
Onset of Adverse Abdominal Events Due to Intestinal Ischemia-Reperfusion Injury after Aortic Cross-Clamping Is Associated with Elevated HSP70 Serum Levels in the Early Postoperative Phase
 , and
, and
Abstract
:1. Introduction
2. Results
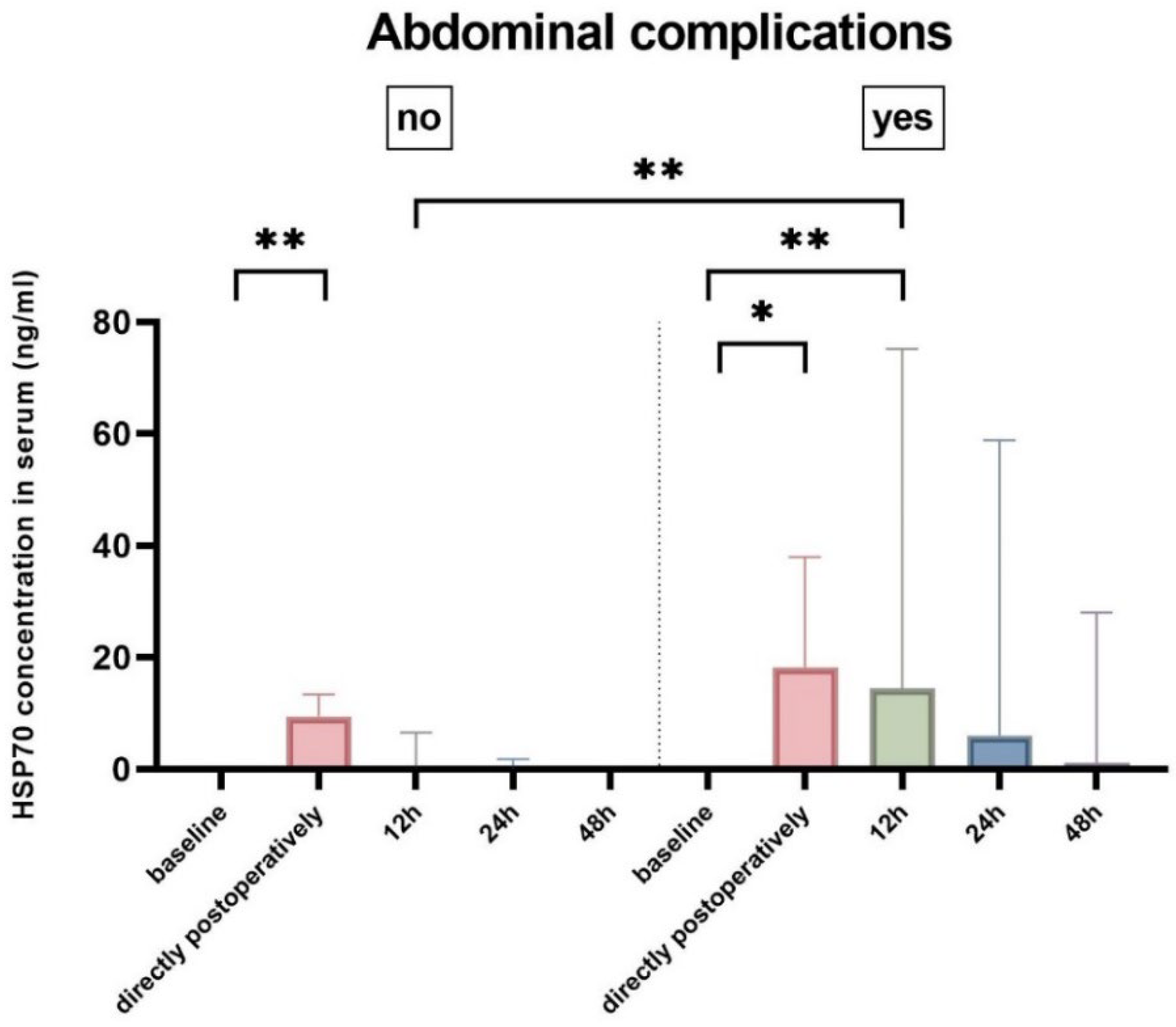
2.1. Persisting Elevation of HSP70 Serum Levels in Patients with Abdominal Complications
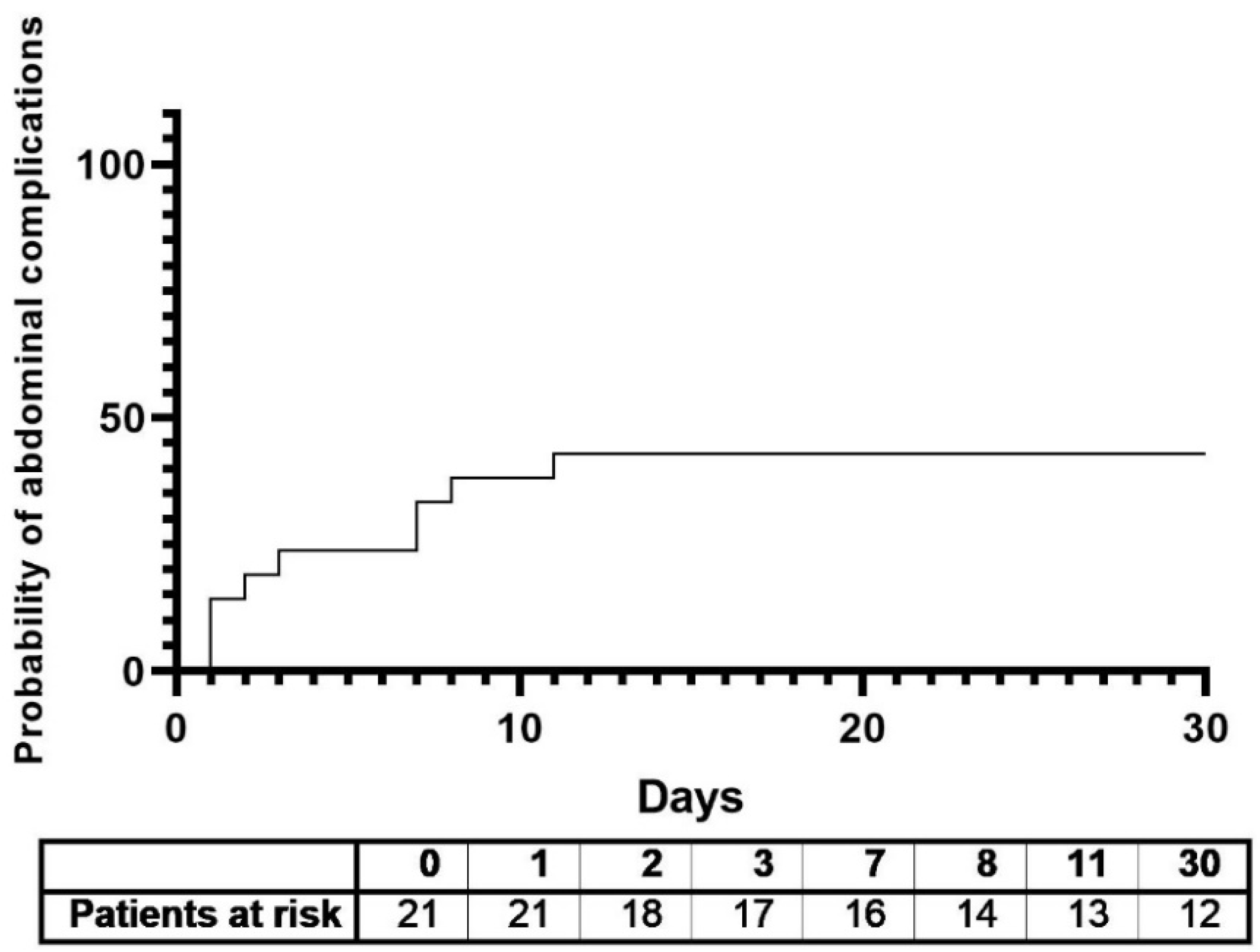
2.2. HSP70 Levels as a Biomarker for Abdominal Complications
3. Discussion
Strengths and Limitations
4. Materials and Methods
4.1. Study Design
4.2. Surgery
4.3. HSP70 Measurements
4.4. Endpoints
4.5. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, M.-Y.; Yiang, G.-T.; Liao, W.-T.; Tsai, A.P.Y.; Cheng, Y.-L.; Cheng, P.-W.; Li, C.-Y.; Li, C.J. Current Mechanistic Concepts in Ischemia and Reperfusion Injury. Cell. Physiol. Biochem. 2018, 46, 1650–1667. [Google Scholar] [CrossRef] [PubMed]
- Mester, A.; Magyar, Z.; Sogor, V.; Tanczos, B.; Stark, Y.; Cherniavsky, K.; Bidiga, L.; Peto, K.; Nemeth, N. Intestinal ischemia-reperfusion leads to early systemic micro-rheological and multiorgan microcirculatory alterations in the rat. Clin. Hemorheol. Microcirc. 2018, 68, 35–44. [Google Scholar] [CrossRef] [PubMed]
- Zarkowsky, D.S.; Inman, J.T.; Sorrentino, T.A.; Hiramoto, J.S.; Vartanian, S.M.; Eichler, C.M.; Reilly, L.M.; Gasper, W.J.; Conte, M.S. Contemporary Experience with Paravisceral Aortic Aneurysm (PVAAA) Repair in a Tertiary Center. Ann. Vasc. Surg. 2021, 75, 368–379. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Ceyhan, G.O.; Friess, H. Beyond lactate: Is there a role for serum lactate measurement in diagnosing acute mesenteric ischemia? Dig. Surg. 2012, 29, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Fernández, M.R.; Valpuesta, J.M. Hsp70 chaperone: A master player in protein homeostasis [version 1; peer review: 3 approved]. F1000Research 2018, 7, 1497. [Google Scholar] [CrossRef] [Green Version]
- Latchman, D.S. Heat shock proteins and cardiac protection. Cardiovasc. Res. 2001, 51, 637–646. [Google Scholar] [CrossRef] [Green Version]
- Mine, Y.; Fujita, F.; Murase, T.; Ito, S.; Takatsuki, M.; Ikematsu, K.; Eguchi, S. Heat Shock Protein 70 Messenger RNA in Rat Leukocytes Elevates After Severe Intestinal Ischemia–Reperfusion. J. Surg. Res. 2019, 242, 342–348. [Google Scholar] [CrossRef] [Green Version]
- Fleming, S.D.; Starnes, B.W.; Kiang, J.G.; Stojadinovic, A.; Tsokos, G.C.; Shea-Donohue, T. Heat stress protection against mesenteric I/R-induced alterations in intestinal mucosa in rats. J. Appl. Physiol. 2002, 92, 2600–2607. [Google Scholar] [CrossRef] [Green Version]
- Ornellas, F.M.; Ornellas, D.S.; Martini, S.V.; Castiglione, R.C.; Ventura, G.M.; Rocco, P.R.; Gutfilen, B.; de Souza, S.A.; Takiya, C.M.; Morales, M.M. Bone Marrow-Derived Mononuclear Cell Therapy Accelerates Renal Ischemia-Reperfusion Injury Recovery by Modulating Inflammatory, Antioxidant and Apoptotic Related Molecules. Cell. Physiol. Biochem. 2017, 41, 1736–1752. [Google Scholar] [CrossRef] [Green Version]
- Gottlieb, R.A. Cell death pathways in acute ischemia/reperfusion injury. J. Cardiovasc. Pharmacol. Ther. 2011, 16, 233–238. [Google Scholar] [CrossRef]
- Eefting, F.; Rensing, B.; Wigman, J.; Pannekoek, W.J.; Liu, W.M.; Cramer, M.J.; Lips, D.J.; Doevendans, P.A. Role of apoptosis in reperfusion injury. Cardiovasc. Res. 2004, 61, 414–426. [Google Scholar] [CrossRef]
- Kalder, J.; Keschenau, P.; Hanssen, S.J.; Greiner, A.; Windsant, I.C.V.; Kennes, L.N.; Tolba, R.; Prinzen, F.W.; Buurman, W.A.; Jacobs, M.J.; et al. The impact of selective visceral perfusion on intestinal macrohemodynamics and microhemodynamics in a porcine model of thoracic aortic cross-clamping. J. Vasc. Surg. 2012, 56, 149–158. [Google Scholar]
- Valentine, R.; Hagino, R.T.; Jackson, M.R.; Kakish, H.B.; Bengtson, T.D.; Clagett, G. Gastrointestinal complications after aortic surgery. J. Vasc. Surg. 1998, 28, 404–412. [Google Scholar] [CrossRef] [Green Version]
- Clair, D.G.; Beach, J.M. Mesenteric Ischemia. N. Engl. J. Med. 2016, 374, 959–968. [Google Scholar] [CrossRef] [Green Version]
- Schraag, S. Postoperative management. Best Pract. Res. Clin. Anaesthesiol. 2016, 30, 381–393. [Google Scholar]
- Gombert, A.; Frankort, J.; Keszei, A.; Müller, O.; Benning, J.; Kotelis, D.; Jacobs, M.J. Outcome of Elective and Emergency Open Thoraco-Abdominal Aortic Aneurysm Repair in 255 Cases: A Retrospective Single Centre Study. Eur. J. Vasc. Endovasc. Surg. 2022, 63, 578–586. [Google Scholar] [CrossRef]
- Monnot, A.; Dumesnil, A.; Renet, S.; Roquet, M.L.; Richard, V.; Plissonnier, D. A 30-Minute Supraceliac Aortic Clamping in the Rat Causes Death Due to an Inflammatory Response and Pulmonary Lesions. Ann. Vasc. Surg. 2018, 52, 192–200. [Google Scholar]
- Oldenburg, H.; Welborn, M.B.; Pruitt, J.; Boelens, P.; Seeger, J.; Martin, T.; Wesdorp, R.; Rauwerda, J.; van Leeuwen, P.; Moldawer, L. Interleukin-10 Appearance Following Thoraco-abdominal and Abdominal Aortic Aneurysm Repair is Associated with the Duration of Visceral Ischaemia. Eur. J. Vasc. Endovasc. Surg. 2000, 20, 169–172. [Google Scholar] [CrossRef] [Green Version]
- Windsant, I.C.V.; Hellenthal, F.A.; Derikx, J.P.; Prins, M.H.; Buurman, W.A.; Jacobs, M.J.; Schurink, G.W.H. Circulating intestinal fatty acid-binding protein as an early marker of intestinal necrosis after aortic surgery: A prospective observational cohort study. Ann. Surg. 2012, 255, 796–803. [Google Scholar] [CrossRef]
- Björck, M.; Koelemay, M.; Acosta, S.; Goncalves, F.B.; Kölbel, T.; Kolkman, J.J.; Lees, T.; Lefevre, J.H.; Menyhei, G.; Oderich, G.; et al. Editor’s Choice—Management of the Diseases of Mesenteric Arteries and Veins: Clinical Practice Guidelines of the European Society of Vascular Surgery (ESVS). Eur. J. Vasc. Endovasc. Surg. 2017, 53, 460–510. [Google Scholar] [CrossRef] [Green Version]
- Haider, T.; Simader, E.; Glück, O.; Ankersmit, H.J.; Heinz, T.; Hajdu, S.; Negrin, L.L. Systemic release of heat-shock protein 27 and 70 following severe trauma. Sci. Rep. 2019, 9, 9595. [Google Scholar] [PubMed] [Green Version]
- Mommertz, G.; Sigala, F.; Langer, S.; Koeppel, T.; Mess, W.; Schurink, G.; Jacobs, M. Thoracoabdominal aortic aneurysm repair in patients with marfan syndrome. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 181–186. [Google Scholar] [PubMed] [Green Version]
- Jacobs, M.J.; Elenbaas, T.W.; Schurink, G.W.; Mess, W.H.; Mochtar, B. Assessment of spinal cord integrity during thoracoabdominal aortic aneurysm repair. Ann. Thorac. Surg. 2002, 74, S1864–S1866, Discussion S1892–S1898. [Google Scholar] [CrossRef] [PubMed]
- Vather, R.; Trivedi, S.; Bissett, I. Defining postoperative ileus: Results of a systematic review and global survey. J. Gastrointest. Surg. 2013, 17, 962–972. [Google Scholar] [CrossRef] [PubMed]
- Montalvo-Jave, E.E.; Espejel-Deloiza, M.; Chernitzky-Camaño, J.; Peña-Pérez, C.A.; Rivero-Sigarroa, E.; Ortega-León, L.H. Abdominal compartment syndrome: Current concepts and management. Rev. Gastroenterol. Mex. (Engl. Ed.) 2020, 85, 443–451. [Google Scholar]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- European Association for The Study of The Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Thomas, M.E.; Blaine, C.; Dawnay, A.; Devonald, M.A.; Ftouh, S.; Laing, C.; Latchem, S.; Lewington, A.; Milford, D.V.; Ostermann, M. The definition of acute kidney injury and its use in practice. Kidney Int. 2015, 87, 62–73. [Google Scholar] [CrossRef]
- Meyer, N.J.; Gattinoni, L.; Calfee, C.S. Acute respiratory distress syndrome. Lancet 2021, 398, 622–637. [Google Scholar] [CrossRef]
- Rossaint, J.; Zarbock, A. Pathogenesis of Multiple Organ Failure in Sepsis. Crit. Rev. Immunol. 2015, 35, 277–291. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All (n = 21) | No Abdominal Complications (n = 12) | Abdominal Complications (n = 9) | Correlations | |
|---|---|---|---|---|
| Age (years) | 50.6 ± 12.4 | 51.7 ± 11.3 | 49.1 ± 14.3 | −0.1 (p = 0.65) † |
| Women | 6 (28.6) | 3 (25) | 3 (33.3) | 0.67 [0.1–4.48] |
| Smoking | 7 (33.3) | 4 (33.3) | 3 (33.3) | 1 [0.16–6.25] |
| Obesity | 3 (14.3) | 1 (8.3) | 2 (22.2) | 3.14 [0.24–41.5] |
| BMI (m/kg2) | 24.2 ± 4.2 | 24.1 ± 3.7 | 24.4 ± 5 | 0.45 (p = 0.85) † |
| COPD | 4 (19) | 2 (16.7) | 2 (22.2) | 1.43 [0.16–12.7] |
| Hypertension | 18 (81) | 8 (66.7) | 9 (100) | 0.67 [0.45–0.1] |
| CKD | 12 (57.1) | 7 (58.3) | 5 (55.6) | 0.89 [0.16–5.11] |
| Prior aortic procedures | 13 (61.9) | 8 (66.7) | 5 (55.6) | 0.63 [0.1–3.7] |
| Crawford type | ||||
| Type I | 2 (9.5) | 1 (8.3) | 1 (11.1) | 1.375 [0.74–25.43] |
| Type II | 7 (33.3) | 3 (25) | 4 (44.4) | 2.4 [0.38–15.32] |
| Type III | 7 (33.3) | 5 (41.7) | 2 (22.2) | 0.4 [0.57–2.8] |
| Type IV | 5 (23.8) | 3 (25) | 2 (22.2) | 0.86 [0.11–6.62] |
| Max. aortic diameter (cm) | 5.8 ± 1.5 | 6.3 ± 1.3 | 5.1 ± 1.5 | −0.4 (p = 0.67) † |
| Duration of surgery (min) | 520 ± 89.6 | 490.5 ± 89.7 | 550 ± 85.1 | 0.3 (p = 0.19) † |
| Cross-clamping time (min) | 150.6 ± 36.4 | 147.8 ± 41.8 | 155.1 ± 29.5 | 0.1 (p = 0.66) |
| All (n = 21) | No Abdominal Complications (n = 12) | Abdominal Complications (n = 9) | Pearson’s r | p-Value | |
|---|---|---|---|---|---|
| Thirty-day mortality | 4 (19) | 1 (8.3) | 3 (33.3) | 0.32 | 0.164 |
| Hospital stay (days) | 44.5 ± 32.7 | 30.9 ± 15.6 | 62.7 ± 41.1 | 0.49 | 0.02 * |
| Intensive Care Unit stay (days) | 26.1 ± 25.4 | 17.5 ± 16 | 37.7 ± 31.6 | 0.4 | 0.07 |
| Reintervention | 11 (52.4) | 4 (33.3) | 7 (77.8) | 0.44 | 0.046 * |
| 6 (28.6) | 3 (25) | 3 (33.3) | 0.16 | 0.502 |
| 4 (19) | 0 | 4 (44.4) | 0.62 | 0.003 ** |
| 2 (9.5) | 0 | 2 (22.2) | −0.11 | 0.622 |
| 3 (14.3) | 2 (16.6) | 1 (11.1) | −0.04 | 0.863 |
| Time to abdominal complications (days) | 4.8 ± 1.3 | ||||
| Abdominal complications (total) | 9 (42.9) | 0 (0) | 9 (100) | ||
| 2 (9.5) | 0 (0) | 2 (22.2) | ||
| 2 (9.5) | 0 (0) | 2 (22.2) | ||
| 5 (23.8) | 0 (0) | 5 (55.6) | ||
| Postop days to abd. complication (days) | 1.9 ± 3.3 | 0 (0) | 4.4 ± 3.9 | ||
| Sepsis | 7 (33.3) | 2 (16.7) | 5 (55.6) | 0.41 | 0.066 |
| Multi-organ dysfunction syndrome | 4 (19) | 1 (8.3) | 3 (33.3) | 0.32 | 0.164 |
| Acute kidney injury | 13 (61.9) | 6 (50) | 7 (77.8) | 0.28 | 0.214 |
| Liver failure | 4 (19) | 1 (8.3) | 3 (33.3) | 0.32 | 0.164 |
| Acute respiratory distress syndrome | 9 (42.9) | 4 (33.3) | 5 (55.6) | 0.22 | 0.333 |
| Need for catecholamines (days) | 11 ± 10.8 | 6 ± 6.4 | 17.9 ± 12 | 0.56 | 0.013 * |
| All (n = 21) | Adjusted p-Value † | No Abdominal Complications (n = 12) | Adjusted p-Value † | Abdominal Complications (n = 9) | Adjusted p-Value † | p-Value †† | |
|---|---|---|---|---|---|---|---|
| Baseline | 0 [0–0] | 0 [0–0] | 0 [0–0] | 0.92 | |||
| Directly postoperative | 11.77 [6.1–20.8] | <0.001 *** | 9.5 [3.9–13.3] | 0.002 ** | 18.3 [9.5–38] | 0.014 * | 0.1 |
| 12 h | 7.59 [0–14] | 0.002 ** | 0 [0–6.5] | 0.796 | 14.5 [8.8–75.3] | 0.003 ** | 0.007 ** |
| 24 h | 1.33 [0–5.4] | 0.357 | 0 [0–1.8] | 1 | 6 [0.3–58.9] | 0.526 | 0.15 |
| 48 h | 0 [0–1.2] | 1 | 0 [0–0] | 1 | 1.2 [0–28] | 1 | 0.06 |
| Visceral Malperfusion (n = 5) | p-Value | Abdominal Compartment Syndrome (n = 2) | p-Value | Paralytic Ileus (n = 2) | p-Value | |
|---|---|---|---|---|---|---|
| baseline | 0.22 | 0.35 | −0.11 | 0.65 | −0.11 | 0.65 |
| directly postoperatively | 0.3 | 0.19 | 0.35 | 0.12 | −0.13 | 0.56 |
| 12 h | 0.43 | 0.05 * | 0.41 | 0.07 | −0.19 | 0.41 |
| 24 h | 0.3 | 0.22 | 0.08 | 0.75 | −0.36 | 0.12 |
| 48 h | 0.34 | 0.14 | 0.14 | 0.57 | −0.41 | 0.08 |
| AUC | p-Value | Cut-Off | Sensitivity (%) | Specificity (%) | ||
|---|---|---|---|---|---|---|
| HSP70 (ng/mL) | baseline | 0.556 | 0.68 | 1.2 | 11.1 | 100 |
| directly postoperatively | 0.788 | 0.03 * | 14.4 | 66.7 | 83.3 | |
| 12 h | 0.909 | 0.002 ** | 7.6 | 88.9 | 83.3 | |
| 24 h | 0.788 | 0.03 * | 3.3 | 66.7 | 100 | |
| 48 h | 0.808 | 0.02 * | 0.4 | 66.7 | 90.9 | |
| Lactate (mmol/L) | baseline | 0.540 | 0.765 | 0.45 | 88.9 | 33.3 |
| directly postoperatively | 0.667 | 0.188 | 2.65 | 66.7 | 66.7 | |
| 12 h | 0.621 | 0.347 | 2.05 | 77.8 | 50 | |
| 24 h | 0.687 | 0.141 | 1.55 | 77.8 | 78.7 | |
| 48 h | 0.616 | 0.370 | 1.7 | 33.3 | 90.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Doukas, P.; Hellfritsch, G.; Krabbe, H.; Frankort, J.; Jacobs, M.J.; Gombert, A.; Simon, F. Onset of Adverse Abdominal Events Due to Intestinal Ischemia-Reperfusion Injury after Aortic Cross-Clamping Is Associated with Elevated HSP70 Serum Levels in the Early Postoperative Phase. Int. J. Mol. Sci. 2022, 23, 15063. https://doi.org/10.3390/ijms232315063
Doukas P, Hellfritsch G, Krabbe H, Frankort J, Jacobs MJ, Gombert A, Simon F. Onset of Adverse Abdominal Events Due to Intestinal Ischemia-Reperfusion Injury after Aortic Cross-Clamping Is Associated with Elevated HSP70 Serum Levels in the Early Postoperative Phase. International Journal of Molecular Sciences. 2022; 23(23):15063. https://doi.org/10.3390/ijms232315063
Chicago/Turabian StyleDoukas, Panagiotis, Gabriel Hellfritsch, Hanif Krabbe, Jelle Frankort, Michael J. Jacobs, Alexander Gombert, and Florian Simon. 2022. "Onset of Adverse Abdominal Events Due to Intestinal Ischemia-Reperfusion Injury after Aortic Cross-Clamping Is Associated with Elevated HSP70 Serum Levels in the Early Postoperative Phase" International Journal of Molecular Sciences 23, no. 23: 15063. https://doi.org/10.3390/ijms232315063