eosin staining of tissue and cell sections. CSH Protoc. 2008, 4986, pdb-prot4986. [Google Scholar] [CrossRef]
- Schneider, C.A.; Rasband, W.S.; Eliceiri, K.W. NIH Image to ImageJ: 25 years of image analysis. Nat. Methods 2012, 9, 671–675. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji: An open-source platform for biological-image analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damanaki, A.; Beisel-Memmert, S.; Nokhbehsaim, M.; Abedi, A.; Rath-Deschner, B.; Nogueira, A.V.B.; Deschner, J. Influence of Occlusal Hypofunction on Alveolar Bone Healing in Rats. Int. J. Mol. Sci. 2023, 24, 9744. https://doi.org/10.3390/ijms24119744
Damanaki A, Beisel-Memmert S, Nokhbehsaim M, Abedi A, Rath-Deschner B, Nogueira AVB, Deschner J. Influence of Occlusal Hypofunction on Alveolar Bone Healing in Rats. International Journal of Molecular Sciences. 2023; 24(11):9744. https://doi.org/10.3390/ijms24119744
Chicago/Turabian StyleDamanaki, Anna, Svenja Beisel-Memmert, Marjan Nokhbehsaim, Ali Abedi, Birgit Rath-Deschner, Andressa V. B. Nogueira, and James Deschner. 2023. "Influence of Occlusal Hypofunction on Alveolar Bone Healing in Rats" International Journal of Molecular Sciences 24, no. 11: 9744. https://doi.org/10.3390/ijms24119744