
A Comprehensive Assessment of Qualitative and Quantitative Prodromal Parkinsonian Features in Carriers of Gaucher Disease—Identifying Those at the Greatest Risk

Abstract
:1. Introduction
2. Results
2.1. Study Cohort
2.2. Abnormal Prodromal Tests
2.3. Variables Associated with Abnormal Prodromal Tests
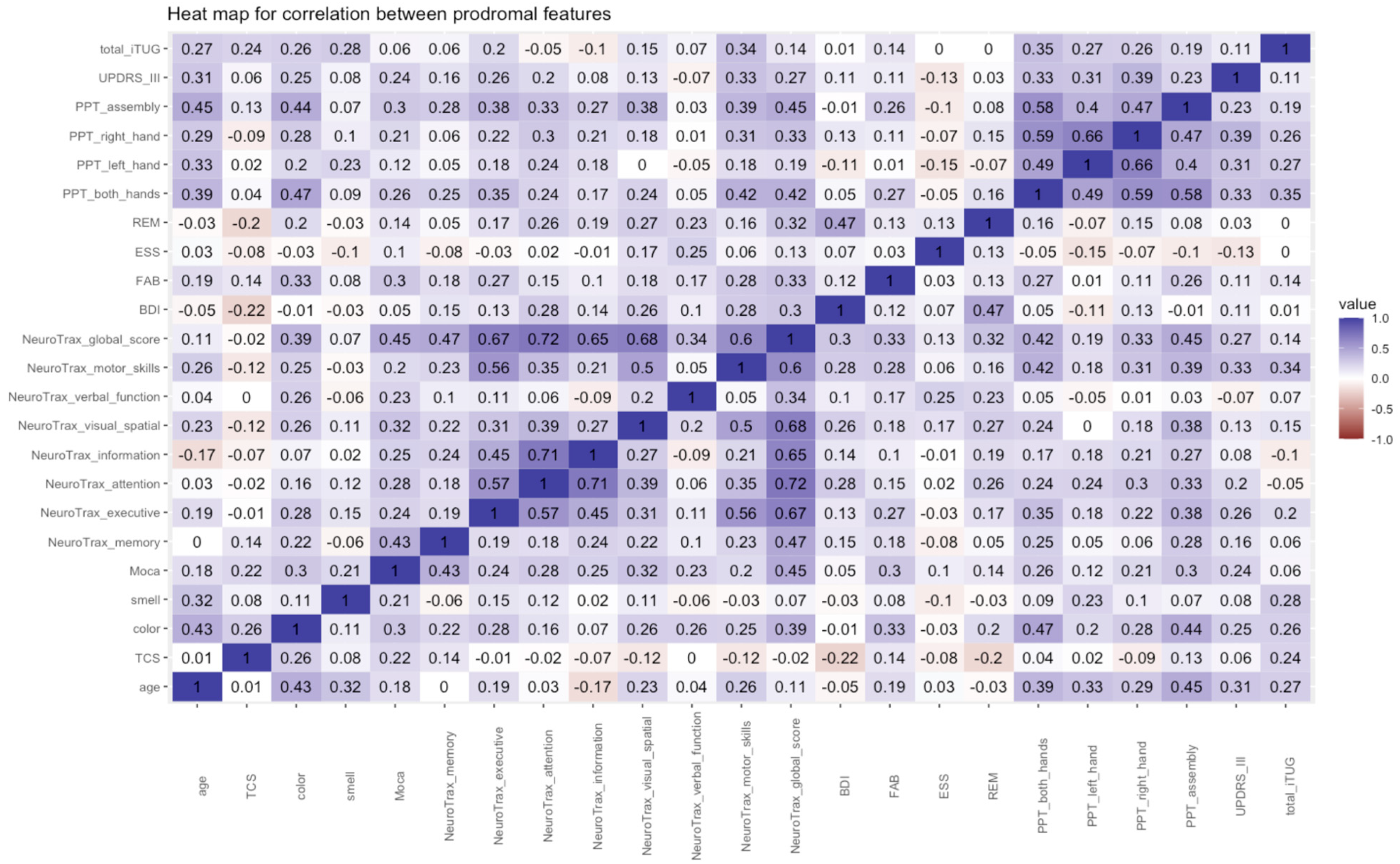
2.4. Correlations
2.5. Most “Abnormal” Prodromal Tests
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.2. Prodromal Tests
4.3. Imaging
4.4. Sensory and Autonomic Assessments
4.5. Cognitive and Mental
4.6. Sleep Disorder
4.7. Motor
4.8. Genetic Analysis and Biobank
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Neudorfer, O.; Giladi, N.; Elstein, D.; Abrahamov, A.; Turezkite, T.; Aghai, E.; Reches, A.; Bembi, B.; Zimran, A. Occurrence of Parkinson’s syndrome in type I Gaucher disease. QJM 1996, 89, 691–694. [Google Scholar] [CrossRef] [PubMed]
- Gan-Or, Z.; Giladi, N.; Rozovski, U.; Shifrin, C.; Rosner, S.; Gurevich, T.; Bar-Shira, A.; Orr-Urtreger, A. Genotype-phenotype correlations between GBA mutations and Parkinson disease risk and onset. Neurology 2008, 70, 2277–2283. [Google Scholar] [CrossRef] [PubMed]
- Sidransky, E.; Nalls, M.A.; Aasly, J.O.; Aharon-Peretz, J.; Annesi, G.; Barbosa, E.R.; Bar-Shira, A.; Berg, D.; Bras, J.; Brice, A.; et al. Multicenter analysis of glucocerebrosidase mutations in Parkinson’s disease. N. Engl. J. Med. 2009, 361, 1651–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alcalay, R.N.; Levy, O.A.; Waters, C.C.; Fahn, S.; Ford, B.; Kuo, S.H.; Mazzoni, P.; Pauciulo, M.W.; Nichols, W.C.; Gan-Or, Z.; et al. Glucocerebrosidase activity in Parkinson’s disease with and without GBA mutations. Brain 2015, 138 Pt 9, 2648–2658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gan-Or, Z.; Amshalom, I.; Kilarski, L.L.; Bar-Shira, A.; Gana-Weisz, M.; Mirelman, A.; Marder, K.; Bressman, S.; Giladi, N.; Orr-Urtreger, A. Differential effects of severe vs mild GBA mutations on Parkinson disease. Neurology 2015, 84, 880–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez, G.; Kim, J.; Wiggs, E.; Cintron, D.; Groden, C.; Tayebi, N.; Mistry, P.K.; Pastores, G.M.; Zimran, A.; Goker-Alpan, O.; et al. Clinical course and prognosis in patients with Gaucher disease and parkinsonism. Neurol. Genet. 2016, 2, e57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahlknecht, P.; Seppi, K.; Poewe, W. The Concept of Prodromal Parkinson’s Disease. J. Parkinsons Dis. 2015, 5, 681–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, D.; Postuma, R.B.; Adler, C.H.; Bloem, B.R.; Chan, P.; Dubois, B.; Gasser, T.; Goetz, C.G.; Halliday, G.; Joseph, L.; et al. MDS research criteria for prodromal Parkinson’s disease. Mov. Disord. 2015, 30, 1600–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinzel, S.; Berg, D.; Gasser, T.; Chen, H.; Yao, C.; Postuma, R.B.; MDS Task Force on the Definition of Parkinson’s Disease. Update of the MDS research criteria for prodromal Parkinson’s disease. Mov. Disord. 2019, 34, 1464–1470. [Google Scholar] [CrossRef] [PubMed]
- Cacabelos, R. Parkinson’s Disease: From Pathogenesis to Pharmacogenomics. Int. J. Mol. Sci. 2017, 18, 551. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Rodriguez, P.; Zampese, E.; Stout, K.A.; Guzman, J.N.; Ilijic, E.; Yang, B.; Tkatch, T.; Stavarache, M.A.; Wokosin, D.L.; Gao, L.; et al. Disruption of mitochondrial complex I induces progressive parkinsonism. Nature 2021, 599, 650–656. [Google Scholar] [CrossRef]
- Miller, D.B.; O’Callaghan, J.P. Biomarkers of Parkinson’s disease: Present and future. Metabolism 2015, 64 (Suppl. 1), S40–S46. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.J.; Okun, M.S. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Revel-Vilk, S.; Szer, J.; Zimran, A. Gaucher disease and related lysosomal storage diseases. In Williams Hematology, 10th ed.; Kaushansky, K., Lichtman, M., Prchal, J., Levi, M., Press, O., Burns, L., Caligiuri, M., Eds.; McGraw-Hill: New York, NY, USA, 2021; pp. 1189–1202. [Google Scholar]
- Beavan, M.; McNeill, A.; Proukakis, C.; Hughes, D.A.; Mehta, A.; Schapira, A.H. Evolution of prodromal clinical markers of Parkinson disease in a GBA mutation-positive cohort. JAMA Neurol. 2015, 72, 201–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simuni, T.; Uribe, L.; Cho, H.R.; Caspell-Garcia, C.; Coffey, C.S.; Siderowf, A.; Trojanowski, J.Q.; Shaw, L.M.; Seibyl, J.; Singleton, A.; et al. Clinical and dopamine transporter imaging characteristics of non-manifest LRRK2 and GBA mutation carriers in the Parkinson’s Progression Markers Initiative (PPMI): A cross-sectional study. Lancet Neurol. 2020, 19, 71–80. [Google Scholar] [CrossRef]
- Krohn, L.; Ruskey, J.A.; Rudakou, U.; Leveille, E.; Asayesh, F.; Hu, M.T.M.; Arnulf, I.; Dauvilliers, Y.; Hogl, B.; Stefani, A.; et al. GBA variants in REM sleep behavior disorder: A multicenter study. Neurology 2020, 95, e1008–e1016. [Google Scholar] [CrossRef] [PubMed]
- Arkadir, D.; Dinur, T.; Becker Cohen, M.; Revel-Vilk, S.; Tiomkin, M.; Bruggemann, N.; Cozma, C.; Rolfs, A.; Zimran, A. Prodromal substantia nigra sonography undermines suggested association between substrate accumulation and the risk for GBA-related Parkinson’s disease. Eur. J. Neurol. 2019, 26, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Omrani, F.; Ansari-Damavandi, S.; Zamani, B.; Omrani, Z.; Mohammadzade, N.; Rohani, S.; Rohani, M. Transcranial sonography in carriers of Gaucher disease. Iran J. Neurol. 2018, 17, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Perrin, A.J.; Nosova, E.; Co, K.; Book, A.; Iu, O.; Silva, V.; Thompson, C.; McKeown, M.J.; Stoessl, A.J.; Farrer, M.J.; et al. Gender differences in Parkinson’s disease depression. Park. Relat. Disord. 2017, 36, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Parker, G.; Brotchie, H. Gender differences in depression. Int. Rev. Psychiatry 2010, 22, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Zhou, H.Y.; Sun, Q.; Tan, Y.Y.; Hu, Y.Y.; Zhan, W.W.; Li, D.H.; Wang, Y.; Xiao, Q.; Liu, J.; Chen, S.D. Substantia nigra echogenicity correlated with clinical features of Parkinson’s disease. Park. Relat. Disord. 2016, 24, 28–33. [Google Scholar] [CrossRef]
- Li, K.; Ge, Y.L.; Gu, C.C.; Zhang, J.R.; Jin, H.; Li, J.; Cheng, X.Y.; Yang, Y.P.; Wang, F.; Zhang, Y.C.; et al. Substantia nigra echogenicity is associated with serum ferritin, gender and iron-related genes in Parkinson’s disease. Sci. Rep. 2020, 10, 8660. [Google Scholar] [CrossRef] [PubMed]
- Xu, R.; Chen, G.; Mao, Z.; Gao, H.; Deng, Y.; Tao, A. Diagnostic Performance of Transcranial Sonography for Evaluating Substantia Nigra Hyper-echogenicity in Patients with Parkinson’s Disease. Ultrasound Med. Biol. 2020, 46, 1208–1215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toomsoo, T.; Liepelt-Scarfone, I.; Berg, D.; Kerner, R.; Pool, A.H.; Kadastik-Eerme, L.; Rubanovits, I.; Asser, T.; Taba, P. Effect of Age on Substantia Nigra Hyper-echogenicity in Parkinson’s Disease Patients and Healthy Controls. Ultrasound Med. Biol. 2019, 45, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Arkadir, D.; Dinur, T.; Mullin, S.; Mehta, A.; Baris, H.N.; Alcalay, R.N.; Zimran, A. Trio approach reveals higher risk of PD in carriers of severe vs. mild GBA mutations. Blood Cells Mol. Dis. 2018, 68, 115–116. [Google Scholar] [CrossRef] [PubMed]
- Koros, C.; Simitsi, A.; Stefanis, L. Genetics of Parkinson’s Disease: Genotype-Phenotype Correlations. Int. Rev. Neurobiol. 2017, 132, 197–231. [Google Scholar]
- Scholz, S.W.; Jeon, B.S. GBA mutations and Parkinson disease: When genotype meets phenotype. Neurology 2015, 84, 866–867. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.P.; Lopez, G.; Gregory, M.D.; Berman, K.F.; Sidransky, E. Comparison of Transcranial Sonography and [(18) F]-Fluorodopa PET Imaging in GBA1 Mutation Carriers. Mov. Disord. 2022, 37, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Khoury, T.; Ishay, Y.; Rotnemer-Golinkin, D.; Zolotarovya, L.; Arkadir, D.; Zimran, A.; Ilan, Y. A synergistic effect of Ambroxol and Beta-Glucosylceramide in alleviating immune-mediated hepatitis: A novel immunomodulatory non-immunosuppressive formulation for treatment of immune-mediated disorders. Biomed. Pharmacother. 2020, 132, 110890. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.; Gaenslen, A.; Prahl, K.; Srulijes, K.; Hauser, A.K.; Schulte, C.; Csoti, I.; Berg, D.; Brockmann, K. Patient’s perception: Shorter and more severe prodromal phase in GBA-associated PD. Eur. J. Neurol. 2019, 26, 694–698. [Google Scholar] [CrossRef] [PubMed]
- Halperin, A.; Elstein, D.; Zimran, A. Increased incidence of Parkinson disease among relatives of patients with Gaucher disease. Blood Cells Mol. Dis. 2006, 36, 426–428. [Google Scholar] [CrossRef]
- Bor-Seng-Shu, E.; Paschoal, F.M.; Almeida, K.J.; De Lima Oliveira, M.; Nogueira, R.C.; Teixeira, M.J.; Walter, U. Transcranial brain sonography for Parkinsonian syndromes. J. Neurosurg. Sci. 2019, 63, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Walter, U.; Skoloudik, D. Transcranial sonography (TCS) of brain parenchyma in movement disorders: Quality standards, diagnostic applications and novel technologies. Ultraschall Med. 2014, 35, 322–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaenslen, A.; Unmuth, B.; Godau, J.; Liepelt, I.; Di Santo, A.; Schweitzer, K.J.; Gasser, T.; Machulla, H.J.; Reimold, M.; Marek, K.; et al. The specificity and sensitivity of transcranial ultrasound in the differential diagnosis of Parkinson’s disease: A prospective blinded study. Lancet Neurol. 2008, 7, 417–424. [Google Scholar] [CrossRef]
- Archibald, N.K.; Clarke, M.P.; Mosimann, U.P.; Burn, D.J. The retina in Parkinson’s disease. Brain 2009, 132 Pt 5, 1128–1145. [Google Scholar] [CrossRef] [Green Version]
- Brandies, R.; Yehuda, S. The possible role of retinal dopaminergic system in visual performance. Neurosci. Biobehav. Rev. 2008, 32, 611–656. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Gagnon, J.F.; Vendette, M.; Montplaisir, J.Y. Markers of neurodegeneration in idiopathic rapid eye movement sleep behaviour disorder and Parkinson’s disease. Brain 2009, 132 Pt 12, 3298–3307. [Google Scholar] [CrossRef] [Green Version]
- Kinnear, P.R.; Sahraie, A. New Farnsworth-Munsell 100 hue test norms of normal observers for each year of age 5–22 and for age decades 30–70. Br. J. Ophthalmol. 2002, 86, 1408–1411. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Q.; Chen, S.; Le, W. Hyposmia: A possible biomarker of Parkinson’s disease. Neurosci. Bull 2014, 30, 134–140. [Google Scholar] [CrossRef] [Green Version]
- Cao, M.; Li, Y.; Gu, Z.; Mi, T.; Xu, X.; Ma, C.; Chen, M.; Wu, M.; Chan, P. Validation of the utility of the Brief Smell Identification Test in Chinese patients with Parkinson’s disease. J. Clin. Neurosci. 2019, 60, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Cao, M.; Wang, N.; Zheng, P.; Gu, Z.; Chan, P. Validation of a new olfactory test for Chinese Parkinson’s disease patients. J. Clin. Neurosci. 2020, 76, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Mu, F.; Jiao, Q.; Du, X.; Jiang, H. Association of orthostatic hypotension with Parkinson’s disease: A meta-analysis. Neurol. Sci. 2020, 41, 1419–1426. [Google Scholar] [CrossRef] [PubMed]
- Mahlknecht, P.; Gasperi, A.; Djamshidian, A.; Kiechl, S.; Stockner, H.; Willeit, P.; Willeit, J.; Rungger, G.; Poewe, W.; Seppi, K. Performance of the Movement Disorders Society criteria for prodromal Parkinson’s disease: A population-based 10-year study. Mov. Disord. 2018, 33, 405–413. [Google Scholar] [CrossRef]
- Weintraub, D.; Simuni, T.; Caspell-Garcia, C.; Coffey, C.; Lasch, S.; Siderowf, A.; Aarsland, D.; Barone, P.; Burn, D.; Chahine, L.M.; et al. Cognitive performance and neuropsychiatric symptoms in early, untreated Parkinson’s disease. Mov. Disord. 2015, 30, 919–927. [Google Scholar] [CrossRef] [Green Version]
- Hanna-Pladdy, B.; Enslein, A.; Fray, M.; Gajewski, B.J.; Pahwa, R.; Lyons, K.E. Utility of the NeuroTrax computerized battery for cognitive screening in Parkinson’s disease: Comparison with the MMSE and the MoCA. Int. J. Neurosci. 2010, 120, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Visser, M.; Leentjens, A.F.; Marinus, J.; Stiggelbout, A.M.; van Hilten, J.J. Reliability and validity of the Beck depression inventory in patients with Parkinson’s disease. Mov. Disord. 2006, 21, 668–672. [Google Scholar] [CrossRef]
- Torbey, E.; Pachana, N.A.; Dissanayaka, N.N. Depression rating scales in Parkinson’s disease: A critical review updating recent literature. J. Affect Disord. 2015, 184, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Hurtado-Pomares, M.; Carmen Terol-Cantero, M.; Sanchez-Perez, A.; Peral-Gomez, P.; Valera-Gran, D.; Navarrete-Munoz, E.M. The frontal assessment battery in clinical practice: A systematic review. Int. J. Geriatr. Psychiatry 2018, 33, 237–251. [Google Scholar] [CrossRef]
- Stiasny-Kolster, K.; Mayer, G.; Schafer, S.; Moller, J.C.; Heinzel-Gutenbrunner, M.; Oertel, W.H. The REM sleep behavior disorder screening questionnaire--a new diagnostic instrument. Mov. Disord. 2007, 22, 2386–2393. [Google Scholar] [CrossRef]
- Sobreira-Neto, M.A.; Pena-Pereira, M.A.; Sobreira, E.S.T.; Chagas, M.H.N.; Fernandes, R.M.F.; Tumas, V.; Eckeli, A.L. High Frequency of Sleep Disorders in Parkinson’s Disease and Its Relationship with Quality of Life. Eur. Neurol. 2017, 78, 330–337. [Google Scholar] [CrossRef]
- Kim, R.; Yoo, D.; Im, J.H.; Kim, H.J.; Jeon, B. REM sleep behavior disorder predicts functional dependency in early Parkinson’s disease. Park. Relat. Disord. 2019, 66, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Marvin, K. Purdue Pegboard Test (PPT). Available online: Https://Strokengine.ca/En/Assessments/Purdue-Pegboard-Test-Ppt/ (accessed on 31 July 2022).
- Haaxma, C.A.; Bloem, B.R.; Overeem, S.; Borm, G.F.; Horstink, M.W. Timed motor tests can detect subtle motor dysfunction in early Parkinson’s disease. Mov. Disord. 2010, 25, 1150–1156. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Lang, A.E.; Gagnon, J.F.; Pelletier, A.; Montplaisir, J.Y. How does parkinsonism start? Prodromal parkinsonism motor changes in idiopathic REM sleep behaviour disorder. Brain 2012, 135 Pt 6, 1860–1870. [Google Scholar] [CrossRef] [PubMed]
- Skorvanek, M.; Martinez-Martin, P.; Kovacs, N.; Zezula, I.; Rodriguez-Violante, M.; Corvol, J.C.; Taba, P.; Seppi, K.; Levin, O.; Schrag, A.; et al. Relationship between the MDS-UPDRS and Quality of Life: A large multicenter study of 3206 patients. Park. Relat. Disord. 2018, 52, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Yahalom, G.; Yekutieli, Z.; Israeli-Korn, S.; Elincx-Benizri, S.; Livneh, V.; Fay-Karmon, T.; Tchelet, K.; Rubel, Y.; Hassin-Baer, S. Smartphone Based Timed Up and Go Test Can Identify Postural Instability in Parkinson’s Disease. Isr. Med. Assoc. J. 2020, 22, 37–42. [Google Scholar]
- Tchelet, K.; Stark-Inbar, A.; Yekutieli, Z. Pilot Study of the EncephaLog Smartphone Application for Gait Analysis. Sensors 2019, 19, 5179. [Google Scholar] [CrossRef] [Green Version]
- Salama, M.; Ellaithy, A.; Helmy, B.; El-Gamal, M.; Tantawy, D.; Mohamed, M.; Sheashaa, H.; Sobh, M.; Arias-Carrión, O. Colchicine protects dopaminergic neurons in a rat model of Parkinson’s disease. CNS Neurol Disord. Drug Targets 2012, 11, 836–843. [Google Scholar] [CrossRef]
- Rai, S.N.; Zahra, W.; Singh, S.S.; Birla, H.; Keswani, C.; Dilnashin, H.; Rathore, A.S.; Singh, R.; Singh, R.K.; Singh, S.P. Anti-inflammatory Activity of Ursolic Acid in MPTP-Induced Parkinsonian Mouse Model. Neurotox Res. 2019, 36, 452–462. [Google Scholar] [CrossRef]
- Mahlknecht, P.; Marini, K.; Werkmann, M.; Poewe, W.; Seppi, K. Prodromal Parkinson’s disease: Hype or hope for disease-modification trials? Transl. Neurodegener. 2022, 11, 11. [Google Scholar] [CrossRef]


{kind=link}
| Total | |
|---|---|
| Male | 43 |
| Age, median (range) | 51 (40–73) |
| Age categories | |
| 40–44 | 22 |
| 45–49 | 20 |
| 50–54 | 16 |
| 55–59 | 11 |
| 60–64 | 11 |
| 65–69 | 11 |
| 70–74 | 7 |
| GBA1variant * | |
| N370 | 71 |
| 84GG | 12 |
| L444P | 5 |
| R496H | 4 |
| V394L | 3 |
| Other ** | 3 |
| Relatives with Parkinson’s disease | 25 |
| 1st degree | 15 |
| 2nd degree | 13 |
| Caffeine use *** | 82 |
| Smoking *** | |
| Current | 9 |
| Former | 23 |
| Never | 61 |
| Regular pesticide exposure *** | 6 |
| Occupational solvent exposure *** | 4 |
| Median (Range) | Abnormal Cutoff * | Abnormal/Tested (%) | |
|---|---|---|---|
| (a) Imaging | |||
| Transcranial sonography, cm2 | 0.12 (0–0.28) | ≥0.2 | 20/91 (22) |
| (b) Sensory and autonomic | |||
| Color discrimination test (Total error score) | 41.5 (4–171) | Age 40–49 years > 100 Age 50–59 years > 130 Age 60–69 years > 170 Age 70–79 years > 195 | 2/92 (2.2) |
| UPSIT smell test | 10 (0–12) | <8 | 12/97 (12.4) |
| Orthostatic hypotension | NR | >20 SBP or > 10 mmHg DBP | 6/98 (6.1) |
| Bowel movement (daily) | NR | ≤0.5 | 4/98 (4.1) |
| Urinary dysfunction | NR | Yes/No | 15/92 (16.3) |
| Erectile dysfunction | NR | Yes/No | 7/43 male (16.6) |
| (c) Cognitive and mental | |||
| Beck depression inventory | 4 (0–25) | ≥14 | 9/96 (9.4) |
| Frontal assessment battery | 18 (15–18) | <16 | 2/96 (2.1) |
| MoCA- Total score Visuospatial/executive Language fluency | 28 (22–30) 4 (2–5) 1 (0–1) | ≤25 ≤3 =0 | 23/97 (23.7) 26/98 (26.5) 15/98 (15.3) |
| NeuroTrax- Memory Executive function Attention Information processing Visual-spatial Verbal function Motor skills Global cognitive score | 104.5 (61.1–114.5) 106.1 (77.7–134.2) 103.9 (63.5–119.4) 101.7 (69.1–139) 109.1 (59–132.3) 107.6 (38.2–116.4) 108.4 (69.2–120.5) 104.7 (89.4–120.8) | <85 percentiles <85 percentiles <85 percentiles <85 percentiles <85 percentiles <85 percentiles <85 percentiles <85 percentiles | 8/98 (8.1) 3/98 (3.1) 3/98 (3.1) 7/97 (7.2) 10/98 (10.2) 6/98 (6.1) 1/97 (1.03) 0/98 (0) |
| (d) Sleeping disorder | |||
| REM sleep behavior disorder | 2 (0–12) | ≥5 | 11/96 (11.5) |
| Epworth sleepiness scale | 6 (0–20) | >10 | 11/98 (11.2) |
| (e) Motor | |||
| Perdue pegboard | 14.3 (8.2–18.8) | <11 ** | 2/96 (2.1) |
| UPDRS-III | 2 (0–13) | >6 *** | 16/93 (17.2) |
| iTUG time, seconds | 19.9 (14.6–25.9) | NA | NA |
| (a) Sex | Female (n = 55) | Male (n = 43) | p |
|---|---|---|---|
| Transcranial sonography, cm | 0.09 (0–0.27) | 0.13 (0.06–0.28) | <0.001 |
| NeuroTrax Visual-spatial Motor skills | 105.1 (64.6–123.9) 106 (69.2–119.5) | 113.6 (89.1–132.4) 111.1 (93.7–120.5) | 0.003 <0.001 |
| Beck depression inventory | 5 (0–25) | 2 (0–20) | <0.001 |
| (b) Family history | No (n = 73) | Yes (n = 25) | |
| NeuroTrax Executive function Visual-spatial Global cognitive score | 109.8 (79.7–134.2) 110.2 (64.6–132.4) 106.1 (89.9–120.5) | 100.8 (77.7–122.9) 99.8 (69.3–120.5) 101.7 (89.4–112.4) | 0.003 0.008 0.004 |
| GBA1 Variant | Number of Subjects | % of “Abnormal” Tests per Subject * |
|---|---|---|
| N370 | 71 | 4.76 (0–43.48) |
| 84GG | 12 | 7.05 (0–34.78) |
| L444P | 5 | 23.81 (0–34.78) |
| R496H | 4 | 8.70 (0–31.82) |
| V394L | 3 | 0.00 (0–4.35) |
| Other ** | 3 | 4.35 (0–4.35) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Becker-Cohen, M.; Zimran, A.; Dinur, T.; Tiomkin, M.; Cozma, C.; Rolfs, A.; Arkadir, D.; Shulman, E.; Manor, O.; Paltiel, O.; et al. A Comprehensive Assessment of Qualitative and Quantitative Prodromal Parkinsonian Features in Carriers of Gaucher Disease—Identifying Those at the Greatest Risk. Int. J. Mol. Sci. 2022, 23, 12211. https://doi.org/10.3390/ijms232012211
Becker-Cohen M, Zimran A, Dinur T, Tiomkin M, Cozma C, Rolfs A, Arkadir D, Shulman E, Manor O, Paltiel O, et al. A Comprehensive Assessment of Qualitative and Quantitative Prodromal Parkinsonian Features in Carriers of Gaucher Disease—Identifying Those at the Greatest Risk. International Journal of Molecular Sciences. 2022; 23(20):12211. https://doi.org/10.3390/ijms232012211
Chicago/Turabian StyleBecker-Cohen, Michal, Ari Zimran, Tama Dinur, Maayan Tiomkin, Claudia Cozma, Arndt Rolfs, David Arkadir, Elena Shulman, Orly Manor, Ora Paltiel, and et al. 2022. "A Comprehensive Assessment of Qualitative and Quantitative Prodromal Parkinsonian Features in Carriers of Gaucher Disease—Identifying Those at the Greatest Risk" International Journal of Molecular Sciences 23, no. 20: 12211. https://doi.org/10.3390/ijms232012211