
Safety of Special Waveform of Transcranial Electrical Stimulation (TES): In Vivo Assessment

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Results
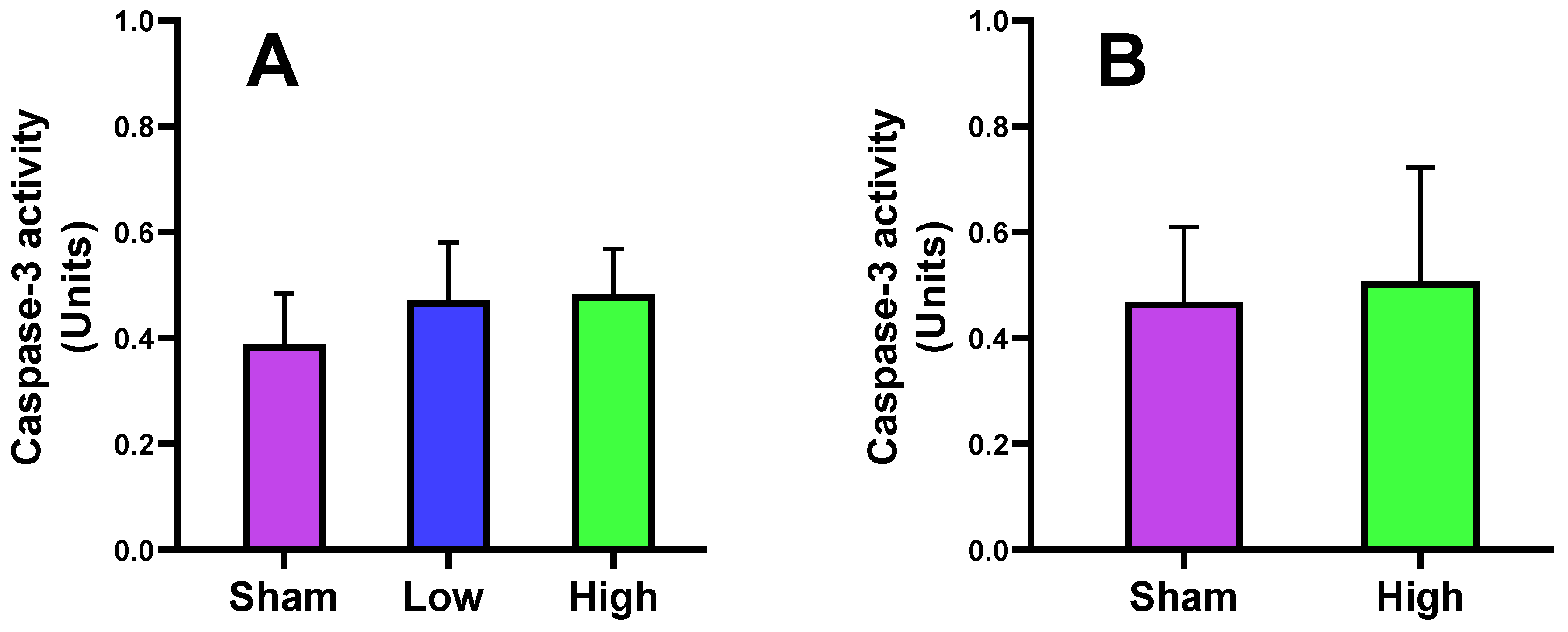
2.1. Effect of tDCS-iTBS on Caspase-3 Activity
2.2. Effect of tDCS-iTBS on Brain and Skin/Serum Biomarkers
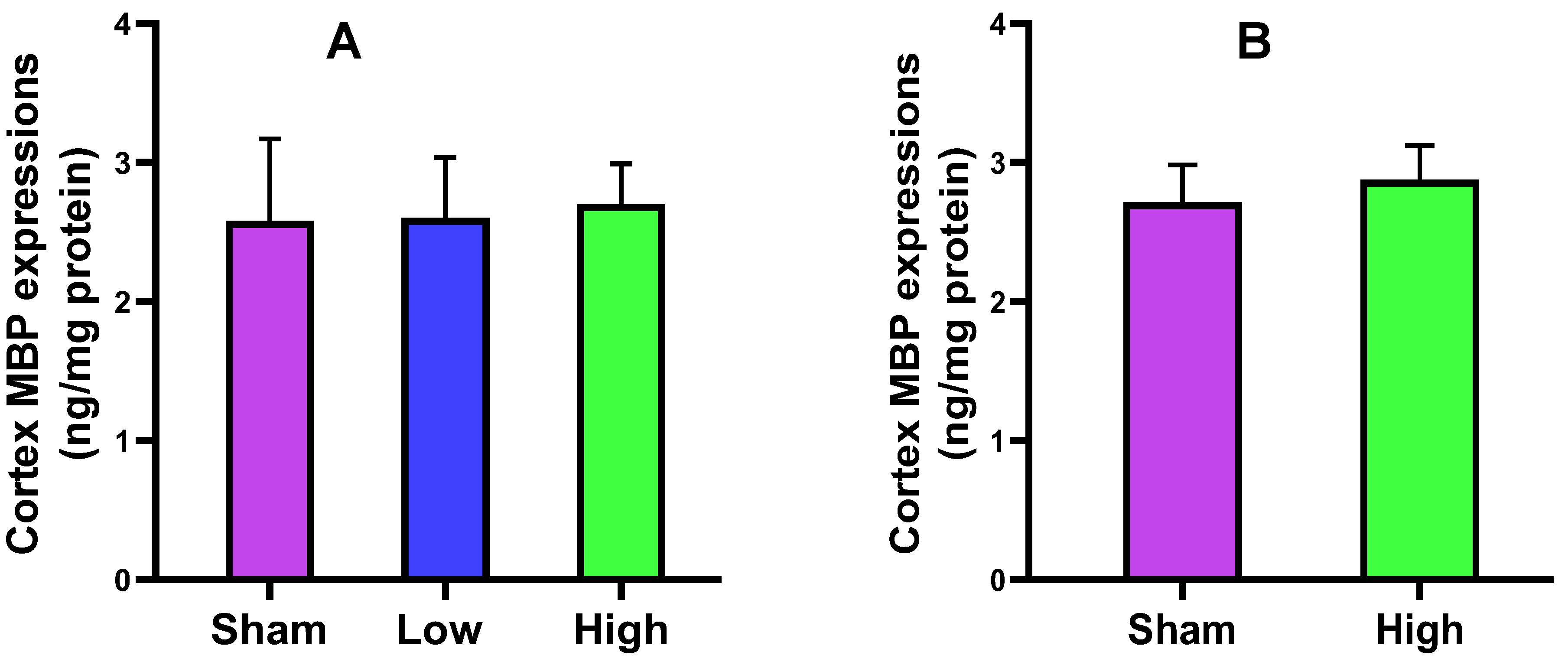
2.2.1. Cortical MBP Expression
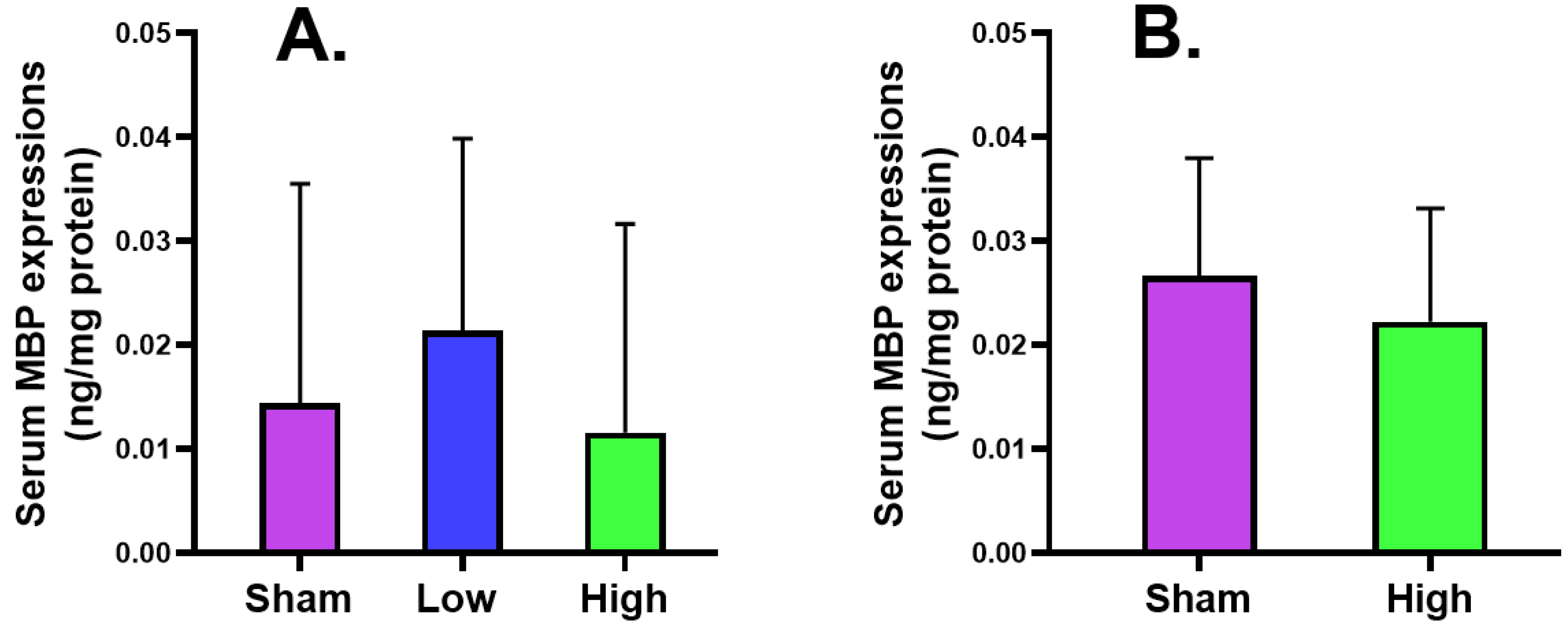
2.2.2. Serum MBP Expression
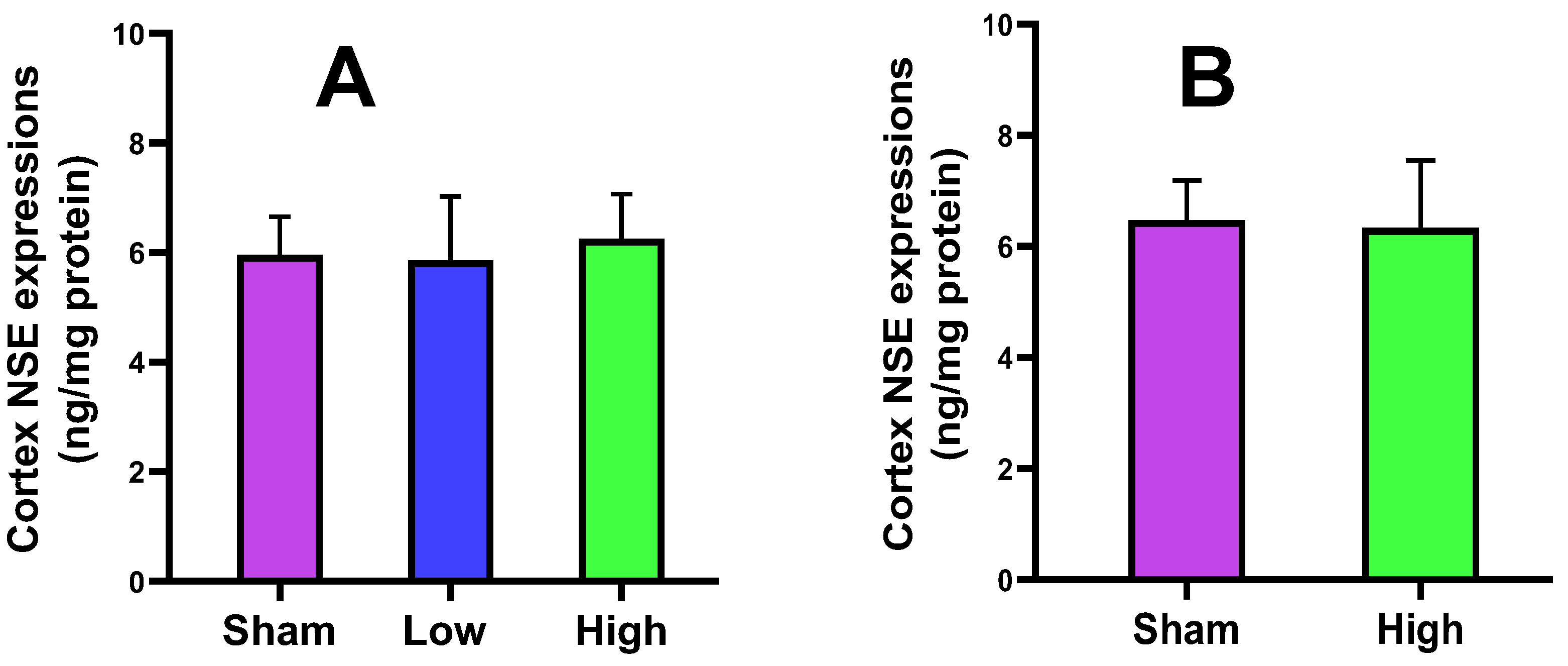
2.2.3. Cortical NSE Expression
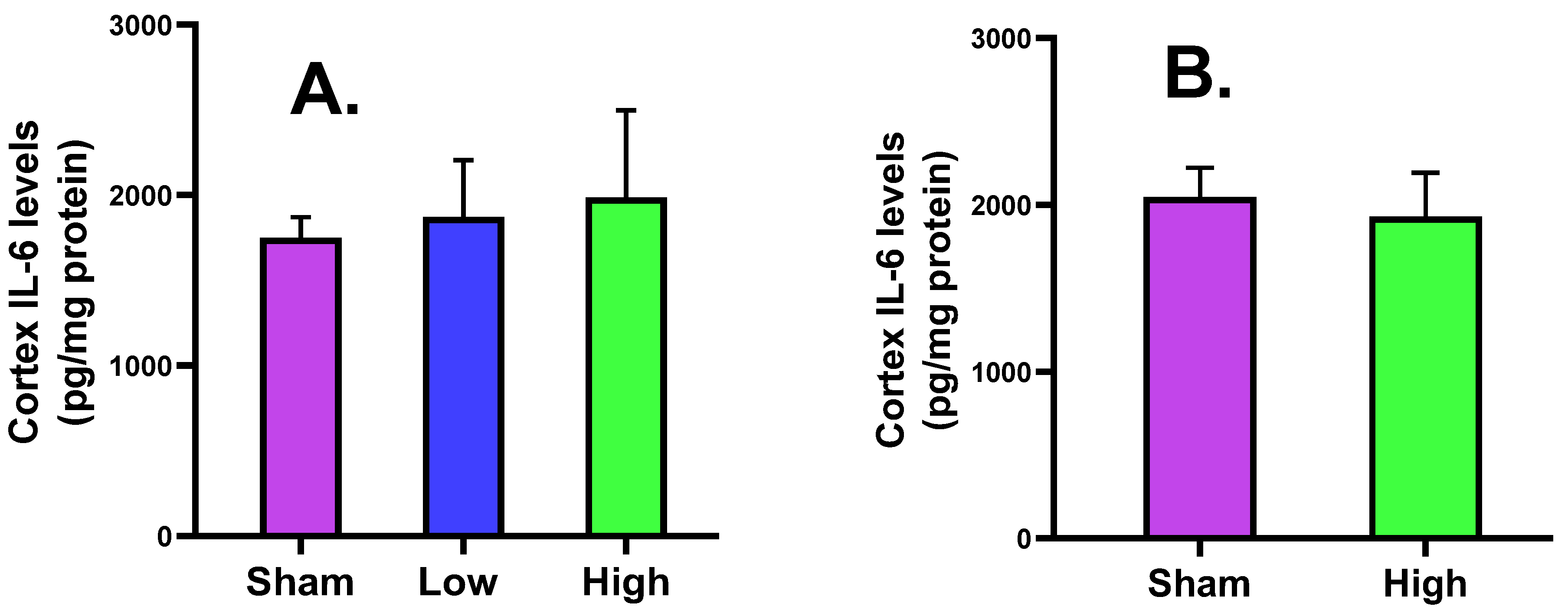
2.2.4. Cortical IL-6 Levels
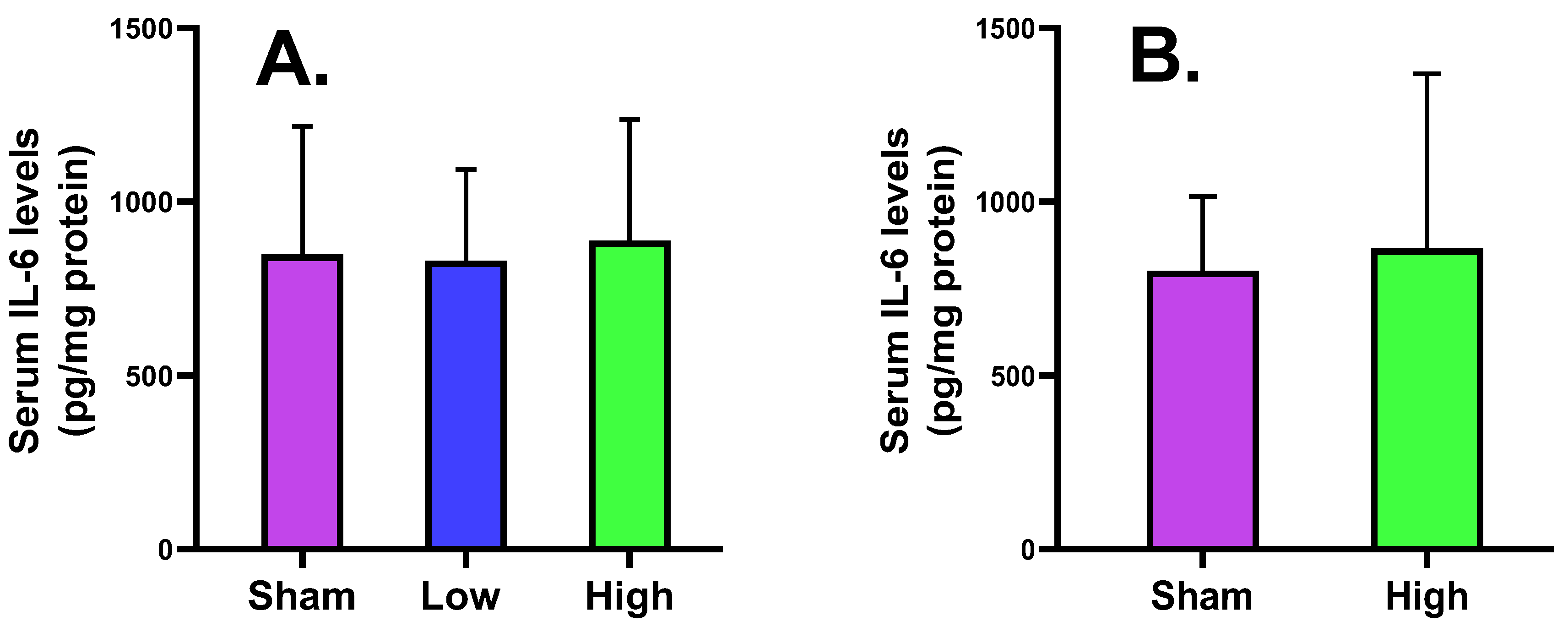
2.2.5. Serum Tissue IL-6 Levels
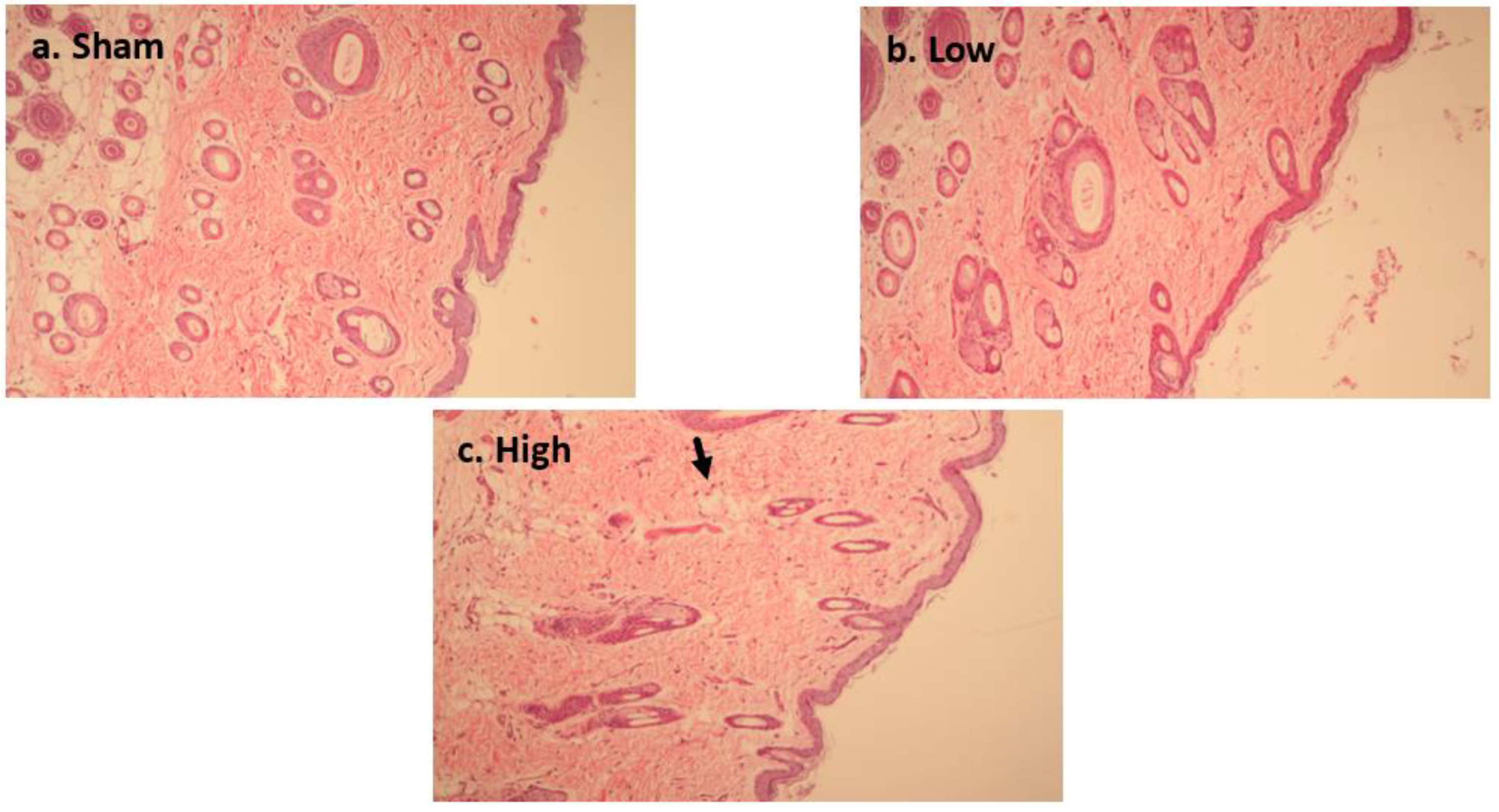
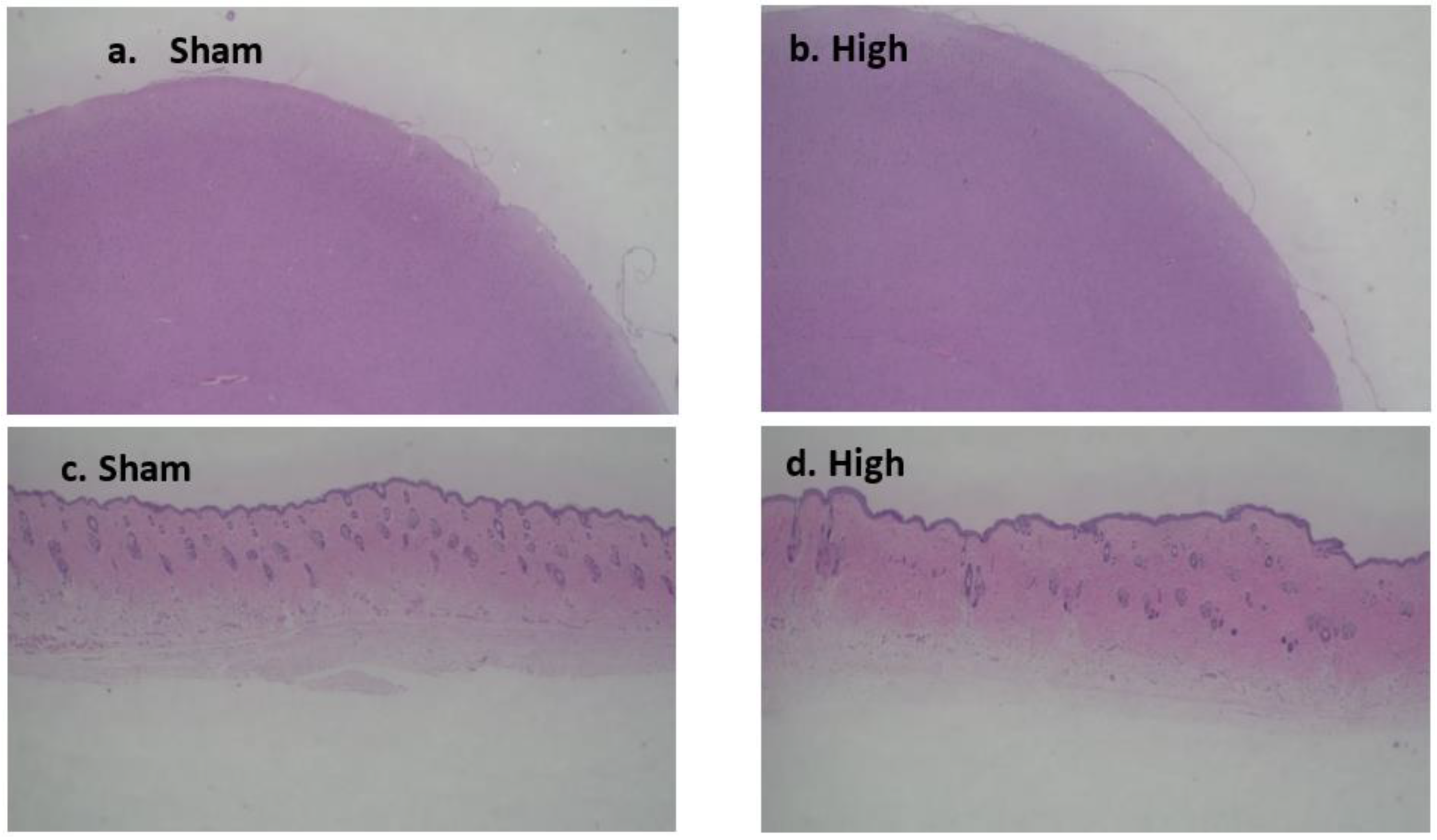
2.3. Effect of tDCS-iTBS on Brain Tissue Morphology (H&E Staining)
2.3.1. Short-Term Stimulation H&E Staining
2.3.2. Long-Term Stimulation Staining
3. Discussion
4. Materials and Methods
4.1. Animal Handling and Tissue Extraction
4.1.1. Selection and Care of Animals
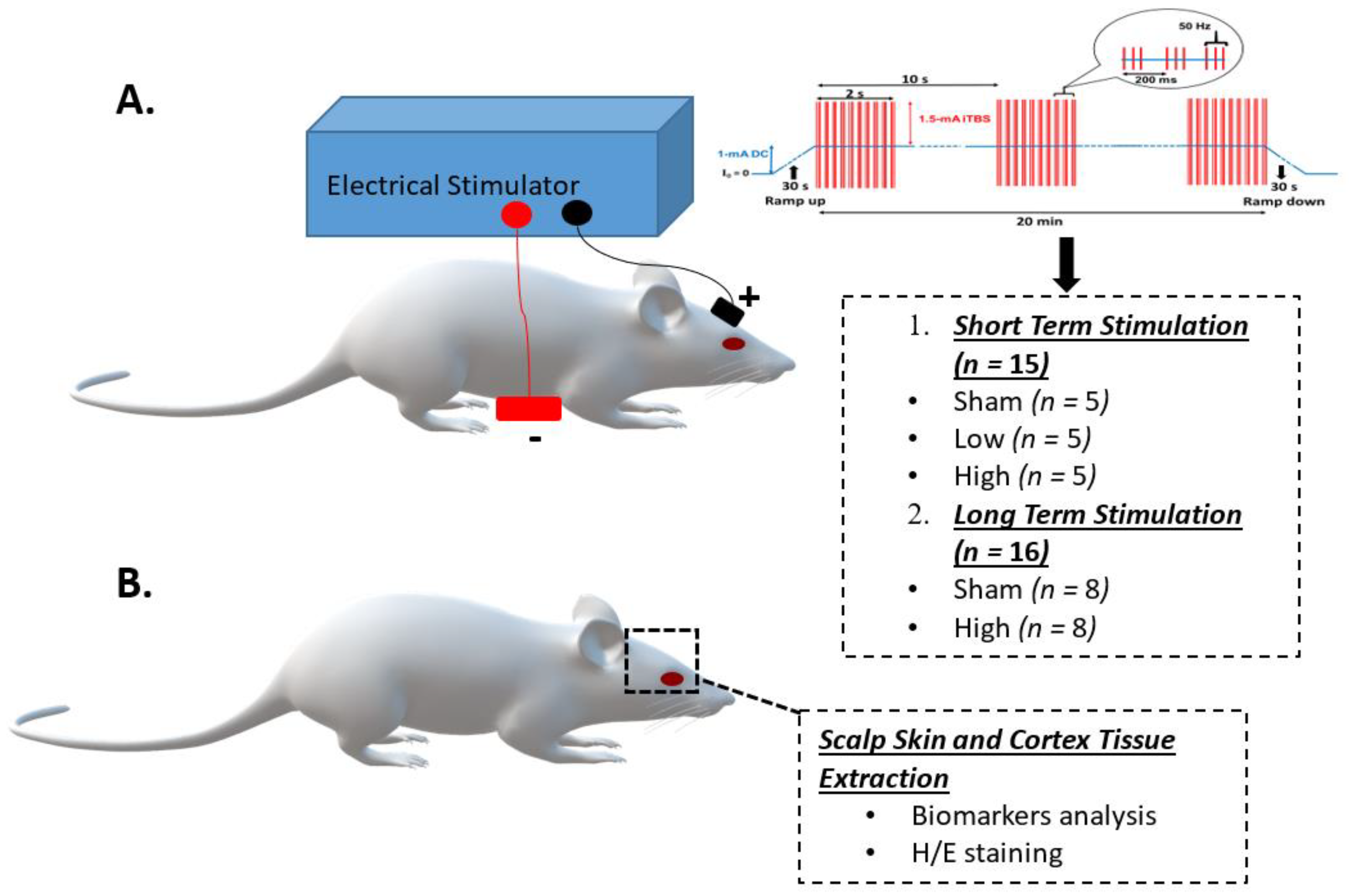
4.1.2. Grouping and Experiment Schedule of Animals
4.1.3. tDCS-iTBS Brain Stimulation Protocol
4.1.4. Sacrifice, Removal of Brain Samples, and Brain and Skin Tissue Collection
4.2. Biochemical Analysis
4.2.1. Evaluation of Caspase-3 Activity
4.2.2. Enzyme-Linked Immunosorbent Assay (ELISA)
4.3. Histological Analysis
4.4. Statistical Analysis
5. Conclusions
Future Research Direction
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. Brain Res. 2000, 527, 633. [Google Scholar] [CrossRef] [PubMed]
- Boroojerdi, B.; Prager, A.; Muellbacher, W.; Cohen, L.G. Reduction of human visual cortex excitability using 1-Hz transcranial magnetic stimulation. Neurology 2000, 54, 1529–1531. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Pascual-Leone, A.; Valls-Solé, J.; Wassermann, E.M.; Hallett, M. Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain 1994, 117, 847–858. [Google Scholar] [CrossRef]
- Cantello, R.; Gianelli, M.; Bettucci, D.; Civardi, C.; De Angelis, M.S.; Mutani, R. Parkinson’s disease rigidity: Magnetic motor evoked potentials in a small hand muscle. Neurology 1991, 41, 1449–1456. [Google Scholar] [CrossRef]
- Li, Y.-T.; Chen, S.-C.; Yang, L.-Y.; Hsieh, T.-H.; Peng, C.-W. Designing and implementing a novel transcranial electrostimulation system for neuroplastic applications: A preliminary study. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 805–813. [Google Scholar] [CrossRef]
- Di Lazzaro, V.; Pilato, F.; Dileone, M.; Profice, P.; Oliviero, A.; Mazzone, P.; Insola, A.; Ranieri, F.; Meglio, M.; Tonali, P.A.; et al. The physiological basis of the effects of intermittent theta burst stimulation of the human motor cortex. J. Physiol. 2008, 586, 3871–3879. [Google Scholar] [CrossRef]
- Huang, Y.-Z.; Edwards, M.J.; Rounis, E.; Bhatia, K.P.; Rothwell, J.C. Theta burst stimulation of the human motor cortex. Neuron 2005, 45, 201–206. [Google Scholar] [CrossRef] [Green Version]
- Woods, A.J.; Antal, A.; Bikson, M.; Boggio, P.S.; Brunoni, A.R.; Celnik, P.; Cohen, L.G.; Fregni, F.; Herrmann, C.S.; Kappenman, E.S. A technical guide to tDCS, and related non-invasive brain stimulation tools. Clin. Neurophysiol. 2016, 127, 1031–1048. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Nitsche, M.A.; Bolognini, N.; Bikson, M.; Wagner, T.; Merabet, L.; Edwards, D.J.; Valero-Cabre, A.; Rotenberg, A.; Pascual-Leone, A. Clinical research with transcranial direct current stimulation (tDCS): Challenges and future directions. Brain Stimul. 2012, 5, 175–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitsche, M.A.; Cohen, L.G.; Wassermann, E.M.; Priori, A.; Lang, N.; Antal, A.; Paulus, W.; Hummel, F.; Boggio, P.S.; Fregni, F. Transcranial direct current stimulation: State of the art 2008. Brain Stimul. 2008, 1, 206–223. [Google Scholar] [CrossRef] [PubMed]
- Lisman, J.E.; Idiart, M.A. Storage of 7 +/- 2 short-term memories in oscillatory subcycles. Science 1995, 267, 1512–1515. [Google Scholar] [CrossRef] [PubMed]
- Di Lazzaro, V.; Pilato, F.; Saturno, E.; Oliviero, A.; Dileone, M.; Mazzone, P.; Insola, A.; Tonali, P.A.; Ranieri, F.; Huang, Y.Z.; et al. Theta-burst repetitive transcranial magnetic stimulation suppresses specific excitatory circuits in the human motor cortex. J. Physiol. 2005, 565, 945–950. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Nitsche, M.S.; Klein, C.C.; Tergau, F.; Rothwell, J.C.; Paulus, W. Level of action of cathodal DC polarisation induced inhibition of the human motor cortex. Clin. Neurophysiol. 2003, 114, 600–604. [Google Scholar] [CrossRef]
- Stagg, C.J.; Nitsche, M.A. Physiological basis of transcranial direct current stimulation. Neurosci. A Rev. J. Bringing Neurobiol. Neurol. Psychiatry 2011, 17, 37–53. [Google Scholar] [CrossRef]
- Bakker, N.; Shahab, S.; Giacobbe, P.; Blumberger, D.M.; Daskalakis, Z.J.; Kennedy, S.H.; Downar, J. rTMS of the dorsomedial prefrontal cortex for major depression: Safety, tolerability, effectiveness, and outcome predictors for 10 Hz versus intermittent theta-burst stimulation. Brain Stimul. 2015, 8, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Mayberg, H.S.; Brannan, S.K.; Tekell, J.L.; Silva, J.A.; Mahurin, R.K.; McGinnis, S.; Jerabek, P.A. Regional metabolic effects of fluoxetine in major depression: Serial changes and relationship to clinical response. Biol. Psychiatry 2000, 48, 830–843. [Google Scholar] [CrossRef]
- Duman, R.S.; Monteggia, L.M. A neurotrophic model for stress-related mood disorders. Biol. Psychiatry 2006, 59, 1116–1127. [Google Scholar] [CrossRef]
- Rohan, J.G.; Carhuatanta, K.A.; McInturf, S.M.; Miklasevich, M.K.; Jankord, R. Modulating hippocampal plasticity with in vivo brain stimulation. J. Neurosci. 2015, 35, 12824–12832. [Google Scholar] [CrossRef] [Green Version]
- Rahman, A.; Reato, D.; Arlotti, M.; Gasca, F.; Datta, A.; Parra, L.C.; Bikson, M. Cellular effects of acute direct current stimulation: Somatic and synaptic terminal effects. J. Physiol. 2013, 591, 2563–2578. [Google Scholar] [CrossRef] [PubMed]
- Márquez-Ruiz, J.; Leal-Campanario, R.; Sánchez-Campusano, R.; Molaee-Ardekani, B.; Wendling, F.; Miranda, P.C.; Ruffini, G.; Gruart, A.; Delgado-García, J.M. Transcranial direct-current stimulation modulates synaptic mechanisms involved in associative learning in behaving rabbits. Proc. Natl. Acad. Sci. USA 2012, 109, 6710–6715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Datta, A.; Bansal, V.; Diaz, J.; Patel, J.; Reato, D.; Bikson, M. Gyri-precise head model of transcranial direct current stimulation: Improved spatial focality using a ring electrode versus conventional rectangular pad. Brain Stim. 2009, 2, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kronberg, G.; Bridi, M.; Abel, T.; Bikson, M.; Parra, L.C. Direct current stimulation modulates LTP and LTD: Activity dependence and dendritic effects. Brain Stim. 2017, 10, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loo, C.K.; Alonzo, A.; Martin, D.; Mitchell, P.B.; Galvez, V.; Sachdev, P. Transcranial direct current stimulation for depression: 3-week, randomised, sham-controlled trial. Br. J. Psychiatry 2012, 200, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunoni, A.; Ferrucci, R.; Bortolomasi, M.; Vergari, M.; Tadini, L.; Boggio, P.; Giacopuzzi, M.; Barbieri, S.; Priori, A. Transcranial direct current stimulation (tDCS) in unipolar vs. bipolar depressive disorder. Prog. Neuro-Psychopharmacol. Biol. Psych. 2011, 35, 96–101. [Google Scholar] [CrossRef]
- Edwards, D.; Krebs, H.; Rykman, A.; Zipse, J.; Thickbroom, G.; Mastaglia, F.; Pascual-Leone, A.; Volpe, B.T. Raised corticomotor excitability of M1 forearm area following anodal tDCS is sustained during robotic wrist therapy in chronic stroke. Restor. Neurol. Neurosci. 2009, 27, 199–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galletta, E.E.; Cancelli, A.; Cottone, C.; Simonelli, I.; Tecchio, F.; Bikson, M.; Marangolo, P. Use of computational modeling to inform tDCS electrode montages for the promotion of language recovery in post-stroke aphasia. Brain Stim. 2015, 8, 1108–1115. [Google Scholar] [CrossRef]
- Fridriksson, J.; Richardson, J.D.; Baker, J.M.; Rorden, C. Transcranial direct current stimulation improves naming reaction time in fluent aphasia: A double-blind, sham-controlled study. Stroke 2011, 42, 819–821. [Google Scholar] [CrossRef] [Green Version]
- Baker, J.M.; Rorden, C.; Fridriksson, J. Using transcranial direct-current stimulation to treat stroke patients with aphasia. Stroke 2010, 41, 1229–1236. [Google Scholar] [CrossRef] [Green Version]
- Castillo-Saavedra, L.; Gebodh, N.; Bikson, M.; Diaz-Cruz, C.; Brandao, R.; Coutinho, L.; Truong, D.; Datta, A.; Shani-Hershkovich, R.; Weiss, M.; et al. Clinically effective treatment of fibromyalgia pain with high-definition transcranial direct current stimulation: Phase II open-label dose optimization. J. Pain 2016, 17, 14–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DaSilva, A.F.; Mendonca, M.E.; Zaghi, S.; Lopes, M.; Dossantos, M.F.; Spierings, E.L.; Bajwa, Z.; Datta, A.; Bikson, M.; Fregni, F. tDCS-induced analgesia and electrical fields in pain-related neural networks in chronic migraine. Headache J. Head Face Pain 2012, 52, 1283–1295. [Google Scholar] [CrossRef] [PubMed]
- Fregni, F.; Boggio, P.S.; Lima, M.C.; Ferreira, M.J.; Wagner, T.; Rigonatti, S.P.; Castro, A.W.; Souza, D.R.; Riberto, M.; Freedman, S.D.; et al. A sham-controlled, phase II trial of transcranial direct current stimulation for the treatment of central pain in traumatic spinal cord injury. Pain 2006, 122, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Vanderhasselt, M.-A. Working memory improvement with non-invasive brain stimulation of the dorsolateral prefrontal cortex: A systematic review and meta-analysis. Brain Cogn. 2014, 86, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palm, U.; Segmiller, F.M.; Epple, A.N.; Freisleder, F.-J.; Koutsouleris, N.; Schulte-Körne, G.; Padberg, F. Transcranial direct current stimulation in children and adolescents: A comprehensive review. J. Neural Trans. 2016, 123, 1219–1234. [Google Scholar] [CrossRef]
- Gbadeyan, O.; Steinhauser, M.; McMahon, K.; Meinzer, M. Safety, tolerability, blinding efficacy and behavioural effects of a novel MRI-compatible, high-definition tDCS set-up. Brain Stim. 2016, 9, 545–552. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Vascular safety of brain plasticity induction via transcranial direct currents. Neurology 2015, 84, 556–557. [Google Scholar] [CrossRef] [Green Version]
- Kasschau, M.; Sherman, K.; Haider, L.; Frontario, A.; Shaw, M.; Datta, A.; Bikson, M.; Charvet, L. A protocol for the use of remotely-supervised transcranial direct current stimulation (tDCS) in multiple sclerosis (MS). J. Vis. Exp. JoVE 2015, 106, e53542. [Google Scholar] [CrossRef] [Green Version]
- Bikson, M.; Datta, A.; Elwassif, M. Establishing safety limits for transcranial direct current stimulation. Clin. Neurophysiol. 2009, 120, 1033. [Google Scholar] [CrossRef] [Green Version]
- Jackson, M.P.; Rahman, A.; Lafon, B.; Kronberg, G.; Ling, D.; Parra, L.C.; Bikson, M. Animal models of transcranial direct current stimulation: Methods and mechanisms. Clin. Neurophysiol. 2016, 127, 3425–3454. [Google Scholar] [CrossRef] [Green Version]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of transcranial direct current stimulation: Evidence based update 2016. Brain Stim. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterchev, A.V.; Wagner, T.A.; Miranda, P.C.; Nitsche, M.A.; Paulus, W.; Lisanby, S.H.; Pascual-Leone, A.; Bikson, M. Fundamentals of transcranial electric and magnetic stimulation dose: Definition, selection, and reporting practices. Brain Stim. 2012, 5, 435–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koc, G.; Gokcil, Z.; Bek, S.; Kasikci, T.; Eroglu, E.; Odabasi, Z. Effects of continuous theta burst transcranial magnetic stimulation on cortical excitability in patients with idiopathic generalized epilepsy. Epilepsy 2017, 77, 26–29. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Shin, J.C.; Jung, S.; Jung, T.-M.; Kim, D.Y. Effects of intermittent theta burst stimulation on spasticity after stroke. Neuroreport 2015, 26, 561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.-C.; Yang, L.-Y.; Adeel, M.; Lai, C.-H.; Peng, C.-W. Transcranial electrostimulation with special waveforms enhances upper-limb motor function in patients with chronic stroke: A pilot randomized controlled trial. J. NeuroEng. Rehab. 2021, 18, 106. [Google Scholar] [CrossRef]
- Rueger, M.A.; Keuters, M.H.; Walberer, M.; Braun, R.; Klein, R.; Sparing, R.; Fink, G.R.; Graf, R.; Schroeter, M. Multi-session transcranial direct current stimulation (tDCS) elicits inflammatory and regenerative processes in the rat brain. PLoS ONE 2012, e43776. [Google Scholar] [CrossRef] [Green Version]
- Gellner, A.-K.; Reis, J.; Fritsch, B. Glia: A neglected player in non-invasive direct current brain stimulation. Front. Cell. Neurosci. 2016, 10, 188. [Google Scholar] [CrossRef]
- Jackson, M.P.; Truong, D.; Brownlow, M.L.; Wagner, J.A.; McKinley, R.A.; Bikson, M.; Jankord, R. Safety parameter considerations of anodal transcranial direct current stimulation in rats. Brain Behav. Immun. 2017, 64, 152–161. [Google Scholar] [CrossRef]
- Liebetanz, D.; Koch, R.; Mayenfels, S.; König, F.; Paulus, W.; Nitsche, M.A. Safety limits of cathodal transcranial direct current stimulation in rats. Clin. Neurophysiol. 2009, 120, 1161–1167. [Google Scholar] [CrossRef]
- Iyer, M.; Mattu, U.; Grafman, J.; Lomarev, M.; Sato, S.; Wassermann, E. Safety and cognitive effect of frontal DC brain polarization in healthy individuals. Neurology 2005, 64, 872–875. [Google Scholar] [CrossRef]
- Nitsche, M.; Niehaus, L.; Hoffmann, K.; Hengst, S.; Liebetanz, D.; Paulus, W.; Meyer, B.-U. MRI study of human brain exposed to weak direct current stimulation of the frontal cortex. Clin. Neurophysiol. 2004, 115, 2419–2423. [Google Scholar] [CrossRef] [PubMed]
- Praveen Rajneesh, C.; Hsieh, T.-H.; Chen, S.-C.; Lai, C.-H.; Yang, L.-Y.; Chin, H.-Y.; Peng, C.W. Deep brain stimulation of the pedunculopontine tegmental nucleus renders neuroprotection through the suppression of hippocampal apoptosis: An experimental animal study. Brain Sci. 2020, 10, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mix, A.; Benali, A.; Eysel, U.T.; Funke, K. Continuous and intermittent transcranial magnetic theta burst stimulation modify tactile learning performance and cortical protein expression in the rat differently. Eur. J. Neurosci. 2010, 32, 1575–1586. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.-Y.; Rui, G.; Zhang, J.-P.; Guo, L.; An, G.-Z.; Lin, J.-J.; He, W.; Ding, G.-R. Cathodal tDCS exerts neuroprotective effect in rat brain after acute ischemic stroke. BMC Neurosci. 2020, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fertonani, A.; Ferrari, C.; Miniussi, C. What do you feel if I apply transcranial electric stimulation? Safety, sensations and secondary induced effects. Clin. Neurophysiol. 2015, 126, 2181–2188. [Google Scholar] [CrossRef] [PubMed]
- Poreisz, C.; Boros, K.; Antal, A.; Paulus, W. Safety aspects of transcranial direct current stimulation concerning healthy subjects and patients. Brain Res. Bull. 2007, 72, 208–214. [Google Scholar] [CrossRef]
- Durand, S.; Fromy, B.; Bouyé, P.; Saumet, J.; Abraham, P. Vasodilatation in response to repeated anodal current application in the human skin relies on aspirin-sensitive mechanisms. J. Physiol. 2002, 540, 261–269. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef]
- Palm, U.; Keeser, D.; Schiller, C.; Fintescu, Z.; Nitsche, M.; Reisinger, E.; Padberg, F.; Nitsche, M. Skin lesions after treatment with transcranial direct current stimulation (tDCS). Brain Stimul. 2008, 1, 386–387. [Google Scholar] [CrossRef]
- Voss, U.; Holzmann, R.; Hobson, A.; Paulus, W.; Koppehele-Gossel, J.; Klimke, A.; Nitsche, M.A. Induction of self awareness in dreams through frontal low current stimulation of gamma activity. Nature Neurosci. 2014, 17, 810–812. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Jakoubkova, M.; Thirugnanasambandam, N.; Schmalfuss, L.; Hullemann, S.; Sonka, K.; Paulus, W.; Trenkwalder, C.; Happe, S. Contribution of the premotor cortex to consolidation of motor sequence learning in humans during sleep. J. Neurophysiol. 2010, 104, 2603–2614. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, T.-H.; Huang, Y.-Z.; Chen, J.-J.J.; Rotenberg, A.; Chiang, Y.-H.; Chien, W.-S.C.; Chang, H.-S.; Wang, J.-Y.; Peng, C.-W. Novel use of theta burst cortical electrical stimulation for modulating motor plasticity in rats. J. Med. Biol. Eng. 2015, 35, 62–68. [Google Scholar] [CrossRef]
- Fonoff, E.T.; Pereira, J.F., Jr.; Camargo, L.V.; Dale, C.S.; Pagano, R.L.; Ballester, G.; Teixeira, M.J. Functional mapping of the motor cortex of the rat using transdural electrical stimulation. Behav. Brain Res. 2009, 202, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Gamboa, O.L.; Antal, A.; Laczo, B.; Moliadze, V.; Nitsche, M.A.; Paulus, W. Impact of repetitive theta burst stimulation on motor cortex excitability. Brain Stimul. 2011, 4, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Cenedella, R.; Galli, C.; Paoletti, R. Brain free fatty acid levels in rats sacrificed by decapitation versus focused microwave irradiation. Lipids 1975, 10, 290–293. [Google Scholar] [CrossRef] [PubMed]
- Oehmichen, M.; Auer, R.N.; König, H.G. Electrical trauma. In Forensic Neuropathology and Associated Neurology; Springer: Berlin/Heidelberg, Germany, 2006. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subgroups | Sham | Low | High | |||||
|---|---|---|---|---|---|---|---|---|
| Parameters | Mean ± SD | Min–Max | Mean ± SD | Min–Max | Mean ± SD | Min–Max | ||
| Groups | Short-term stimulation (n = 15) | Caspase-3 (units) | 0.39 ± 0.10 | 0.24–0.50 | 0.47 ± 0.11 | 0.34–0.56 | 0.48 ± 0.08 | 0.34–0.56 |
| Cortical MBP (ng/mg) | 2.57 ± 0.57 | 2.10–3.55 | 2.62 ± 0.44 | 2.10–3.30 | 2.71 ± 0.27 | 2.51–3.18 | ||
| Serum MBP (ng/mL) | 0.01 ± 0.02 | 0.00–0.05 | 0.02 ± 0.02 | 0.01–0.05 | 0.01 ± 0.02 | 0.00–0.05 | ||
| Cortical NSE (ng/mg) | 5.96 ± 0.69 | 4.81–6.60 | 5.86 ± 1.16 | 3.93–6.80 | 6.26 ± 0.80 | 5.48–7.58 | ||
| Cortical IL-6 (pg/mg) | 1748.81 ± 122.30 | 1577.53–1902.30 | 1871.44 ± 332.47 | 1435.70–2300.69 | 1985.92 ± 511.68 | 1275.53–2542.05 | ||
| Serum IL-6 (pg/mg) | 848.71 ± 368.95 | 492.57–1436.97 | 830.49 ± 263.27 | 535.99–1200.00 | 888.29 ± 347.84 | 283.70–1138.80 | ||
| Long-term stimulation (n = 16) | Caspase-3 (units) | 0.47 ± 0.14 | 0.24–0.72 | -- | -- | 0.51 ± 0.21 | 0.23–0.87 | |
| Cortical MBP (ng/mg) | 2.71 ± 0.27 | 2.34–3.10 | -- | -- | 2.87 ± 0.25 | 2.50–3.20 | ||
| Serum MBP (ng/mL) | 0.03 ± 0.01 | 0.01–0.04 | -- | -- | 0.02 ± 0.01 | 0.01–0.04 | ||
| Cortical NSE (ng/mg) | 6.48 ± 0.72 | 5.40–7.30 | -- | -- | 6.33 ± 1.21 | 3.90–7.70 | ||
| Cortical IL-6 (pg/mg) | 2046.38 ± 175.93 | 1833.00–2432.00 | -- | -- | 1930.00 ± 263.71 | 1576.00–2455.00 | ||
| Serum IL-6 (pg/mg) | 801.63 ± 213.89 | 490.00–1200.00 | -- | -- | 865.75 ± 502.56 | 145.00–1600.00 | ||
| Parameters | Short-Term Stimulation (n = 15) | Long-Term Stimulation (n = 16) | ||||
|---|---|---|---|---|---|---|
| Sham | Low | High | Sham | High | ||
| Current (mA) | 0 | 2.5 | 4.5 | 0 | 4.5 | |
| Current density (mA/cm2) | 0 | 2.5 | 4.5 | 0 | 4.5 | |
| Charge (C) | 0 | 9 | 16.2 | 0 | 8.1 | |
| Charge density (C/m2) | 0 | 90,000 | 162,000 | 0 | 81,000 | |
| Duration | 1 h | 1 h | 1 h | 30 min | 30 min | |
| Number of sessions | 1 session | 1 session | 1 session | 12 sessions | 12 sessions | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adeel, M.; Chen, C.-C.; Lin, B.-S.; Chen, H.-C.; Liou, J.-C.; Li, Y.-T.; Peng, C.-W. Safety of Special Waveform of Transcranial Electrical Stimulation (TES): In Vivo Assessment. Int. J. Mol. Sci. 2022, 23, 6850. https://doi.org/10.3390/ijms23126850
Adeel M, Chen C-C, Lin B-S, Chen H-C, Liou J-C, Li Y-T, Peng C-W. Safety of Special Waveform of Transcranial Electrical Stimulation (TES): In Vivo Assessment. International Journal of Molecular Sciences. 2022; 23(12):6850. https://doi.org/10.3390/ijms23126850
Chicago/Turabian StyleAdeel, Muhammad, Chun-Ching Chen, Bor-Shing Lin, Hung-Chou Chen, Jian-Chiun Liou, Yu-Ting Li, and Chih-Wei Peng. 2022. "Safety of Special Waveform of Transcranial Electrical Stimulation (TES): In Vivo Assessment" International Journal of Molecular Sciences 23, no. 12: 6850. https://doi.org/10.3390/ijms23126850