
Genotypes and Variants of BKPyV in Organ Donors after Brain Death

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Results
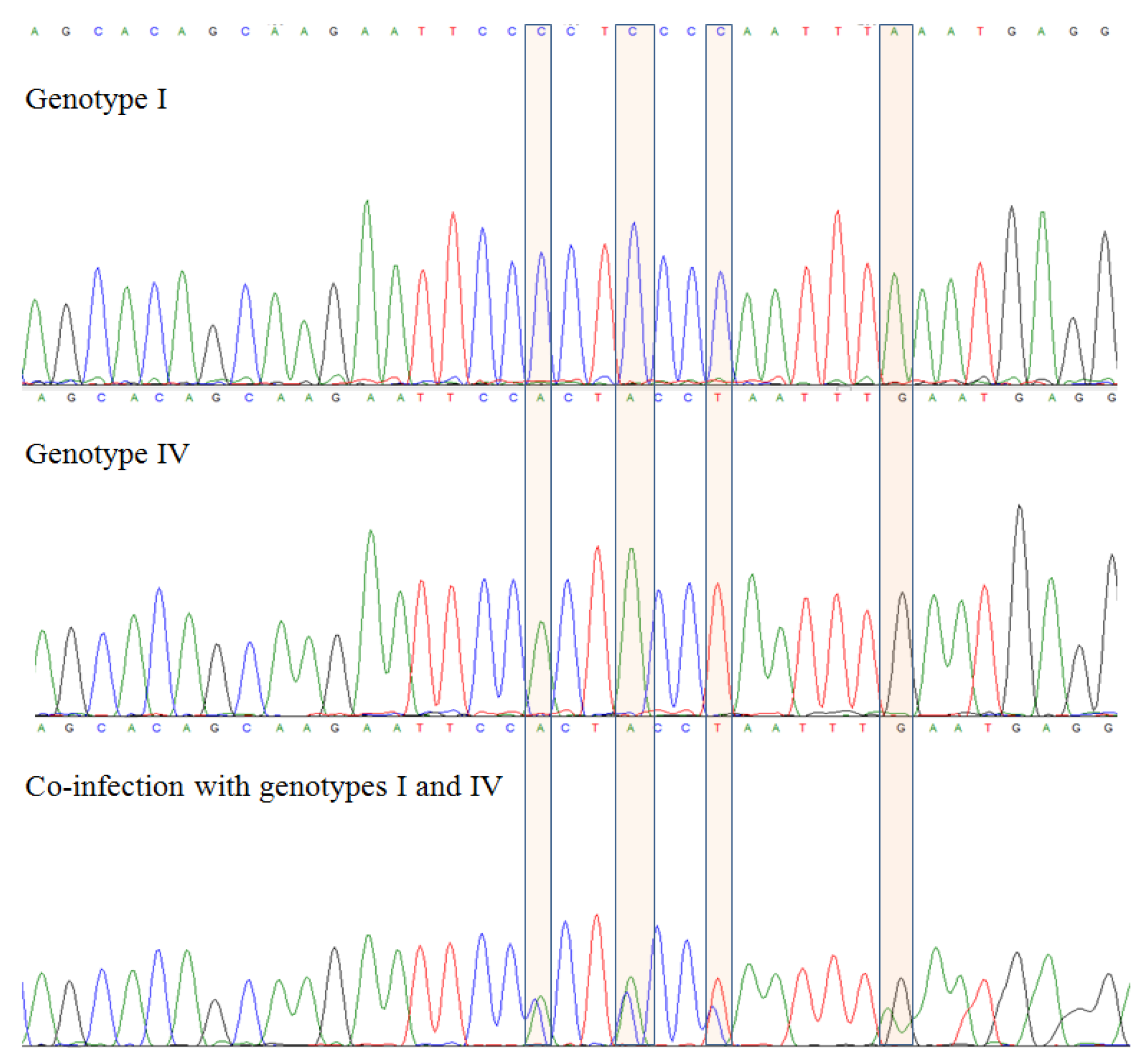
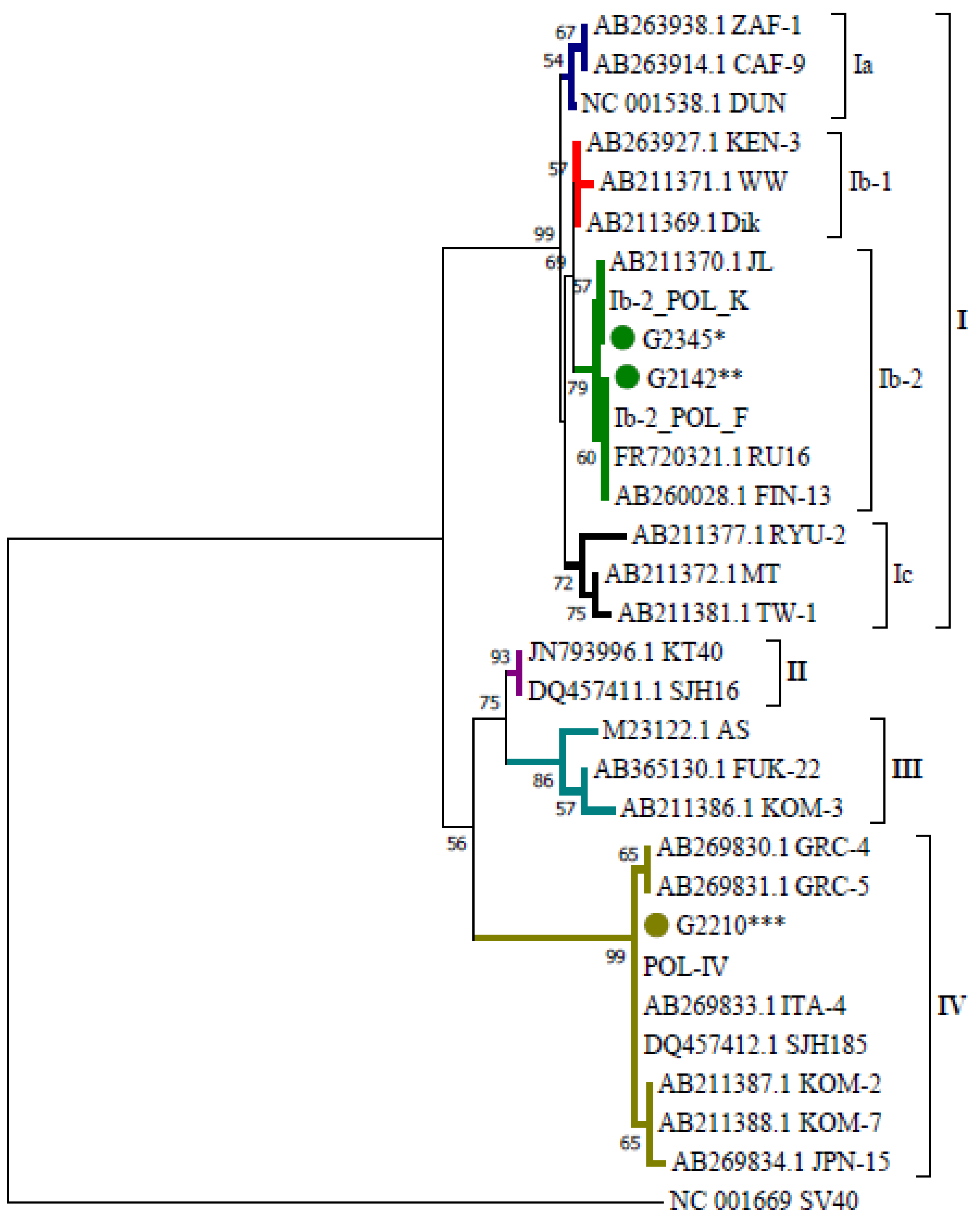
2.1. Genotypes
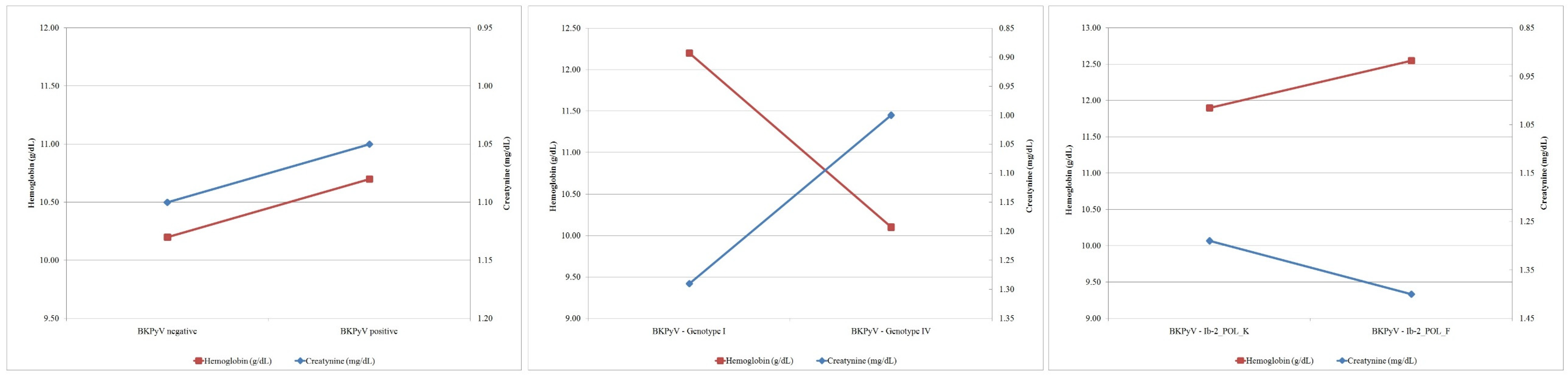
2.2. Biomarkers
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. DNA Extraction and PCR Amplification
4.3. Sequencing and Bioinformatic Processing
4.4. Evaluation of Viral Load
4.5. Blood Cell Count and Derived Ratios
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dalianis, T.; Hirsch, H.H. Human polyomaviruses in disease and cancer. Virology 2013, 437, 63–72. [Google Scholar] [CrossRef]
- Dekeyser, M.; François, H.; Beaudreuil, S.; Durrbach, A. Polyomavirus-specific cellular immunity: From BK-virus-specific cellular immunity to BK-virus-associated nephropathy? Front. Immunol. 2015, 6, 307. [Google Scholar] [CrossRef]
- Schmitt, C.; Raggub, L.; Linnenweber-Held, S.; Adams, O.; Schwarz, A.; Heim, A. Donor origin of BKV replication after kidney transplantation. J. Clin. Virol. 2014, 59, 120–125. [Google Scholar] [CrossRef]
- Bohl, D.L.; Storch, G.A.; Ryschkewitsch, C.; Gaudreault-Keener, M.; Schnitzler, M.A.; Major, E.O.; Brennan, D.C. Donor origin of BK virus in renal transplantation and role of HLA C7 in susceptibility to sustained BK viremia. Am. J. Transplant. 2005, 5, 2213–2221. [Google Scholar] [CrossRef]
- Sawinski, D.; Goral, S. BK virus infection: An update on diagnosis and treatment. Nephrol. Dial. Transplant. 2015, 30, 209–217. [Google Scholar] [CrossRef]
- Sayilar, E.I.; Çelik, S.; Ince, M.E.; Ergün, I. The post-transplant neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in relation to graft function among renal transplant recipients. Duzce. Med. J. 2020, 22, 212–217. [Google Scholar] [CrossRef]
- Yombi, J.C.; Schwab, P.E.; Thienpont, E. Neutrophil-to-lymphocyte ratio (NLR) distribution shows a better kinetic pattern than C-reactive protein distribution for the follow-up of early inflammation after total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3287–3292. [Google Scholar] [CrossRef]
- Kwon, J.H.; Jang, J.W.; Kim, Y.W.; Lee, S.W.; Nam, S.W.; Jaegal, D.; Lee, S.; Bae, S.H. The usefulness of C-reactive protein and neutrophil-to-lymphocyte ratio for predicting the outcome in hospitalized patients with liver cirrhosis. BMC Gastroenterol. 2015, 15, 146. [Google Scholar] [CrossRef]
- Li, H.; Lu, X.; Xiong, R.; Wang, S. High Neutrophil-to-Lymphocyte Ratio Predicts Cardiovascular Mortality in Chronic Hemodialysis Patients. Mediat. Inflamm. 2017, 2017, 9327136. [Google Scholar] [CrossRef]
- Mureșan, A.V.; Russu, E.; Arbănași, E.M.; Kaller, R.; Hosu, I.; Arbănași, E.M.; Voidăzan, S.T. The predictive value of NLR, MLR, and PLR in the outcome of end-stage kidney disease patients. Biomedicines 2022, 10, 1272. [Google Scholar] [CrossRef]
- Liu, J.; Ao, W.; Zhou, J.; Luo, P.; Wang, Q.; Xiang, D. The correlation between PLR-NLR and prognosis in acute myocardial infarction. Am. J. Transl. Res. 2021, 13, 4892–4899. [Google Scholar] [PubMed]
- Fang, T.; Wang, Y.; Yin, X.; Zhai, Z.; Zhang, Y.; Yang, Y.; You, Q.; Li, Z.; Ma, Y.; Li, C.; et al. Diagnostic Sensitivity of NLR and PLR in Early Diagnosis of Gastric Cancer. J. Immunol. Res. 2020, 2020, 9146042. [Google Scholar] [CrossRef] [PubMed]
- Gabay, C.; Kushner, I. Acute-phase proteins and other systemic responses to inflammation. N. Engl. J. Med. 1999, 340, 448–454. [Google Scholar] [CrossRef]
- Furmaga, J.; Kowalczyk, M.; Furmaga, O.; Rokos, C.A.; Zapolski, T.; Krakowski, L.; Jakubczak, A.; Rudzki, S. Molecular Epidemiology and Variation of the BK Polyomavirus in the Population of Central and Eastern Europe Based on the Example of Poland. Viruses 2022, 14, 209. [Google Scholar] [CrossRef]
- Vuong, N.L.; Le Duyen, H.T.; Lam, P.K.; Tam, D.T.H.; Vinh Chau, N.V.; Chanpheaktra, N.; See Lum, L.; Pleités, E.; Jones, N.; Simmons, C. C-reactive protein as a potential biomarker for disease progression in dengue: A multi-country observational study. BMC Med. 2020, 18, 35. [Google Scholar] [CrossRef]
- Malik, P.; Patel, U.; Mehta, D.; Patel, N.; Kelkar, R.; Akrmah, M.; Gabrilove, J.L.; Sacks, H. Biomarkers and Outcomes of COVID-19 Hospitalisations: Systematic Review and Meta-Analysis. BMJ Evid-Based Med. 2020, 26, 107–108. [Google Scholar] [CrossRef]
- Vasileva, D.; Badawi, A. C-Reactive Protein as a Biomarker of Severe H1N1 Influenza. Inflamm. Res. 2019, 68, 39–46. [Google Scholar] [CrossRef]
- Kamminga, S.; van der Meijden, E.; Feltkamp, M.C.W.; Zaaijer, H.L. Seroprevalence of fourteen human polyomaviruses determined in blood donors. PLoS ONE 2018, 13, e0206273. [Google Scholar] [CrossRef]
- Antonsson, A.; Green, A.C.; Mallitt, K.A.; O’Rourke, P.K.; Pawlita, M.; Waterboer, T.; Neale, R.E. Prevalence and stability of antibodies to the BK and JC polyomaviruses: A long-term longitudinal study of Australians. J. Gen. Virol. 2010, 91, 1849–1853. [Google Scholar] [CrossRef]
- Boukoum, H.; Nahdi, I.; Sahtout, W.; Skiri, H.; Segondy, M.; Aouni, M. BK and JC virus infections in healthy patients compared to kidney transplant recipients in Tunisia. Microb. Pathog. 2016, 97, 204–208. [Google Scholar] [CrossRef]
- Egli, A.; Infanti, L.; Dumoulin, A.; Buser, A.; Samaridis, J.; Stebler, C.; Gosert, R.; Hirsch, H.H. Prevalence of Polyomavirus BK and JC Infection and Replication in 400 Healthy Blood Donors. J. Infect. Dis. 2009, 199, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Zhong, S.; Zheng, H.Y.; Suzuki, M.; Chen, Q.; Ikegaya, H.; Aoki, N.; Usuku, S.; Kobayashi, N.; Nukuzuma, S.; Yasuda, Y.; et al. Age-related urinary excretion of BK polyomavirus by nonimmunocompromised individuals. J. Clin. Microbiol. 2007, 45, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Alalawi, F.; Alnour, H.; El Kossi, M.; Jenkins, J.R.; Halawa, A. BK Virus Infection in Adult Renal Transplant Recipients; Risk Factors and their Impact on Allograft Survival. Trends Transpl. 2020, 13, 1–10. [Google Scholar] [CrossRef]
- Toan, P.Q.; Hang, D.T.T.; Anh, T.T.M.; Lanh, N.S.; Su, H.X. Identification of BK Virus Genotypes in Recipients of Renal Transplant in Vietnam. Transplant. Proc. 2019, 51, 2683–2688. [Google Scholar] [CrossRef] [PubMed]
- Boan, P.; Hewison, C.; Swaminathan, R.; Irish, A.; Warr, K.; Sinniah, R.; Pryce, T.M.; Flexman, J. Optimal use of plasma and urine BK viral loads for screening and predicting BK nephropathy. BMC Infect. Dis. 2016, 16, 342. [Google Scholar] [CrossRef]
- Funahashi, Y.; Kato, M.; Fujita, T.; Takai, S.; Kimura, Y.; Gotoh, M. Prevalence of polyomavirus positivity in urine after renal transplantation. Transpl. Proc. 2014, 46, 564–566. [Google Scholar] [CrossRef]
- Hsieh, M.C.; Hung, C.W.; Chiou, H.L.; Yang, S.F. Effect of a BK viruria reaction detected by qualitative polymerase chain reaction on the renal function of kidney transplant recipients. Mol. Med. Rep. 2013, 7, 1319–1323. [Google Scholar] [CrossRef]
- Abolbashari, S.; Shakeri, M.; Hami, M.; Gholoobi, A.; Chechaklou, A.H.; Damavandi, M.; Movaqar, A.; Yousefi, R.; Meshkat, Z.; Hajebi-Khaniki, S. Higher Viral Load of Polyomavirus Type BK but not JC among Renal Transplant Recipients in Comparison to Donors. Iran. J. Pathol. 2022, 17, 8–14. [Google Scholar] [CrossRef]
- Ikegaya, H.; Motani, H.; Saukko, P.; Sato, K.; Akutsu, T.; Sakurada, K. BK virus genotype distribution offers information of tracing the geographical origins of unidentitied cadaver. Forensic Sci. Int. 2007, 173, 41–46. [Google Scholar] [CrossRef]
- Carr, M.J.; McCormack, G.P.; Mutton, K.J.; Crowley, B. Unique BK virus non-coding control region (NCCR) variants in hematopoietic stem cell transplant recipients with and without hemorrhagic cystitis. J. Med. Virol. 2006, 78, 485–493. [Google Scholar] [CrossRef]
- Krumbholz, A.; Zell, R.; Egerer, R.; Sauerbrei, A.; Helming, A.; Gruhry, B.; Wutzler, P. Prevalence of BK virus subtype I in Germany. J. Med.Virol. 2006, 78, 1588–1598. [Google Scholar] [CrossRef] [PubMed]
- Nishimoto, Y.; Zheng, H.Y.; Zhong, S.; Ikegaya, H.; Chen, Q.; Sugimoto, C.; Kitamura, T.; Yogo, Y. An Asian origin for subtype IV BK virus based on phylogenetic analysis. J. Mol.Evol. 2007, 65, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Zheng, H.Y.; Nishimoto, Y.; Chen, Q.; Hasegawa, M.; Zhong, S.; Ikegaya, H.; Ohno, N.; Sugimoto, C.; Takasaka, T.; Kitamura, T.; et al. Relationships between BK virus lineages and human populations. Microbes Infect. 2007, 9, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Momynaliev, K.T.; Gorbatenko, E.V.; Shevtsov, A.B.; Gribanov, O.G.; Babenko, N.N.; Kaabak, M.M. Prevalence and subtypes of BK virus in pediatric renal transplant recipients in Russia. Pediatr. Transplant. 2012, 16, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Jin, L. Rapid Genomic Typing of BK Virus Directly from Clinical Specimens. Mol. Cell. Probes. 1993, 7, 331–334. [Google Scholar] [CrossRef] [PubMed]
- Furmaga, J.; Kowalczyk, M.; Zapolski, T.; Furmaga, O.; Krakowski, L.; Rudzki, G.; Jaroszyński, A.; Jakubczak, A. BK Polyomavirus—Biology, Genomic Variation and Diagnosis. Viruses 2021, 13, 1502. [Google Scholar] [CrossRef]
- Tremolada, S.; Delbue, S.; Larocca, S.; Carloni, C.; Elia, F.; Khalili, K.; Gordon, J.; Ferrante, P. Polymorphisms of the BK virus subtypes and their influence on viral in vitro growth efficiency. Virus Res. 2010, 149, 190–196. [Google Scholar] [CrossRef]
- Zhong, S.; Randhawa, P.S.; Ikegaya, H.; Chen, Q.; Zheng, H.Y.; Suzuki, M.; Takeuchi, T.; Shibuya, A.; Kitamura, T.; Yogo, Y. Distribution patterns of BK polyomavirus (BKV) subtypes and subgroups in American, European and Asian populations suggest co-migration of BKV and the human race. J. Gen. Virol. 2009, 90, 144–152. [Google Scholar] [CrossRef]
- Morel, V.; Martin, E.; Francois, C.; Helle, F.; Faucher, J.; Mourez, T.; Choukroun, G.; Duverlie, G.; Castelain, S.; Brochot, E. A Simple and Reliable Strategy for BK Virus Subtyping and Subgrouping. J. Clin. Microbiol. 2017, 55, 1177–1185. [Google Scholar] [CrossRef]
- Ikegaya, H.; Saukko, P.J.; Tertti, R.; Metsarinne, K.P.; Carr, M.J.; Crowley, B.; Sakurada, K.; Zheng, H.-Y.; Kitamura, T.; Yogo, Y. Identification of a genomic subgroup of BK polyomavirus spread in European populations. J. Gen. Virol. 2006, 87, 3201–3208. [Google Scholar] [CrossRef]
- Muñoz-Gallego, I.; Díaz-Madridano, N.; Moral, N.; Pascual, C.; Polanco, N.; González, E.; Andres, A.; Folgueira, M.D. Detection of BK polyomavirus genotypes to predict the development of BK polyomavirus-associated complications in kidney transplant recipients: A retrospective analysis. Transpl. Infect. Dis. 2021, 23, e13615. [Google Scholar] [CrossRef] [PubMed]
- Shen, C.-L.; Wu, B.-S.; Lien, T.-J.; Yang, A.-H.; Yang, C.-Y. BK Polyomavirus Nephropathy in Kidney Transplantation: Balancing Rejection and Infection. Viruses 2021, 13, 487. [Google Scholar] [CrossRef] [PubMed]
- Halazun, K.J.; Marangoni, G.; Hakeem, A.; Fraser, S.M.; Farid, S.G.; Ahmad, N. Elevated preoperative recipient neutrophil-lymphocyte ratio is associated with delayed graft function following kidney transplantation. Transplant. Proc. 2013, 45, 3254–3257. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, M.; Agrawal, A.; Goyal, A.; Rangaswami, J. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio predict acute cellular rejection in the kidney allograft. Ann. Transplant. 2018, 23, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Królicki, T.; Bardowska, K.; Koscielska-Kasprzak, K.; Mazanowska, O.; Krajewska, M.; Kamińska, D. Systemic inflammatory markers predict detrimental outcome of urosepsis in kidney transplant recipients. Transplant. Proc. 2020, 52, 2382–2387. [Google Scholar] [CrossRef]
- Pinto, A.Y.D.; Valente, V.D.; Coura, J.R.; Valente, S.A.D.; Junqueira, A.C.V.; Santos, L.C.; Ferreira, A.G.; de Macedo, R.C. Clinical Follow-Up of Responses to Treatment with Benznidazol in Amazon: A Cohort Study of Acute Chagas Disease. PLoS ONE 2013, 8, e64450. [Google Scholar] [CrossRef]
- Randhawa, P.S.; Khaleel-Ur-Rehman, K.; Swalsky, P.A.; Vats, A.; Scantlebury, V.; Shapiro, R.; Finkelstein, S. DNA sequencing of viral capsid protein VP-1 region in patients with BK virus interstitial nephritis. Transplantation 2002, 73, 1090–1094. [Google Scholar] [CrossRef]
- Proctor, M.J.; McMillan, D.C.; Morrison, D.S.; Fletcher, C.D.; Horgan, P.G.; Clarke, S.J. A derived neutrophil to lymphocyte ratio predicts survival in patients with cancer. Br. J. Cancer 2012, 107, 695–699. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| BKPyV Positive | Total BKPyV Negative | Total | ||||
|---|---|---|---|---|---|---|
| Genotype I (Ib-2_POL_K/Ib-2_POL_F) | Genotype IV | Genotype I and IV (Co-Infection) | Total BKPyV Positive | |||
| M | 16 (10/6)—(23.19%–14.49%/8.70%) | 14 (20.29%) | 3 (4.35%) | 33 (47.83%) | 36 (52.17%) | 69 (100%) |
| F | 5 (3/2)—(14.71%–8.82%/5.88%) | 10 (29.41%) | 1 (2.94%) | 16 (47.06%) | 18 (52.94%) | 34 (100%) |
| Total | 21 (13/8)—(20.39%–12.62%/7.77%) | 24 (23.30%) | 4 (3.88%) | 49 (47.57%) | 54 (52.43%) | 103 (100%) |
| Average Viral Load (Copies/mL) | FREQUENCY | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Sex | Age | Number | Average Number of Copies | Genotype I | Genotype IV | Subtype-Variant | |||
| Ib-2_POL_K | Ib-2_POL_F | POL-IV | Co-Infection | ||||||
| M | <20 | 2 (6.06%) | 3.07 × 103 | - | 8.30 × 102 | - | - | 1 | 1 |
| 20–29 | 3 (9.09%) | 3.37 × 103 | 4.86 × 103 | 4.10 × 102 | 1 | 1 | 1 | - | |
| 30–39 | 5 (15.15%) | 1.52 × 106 | 2.32 × 106 | 3.25 × 105 | - | 3 | 2 | - | |
| 40–49 | 9 (27.27%) | 1.27 × 106 | 2.25 × 106 | 6.46 × 104 | 4 | 1 | 3 | 1 | |
| 50–59 | 12 (36.36) | 2.01 × 104 | 7.75 × 103 | 3.88 × 104 | 5 | 1 | 5 | 1 | |
| 60–69 | 2 (6.06%) | 2.45 × 103 | - | 2.45 × 103 | - | - | 2 | - | |
| Total | 33 | 5.86 × 105 | 1.14 × 106 | 7.46 × 104 | 10 (30.30%) | 6 (18.18%) | 14 (42.42%) | 3 (9.09%) | |
| F | <20 | - | - | - | - | ||||
| 20–29 | 3 (18.75%) | 1.24 × 106 | - | 1.24 × 106 | - | - | 3 | - | |
| 30–49 | - | - | - | - | |||||
| 40–49 | 3 (18.75%) | 2.37 × 107 | 2.37 × 107 | - | 2 | 1 | - | - | |
| 50–59 | 7 (43.75%) | 1.27 × 104 | 2.12 × 103 | 7.11 × 103 | 1 | 1 | 4 | 1 | |
| 60–69 | 3 (18.75%) | 1.77 × 104 | - | 1.77 × 104 | - | - | 3 | - | |
| Total | 16 | 4.68 × 106 | 1.42 × 107 | 3.81 × 105 | 3 (18.75%) | 2 (12.50%) | 10 (62.50%) | 1 (6.25%) | |
| M and F | <20 | 2 (4.08%) | 3.07 × 103 | - | 8.30 × 102 | - | - | 1 | 1 |
| 20–29 | 6 (12.24%) | 6.23 × 105 | 4.86 × 103 | 9.33 × 105 | 1 | 1 | 4 | - | |
| 30–39 | 5 (10.20%) | 1.52 × 106 | 2.32 × 106 | 3.25 × 105 | - | 3 | 2 | - | |
| 40–49 | 12 (24.49%) | 6.87 × 106 | 1.03 × 107 | 6.46 × 104 | 6 | 2 | 3 | 1 | |
| 50–59 | 19 (38.78%) | 1.74 × 104 | 6.34 × 103 | 2.47 × 104 | 6 | 2 | 9 | 2 | |
| 60–69 | 5 (10.20%) | 1.16 × 104 | - | 1.16 × 104 | - | - | 5 | - | |
| Total | 49 | 1.92 × 106 | 4.25 × 106 | 2.02 × 105 | 13 (26.53%) | 8 (16.33%) | 24 (48.98%) | 4 (8.16%) | |
| BKPyV (+) | BKPyV (−) | Total | p-Value | |||||
|---|---|---|---|---|---|---|---|---|
| Factor | Sex | Positive, n = 49 | Negative, n = 54 | n = 103 | ||||
| Mean | STD | Mean | STD | Mean | STD | |||
| Age | M | 43.55 | 13.34 | 37.53 | 14.25 | 40.41 | 14.05 | 0.708 |
| F | 48.88 | 15.35 | 44.67 | 14.15 | 46.65 | 14.66 | 0.741 | |
| Total | 45.29 | 14.09 | 39.91 | 14.49 | 42.47 | 14.48 | 0.849 | |
| BMl | M | 25.57 | 3.80 | 25.51 | 4.04 | 25.54 | 3.90 | 0.734 |
| F | 24.99 | 5.26 | 25.84 | 5.47 | 25.44 | 5.31 | 0.883 | |
| Total | 25.38 | 4.28 | 25.62 | 4.52 | 25.50 | 4.39 | 0.712 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Furmaga, J.; Kowalczyk, M.; Furmaga-Rokou, O.; Rokos, C.A.; Zapolski, T.; Krakowski, L.; Jakubczak, A.; Rudzki, S. Genotypes and Variants of BKPyV in Organ Donors after Brain Death. Int. J. Mol. Sci. 2022, 23, 9173. https://doi.org/10.3390/ijms23169173
Furmaga J, Kowalczyk M, Furmaga-Rokou O, Rokos CA, Zapolski T, Krakowski L, Jakubczak A, Rudzki S. Genotypes and Variants of BKPyV in Organ Donors after Brain Death. International Journal of Molecular Sciences. 2022; 23(16):9173. https://doi.org/10.3390/ijms23169173
Chicago/Turabian StyleFurmaga, Jacek, Marek Kowalczyk, Olga Furmaga-Rokou, Christos A. Rokos, Tomasz Zapolski, Leszek Krakowski, Andrzej Jakubczak, and Sławomir Rudzki. 2022. "Genotypes and Variants of BKPyV in Organ Donors after Brain Death" International Journal of Molecular Sciences 23, no. 16: 9173. https://doi.org/10.3390/ijms23169173