
A Scoping Analysis of Cathelicidin in Response to Organic Dust Exposure and Related Chronic Lung Illnesses

 ,
, 
Abstract
:1. Introduction
1.1. Rationale
1.2. Objectives
2. Results
2.1. Exposure to Organic Dust
2.2. Hypersensitivity Pneumonitis
2.3. COPD
2.3.1. Changes in Cathelicidin Level in COPD
2.3.2. Cathelicidin Level Correlates with Lung Function
2.3.3. Cathelicidin as an Antimicrobial Agent in Combating Infections in COPD
2.3.4. Cathelicidin Contributes to COPD Development
Cathelicidin Sustaining Persistent Inflammation in COPD
Cathelicidin Contributes to Lung Tissue Remodelling in COPD
Cathelicidin Enhances Mucous Production in COPD
2.3.5. Cathelicidin and Corticosteroids Treatment in COPD and Asthma
2.4. Asthma
2.4.1. Cathelicidin Levels Are Altered in Asthma
2.4.2. Cathelicidin Enhances Inflammation in Asthma
2.4.3. Cathelicidin as an Antimicrobial Agent in Combating Infections in Asthma
2.4.4. Cathelicidin and Vitamin D in Asthma and COPD
3. Discussion
Limitations
4. Materials and Methods
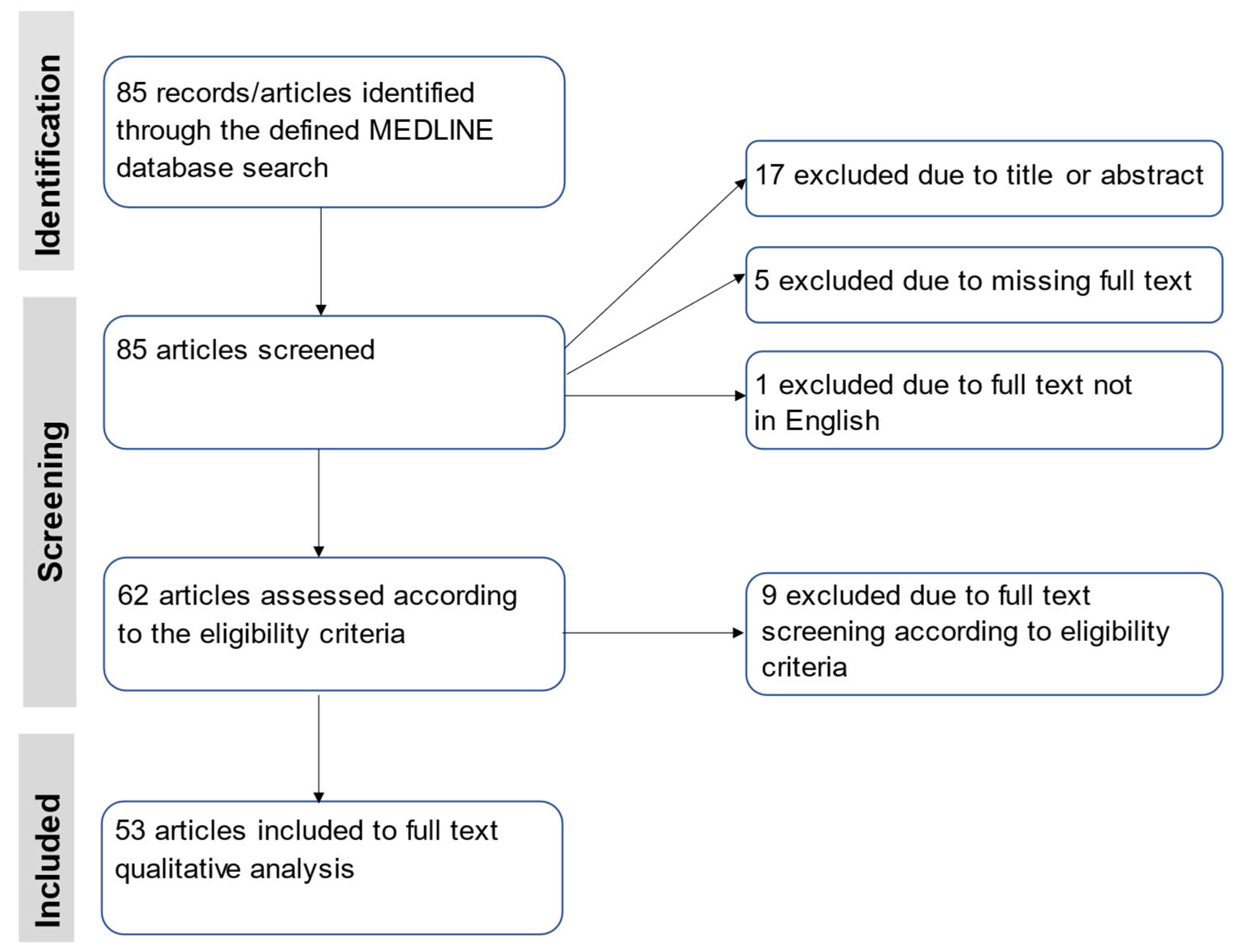
4.1. Search Strategy
4.2. Inclusion and Exclusion Criteria
4.3. Selection of Studies
4.4. Charting the Data
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Food and Agriculture Organization of the United Nations: World Food and Agriculture Statistical Pocketbook 2018. Rome. 2018. Available online: https://www.globalagriculture.org/fileadmin/files/weltagrarbericht/Weltagrarbericht/10B%C3%A4uerlicheIndustrielleLW/Pocketbook2018.pdf (accessed on 1 December 2021).
- Rylander, R. Endotoxin and occupational airway disease. Curr. Opin. Allergy Clin. Immunol. 2006, 6, 62–66. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.; Romberger, D.J. Immunological and inflammatory responses to organic dust in agriculture. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 126–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Góra, A.; Mackiewicz, B.; Krawczyk, P.; Golec, M.; Skórska, C.; Sitkowska, J.; Cholewa, G.; Larsson, L.; Jarosz, M.; Wójcik-Fatla, A.; et al. Occupational exposure to organic dust, microorganisms, endotoxin and peptidoglycan among plants processing workers in Poland. Ann. Agric. Environ. Med. 2009, 16, 143–150. [Google Scholar] [PubMed]
- Harkema, J.R.; Hotchkiss, J.A. Ozone- and endotoxin-induced mucous metaplasias in rat airway epithelium: Novel animal models to study toxicant-induced epithelial transformation in airways. Toxicol. Lett. 1993, 68, 251–263. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Thorne, P.S.; Yagla, S.J.; Burmeister, L.F.; Olenchock, S.A.; Watt, J.L.; Quinn, T.J. The role of endotoxin in grain dust-induced lung disease. Am. J. Respir. Crit. Care Med. 1995, 152, 603–608. [Google Scholar] [CrossRef]
- Schwartz, D.A.; Thorne, P.S.; Jagielo, P.J.; White, G.E.; Bleuer, S.A.; Frees, K.L. Endotoxin responsiveness and grain dust-induced inflammation in the lower respiratory tract. Am. J. Physiol. 1994, 267, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Nell, M.J.; Grote, J.J. Effects of bacterial toxins on air-exposed cultured human respiratory sinus epithelium. Ann. Otol. Rhinol. Laryngol. 2003, 112, 461–468. [Google Scholar] [CrossRef]
- Rosenfeld, Y.; Shai, Y. Lipopolysaccharide (Endotoxin)—Host defence antibacterial peptides interactions: Role in bacterial resistance and prevention of sepsis. Biochim. Biophys. Acta 2006, 1758, 1513–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Śpiewak, R.; Dutkiewicz, J. In vitro study of pro-inflammatory and anti-tumour properties of microvesicles from bacterial cell wall of Pantoea agglomerans. Ann. Agric. Environ. Med. 2008, 15, 153–161. [Google Scholar] [PubMed]
- Golec, M.; Reichel, C.; Mackiewicz, B.; Skorska, C.; Curzytek, K.; Lemieszek, M.; Dutkiewicz, J.; Gora, A.; Ziesche, R.; Boltuc, J.; et al. Cathelicidin LL-37, granzymes, TGF-beta1 and cytokines levels in induced sputum from farmers with and without COPD. Ann. Agric. Environ. Med. 2009, 16, 289–297. [Google Scholar] [PubMed]
- Diamond, G.; Russell, J.P.; Bevins, C.L. Inducible expression of an antibiotic peptide gene in lipopolysaccharide-challenged tracheal epithelial cells. Proc. Natl. Acad. Sci. USA 1995, 93, 5156–5160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nell, M.J.; Tjabringa, S.G.; Vonk, M.J.; Hiemstra, P.S.; Grote, J.J. Bacterial products increase expression of the human cathelicidin hCAP18/LL-37 in cultured human sinus epithelial cells. FEMS Immunol. Med. Microbiol. 2004, 42, 225–231. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, Y.; Papo, N.; Shai, Y. Endotoxin (lipopolysaccharide) neutralization by innate immunity host-defense peptides. J. Biol. Chem. 2006, 281, 1636–1643. [Google Scholar] [CrossRef] [Green Version]
- Selman, M.; Pardo, A.; King, T.E., Jr. Hypersensitivity pneumonitis: Insights in diagnosis and pathobiology. Am. J. Respir. Crit. Care Med. 2012, 186, 314–324. [Google Scholar] [CrossRef] [Green Version]
- Eisner, M.D.; Anthonisen, N.; Coultas, D.; Kuenzli, N.; Perez-Padilla, R.; Postma, D.; Romieu, I.; Silverman, E.K.; Balmes, J.R. An official American Thoracic Society public policy statement: Novel risk factors and the global burden of chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2010, 182, 693–718. [Google Scholar] [CrossRef]
- Salvi, S.S.; Barnes, P.J. Chronic obstructive pulmonary disease in non-smokers. Lancet 2009, 374, 733–743. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Pulmonary Disease: Global Strategy for the Diagnosis, Management and Prevention of COPD (2020 Report). Available online: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf (accessed on 1 December 2021).
- Zhang, Y.; Ye, B.; Zheng, H.; Zhang, W.; Han, L.; Yuan, P.; Zhang, C. Association between Organic Dust Exposure and Adult-Asthma: A Systematic Review and Meta-Analysis of Case-Control Studies. Allergy Asthma Immunol. Res. 2019, 11, 818–829. [Google Scholar] [CrossRef]
- Wunschel, J.; Poole, J.A. Occupational agriculture organic dust exposure and its relationship to asthma and airway inflammation in adults. J. Asthma 2016, 53, 471–477. [Google Scholar] [CrossRef] [Green Version]
- Brandsma, C.A.; Van den Berge, M.; Hackett, T.L.; Brusselle, G.; Timens, W. Recent advances in chronic obstructive pulmonary disease pathogenesis: From disease mechanisms to precision medicine. J. Pathol. 2020, 250, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Vasakova, M.; Selman, M.; Morell, F.; Sterclova, M.; Molina-Molina, M.; Raghu, G. Hypersensitivity Pneumonitis: Current Concepts of Pathogenesis and Potential Targets for Treatment. Am. J. Respir. Crit. Care Med. 2019, 200, 301–308. [Google Scholar] [CrossRef] [PubMed]
- Cevhertas, L.; Ogulur, I.; Maurer, D.J.; Burla, D.; Ding, M.; Jansen, K.; Koch, J.; Liu, C.; Ma, S.; Mitamura, Y.; et al. Advances and recent developments in asthma in 2020. Allergy 2020, 75, 3124–3146. [Google Scholar] [CrossRef] [PubMed]
- Golec, M. Cathelicidin LL-37: LPS-neutralizing, pleiotropic peptide. Ann. Agric. Environ. Med. 2007, 14, 1–4. [Google Scholar] [PubMed]
- Herr, C.; Shaykhiev, R.; Bals, R. The role of cathelicidin and defensins in pulmonary inflammatory diseases. Expert Opin. Biol. Ther. 2007, 7, 1449–1461. [Google Scholar] [CrossRef] [PubMed]
- 27 Ziesche, R.; Golec, M.; Samaha, E. The RESOLVE concept: Approaching pathophysiology of fibroproliferative disease in aged individuals. Biogerontology 2013, 14, 679–685. [Google Scholar] [CrossRef] [PubMed]
- Fabisiak, A.; Murawska, N.; Fichna, J. LL-37: Cathelicidin-related antimicrobial peptide with pleiotropic activity. Pharmacol. Rep. 2016, 68, 802–808. [Google Scholar] [CrossRef]
- Ginde, A.A.; Mansbach, J.M.; Camargo, C.A., Jr. Vitamin D, respiratory infections, and asthma. Curr. Allergy Asthma Rep. 2009, 9, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Kerley, C.P.; Elnazir, B.; Faul, J.; Cormican, L. Vitamin D as an adjunctive therapy in asthma. Part 1: A review of potential mechanisms. Pulm. Pharmacol. Ther. 2015, 32, 60–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansdottir, S.; Monick, M.M. Vitamin D effects on lung immunity and respiratory diseases. Vitam. Horm. 2011, 86, 217–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Székely, J.I.; Pataki, Á. Effects of vitamin D on immune disorders with special regard to asthma, COPD and autoimmune diseases: A short review. Expert Rev. Respir. Med. 2012, 6, 683–704. [Google Scholar] [CrossRef] [PubMed]
- Bozinovski, S.; Anthony, D.; Vlahos, R. Targeting pro-resolution pathways to combat chronic inflammation in COPD. J. Thorac. Dis. 2014, 6, 1548–1556. [Google Scholar] [CrossRef] [PubMed]
- Casanova, V.; Sousa, F.H.; Stevens, C.; Barlow, P.G. Antiviral therapeutic approaches for human rhinovirus infections. Future Virol. 2018, 13, 505–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.Y.; Xiao, W.; Zhu, M.X.; Yang, Z.H.; Pan, X.J.; Zhang, Y.; Sun, C.-C.; Xing, Y. The effect of human antibacterial peptide LL-37 in the pathogenesis of chronic obstructive pulmonary disease. Respir. Med. 2012, 106, 1680–1689. [Google Scholar] [CrossRef] [Green Version]
- Lemieszek, M.K.; Sawa-Wejksza, K.; Golec, M.; Dutkiewicz, J.; Zwoliński, J.; Milanowski, J. Beneficial impact of cathelicidin on hypersensitivity pneumonitis treatment-in vivo studies. PLoS ONE 2021, 16, e0251237. [Google Scholar] [CrossRef]
- Golec, M.; Lemieszek, M.K.; Skórska, C.; Sitkowska, J.; Zwoliński, J.; Mackiewicz, B.; Góra-Florek, A.; Milanowski, J.; Dutkiewicz, J. Cathelicidin related antimicrobial peptide, laminin, Toll-like receptors and chemokines levels in experimental hypersensitivity pneumonitis in mice. Pathol. Biol. 2015, 63, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease—Global Initiative for Chronic Obstructive Lung Disease—GOLD (goldcopd.org). Available online: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf (accessed on 1 December 2021).
- Golec, M.; Reichel, C.; Lemieszek, M.; Mackiewicz, B.; Buczkowski, J.; Sitkowska, J.; Skòrska, C.; Dutkiewicz, J.; Milanowski, J.; Ziesche, R. Cathelicidin LL-37 in bronchoalveolar lavage and epithelial lining fluids from COPD patients and healthy individuals. J. Biol. Regul. Homeost. Agents 2012, 26, 617–625. [Google Scholar] [PubMed]
- Uysal, P.; Simsek, G.; Durmus, S.; Sozer, V.; Aksan, H.; Yurt, S.; Cuhadaroglu, C.; Kosar, F.; Gelisgen, R.; Uzun, H. Evaluation of plasma antimicrobial peptide LL-37 and nuclear factor-κB levels in stable chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 321–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.M.; Guo, Y.F.; Zhang, H.S.; Sun, T.Y. Antimicrobial peptide LL-37 circulating levels in chronic obstructive pulmonary disease patients with high risk of frequent exacerbations. J. Thorac. Dis. 2015, 7, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Burkes, R.M.; Ceppe, A.S.; Couper, D.J.; Comellas, A.P.; Wells, J.M.; Peters, S.P.; Criner, G.J.; Kanner, R.E.; Iii, R.P.; Christenson, S.A.; et al. Plasma Cathelicidin is Independently Associated with Reduced Lung Function in COPD: Analysis of the Subpopulations and Intermediate Outcome Measures in COPD Study Cohort. Chronic Obstr. Pulm. Dis. 2020, 7, 370–381. [Google Scholar] [CrossRef]
- Wright, T.K.; Gibson, P.G.; Simpson, J.L.; McDonald, V.M.; Wood, L.G.; Baines, K.J. Neutrophil extracellular traps are associated with inflammation in chronic airway disease. Respirology 2016, 21, 467–475. [Google Scholar] [CrossRef] [Green Version]
- Serré, J.; Mathyssen, C.; Ajime, T.T.; Korf, H.; Maes, K.; Heulens, N.; Gysemans, C.; Mathieu, C.; Vanaudenaerde, B.; Janssens, W.; et al. Airway infection with Nontypeable Haemophilus influenzae is more rapidly eradicated in vitamin D deficient mice. J. Steroid Biochem. Mol. Biol. 2019, 187, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Parameswaran, G.I.; Sethi, S.; Murphy, T.F. Effects of bacterial infection on airway antimicrobial peptides and proteins in COPD. Chest 2011, 140, 611–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mallia, P.; Footitt, J.; Sotero, R.; Jepson, A.; Contoli, M.; Trujillo-Torralbo, M.B.; Kebadze, T.; Aniscenko, J.; Oleszkiewicz, G.; Gray, K.; et al. Rhinovirus infection induces degradation of antimicrobial peptides and secondary bacterial infection in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 2012, 186, 1117–1124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangedal, S.; Nielsen, R.; Aanerud, M.; Persson, L.J.; Wiker, H.G.; Bakke, P.S.; Hiemstra, P.S.; Eagan, T.M. Sputum microbiota and inflammation at stable state and during exacerbations in a cohort of chronic obstructive pulmonary disease (COPD) patients. PLoS ONE 2019, 14, e0222449. [Google Scholar] [CrossRef] [Green Version]
- Tjabringa, G.S.; Ninaber, D.K.; Drijfhout, J.W.; Rabe, K.F.; Hiemstra, P.S. Human cathelicidin LL-37 is a chemoattractant for eosinophils and neutrophils that acts via formyl-peptide receptors. Int. Arch. Allergy Immunol. 2006, 140, 103–112. [Google Scholar] [CrossRef]
- Pouwels, S.D.; Hesse, L.; Faiz, A.; Lubbers, J.; Bodha, P.K.; ten Hacken, N.H.T.; van Oosterhout, A.J.M.; Nawijn, M.C.; Heijink, I.H. Susceptibility for cigarette smoke-induced DAMP release and DAMP-induced inflammation in COPD. Am. J. Physiol. Lung Cell Mol. Physiol. 2016, 311, L881–L892. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Z.; Zhang, Y.; Zhu, Y.; Li, C.; Zhou, L.; Li, X.; Zhang, F.; Qiu, X.; Qu, Y. Cathelicidin induces epithelial-mesenchymal transition to promote airway remodeling in smoking-related chronic obstructive pulmonary disease. Ann. Transl. Med. 2021, 9, 223. [Google Scholar] [CrossRef]
- Sun, C.; Zhu, M.; Yang, Z.; Pan, X.; Zhang, Y.; Wang, Q.; Xiao, W. LL-37 secreted by epithelium promotes fibroblast collagen production: A potential mechanism of small airway remodeling in chronic obstructive pulmonary disease. Lab. Investig. 2014, 94, 991–1002. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Jiang, Y.; Sun, C.; Wang, Q.; Yang, Z.; Pan, X.; Zhu, M.; Xiao, W. The human cathelicidin LL-37 enhances airway mucus production in chronic obstructive pulmonary disease. Biochem. Biophys. Res. Commun. 2014, 443, 103–109. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhu, M.; Yang, Z.; Pan, X.; Jiang, Y.; Sun, C.; Wang, Q.; Xiao, W. The human Cathelicidin LL-37 induces MUC5AC mucin production by airway epithelial cells via TACE-TGF-alpha-EGFR pathway. Exp. Lung Res. 2014, 40, 333–342. [Google Scholar] [CrossRef]
- Singanayagam, A.; Glanville, N.; Cuthbertson, L.; Bartlett, N.W.; Finney, L.J.; Turek, E.; Bakhsoliani, E.; Calderazzo, M.A.; Trujillo-Torralbo, M.-B.; Footitt, J.; et al. Inhaled corticosteroid suppression of cathelicidin drives dysbiosis and bacterial infection in chronic obstructive pulmonary disease. Sci. Transl. Med. 2019, 11, eaav3879. [Google Scholar] [CrossRef] [PubMed]
- Weng, J.Z.; Wang, Y.; Sun, T.Y. Cathelicidin LL-37 restoring glucocorticoid function in smoking and lipopolysaccharide-induced airway inflammation in rats. Chin. Med. J. 2019, 132, 569–576. [Google Scholar] [CrossRef]
- van den Berge, M.; Jonker, M.R.; Miller-Larsson, A.; Postma, D.S.; Heijink, I.H. Effects of fluticasone propionate and budesonide on the expression of immune defense genes in bronchial epithelial cells. Pulm. Pharmacol. Ther. 2018, 50, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Hsu, Y.P.; Ishizaka, A.; Kirikae, T.; Moss, R.B. Sputum cathelicidin, urokinase plasminogen activation system components, and cytokines discriminate cystic fibrosis, COPD, and asthma inflammation. Chest 2005, 128, 2316–2326. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Tan, X.; Liang, Y.; Hou, C.; Qu, D.; Li, M.; Huang, Q. Differential DAMP release was observed in the sputum of COPD, asthma and asthma-COPD overlap (ACO) patients. Sci. Rep. 2019, 9, 19241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arikoglu, T.; Akyilmaz, E.; Yildirim, D.D.; Batmaz, S.B.; Ulger, S.T.; Aslan, G.; Kuyucu, S. The relation of innate and adaptive immunity with viral-induced acute asthma attacks: Focusing on IP-10 and cathelicidin. Allergol. Immunopathol. 2017, 45, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Arikoglu, T.; Kuyucu, S.; Karaismailoglu, E.; Batmaz, S.B.; Balci, S. The association of vitamin D, cathelicidin, and vitamin D binding protein with acute asthma attacks in children. Allergy Asthma Proc. 2015, 36, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Rohde, G.; Message, S.D.; Haas, J.J.; Kebadze, T.; Parker, H.; Laza-Stanca, V.; Khaitov, M.; Kon, O.M.; Stanciu, L.A.; Mallia, P.; et al. CXC chemokines and antimicrobial peptides in rhinovirus-induced experimental asthma exacerbations. Clin. Exp. Allergy 2014, 44, 930–939. [Google Scholar] [CrossRef] [Green Version]
- Thijs, W.; Janssen, K.; van Schadewijk, A.M.; Papapoulos, S.E.; le Cessie, S.; Middeldorp, S.; Melissant, C.F.; Rabe, K.F.; Hiemstra, P.S. Nasal Levels of Antimicrobial Peptides in Allergic Asthma Patients and Healthy Controls: Differences and Effect of a Short 1,25(OH)2 Vitamin D3 Treatment. PLoS ONE 2015, 10, e0140986. [Google Scholar] [CrossRef] [PubMed]
- Jiao, D.; Wong, C.K.; Tsang, M.S.; Chu, I.M.; Liu, D.; Zhu, J.; Chu, M.; Lam, C.W.-K. Activation of Eosinophils Interacting with Bronchial Epithelial Cells by Antimicrobial Peptide LL-37: Implications in Allergic Asthma. Sci. Rep. 2017, 7, 1848. [Google Scholar] [CrossRef] [PubMed]
- Greiller, C.L.; Suri, R.; Jolliffe, D.A.; Kebadze, T.; Hirsman, A.G.; Griffiths, C.J.; Johnston, S.L.; Martineau, A.R. Vitamin D attenuates rhinovirus-induced expression of intercellular adhesion molecule-1 (ICAM-1) and platelet-activating factor receptor (PAFR) in respiratory epithelial cells. J. Steroid Biochem. Mol. Biol. 2019, 187, 152–159. [Google Scholar] [CrossRef]
- GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990-2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef] [Green Version]
- Persson, L.J.; Aanerud, M.; Hardie, J.A.; Nilsen, R.M.; Bakke, P.S.; Eagan, T.M.; Hiemstra, P. Antimicrobial peptide levels are linked to airway inflammation, bacterial colonisation and exacerbations in chronic obstructive pulmonary disease. Eur. Respir. J. 2017, 15, 1601328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemshekhar, M.; Piyadasa, H.; Mostafa, D.; Chow, L.N.Y.; Halayko, A.J.; Mookherjee, N. Cathelicidin and Calprotectin Are Disparately Altered in Murine Models of Inflammatory Arthritis and Airway Inflammation. Front. Immunol. 2020, 11, 1932. [Google Scholar] [CrossRef]
- Casanova, V.; Sousa, F.H.; Shakamuri, P.; Svoboda, P.; Buch, C.; D’Acremont, M.; Christophorou, M.A.; Pohl, J.; Stevens, C.; Barlow, P.G. Citrullination Alters the Antiviral and Immunomodulatory Activities of the Human Cathelicidin LL-37 During Rhinovirus Infection. Front. Immunol. 2020, 11, 85. [Google Scholar] [CrossRef]
- Kilsgård, O.; Andersson, P.; Malmsten, M.; Nordin, S.L.; Linge, H.M.; Eliasson, M.; Sörenson, E.; Erjefält, J.S.; Bylund, J.; Olin, A.I.; et al. Peptidylarginine deiminases present in the airways during tobacco smoking and inflammation can citrullinate the host defense peptide LL-37, resulting in altered activities. Am. J. Respir. Cell Mol. Biol. 2012, 46, 240–248. [Google Scholar] [CrossRef]
- Ramos-Martínez, E.; López-Vancell, M.R.; Fernández de Córdova-Aguirre, J.C.; Rojas-Serrano, J.; Chavarría, A.; Velasco-Medina, A.; Velázquez-Sámano, G. Reduction of respiratory infections in asthma patients supplemented with vitamin D is related to increased serum IL-10 and IFN gamma levels and cathelicidin expression. Cytokine 2018, 108, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Telcian, A.G.; Zdrenghea, M.T.; Edwards, M.R.; Laza-Stanca, V.; Mallia, P.; Johnston, S.L.; Stanciu, L.A. Vitamin D increases the antiviral activity of bronchial epithelial cells in vitro. Antivir. Res. 2017, 137, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Sousa, F.H.; Casanova, V.; Findlay, F.; Stevens, C.; Svoboda, P.; Pohl, J.; Proudfoot, L.; Barlow, P.G. Cathelicidins display conserved direct antiviral activity towards rhinovirus. Peptides 2017, 95, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Lahore, H.; McDonnell, S.L.; Baggerly, C.A.; French, C.B.; Aliano, J.L.; Bhattoa, H.P. Evidence that Vitamin D Supplementation Could Reduce Risk of Influenza and COVID-19 Infections and Deaths. Nutrients 2020, 12, 988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golec, M.; Reichel, C.; Lemieszek, M.; Buczkowski, J.; Mackiewicz, B.; Skórska, C.; Dutkiewicz, J.; Góra, A.; Ziesche, R.; Milanowski, J. Cathelicidin LL-37 in bronchoalveolar lavage and epithelial lining fluids from healthy individuals and sarcoidosis patients. J. Biol. Regul. Homeost. Agents 2014, 28, 73–79. [Google Scholar] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: http://www.prisma-statement.org/Extensions/ScopingReviews (accessed on 1 December 2021).
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tatsuta, M.; Kan-O, K.; Ishii, Y.; Yamamoto, N.; Ogawa, T.; Fukuyama, S.; Ogawa, A.; Fujita, A.; Nakanishi, Y.; Matsumoto, K. Effects of cigarette smoke on barrier function and tight junction proteins in the bronchial epithelium: Protective role of cathelicidin LL-37. Respir. Res. 2019, 20, 251. [Google Scholar] [CrossRef] [PubMed]
- Schrumpf, J.A.; Ninaber, D.K.; van der Does, A.M.; Hiemstra, P.S. TGF-β1 Impairs Vitamin D-Induced and Constitutive Airway Epithelial Host Defense Mechanisms. J. Innate Immun. 2020, 12, 74–89. [Google Scholar] [CrossRef] [PubMed]
- Mathyssen, C.; Serré, J.; Sacreas, A.; Everaerts, S.; Maes, K.; Verleden, S.; Verlinden, L.; Verstuyf, A.; Pilette, C.; Gayan-Ramirez, G.; et al. Vitamin D Modulates the Response of Bronchial Epithelial Cells Exposed to Cigarette Smoke Extract. Nutrients 2019, 6, 2138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schrumpf, J.A.; van Sterkenburg, M.A.; Verhoosel, R.M.; Zuyderduyn, S.; Hiemstra, P.S. Interleukin 13 exposure enhances vitamin D-mediated expression of the human cathelicidin antimicrobial peptide 18/LL-37 in bronchial epithelial cells. Infect. Immun. 2012, 80, 4485–4494. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.C.; Xiao, H.Q.; Brown, A.J.; Ritter, C.S.; Schroeder, J. Association of vitamin D and antimicrobial peptide production during late-phase allergic responses in the lung. Clin. Exp. Allergy 2012, 42, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, X.; Wang, H.; Li, Y.; Lan, N.; Yuan, X.; Wu, M.; Liu, Z.; Li, G. Allergen specific immunotherapy enhanced defense against bacteria via TGF-β1-induced CYP27B1 in asthma. Oncotarget 2017, 2, 68681–68695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goleva, E.; Searing, D.A.; Jackson, L.P.; Richers, B.N.; Leung, D.Y. Steroid requirements and immune associations with vitamin D are stronger in children than adults with asthma. J. Allergy Clin. Immunol. 2012, 129, 1243–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, P.; Wang, X.; Yang, X.; Liu, Z.; Wu, M.; Li, G. Budesonide suppresses pulmonary antibacterial host defense by down-regulating cathelicidin-related antimicrobial peptide in allergic inflammation mice and in lung epithelial cells. BMC Immunol. 2013, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gela, A.; Bhongir, R.K.; Mori, M.; Keenan, P.; Mörgelin, M.; Erjefält, J.S.; Herwald, H.; Egesten, A.; Kasetty, G. Osteopontin That Is Elevated in the Airways during COPD Impairs the Antibacterial Activity of Common Innate Antibiotics. PLoS ONE 2016, 5, e0146192. [Google Scholar] [CrossRef]
- Chen, K.; Liu, M.; Liu, Y.; Wang, C.; Yoshimura, T.; Gong, W.; Le, Y.; Tessarollo, L.; Wang, J.M. Signal relay by CC chemokine receptor 2 (CCR2) and formylpeptide receptor 2 (Fpr2) in the recruitment of monocyte-derived dendritic cells in allergic airway inflammation. J. Biol. Chem. 2013, 288, 16262–16273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaykhiev, R.; Beisswenger, C.; Kandler, K.; Senske, J.; Puchner, A.; Damm, T.; Behr, J.; Bals, R. Human endogenous antibiotic LL-37 stimulates airway epithelial cell proliferation and wound closure. Am. J. Physiol.-Lung Cell. Mol. Physiol. 2005, 289, 842–848. [Google Scholar] [CrossRef]
- Gennaro, R.; Zanetti, M. Structural features and biological activities of the cathelicidin-derived antimicrobial peptides. Biopolymers 2000, 55, 31–49. [Google Scholar] [CrossRef]
- Bowdish, D.M.E.; Davidson, D.J.; Scott, M.G.; Hancock, R.E.W. Immunomodulatory activities of small host defence peptides. Antimicrob. Agents Chemother. 2005, 49, 1727–1732. [Google Scholar] [CrossRef] [Green Version]
- Pütsep, K.; Carlsson, G.; Boman, H.G.; Andersson, M. Deficiency of antibacterial peptides in patients with morbus Kostmann: An observation study. Lancet 2002, 360, 1144–1149. [Google Scholar] [CrossRef]
- De Smet, K.; Contreras, R. Human antimicrobial peptides: Defensins, cathelicidins and histatins. Biotechnol. Lett. 2005, 27, 1337–1413. [Google Scholar] [CrossRef] [PubMed]
- Koczulla, R.; von Degenfeld, G.; Kupatt, C.; Krotz, F.; Zahler, S.; Gloe, T.; Issbrucker, K.; Unterberger, P.; Zaiou, M.; Lebherz, C.; et al. An angiogenic role for the human peptide antibiotic LL-37/hCAP-18. J. Clin. Investig. 2003, 111, 1665–1672. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Setting * | Study Type ** | ||
|---|---|---|---|
| Exposure to organic dust | 6 (11.3%) | clinical study | 26 (49.1%) |
| HP | 3 (5.6%) | cohort | 10 (18.9%) |
| COPD | 34 (64.1%) | cross-sectional | 16 (30.2%) |
| Asthma | 27 (51%) | animal model | 9 (17%) |
| in vitro | 11 (20.7%) | ||
| Publication Years | review | 7 (13.2%) | |
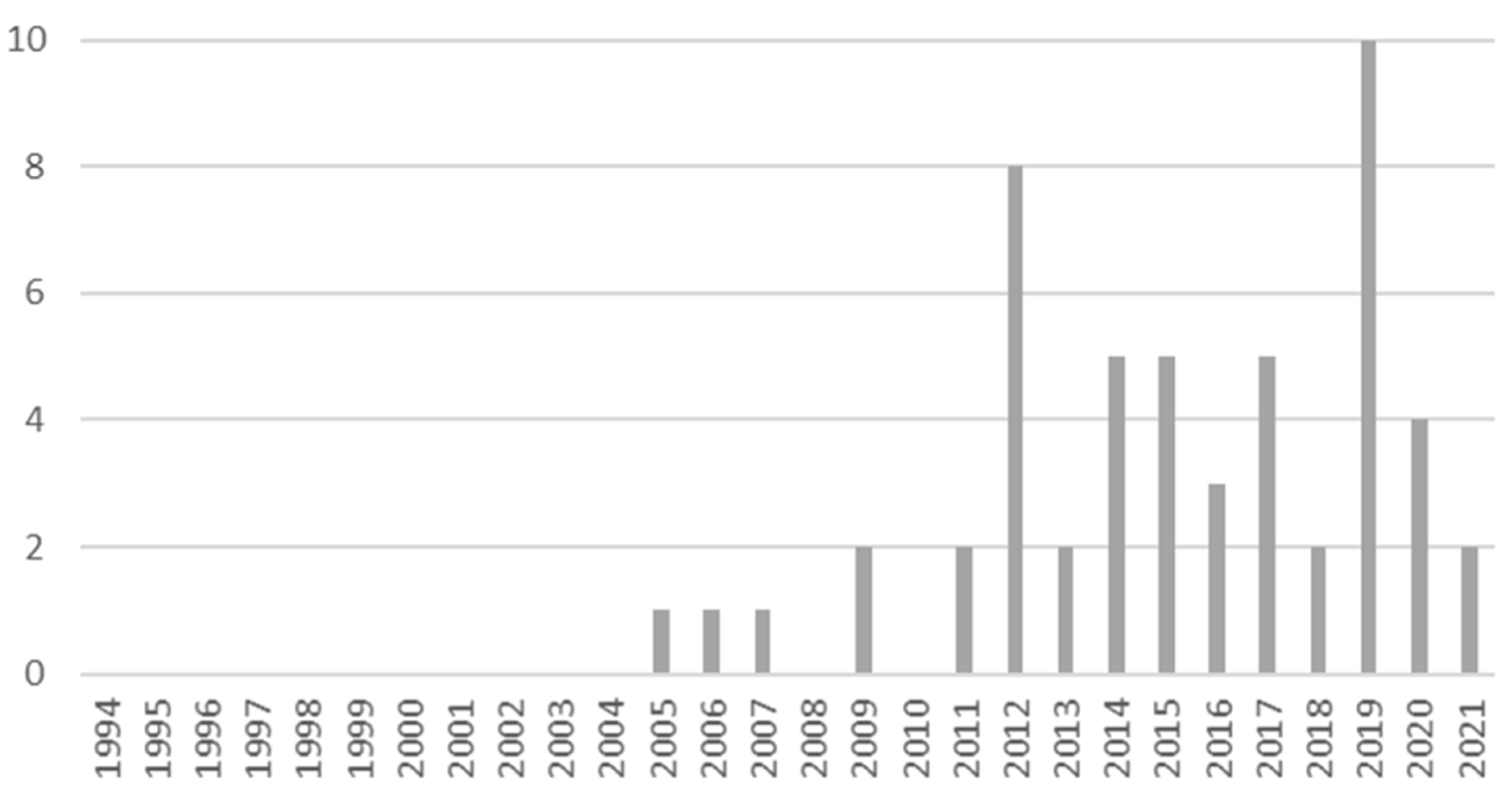
| 1994–2011 | 6 (14%) | Peptide ** | |
| 2012–2021 | 46 (86%) | LL-37 | 45 (84.9%) |
| Regions | CRAMP | 10 (18.9%) | |
| Europe | 29 (54.7%) | Sample Size of Clinical Studies # | |
| Asia | 13 (24.5%) | <100 | 17 (65.4%) |
| North America | 9 (17.0%) | 100–200 | 3 (11.5%) |
| Australia and Oceania | 2 (3.8%) | 200–500 | 5 (19.3%) |
| >500 | 1 (3.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Golec, M.; Lemieszek, M.K.; Dutkiewicz, J.; Milanowski, J.; Barteit, S. A Scoping Analysis of Cathelicidin in Response to Organic Dust Exposure and Related Chronic Lung Illnesses. Int. J. Mol. Sci. 2022, 23, 8847. https://doi.org/10.3390/ijms23168847
Golec M, Lemieszek MK, Dutkiewicz J, Milanowski J, Barteit S. A Scoping Analysis of Cathelicidin in Response to Organic Dust Exposure and Related Chronic Lung Illnesses. International Journal of Molecular Sciences. 2022; 23(16):8847. https://doi.org/10.3390/ijms23168847
Chicago/Turabian StyleGolec, Marcin, Marta Kinga Lemieszek, Jacek Dutkiewicz, Janusz Milanowski, and Sandra Barteit. 2022. "A Scoping Analysis of Cathelicidin in Response to Organic Dust Exposure and Related Chronic Lung Illnesses" International Journal of Molecular Sciences 23, no. 16: 8847. https://doi.org/10.3390/ijms23168847