Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies

 ,
,  ,
,
Abstract
:1. Introduction
2. Epidemiology and Risk Factors for Gastric Carcinoma Development
2.1. Incidence, Mortality and Geographical Variability
2.2. Trends
2.3. Risk Factors
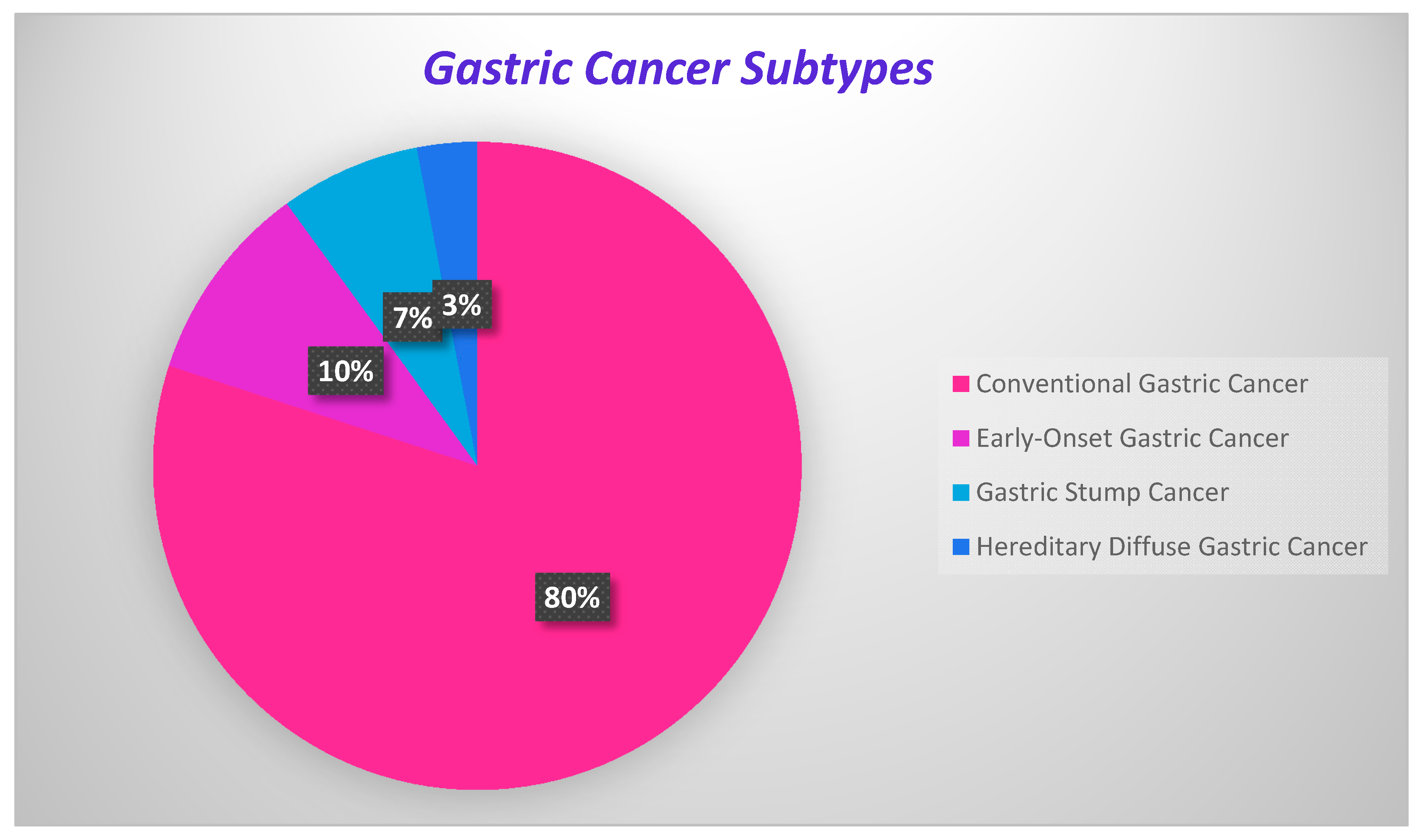
3. Gastric Cancer Classification
3.1. Classification Systems in Gastric Cancer
3.2. Conventional Gastric Cancer
3.3. Early-Onset Gastric Cancer
3.4. Gastric Stump Cancer
3.5. Hereditary Diffuse Gastric Cancer
4. Genomic Characteristics of Gastric Cancer Development
Possible Biomarkers of Gastric Cancer
5. Prevention and Treatment Strategies
5.1. Prevention Strategies for Gastric Cancer
5.2. Improvement in Diet
5.3. Helicobacter pylori Eradication
5.4. Early Detection Importance
5.5. Treatment Strategies for Gastric Cancer: Surgical Resection
5.6. Adjuvant Chemotherapy
5.7. Neo-Adjuvant Chemotherapy
5.8. Targeted Therapy
5.9. Imaging Strategies
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| ASLE | advanced adenocarcinoma of the stomach and lower esophagus |
| CA 15-3 | carbohydrate antigen 15-3 |
| CA 19-9 | carbohydrate antigen 19-9 |
| CA 72-4 | carbohydrate antigen 72-4 |
| CDH1 | cadherin 1 gene |
| CEA | carcinoembryonic antigen |
| EBV | Epstein-Barr virus |
| ECF | epirubicin, cisplatin, and infused fluorouracil |
| EOGC | early-onset gastric cancer |
| EPIC | early postoperative intraperitoneal chemotherapy |
| ESD | endoscopic submucosal dissection |
| FAMTX | fluorouracil, doxorubicin, and methotrexate |
| FP | 5-fluorouracil and cisplatin |
| GC | gastric cancer |
| GSC | gastric stump cancer |
| H. pylori | Helicobacter pylori |
| HDGC | hereditary diffuse gastric cancer |
| HIIC | hyperthermic intraoperative intraperitoneal chemotherapy |
| HIPEC | hyperthermic intraperitoneal chemotherapy |
| MSI | microsatellite instability |
| PIPAC | pressurized intraperitoneal aerosol chemotherapy |
| PUD | peptic ulcer disease |
References
- Yusefi, A.R.; Lankarani, K.B.; Bastani, P.; Radinmanesh, M.; Kavosi, Z. Risk Factors for Gastric Cancer: A Systematic Review. Asian Pac. J. Cancer Prev. 2018, 19, 591–603. [Google Scholar]
- Zhang, X.-Y.; Zhang, P.-Y. Gastric cancer: Somatic genetics as a guide to therapy. J. Med. Genet. 2016, 54, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.-P.; Xu, W.; Liu, W.T.; Yan, M.; Zhu, Z.-G. Tumor heterogeneity of gastric cancer: From the perspective of tumor-initiating cell. World J. Gastroenterol. 2018, 24, 2567–2581. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Von Karsa, L.; Herrero, R. Prevention Strategies for Gastric Cancer: A Global Perspective. Clin. Endosc. 2014, 47, 478–489. [Google Scholar] [CrossRef] [PubMed]
- Kong, X.; Wang, J.-L.; Chen, H.-M.; Fang, J.-Y. Comparison of the clinicopathological characteristics of young and Elderly patients with gastric carcinoma: A meta analysis. J. Surg. Oncol. 2012, 106, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Kunisaki, C.; Akiyama, H.; Nomura, M.; Matsuda, G.; Otsuka, Y.; Ono, H.A.; Takagawa, R.; Nagahori, Y.; Takahashi, M.; Kito, F.; et al. Clinicopathological Features of Gastric Carcinoma in Younger and Middle-Aged Patients: A Comparative Study. J. Gastrointest. Surg. 2006, 10, 1023–1032. [Google Scholar] [CrossRef]
- Llanos, O.; Butte, J.M.; Crovari, F.; Duarte, I.; Guzmán, S. Survival of Young Patients after Gastrectomy for Gastric Cancer. World J. Surg. 2005, 30, 17–20. [Google Scholar] [CrossRef]
- Takatsu, Y.; Hiki, N.; Nunobe, S.; Ohashi, M.; Honda, M.; Yamaguchi, T.; Nakajima, T.; Sano, T. Clinicopathological features of gastric cancer in young patients. Gastric Cancer 2015, 19, 472–478. [Google Scholar] [CrossRef]
- Milne, A.N.; Sitarz, R.; Carvalho, R.; Carneiro, F.; Offerhaus, G.J.A. Early onset gastric cancer: On the road to unraveling gastric carcinogenesis. Curr. Mol. Med. 2007, 7, 15–28. [Google Scholar] [CrossRef]
- Lauren, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Bosman, F.T.; Carneiro, F.; Hruban, R.H.; Theise, N.D. WHO Classification of Tumours of the Digestive System, 4th ed.; IARC: Lyon, France, 2010. [Google Scholar]
- Vogelaar, I.; Van Der Post, R.S.; Van Krieken, J.H.J.; Spruijt, L.; Van Zelst-Stams, W.A.; Kets, C.M.; Lubinski, J.; Jakubowska, A.; Teodorczyk, U.; Aalfs, C.M.; et al. Unraveling genetic predisposition to familial or early onset gastric cancer using germline whole-exome sequencing. Eur. J. Hum. Genet. 2017, 25, 1246–1252. [Google Scholar] [CrossRef] [PubMed]
- Pernot, S.; Voron, T.; Perkins, G.; Lagorce-Pages, C.; Berger, A.; Taieb, J. Signet-ring cell carcinoma of the stomach: Impact on prognosis and specific therapeutic challenge. World J. Gastroenterol. 2015, 21, 11428–11438. [Google Scholar] [CrossRef] [PubMed]
- Milne, A.N.; Offerhaus., G.J.A. Early-onset gastric cancer: Learning lessons from the young. World J. Gastrointest. Oncol. 2010, 2, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Bray, F.; Forman, D.; Mathers, C.; Parkin, N.M.; Shin, H.-R. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef]
- Jemal, A.; Center, M.M.; DeSantis, C.; Ward, E.M. Global Patterns of Cancer Incidence and Mortality Rates and Trends. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1893–1907. [Google Scholar] [CrossRef] [Green Version]
- Ang, T.; Fock, K.M. Clinical epidemiology of gastric cancer. Singap. Med. J. 2014, 55, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, T.; Saika, K. The 5-Year Relative Survival Rate of Stomach Cancer in the USA, Europe and Japan. Jpn. J. Clin. Oncol. 2013, 43, 1157–1158. [Google Scholar] [CrossRef] [Green Version]
- Ferro, A.; Peleteiro, B.; Malvezzi, M.; Bosetti, C.; Bertuccio, P.; Levi, F.; Negri, E.; La Vecchia, C.; Lunet, N. Worldwide trends in gastric cancer mortality (1980–2011), with predictions to 2015, and incidence by subtype. Eur. J. Cancer 2014, 50, 1330–1344. [Google Scholar] [CrossRef] [Green Version]
- Edwards, B.K.; Noone, A.-M.; Mariotto, A.B.; Simard, E.P.; Boscoe, F.P.; Henley, S.J.; Jemal, A.; Cho, H.; Anderson, R.N.; Kohler, B.A.; et al. Annual Report to the Nation on the status of cancer, 1975–2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 2013, 120, 1290–1314. [Google Scholar] [CrossRef]
- Kaneko, S.; Yoshimura, T. Time trend analysis of gastric cancer incidence in Japan by histological types, 1975–1989. Br. J. Cancer 2001, 84, 400–405. [Google Scholar] [CrossRef]
- Sitarz, R.; Skierucha, M.; Mielko, J.; Offerhaus, G.J.A.; Maciejewski, R.; Polkowski, W.P. Gastric cancer: Epidemiology, prevention, classification, and treatment. Cancer Manag. Res. 2018, 10, 239–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yaghoobi, M.; Bijarchi, R.; Narod, S.A. Family history and the risk of gastric cancer. Br. J. Cancer 2009, 102, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Lauwers, G.Y.; Mullen, J.T.; Schreiber, K.E.C.; Chung, D.C. Familial Gastric Cancers. Pathol. Case Rev. 2014, 19, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Boland, C.R.; Yurgelun, M.B. Historical Perspective on Familial Gastric Cancer. Cell. Mol. Gastroenterol. Hepatol. 2017, 3, 192–200. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, H.; Oliveira, C.; Seruca, R.; Carneiro, F. Hereditary diffuse gastric cancer–Pathophysiology and clinical management. Best Pr. Res. Clin. Gastroenterol. 2014, 28, 1055–1068. [Google Scholar] [CrossRef]
- Lim, S.H.; Kwon, J.-W.; Kim, N.; Kim, G.H.; Kang, J.M.; Park, M.J.; Yim, J.Y.; Kim, H.U.; Baik, G.H.; Seo, G.S.; et al. Prevalence and risk factors of Helicobacter pylori infection in Korea: Nationwide multicenter study over 13 years. BMC Gastroenterol. 2013, 13, 104. [Google Scholar] [CrossRef] [Green Version]
- Corso, G.; Marrelli, D. Frequency of Familial Gastric Cancer. In Spotlight on Familial and Hereditary Gastric Cancer; Corso, G., Roviello, F., Eds.; Springer: Dordrecht, The Netherlands, 2013; pp. 11–18. [Google Scholar]
- Kim, J.; Cho, Y.A.; Choi, W.J.; Jeong, S.H. Gene-diet interactions in gastric cancer risk: A systematic review. World J. Gastroenterol. 2014, 20, 9600–9610. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, X. Salt taste preference, sodium intake and gastric cancer in China. Asian Pac. J. Cancer Prev. 2011, 12, 1207–1210. [Google Scholar]
- Keszei, A.P.; Goldbohm, R.A.; Schouten, L.J.; Jakszyn, P.; Brandt, P.A.V.D. Dietary N-nitroso compounds, endogenous nitrosation, and the risk of esophageal and gastric cancer subtypes in the Netherlands Cohort Study. Am. J. Clin. Nutr. 2012, 97, 135–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moy, K.A.; Fan, Y.; Wang, R.; Gao, Y.-T.; Yu, M.C.; Yuan, J.-M. Alcohol and tobacco use in relation to gastric cancer: A prospective study of men in Shanghai, China. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2287–2297. [Google Scholar] [CrossRef] [Green Version]
- Duell, E.J.; Travier, N.; Lujan-Barroso, L.; Clavel-Chapelon, F.; Ruault, B.-; Morois, S.; Palli, D.; Krogh, V.; Panico, S.; Tumino, R.; et al. Alcohol consumption and gastric cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Am. J. Clin. Nutr. 2011, 94, 1266–1275. [Google Scholar] [CrossRef] [PubMed]
- Shin, C.M.; Kim, N.; Cho, S.-I.; Kim, J.S.; Jung, H.C.; Song, I.S. Association between alcohol intake and risk for gastric cancer with regard to ALDH2 genotype in the Korean population. Int. J. Epidemiol. 2011, 40, 1047–1055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishaq, S.; Nunn, L. Helicobacter pylori and gastric cancer: A state of the art review. Gastroenterol. Hepatol. Bed Bench 2015, 8, S6–S14. [Google Scholar] [PubMed]
- Khatoon, J.; Rai, R.P.; Prasad, K.N. Role of Helicobacter pylori in gastric cancer: Updates. World J. Gastrointest. Oncol. 2016, 8, 147–158. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.L.; Yeh, Y.C.; Sheu, B.S. The impacts of H. pylori virulence factors on the development of gastroduodenaldiseases. J. Biomed. Sci. 2018, 25, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roesler, B.M.; Rabelo-Gonçalves, E.M.; Zeitune, J.M. Virulence Factors ofHelicobacter pylori:A Review. Clin. Med. Insights Gastroenterol. 2014, 7, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Baj, J.; Brzozowska, K.; Forma, A.; Maani, A.; Sitarz, E.; Portincasa, P. Immunological Aspects of the Tumor Microenvironment and Epithelial-Mesenchymal Transition in Gastric Carcinogenesis. Int. J. Mol. Sci. 2020, 21, 2544. [Google Scholar] [CrossRef] [Green Version]
- Baj, J.; Korona-Glowniak, I.; Forma, A.; Maani, A.; Sitarz, E.; Rahnama-Hezavah, M.; Radzikowska, E.; Portincasa, P. Mechanisms of the Epithelial–Mesenchymal Transition and Tumor Microenvironment in Helicobacter pylori-Induced Gastric Cancer. Cells 2020, 9, 1055. [Google Scholar] [CrossRef] [Green Version]
- Iizasa, H.; Nanbo, A.; Nishikawa, J.; Jinushi, M.; Yoshiyama, H. Epstein-Barr Virus (EBV)-associated Gastric Carcinoma. Viruses 2012, 4, 3420–3439. [Google Scholar] [CrossRef] [Green Version]
- Fukayama, M.; Hayashi, Y.; Iwasaki, Y.; Chong, J.; Ooba, T.; Takizawa, T.; Koike, M.; Mizutani, S.; Miyaki, M.; Hirai, K. Epstein-Barr virus-associated gastric carcinoma and Epstein-Barr virus infectionof the stomach. Lab Investig. 1994, 71, 73–81. [Google Scholar]
- Camargo, M.C.; Murphy, G.; Koriyama, C.; Pfeiffer, R.M.; Kim, W.H.; Herrera-Goepfert, R.; Corvalán, A.H.; Carrascal, E.; Abdirad, A.; Anwar, M.; et al. Determinants of Epstein-Barr virus-positive gastric cancer: An international pooled analysis. Br. J. Cancer 2011, 105, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Hu, B.; El Hajj, N.; Sittler, S.; Lammert, N.; Barnes, R.; Meloni-Ehrig, A. Gastric cancer: Classification, histology and application of molecular pathology. J. Gastrointest. Oncol. 2012, 3, 251–261. [Google Scholar] [PubMed]
- Fléjou, J.F. WHO Classification of digestive tumors: The fourth edition. Ann. Pathol. 2011, 31, S27–S31. [Google Scholar] [CrossRef] [PubMed]
- Sarbia, M. Pathology of upper gastrointestinal malignancies. Semin. Oncol. 2004, 31, 465–475. [Google Scholar] [CrossRef]
- Werner, M.; Becker, K.; Keller, G.; Höfler, H. Gastric adenocarcinoma: Pathomorphology and molecular pathology. J. Cancer Res. Clin. Oncol. 2001, 127, 207–216. [Google Scholar] [CrossRef]
- Kikuchi, S.; Nakajima, T.; Nishi, T.; Kobayashi, O.; Konishi, T.; Inaba, Y.; Wada, O.; Satou, H.; Ishibashi, T.; Ichikawa, S.; et al. Association between Family History and Gastric Carcinoma among Young Adults. Jpn. J. Cancer Res. 1996, 87, 332–336. [Google Scholar] [CrossRef]
- Forman, D.; Burley, V. Gastric cancer: Global pattern of the disease and an overview of environmental risk factors. Best Pract. Res. Clin. Gastroenterol. 2006, 20, 633–649. [Google Scholar] [CrossRef]
- Correa, P. Human gastric carcinogenesis: A multistep and multifactorial process—First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res. 1992, 52, 6735–6740. [Google Scholar]
- Skierucha, M.; Milne, A.N.; Offerhaus, G.J.A.; Polkowski, W.P.; Maciejewski, R.; Sitarz, R. Molecular alterations in gastric cancer with special reference to the early-onset subtype. World J. Gastroenterol. 2016, 22, 2460–2474. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, R.; Milne, A.N.; Van Rees, B.P.; Caspers, E.; Cirnes, L.; Figueiredo, C.; Offerhaus, G.J.A.; Weterman, M.A. Early-onset gastric carcinomas display molecular characteristics distinct from gastric carcinomas occurring at a later age. J. Pathol. 2004, 204, 75–83. [Google Scholar] [CrossRef]
- Kokkola, A.; Sipponen, P. Gastric carcinoma in young adults. Hepatogastroenterology 2002, 48, 1552–1555. [Google Scholar]
- Milne, A.N.; Carvalho, R.; Morsink, F.M.; Musler, A.R.; De Leng, W.W.; Ristimäki, A.; Offerhaus, G.J.A. Early-onset gastric cancers have a different molecular expression profile than conventional gastric cancers. Mod. Pathol. 2006, 19, 564–572. [Google Scholar] [CrossRef]
- Toftgaard, C. Gastric Cancer after Peptic Ulcer Surgery. Ann. Surg. 1989, 210, 159–164. [Google Scholar] [CrossRef]
- Sinning, C.; Schaefer, N.; Standop, J.; Hirner, A.; Wolff, M. Gastric stump carcinoma—Epidemiology and current concepts in pathogenesisand treatment. Eur. J. Surg. Oncol. 2007, 33, 133–139. [Google Scholar] [CrossRef]
- Viste, A.; Bjørnestad, E.; Opheim, P.; Skarstein, A.; Thunold, J.; Hartveit, F.; Eide, G.E.; Eide, T.J.; Søreide, O. Risk of carcinoma following gastric operations for benign disease. A historical cohort study of 3470 patients. Lancet 1986, 2, 502–505. [Google Scholar] [CrossRef]
- Luo, W.; Fedda, F.; Lynch, P.; Tan, D. CDH1 Gene and Hereditary Diffuse Gastric Cancer Syndrome: Molecular and Histological Alterations and Implications for Diagnosis and Treatment. Front. Pharmacol. 2018, 9, 1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- La Vecchia, C.; Negri, E.; Gentile, A.; Franceschi, S. Family history and the risk of stomach and colorectal cancer. Cancer 1992, 70, 50–55. [Google Scholar] [CrossRef]
- Kaurah, P.; Huntsman, D.G. Hereditary Diffuse Gastric Cancer. In GeneReviews [Internet]; Adam, M.P., Ardinger, H.H., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Stephens, K., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993–2019. [Google Scholar]
- Guilford, P.; Blair, V.; More, H.; Humar, B. A short guide to hereditary diffuse gastric cancer. Hered. Cancer Clin. Pr. 2007, 5, 183–194. [Google Scholar] [CrossRef] [Green Version]
- Hansford, S.; Kaurah, P.; Li-Chang, H.; Woo, M.; Senz, J.; Pinheiro, H.; Schrader, K.A.; Schaeffer, D.F.; Shumansky, K.; Zogopoulos, G.; et al. Hereditary Diffuse Gastric Cancer Syndrome. JAMA Oncol. 2015, 1, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Machlowska, J.; Maciejewski, R.; Sitarz, R. The Pattern of Signatures in Gastric Cancer Prognosis. Int. J. Mol. Sci. 2018, 19, 1658. [Google Scholar] [CrossRef] [Green Version]
- Grávalos, C.; Jimeno, A. HER2 in gastric cancer: A new prognostic factor and a novel therapeutic target. Ann. Oncol. 2008, 19, 1523–1529. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-B.; Liao, X.-F.; Zhang, J. Clinicopathological factors associated with HER2-positive gastric cancer. Medicine 2017, 96, e8437. [Google Scholar] [CrossRef] [PubMed]
- Busuttil, R.A.; Zapparoli, G.V.; Haupt, S.; Fennell, C.; Wong, S.Q.; Pang, J.-M.B.; Takeno, E.A.; Mitchell, C.; Di Costanzo, N.; Fox, S.; et al. Role of p53 in the progression of gastric cancer. Oncotarget 2014, 5, 12016–12026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Xing, X.; Guo, J.; Wen, X.; Ding, G.; Li, B.; Dong, B.; Feng, Q.; Li, S.; Zhang, J.; Cheng, X.; et al. Analysis of PD1, PDL1, PDL2 expression and T cells infiltration in 1014 gastric cancer patients. OncoImmunology 2017, 7, e1356144. [Google Scholar] [CrossRef] [Green Version]
- Pilozzi, E.; Talerico, C.; Platt, A.; Fidler, C.; Ruco, L. P73 gene mutations in gastric adenocarcinomas. Mol. Pathol. 2003, 56, 60–62. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, X.-Y.; Xu, L.; Liu, W.-J.; Zhang, J.; Zhang, J.-P. Expression and significance of p53 and mdm2 in atypical intestinal metaplasia and gastric carcinoma. Oncol. Lett. 2011, 2, 707–712. [Google Scholar] [CrossRef]
- Wu, J.; Liu, X.; Cai, H.; Wang, Y. Prediction of tumor recurrence after curative resection in gastric carcinoma based on bcl-2 expression. World J. Surg. Oncol. 2014, 12, 40. [Google Scholar] [CrossRef] [Green Version]
- Gao, P.; Zhou, G.-Y.; Liu, Y.; Li, J.-S.; Zhen, J.-H.; Yuan, Y.-P. Alteration of cyclin D1 in gastric carcinoma and its clinicopathologic significance. World J. Gastroenterol. 2004, 10, 2936–2939. [Google Scholar] [CrossRef] [Green Version]
- Arici, D.S.; Tuncer, E.; Ozer, H.; Simek, G.; Koyuncu, A. Expression of retinoblastoma and cyclin D1 in gastric carcinoma. Neoplasma 2009, 56, 63–67. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, K.; Metzger, R.; Salonga, D.; Danenberg, K.; Leichman, L.P.; Fink, U.; Sendler, A.; Kelsen, D.; Schwartz, G.K.; Groshen, S.; et al. High frequency of simultaneous loss of p16 and p16β gene expression in squamous cell carcinoma of the esophagus but not in adenocarcinoma of the esophagus or stomach. Oncogene 1997, 15, 1481–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feakins, R.M.; Mulcahy, H.E.; Quaglia, A.; Jawhari, A.; Zhang, Z.; Patchett, S.E. p27(Kip1) loss does not predict survival in patients with advanced gastric carcinoma. Cancer 2000, 89, 1684–1691. [Google Scholar] [CrossRef]
- Boltin, R.; Niv, Y. Mucins in Gastric Cancer—An Update. J. Gastrointest. Dig. Syst. 2013, 3, 15519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.S.; Kim, H.S.; Yang, H.K.; Kim, Y.I.; Kim, W.H. MUC1, MUC2, MUC5AC, and MUC6 expressions in gastric carcinomas: Their roles as prognostic indicators. Cancer 2001, 92, 1427–1434. [Google Scholar] [CrossRef]
- Sandusky, G.E.; Mintze, K.S.; E Pratt, S.; Dantzig, A.H. Expression of multidrug resistance-associated protein 2 (MRP2) in normal human tissues and carcinomas using tissue microarrays. Histopathology 2002, 41, 65–74. [Google Scholar] [CrossRef]
- Qiao, W.; Wang, T.; Zhang, L.; Tang, Q.; Wang, D.; Sun, H. Association between single genetic polymorphisms of MDR1 gene and gastric cancer susceptibility in Chinese. Med. Oncol. 2013, 30, 643. [Google Scholar] [CrossRef]
- Zhu, C.-Y.; Lv, Y.-P.; Yan, D.-F.; Gao, F.-L. Knockdown of MDR1 Increases the Sensitivity to Adriamycin in Drug Resistant Gastric Cancer Cells. Asian Pac. J. Cancer Prev. 2013, 14, 6757–6760. [Google Scholar] [CrossRef] [Green Version]
- Hayes, P.C.; A Bouchier, I.; Beckett, G.J. Glutathione S-transferase in humans in health and disease. Gut 1991, 32, 813–818. [Google Scholar] [CrossRef] [Green Version]
- Yu, P.; Du, Y.; Cheng, X.; Yu, Q.; Huang, L.; Dong, R. Expression of multidrug resistance-associated proteins and their relation to postoperative individualized chemotherapy in gastric cancer. World J. Surg. Oncol. 2014, 12, 307. [Google Scholar] [CrossRef] [Green Version]
- Bass, A.J.; Thorsson, V.; Shmulevich, I.; Reynolds, S.M.; Miller, M.; Bernard, B.; Hinoue, T.; Laird, P.W.; Curtis, C.; Shen, H.; et al. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar]
- Polom, K.; Marrelli, D.; Smyth, E.C.; Voglino, C.; Roviello, G.; Pascale, V.; Varas, J.; Vindigni, C.; Roviello, F. The Role of Microsatellite Instability in Positive Margin Gastric Cancer Patients. Surg. Innov. 2018, 25, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [PubMed]
- Feng, F.; Tian, Y.; Xu, G.; Liu, Z.; Liu, S.; Zheng, G.; Guo, M.; Lian, X.; Fan, D.; Zhang, H. Diagnostic and prognostic value of CEA, CA19–9, AFP and CA125 for early gastric cancer. BMC Cancer 2017, 17, 737. [Google Scholar] [CrossRef] [PubMed]
- Kochi, M.; Fujii, M.; Kanamori, N.; Kaiga, T.; Kawakami, T.; Aizaki, K.; Kasahara, M.; Mochizuki, F.; Kasakura, Y.; Yamagata, M. Evaluation of serum CEA and CA19-9 levels as prognostic factors in patients with gastric cancer. Gastric Cancer 2000, 3, 177–186. [Google Scholar] [CrossRef] [Green Version]
- Sisik, A.; Kaya, M.; Bas, G.; Basak, F.; Alimoglu, O. CEA and CA 19-9 are Still Valuable Markers for the Prognosis of Colorectal and Gastric Cancer Patients. Asian Pac. J. Cancer Prev. 2013, 14, 4289–4294. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.-C.; Zhao, H.-J.; Shen, L.-Z. Preoperative Serum CEA and CA19-9 in Gastric Cancer—A Single Tertiary Hospital Study of 1,075 Cases. Asian Pac. J. Cancer Prev. 2015, 16, 2685–2691. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.; Chen, Q.; Zhao, Q.; Liu, M.; Guo, J. Value of Combined Detection of Serum CEA, CA72-4, CA19-9, CA15-3 and CA12-5 in the Diagnosis of Gastric Cancer. Ann. Clin. Lab. Sci. 2017, 47, 260–263. [Google Scholar]
- Sawayama, H.; Iwatsuki, M.; Kuroda, D.; Toihata, T.; Uchihara, T.; Koga, Y.; Yagi, T.; Kiyozumi, Y.; Eto, T.; Hiyoshi, Y.; et al. The association of the lymph node ratio and serum carbohydrate antigen 19-9 with early recurrence after curative gastrectomy for gastric cancer. Surg. Today 2018, 48, 994–1003. [Google Scholar] [CrossRef]
- Hasbahceci, M.; Malya, F.; Kunduz, E.; Guler, M.; Unver, N.; Akcakaya, A. Use of serum and peritoneal CEA and CA19-9 in prediction of peritoneal dissemination and survival of gastric adenocarcinoma patients: Are they prognostic factors? Ann. R. Coll. Surg. Engl. 2018, 100, 257–266. [Google Scholar] [CrossRef]
- Sun, Z.; Zhang, N.-W. Clinical evaluation of CEA, CA19-9, CA72-4 and CA125 in gastric cancer patients with neoadjuvant chemotherapy. World J. Surg. Oncol. 2014, 12, 397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.-X.; Huang, X.-Z.; Gao, P.; Sun, J.-X.; Chen, X.-W.; Yang, Y.-C.; Zhang, C.; Liu, H.-P.; Wang, H.-C.; Wang, Z. Clinicopathologic and Prognostic Value of Serum Carbohydrate Antigen 19-9 in Gastric Cancer: A Meta-Analysis. Dis. Markers 2015, 2015, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, J.; Zheng, W. An Alternative Method for Screening Gastric Cancer Based on Serum Levels of CEA, CA19-9, and CA72-4. J. Gastrointest. Cancer 2016, 49, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Shen, M.; Wang, H.; Wei, K.; Zhang, J.; You, C. Five common tumor biomarkers and CEA for diagnosing early gastric cancer. Medicine 2018, 97, e0577. [Google Scholar] [CrossRef] [PubMed]
- Elingarami, S.; Liu, M.; Fan, J.; He, N. Applications of nanotechnology in gastric cancer: Detection and prevention by nutrition. J. Nanosci. Nanotechnol. 2014, 14, 932–945. [Google Scholar] [CrossRef]
- González, C.A.; Pera, G.; Agudo, A.; Bueno-De-Mesquita, H.B.; Ceroti, M.; Boeing, H.; Schulz, M.; Del Giudice, G.; Plebani, M.; Carneiro, F.; et al. Fruit and vegetable intake and the risk of stomach and oesophagus adenocarcinoma in the European Prospective Investigation into Cancer and Nutrition (EPIC–EURGAST). Int. J. Cancer 2006, 118, 2559–2566. [Google Scholar]
- International Agency for Research on Cancer. Fruit and vegetables. In IARC Handbooks of Cancer Prevention; IARC: Lyon, France, 2003; Volume 8. [Google Scholar]
- Graham, D.Y.; Shiotani, A. The time to eradicate gastric cancer is now. Gut 2005, 54, 735–738. [Google Scholar] [CrossRef] [Green Version]
- Ford, A.C.; Forman, D.; Hunt, R.H.; Yuan, C.Y.; Moayyedi, P. Helicobacter pylori eradication therapy to prevent gastric cancer in healthy asymptomatic infected individuals: Systematic review and meta-analysis of randomised controlled trials. BMJ 2014, 348, g3174. [Google Scholar] [CrossRef] [Green Version]
- Ma, J.-L.; Zhang, L.; Brown, L.M.; Li, J.-Y.; Shen, L.; Pan, K.-F.; Liu, W.-D.; Hu, Y.; Han, Z.-X.; Crystal-Mansour, S.; et al. Fifteen-year effects of Helicobacter pylori, garlic, and vitamin treatments on gastric cancer incidence and mortality. J. Natl. Cancer Inst. 2012, 104, 488–492. [Google Scholar] [CrossRef]
- Choi, J.; Kim, S.G.; Yoon, H.; Im, J.P.; Kim, J.S.; Kim, W.H.; Jung, H.C. Eradication of Helicobacter pylori After Endoscopic Resection of Gastric Tumors Does Not Reduce Incidence of Metachronous Gastric Carcinoma. Clin. Gastroenterol. Hepatol. 2014, 12, 793–800. [Google Scholar] [CrossRef]
- Fukase, K.; Kato, M.; Kikuchi, S.; Inoue, K.; Uemura, N.; Okamoto, S.; Terao, S.; Amagai, K.; Hayashi, S.; Asaka, M. Effect of eradication of Helicobacter pylori on incidence of metachronous gastric carcinoma after endoscopic resection of early gastric cancer: An open-label, randomised controlled trial. Lancet 2008, 372, 392–397. [Google Scholar] [CrossRef] [Green Version]
- Tsubono, Y.; Hisamichi, S. Screening for gastric cancer in Japan. Gastric Cancer 2000, 3, 9–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, K.S.; Suh, M. Screening for Gastric Cancer: The Usefulness of Endoscopy. Clin. Endosc. 2014, 47, 490–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, P.; Islami, F.; Anandasabapathy, S.; Freedman, N.D.; Kamangar, F. Gastric cancer: Descriptive epidemiology, risk factors, screening, and prevention. Cancer Epidemiol. Biomark. Prev. 2014, 23, 700–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsumoto, S.; Ishikawa, S.; Yoshida, Y. Reduction of gastric cancer mortality by endoscopic and radiographic screening in an isolated island: A retrospective cohort study. Aust. J. Rural. Heal. 2013, 21, 319–324. [Google Scholar] [CrossRef]
- Hamashima, C.; Ogoshi, K.; Okamoto, M.; Shabana, M.; Kishimoto, T.; Fukao, A. A community-based, case-control study evaluating mortality reduction from gastric cancer by endoscopic screening in Japan. PLoS ONE 2013, 8, e79088. [Google Scholar] [CrossRef] [Green Version]
- Swan, R.; Miner, T.J. Current role of surgical therapy in gastric cancer. World J. Gastroenterol. 2006, 12, 372–379. [Google Scholar] [CrossRef]
- Parisi, A.; Reim, D.; Borghi, F.; Nguyen, N.T.; Qi, F.; Coratti, A.; Cianchi, F.; Cesari, M.; Bazzocchi, F.; Alimoglu, O.; et al. Minimally invasive surgery for gastric cancer: A comparison between robotic, laparoscopic and open surgery. World J. Gastroenterol. 2017, 23, 2376–2384. [Google Scholar] [CrossRef]
- Facciorusso, A.; Antonino, M.; Di Maso, M.; Muscatiello, N. Endoscopic submucosal dissection vs endoscopic mucosal resection for earlygastric cancer: A meta-analysis. World J. Gastrointest. Endosc. 2014, 6, 555–563. [Google Scholar] [CrossRef]
- Son, T.; Hyung, W.J. Laparoscopic gastric cancer surgery: Current evidence and future perspectives. World J. Gastroenterol. 2016, 22, 727–735. [Google Scholar] [CrossRef]
- Gholami, S.; Cassidy, M.R.; Strong, V.E. Minimally Invasive Surgical Approaches to Gastric Resection. Surg. Clin. North Am. 2017, 97, 249–264. [Google Scholar] [CrossRef]
- Bobo, Z.; Xin, W.; Jiang, L.; Quan, W.; Liang, B.; Xiangbing, D.; Ziqiang, W. Robotic gastrectomy versus laparoscopic gastrectomy for gastric cancer: Meta-analysis and trial sequential analysis of prospective observational studies. Surg. Endosc. 2019, 33, 1033–1048. [Google Scholar] [CrossRef] [PubMed]
- Van Boxel, G.I.; Ruurda, J.P.; Van Hillegersberg, R. Robotic-assisted gastrectomy for gastric cancer: A European perspective. Gastric Cancer 2019, 22, 909–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinami, S.; Nakamura, N.; Tomita, Y.; Miyata, T.; Fujita, H.; Ueda, N.; Kosaka, T. Precision surgical approach with lymph-node dissection in early gastric cancer. World J. Gastroenterol. 2019, 25, 1640–1652. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Yamaguchi, K.; Okumura, N.; Tanahashi, T.; Kodera, Y. Is conversion therapy possible in stage IV gastric cancer: The proposal of new biological categories of classification. Gastric Cancer 2015, 19, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Santoro, R.; Ettorre, G.M.; Santoro, E. Subtotal gastrectomy for gastric cancer. World J. Gastroenterol. 2014, 20, 13667–13680. [Google Scholar] [CrossRef]
- Dixon, W.J.; Longmire, W.P.; Holden, W.D. Use of triethylenethiophosphoramide as an adjuvant to the surgical treatment of gastric and colorectal carcinoma: Ten-year follow-up. Ann. Surg. 1971, 173, 26–39. [Google Scholar] [CrossRef]
- Lise, M.; Nitti, D.; Marchet, A.; Sahmoud, T.; Buyse, M.; Duez, N.; Fiorentino, M.; Dos Santos, J.G.; Labianca, R.; Rougier, P. Final results of a phase III clinical trial of adjuvant chemotherapy with the modified fluorouracil, doxorubicin, and mitomycin regimen in resectable gastric cancer. J. Clin. Oncol. 1995, 13, 2757–2763. [Google Scholar] [CrossRef]
- Coombes, R.C.; Schein, P.S.; Chilvers, C.E.; Wils, J.; Beretta, G.; Bliss, J.M.; Rutten, A.; Amadori, D.; Cortes-Funes, H.; Villar-Grimalt, A. A randomized trial comparing adjuvant fluorouracil, doxorubicin, and mitomycin with no treatment in operable gastric cancer. International Collaborative Cancer Group. J. Clin. Oncol. 1990, 8, 1362–1369. [Google Scholar] [CrossRef]
- Nakajima, T.; Nashimoto, A.; Kitamura, M.; Kito, T.; Iwanaga, T.; Okabayashi, K.; Sasaki, M.; Goto, M. Adjuvant mitomycin and fluorouracil followed by oral uracil plus tegafur in serosa-negative gastric cancer: A randomised trial. Lancet 1999, 354, 273–277. [Google Scholar] [CrossRef]
- Paoletti, X.; Oba, K.; Burzykowski, T.; Michiels, S.; Ohashi, Y.; Pignon, J.-P.; Rougier, P.; Sakamoto, J.; Sargent, D.; Sasako, M.; et al. Benefit of Adjuvant Chemotherapy for Resectable Gastric Cancer. JAMA 2010, 303, 1729. [Google Scholar]
- Sakuramoto, S.; Sasako, M.; Yamaguchi, T.; Kinoshita, T.; Fujii, M.; Nashimoto, A.; Furukawa, H.; Nakajima, T.; Ohashi, Y.; Imamura, H.; et al. Adjuvant Chemotherapy for Gastric Cancer with S-1, an Oral Fluoropyrimidine. N. Engl. J. Med. 2007, 357, 1810–1820. [Google Scholar] [CrossRef] [PubMed]
- Van den Ende, T.; ter Veer, E.; Machiels, M.; Mali, R.; Nijenhuis, F.A.; de Waal, L.; Laarman, M.; Gisbertz, S.S.; Hulshof, M.C.C.M.; van Oijen, M.G.H.; et al. The Efficacy and Safety of (Neo)Adjuvant Therapy for Gastric Cancer: A Network Meta-analysis. Cancers 2019, 11, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noh, S.H.; Park, S.R.; Yang, H.-K.; Chung, H.C.; Chung, I.-J.; Kim, S.-W.; Kim, H.-H.; Choi, J.-H.; Kim, H.-K.; Yu, W.; et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1389–1396. [Google Scholar] [CrossRef]
- Sasako, M.; Sakuramoto, S.; Katai, H.; Kinoshita, T.; Furukawa, H.; Yamaguchi, T.; Nashimoto, A.; Fujii, M.; Nakajima, T.; Ohashi, Y. Five-Year Outcomes of a Randomized Phase III Trial Comparing Adjuvant Chemotherapy With S-1 Versus Surgery Alone in Stage II or III Gastric Cancer. J. Clin. Oncol. 2011, 29, 4387–4393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bang, Y.-J.; Van Cutsem, E.; Fuchs, C.S.; Ohtsu, A.; Tabernero, J.; Ilson, D.H.; Hyung, W.J.; Strong, V.E.; Goetze, T.O.; Yoshikawa, T.; et al. KEYNOTE-585: Phase III study of perioperative chemotherapy with or without pembrolizumab for gastric cancer. Future Oncol. 2019, 15, 943–952. [Google Scholar] [CrossRef]
- Yan, T.D.; Black, D.; Sugarbaker, P.H.; Zhu, J.; Yonemura, Y.; Petrou, G.; Morris, D.L. A Systematic Review and Meta-analysis of the Randomized Controlled Trials on Adjuvant Intraperitoneal Chemotherapy for Resectable Gastric Cancer. Ann. Surg. Oncol. 2007, 14, 2702–2713. [Google Scholar] [CrossRef]
- Ajani, J.A.; Bentrem, D.J.; Besh, S.; D’Amico, T.A.; Das, P.; Denlinger, C.; Fakih, M.G.; Fuchs, C.S.; Gerdes, H.; Glasgow, R.E.; et al. National Comprehensive Cancer Network. Gastric cancer, version 2.2013: Featured updates to the NCCN Guidelines. JNCCN 2013, 11, 531–546. [Google Scholar]
- Okines, A.; Verheij, M.; Allum, W.; Cunningham, D.; Cervantes, A. On behalf of the ESMO Guidelines Working Group Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, v50–v54. [Google Scholar] [CrossRef]
- Das, M. Neoadjuvant chemotherapy: Survival benefit in gastric cancer. Lancet Oncol. 2017, 18, e307. [Google Scholar] [CrossRef]
- Hartgrink, H.; Van De Velde, C.; Putter, H.; Songun, I.; Tesselaar, M.; Kranenbarg, E.M.-K.; De Vries, J.; Wils, J.; Van Der Bijl, J.; Van Krieken, J. Neo-adjuvant chemotherapy for operable gastric cancer: Long term results of the Dutch randomised FAMTX trial. Eur. J. Surg. Oncol. (EJSO) 2004, 30, 643–649. [Google Scholar] [CrossRef]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van De Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative Chemotherapy versus Surgery Alone for Resectable Gastroesophageal Cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Boige, V.; Pignon, J.; Saint-Aubert, B.; Lasser, P.; Conroy, T.; Bouché, O.; Segol, P.; Bedenne, L.; Rougier, P.; Ychou, M. Final results of a randomized trial comparing preoperative 5-fluorouracil (F)/cisplatin (P) to surgery alone in adenocarcinoma of stomach and lower esophagus (ASLE): FNLCC ACCORD07-FFCD 9703 trial. J. Clin. Oncol. 2007, 25, 4510. [Google Scholar] [CrossRef]
- Tsai, C.; Mueller, A.; Maubach, J.; Warschkow, R.; Nussbaum, D.P.; Schmied, B.M.; Blazer, D.; Gloor, B.; Worni, M. No Difference in Survival between Neo-Adjuvant Chemotherapy and Neo-Adjuvant Chemoradiation Therapy in Gastric Cardia Cancer Patients: A Contemporary View from the National Cancer Database. Dig. Surg. 2019, 37, 249–257. [Google Scholar] [CrossRef]
- De Vita, F.; Borg, C.; Farina, G.; Geva, R.; Carton, I.; Cuku, H.; Wei, R.; Muro, K. Ramucirumab and paclitaxel in patients with gastric cancer and prior trastuzumab: Subgroup analysis from RAINBOW study. Futur. Oncol. 2019, 15, 2723–2731. [Google Scholar] [CrossRef] [PubMed]
- Shitara, K.; Yatabe, Y.; Matsuo, K.; Sugano, M.; Kondo, C.; Takahari, D.; Ura, T.; Tajika, M.; Ito, S.; Muro, K. Prognosis of patients with advanced gastric cancer by HER2 status and trastuzumab treatment. Gastric Cancer 2012, 16, 261–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadowaki, S.; Masuishi, T.; Eto, T.; Narita, Y.; Taniguchi, H.; Ura, T.; Ando, M.; Tajika, M.; Niwa, Y.; Yatabe, Y.; et al. Depth of response predicts the clinical outcome of advanced HER2-positive gastric cancer to trastuzumab-based first-line chemotherapy. Cancer Chemother. Pharmacol. 2017, 80, 807–813. [Google Scholar] [CrossRef]
- Hecht, J.R.; Bang, Y.J.; Qin, S.K.; Chung, H.C.; Xu, J.M.; Park, J.O.; Jeziorski, K.; Shparyk, Y.; Hoff, P.M.; Sobrero, A.; et al. Lapatinib in Combination With Capecitabine Plus Oxaliplatin in Human Epidermal Growth Factor Receptor 2-Positive Advanced or Metastatic Gastric, Esophageal, or Gastroesophageal Adenocarcinoma: TRIO-013/LOGiC--A Randomized Phase III Trial. J. Clin. Oncol. 2016, 34, 443–451. [Google Scholar] [CrossRef] [Green Version]
- Tabernero, J.; Hoff, P.M.; Shen, L.; Ohtsu, A.; A Shah, M.; Cheng, K.; Song, C.; Wu, H.; Eng-Wong, J.; Kim, K.; et al. Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): Final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2018, 19, 1372–1384. [Google Scholar] [CrossRef]
- Wang, X.; Fu, R.; Hu, Y.; Du, H.; Li, S.; Liu, Y.; Zhang, L.; Ji, J. EGFR gene status predicts response and survival benefit in a preclinical gastric cancer trial treating patient?derived xenografts with cetuximab. Oncol. Rep. 2017, 38, 2387–2393. [Google Scholar] [CrossRef] [Green Version]
- Lordick, F.; Luber, B.; Lorenzen, S.; Hegewisch-Becker, S.; Folprecht, G.; Wöll, E.; Decker, T.; Endlicher, E.; Röthling, N.; Schuster, T.; et al. Cetuximab plus oxaliplatin/leucovorin/5-fluorouracil in first-line metastatic gastric cancer: A phase II study of the Arbeitsgemeinschaft Internistische Onkologie (AIO). Br. J. Cancer 2010, 102, 500–505. [Google Scholar] [CrossRef] [Green Version]
- Macedo, F.; Ladeira, K.; Filho, A.L.L.; Martins, S.F. Gastric Cancer and Angiogenesis: Is VEGF a Useful Biomarker to Assess Progression and Remission? J. Gastric Cancer 2017, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuchs, C.S.; Tomasek, J.; Yong, C.J.; Dumitru, F.; Passalacqua, R.; Goswami, C.; Safran, H.; Santos, L.; Aprile, G.; Ferry, D.R.; et al. Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): An international, randomised, multicentre, placebo-controlled, phase 3 trial. Lancet 2014, 383, 31–39. [Google Scholar] [CrossRef]
- Wilke, H.; Muro, K.; Van Cutsem, E.; Oh, S.-C.; Bodoky, G.; Shimada, Y.; Hironaka, S.; Sugimoto, N.; Lipatov, O.; Kim, T.-Y.; et al. Ramucirumab plus paclitaxel versus placebo plus paclitaxel in patients with previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (RAINBOW): A double-blind, randomised phase 3 trial. Lancet Oncol. 2014, 15, 1224–1235. [Google Scholar] [CrossRef]
- Su, X.; Zhan, P.; Gavine, P.R.; Morgan, S.; Womack, C.; Ni, X.; Shen, D.; Bang, Y.-J.; Im, S.-A.; Kim, W.H.; et al. FGFR2 amplification has prognostic significance in gastric cancer: Results from a large international multicentre study. Br. J. Cancer 2014, 110, 967–975. [Google Scholar] [CrossRef]
- Inokuchi, M.; Fujimori, Y.; Otsuki, S.; Sato, Y.; Nakagawa, M.; Kojima, K. Therapeutic Targeting of Fibroblast Growth Factor Receptors in Gastric Cancer. Gastroenterol. Res. Pract. 2015, 2015, 1–8. [Google Scholar] [CrossRef]
- Ohtsu, A.; Ajani, J.A.; Bai, Y.-X.; Bang, Y.-J.; Chung, H.C.; Pan, H.-M.; Sahmoud, T.; Shen, L.; Yeh, K.-H.; Chin, K.; et al. Everolimus for Previously Treated Advanced Gastric Cancer: Results of the Randomized, Double-Blind, Phase III GRANITE-1 Study. J. Clin. Oncol. 2013, 31, 3935–3943. [Google Scholar] [CrossRef]
- Ramanathan, R.; McDonough, S.L.; Kennecke, H.F.; Iqbal, S.; Baranda, J.C.; Seery, T.E.; Lim, H.J.; Hezel, A.F.; Vaccaro, G.M.; Blanke, C.D. Phase 2 study of MK-2206, an allosteric inhibitor of AKT, as second-line therapy for advanced gastric and gastroesophageal junction cancer: A SWOG cooperative group trial (S1005). Cancer 2015, 121, 2193–2197. [Google Scholar] [CrossRef] [Green Version]
- Li, R.; Li, J.; Wang, X.; Liang, P.; Gao, J. Detection of gastric cancer and its histological type based on iodine concentration in spectral CT. Cancer Imaging 2018, 18, 42. [Google Scholar] [CrossRef]
- Kwee, R.M.; Kwee, T.C. Imaging in Local Staging of Gastric Cancer: A Systematic Review. J. Clin. Oncol. 2007, 25, 2107–2116. [Google Scholar] [CrossRef]
- Kwee, R.M.; Kwee, T.C. Imaging in assessing lymph node status in gastric cancer. Gastric Cancer 2009, 12, 6–22. [Google Scholar] [CrossRef]
- Coburn, N.G.; Seevaratnam, R.; Paszat, L.; Helyer, L.; Law, C.; Swallow, C.; Cardosa, R.; Mahar, A.; Lourenço, L.G.; Dixon, M.; et al. Optimal Management of Gastric Cancer: Results from an international RAND/UCLA expert panel. Ann. Surg. 2014, 259, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Kwee, R.M.; Kwee, T.C. Modern imaging techniques for preoperative detection of distant metastases in gastric cancer. World J. Gastroenterol. 2015, 21, 10502–10509. [Google Scholar] [CrossRef] [PubMed]
- Bruneton, J.N.; Francois, E.; Padovani, B.; Raffaelli, C. Primary tumor staging of gastric and colorectal cancer. Eur. Radiol. 1996, 6, 140–146. [Google Scholar] [CrossRef]
- Huo, X.; Yuan, K.; Shen, Y.; Li, M.; Wang, Q.; Xing, L.; Shi, G. Clinical value of magnetic resonance imaging in preoperative T staging of gastric cancer and postoperative pathological diagnosis. Oncol. Lett. 2014, 8, 275–280. [Google Scholar] [CrossRef] [Green Version]
- Sohn, K.-M.; Lee, J.M.; Lee, S.Y.; Ahn, B.-Y.; Park, S.-M.; Kim, K.-M. Comparing MR Imaging and CT in the Staging of Gastric Carcinoma. Am. J. Roentgenol. 2000, 174, 1551–1557. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.Y.; Han, J.K.; Seong, C.K.; Kim, T.K.; Choi, B.I. MRI in Staging Advanced Gastric Cancer: Is It Useful Compared with Spiral CT? J. Comput. Assist. Tomogr. 2000, 24, 389–394. [Google Scholar] [CrossRef]
- Zhong, L.; Li, L.; Sun, J.H.; Xu, J.R. Preoperative diagnosis of gastric cancer using 2-D magnetic resonance imaging with 3-D reconstruction techniques. Chin. J. Dig. Dis. 2005, 6, 159–164. [Google Scholar] [CrossRef]
- Wang, Z.; Chen, J. Imaging in assessing hepatic and peritoneal metastases of gastric cancer: A systematic review. BMC Gastroenterol. 2011, 11, 19. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Yu, J. The role of MRI in the diagnosis and treatment of gastric cancer. Diagn. Interv. Radiol. 2020, 26, 176–182. [Google Scholar] [CrossRef]
- Fonocho, E.; Aydin, N.; Reddy, S.; Misra, S. Limitations in the use of 18F-FDG PET in the pre-operative staging of gastric cancer: A case series. Int. J. Surg. Case Rep. 2017, 36, 147–150. [Google Scholar] [CrossRef]
- Stahl, A.; Ott, K.; Weber, W.; Becker, K.; Link, T.; Siewert, J.-R.; Schwaiger, M.; Fink, U. FDG PET imaging of locally advanced gastric carcinomas: Correlation with endoscopic and histopathological findings. Eur. J. Nucl. Med. Mol. Imaging 2003, 30, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Kinkel, K.; Lu, Y.; Both, M.; Warren, R.S.; Thoeni, R.F. Detection of Hepatic Metastases from Cancers of the Gastrointestinal Tract by Using Noninvasive Imaging Methods (US, CT, MR Imaging, PET): A Meta-Analysis. Radiology 2002, 224, 748–756. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Molecular Biomarker | Impact on Gastric Cancer Development | Authors |
|---|---|---|
| HER2 | -Amplification and overexpression in GC, the positive cases range from 6% to 30%. -HER2/neu amplification is higher in the intestinal histologic subtype of GC, compared to the diffuse subtype, and is not associated with gender and age, but with the poor survival of GC patients. | [64,65] |
| p53 | -Mutations in the p53 gene occur in the early stages of gastric carcinoma, and their frequency is increased in advanced stages of cancer development. -TP53-positive patients are also classified as one of the GC subtypes. | [66,67] |
| PD1 | -The expression of PDL1 is significantly increased in cases with PCNA and C-met expression, EBV-positive, and without metastasis; a better outcome is associated with increased PD-L1/PD-1 expression. | [68] |
| p73 | -The p73 gene is not an object of genetic modification in gastric carcinogenesis, wild-type p73 is quite often highly expressed in GC tissues by transcriptional induction of an active allele or the activation of a silent allele. | [69] |
| mdm2 | The expression level of the MDM2 protein is importantly increased in intestinal metaplasia and gastric carcinomas in comparison to simple intestinal metaplasia and chronic gastritis. | [70] |
| Bcl-2 | Lymph node metastases, depth of invasion and the negative expression of Bcl-2 are associated with an increased chance of cancer recurrence. | [71] |
| pRb CCND1 | -Cyclin D1 is a positive regulator of the cell cycle process; retinoblastoma protein (pRb) acts as cell cycle repressor, it promotes G1/S arrest and growth restriction through the inhibition of the E2F transcription factors; their higher expression is merged with cell overgrowth and cancer development. -The expression of pRb and cyclin D1 might be present in the early stages of gastric carcinogenesis, with the higher expression of Rb and cyclin D1 among nonneoplastic mucosa comprising dysplasia, intestinal metaplasia, atrophy and gastritis to carcinoma. | [72,73] |
| p16 | The p16 gene plays a main role as a tumor suppressor gene, the deletion of the p16 gene is associated with the carcinogenesis process, as well as the progression of gastric carcinoma. | [74] |
| p27Kip1 | Cyclin-dependent kinase inhibitor 1B, called p27Kip1 with low protein expression in GC, is assigned to advanced tumors, it is importantly higher in weakly differentiated cases and is described as a negative prognostic factor for the survival of patients. | [75] |
| MUC | Mucins are a group of extracellular, huge molecular weight, strongly glycosylated proteins; they have significant characteristics assigned to cell signalling, the creation of chemical barriers, facilities to create a gel, a major function related to lubrication. One of their main roles is also as an inhibitory function, and the high expression of mucin proteins, like MUC1, MUC2, MUC5AC and MUC6 is associated with gastric carcinogenesis process. | [76,77] |
| MRP2 | The overexpression of MRP2 is significant in the initial absence of reaction to chemotherapy treatments of tumors, which allow us to consider it as an important biomarker for chemotherapy response. | [78] |
| MDR1 | MDR1 is a very significant candidate gene in the progress of GC susceptibility, as well as displaying an important impact on drug resistance response, and the knockdown of MDR1 might reverse this phenotype among GC cells. | [79,80] |
| GST-P | The expression of GST-P is visibly increased in tumors that are chemically induced, it is also associated with tumor invasion and recurrence, as well as poor prognosis. | [81,82] |
| MSI | -Microsatellite instability (MSI) is an important indicator of the DNA mismatch repair deficiency, which is an agent in the higher accumulation of genetic alterations in gastric carcinogenesis; MSI-positive patients do not have a high content of targeted mutations, some of them were detected in PIK3CA, EGFR, ERBB3 and ERBB2 genes. -GC cases with a high MSI can have long-term survival, regardless of the positive resection margin status. | [83,84] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machlowska, J.; Baj, J.; Sitarz, M.; Maciejewski, R.; Sitarz, R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. Int. J. Mol. Sci. 2020, 21, 4012. https://doi.org/10.3390/ijms21114012
Machlowska J, Baj J, Sitarz M, Maciejewski R, Sitarz R. Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies. International Journal of Molecular Sciences. 2020; 21(11):4012. https://doi.org/10.3390/ijms21114012
Chicago/Turabian StyleMachlowska, Julita, Jacek Baj, Monika Sitarz, Ryszard Maciejewski, and Robert Sitarz. 2020. "Gastric Cancer: Epidemiology, Risk Factors, Classification, Genomic Characteristics and Treatment Strategies" International Journal of Molecular Sciences 21, no. 11: 4012. https://doi.org/10.3390/ijms21114012