
Modification with Conventional Surfactants to Improve a Lipid-Based Ionic-Liquid-Associated Transcutaneous Anticancer Vaccine

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
2. Results and Discussion
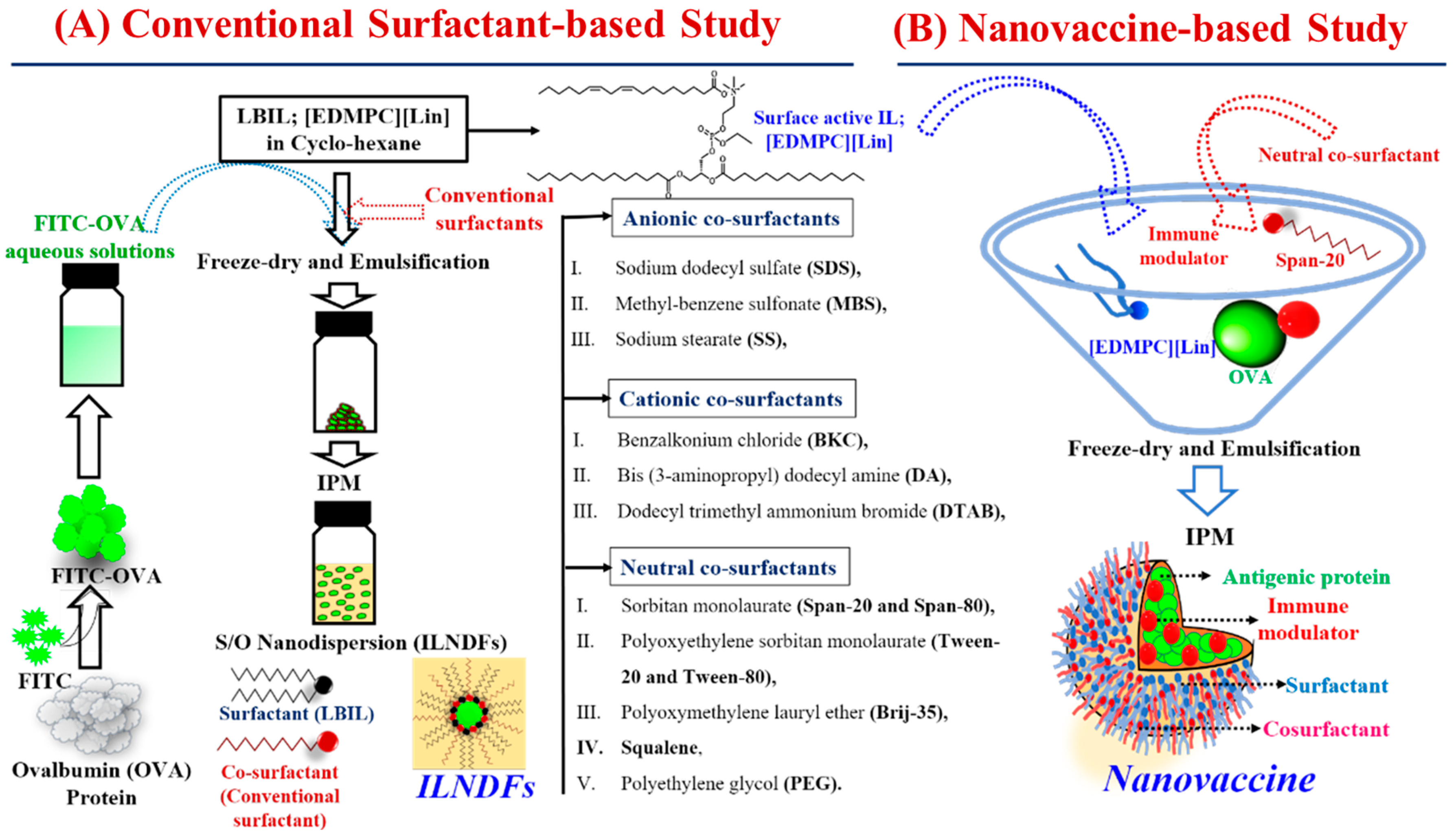
2.1. Selection of Surfactants for IL-Based Formulations
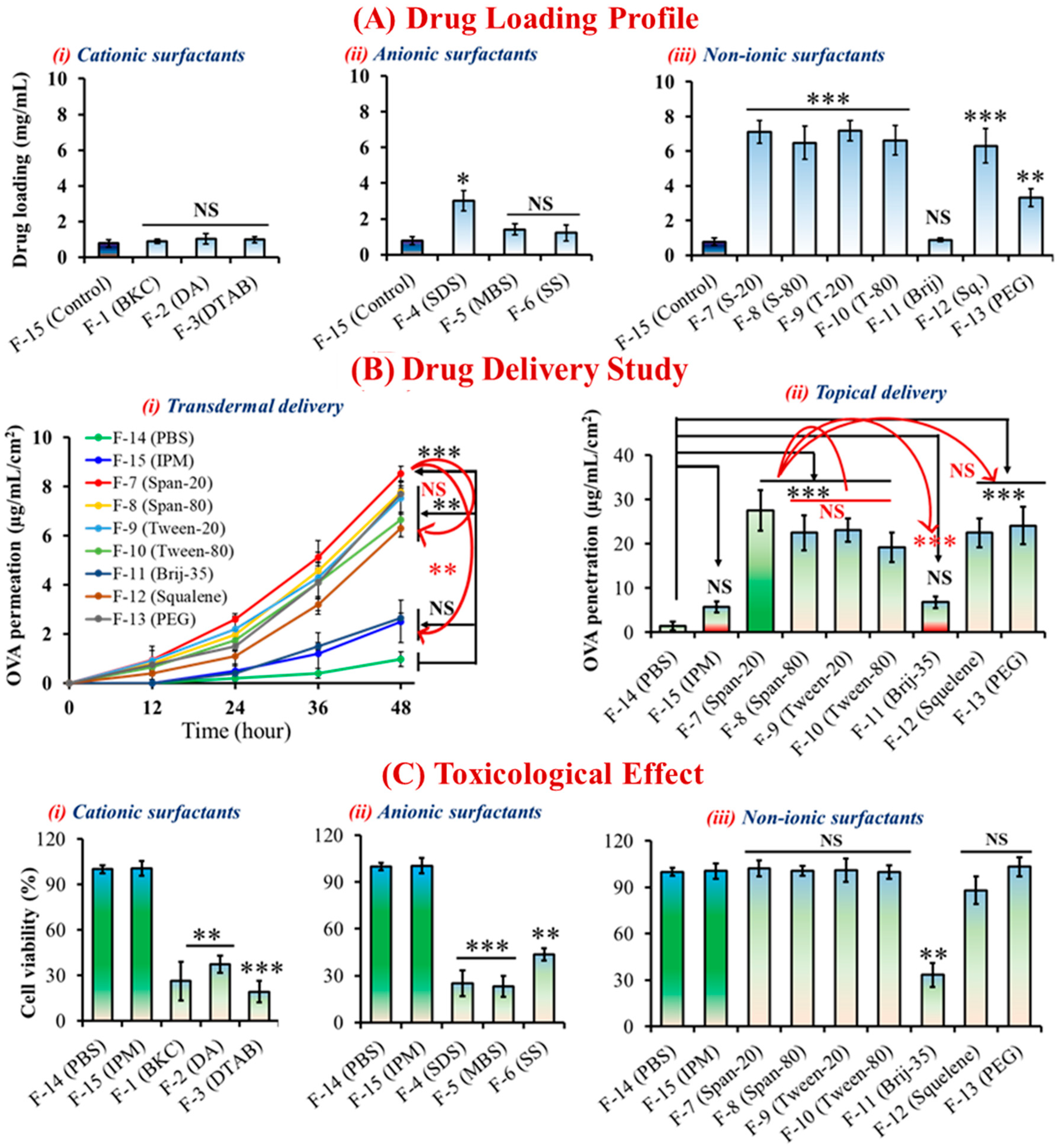
2.2. Morphological Behaviors and Cytotoxicity of ILNDFs
2.3. Effect of ILNDFs on Drug Encapsulation and Skin Permeation
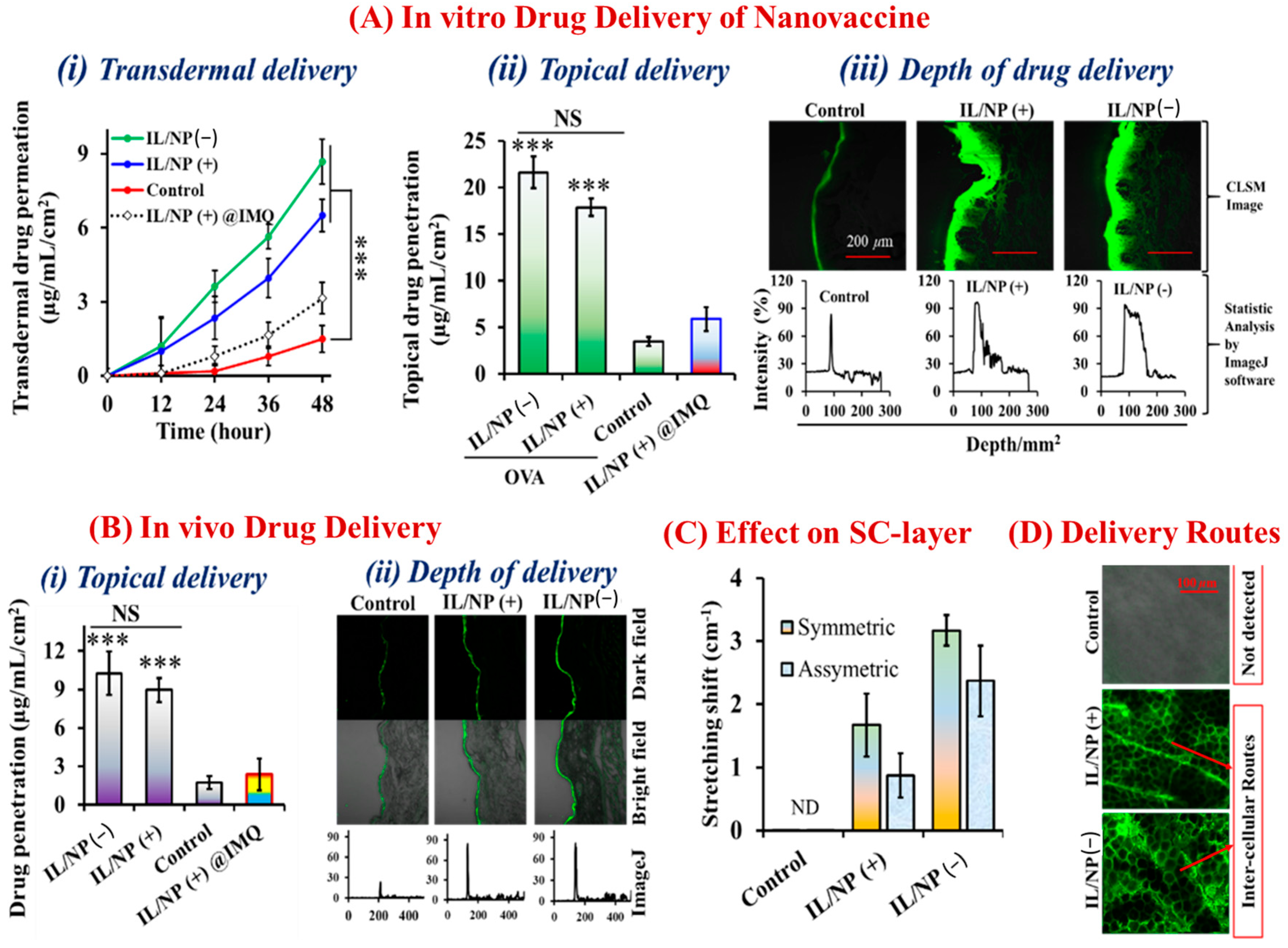
2.4. Morphological and Transdermal Delivery of the Nanovaccine
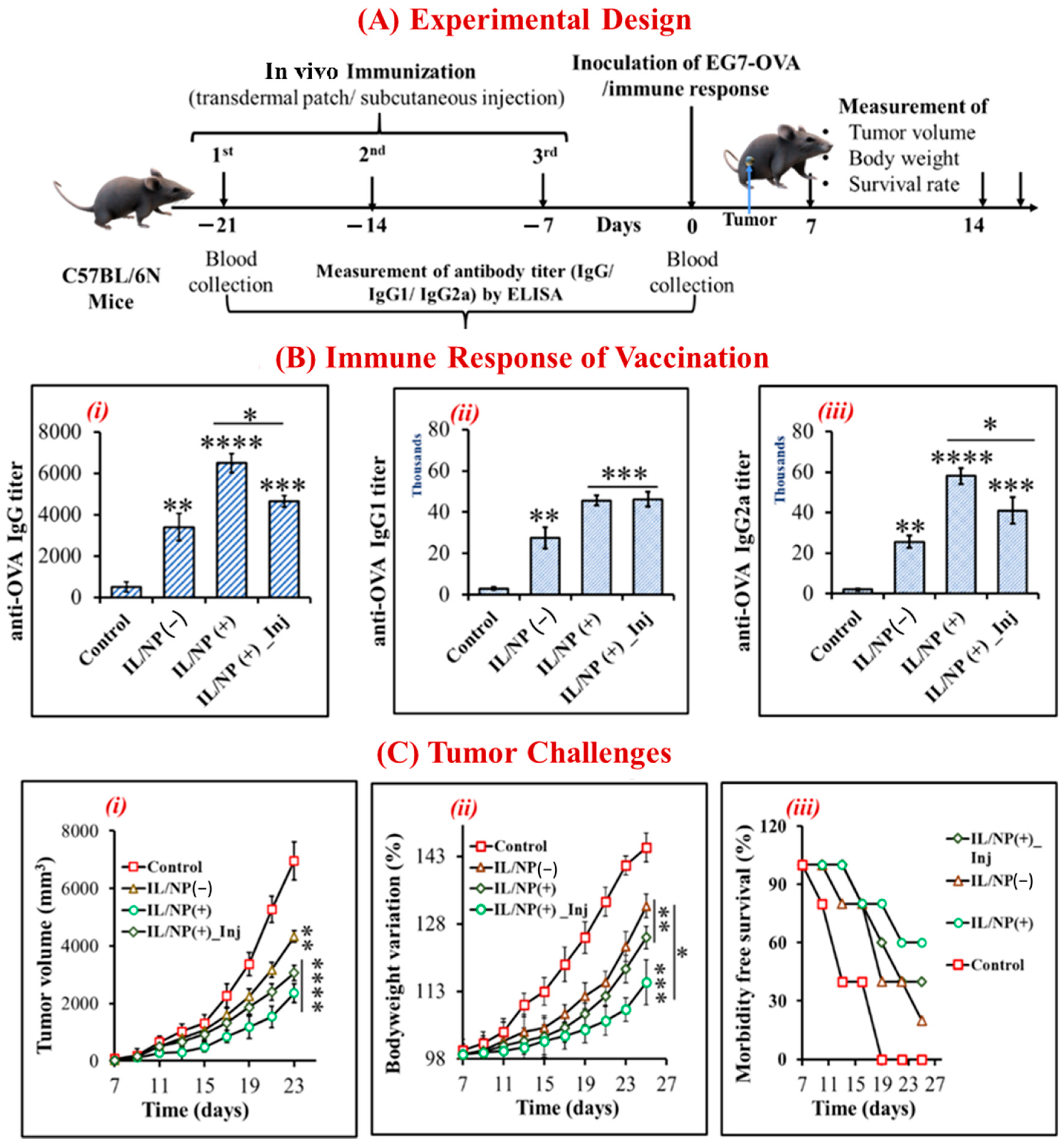
2.5. Prophylactic Effect of the Nanovaccine against Tumors
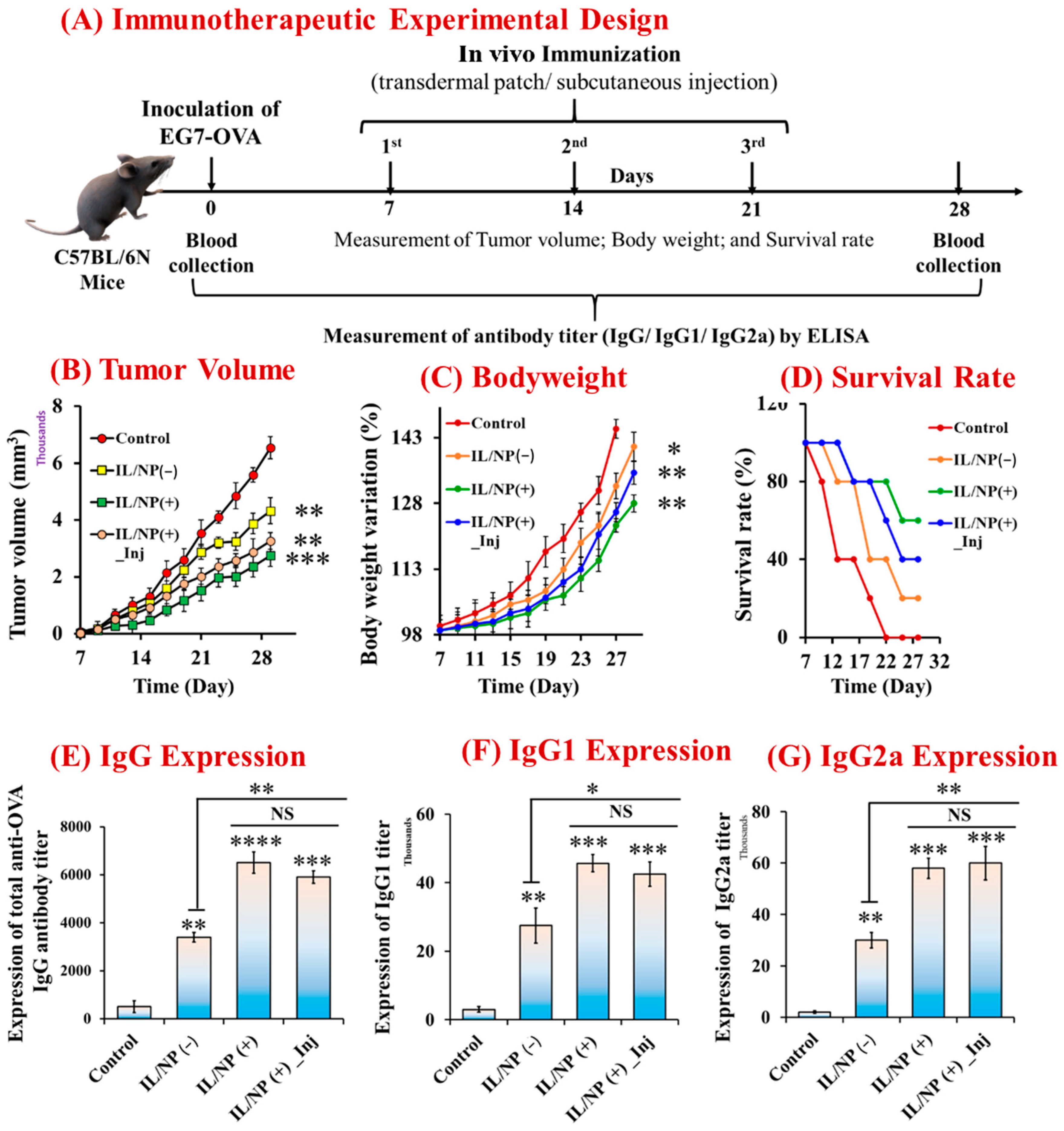
2.6. Therapeutic Immunization and Tumor-Suppressive Effects of the Nanovaccine
2.7. Antitumor Immune Response Induced by the Nanovaccine
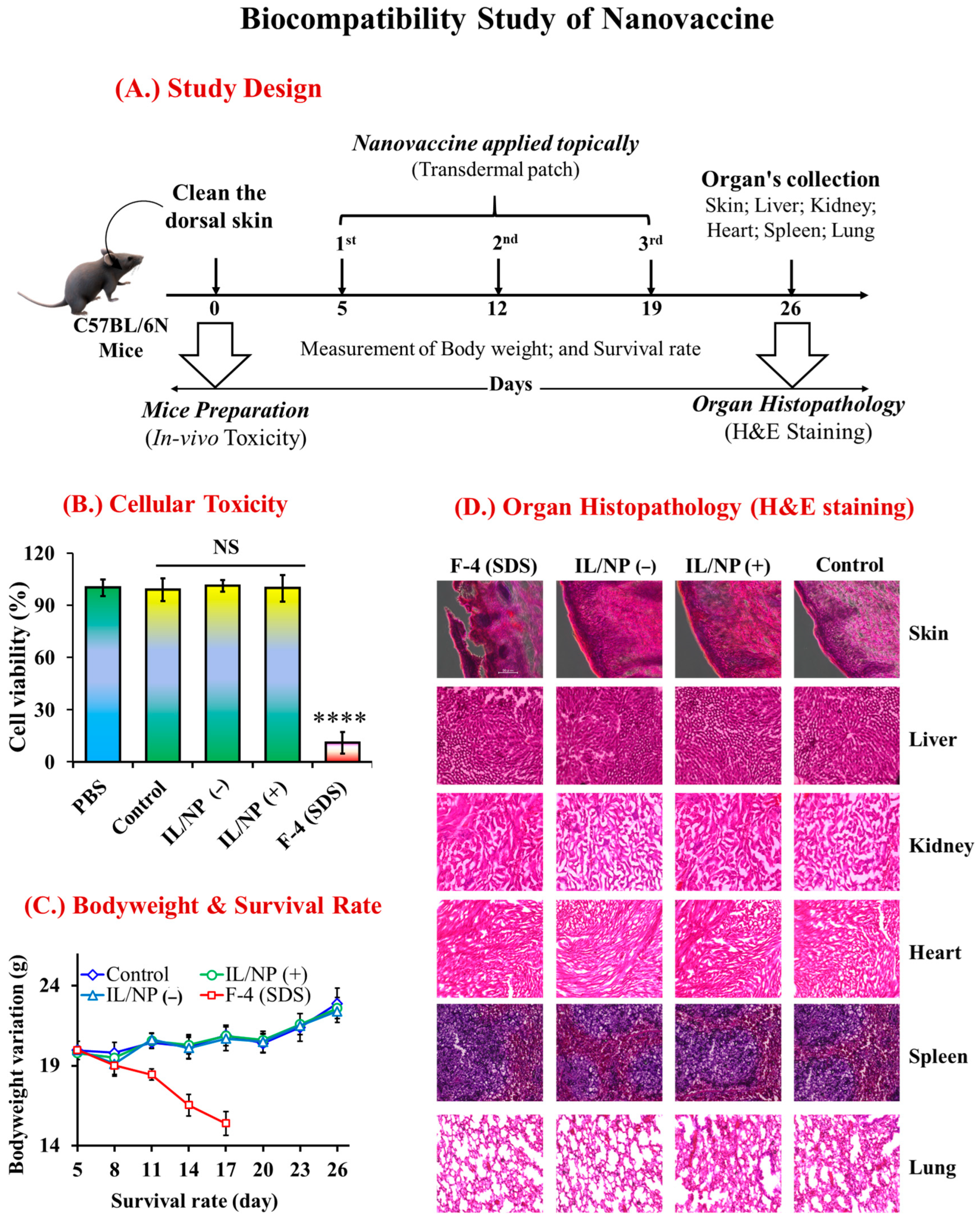
2.8. Biological Safety of the Nanovaccine
3. Experimental Materials and Methods
3.1. Chemicals and Reagents
3.2. Preparation and Morphological Characterizations of ILNDFs
3.3. Drug Loading, Encapsulation, and Skin Permeation of ILNDFs
3.4. In Vitro and In Vivo Toxicity Assessments
3.5. Preparation and Morphological Observation of the Nanovaccine
3.6. TDDS of Nanovaccine
3.7. Drug Release Pathway and Effect on the Skin
3.7.1. Drug Release Pathway
3.7.2. Effect on the SC Layer
3.8. Vaccination and Immune Response against the Tumor
3.9. Prophylactic and Therapeutic Effects of the Nanovaccine against Tumors
3.10. Antigen Uptake by Skin DCs: Flow Cytometric Analysis
3.11. Cytotoxic Immune Cell Counts in the TME
3.12. Statistical Analysis
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- WHO. World Immunization Week 2022-Long Life for All: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2022; ISBN 978-92-4-005114-0.
- Mahmud, N.; Anik, M.I.; Hossain, M.K.; Khan, I.; Uddin, S. Advances in Nanomaterial-Based Platforms to Combat COVID-19: Diagnostics, Preventions, Therapeutics, and Vaccine Developments. ACS Appl. Bio Mater. 2022, 5, 2431–2460. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Vaccine Market Report-2022; World Health Organization: Geneva, Switzerland, 2022; pp. 1–57.
- Uddin, S.; Islam, M.R.; Md Moshikur, R.; Wakabayashi, R.; Kamiya, N.; Moniruzzaman, M.; Goto, M. Transdermal Delivery of Antigenic Protein Using Ionic Liquid-Based Nanocarriers for Tumor Immunotherapy. ACS Appl. Bio Mater. 2022, 5, 2586–2597. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, E.; Balmert, S.C.; Sumpter, T.L.; Carey, C.D.; Erdos, G.; Falo, L.D. Microarray Patches Enable the Development of Skin-Targeted Vaccines against COVID-19. Adv. Drug Deliv. Rev. 2021, 171, 164–186. [Google Scholar] [CrossRef] [PubMed]
- Holmbäck, J.; Rinwa, V.; Halthur, T.; Rinwa, P.; Carlsson, A.; Herslöf, B. AKVANO®: A Novel Lipid Formulation System for Topical Drug Delivery—In Vitro Studies. Pharmaceutics 2022, 14, 794. [Google Scholar] [CrossRef] [PubMed]
- Modeling, M. Pharmacokinetic Study of Triptolide Nanocarrier in Transdermal Drug Delivery System—Combination of Experiment and Mathematical Modeling. Molecules 2023, 28, 553. [Google Scholar] [CrossRef]
- Hassan, M.M.; Islam, M.M.; Uddin, S.; Bhowmik, A.; Rokeya, B. Antihyperglycemic Potential of Ethanolic Extract of Couroupita Guianensis on Streptozocin Induced Experimental Diabetic Rat Model. Asian J. Res. Med. Pharm. Sci. 2018, 5, 1–10. [Google Scholar] [CrossRef]
- Hassan, M.M.; Uddin, S.; Bhowmik, A.; Ashraf, A.; Islam, M.M.; Rokeya, B. Phytochemical Screening and Antidiabetic Effects of Fruit Rind of Momordica Dioica Roxb. on Streptozocin Induced Type 2 Diabetic Rats. Heliyon 2022, 8, 8771. [Google Scholar] [CrossRef]
- Egorova, K.S.; Gordeev, E.G.; Ananikov, V.P. Biological Activity of Ionic Liquids and Their Application in Pharmaceutics and Medicine. Chem. Rev. 2017, 117, 7132–7189. [Google Scholar] [CrossRef] [Green Version]
- Uddin, S.; Rafiqul Islam, M.; Raihan Chowdhury, M.; Wakabayashi, R.; Kamiya, N.; Moniruzzaman, M.; Goto, M. Lipid-Based Ionic-Liquid-Mediated Nanodispersions as Biocompatible Carriers for the Enhanced Transdermal Delivery of a Peptide Drug. ACS Appl. Bio Mater. 2021, 4, 6256–6267. [Google Scholar] [CrossRef]
- Uddin, S.; Chowdhury, M.R.; Wakabayashi, R.; Kamiya, N.; Moniruzzaman, M.; Goto, M. Lipid Based Biocompatible Ionic Liquids: Synthesis, Characterization and Biocompatibility Evaluation. Chem. Commun. 2020, 56, 13756–13759. [Google Scholar] [CrossRef]
- Ali, M.K.; Moshikur, R.M.; Goto, M.; Moniruzzaman, M. Recent Developments in Ionic Liquid-Assisted Topical and Transdermal Drug Delivery. Pharm. Res. 2022, 39, 2335–2351. [Google Scholar] [CrossRef]
- Kozaka, S.; Tahara, Y.; Wakabayashi, R.; Nakata, T.; Ueda, T.; Kamiya, N.; Goto, M. Transcutaneous Cancer Vaccine Using a Reverse Micellar Antigen Carrier. Mol. Pharm. 2020, 17, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Uddin, S.; Islam, M.M.; Hassan, M.M.; Bhowmik, A.; Rokeya, B. Amaranthus Viridis Modulates Anti-Hyperglycemic Pathways in Hemi-Diaphragm and Improves Glycogenesis Liver Function in Rats. J. Pharmacogn. Phyther. 2016, 8, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Chen, B.; Shi, W.; Huang, W.; Qian, H. Ionic Liquids for Enhanced Drug Delivery: Recent Progress and Prevailing Challenges. Mol. Pharm. 2022, 19, 1033–1046. [Google Scholar] [CrossRef] [PubMed]
- Alsaab, H.O.; Alharbi, F.D.; Alhibs, A.S.; Alanazi, N.B.; Alshehri, B.Y.; Saleh, M.A.; Alshehri, F.S.; Algarni, M.A.; Almugaiteeb, T.; Uddin, M.N.; et al. PLGA-Based Nanomedicine: History of Advancement and Development in Clinical Applications of Multiple Diseases. Pharmaceutics 2022, 14, 2728. [Google Scholar] [CrossRef] [PubMed]
- Liang, R.; Zhuang, F.; Meng, Z.; Deng, M.; Zheng, C.; Duan, M. A New Potent Route of DNA Vaccine Inoculation: DNA-Liposome Complexes on Bare Skin Induce Antigen-Special Antibody Responses. Molecules 2003, 8, 120–126. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.X.; Tseng, J.C.; Yu, G.Y.; Luo, Y.; Huang, C.Y.F.; Hong, Y.R.; Chuang, T.H. Recent Advances in the Development of Toll-like Receptor Agonist-Based Vaccine Adjuvants for Infectious Diseases. Pharmaceutics 2022, 14, 423. [Google Scholar] [CrossRef]
- Sun, H.; Li, Y.; Zhang, P.; Xing, H.; Zhao, S.; Song, Y.; Wan, D.; Yu, J. Targeting Toll-like Receptor 7/8 for Immunotherapy: Recent Advances and Prospectives. Biomark. Res. 2022, 10, 89. [Google Scholar] [CrossRef]
- Weiss, A.M.; Hossainy, S.; Rowan, S.J.; Hubbell, J.A.; Esser-Kahn, A.P. Immunostimulatory Polymers as Adjuvants, Immunotherapies, and Delivery Systems. Macromolecules 2022, 55, 6913–6937. [Google Scholar] [CrossRef]
- Chowdhury, M.R.; Moshikur, R.M.; Wakabayashi, R.; Moniruzzaman, M.; Goto, M. Biocompatible Ionic Liquids Assisted Transdermal Co-Delivery of Antigenic Protein and Adjuvant for Cancer Immunotherapy. Int. J. Pharm. 2021, 601, 120582. [Google Scholar] [CrossRef] [PubMed]
- Ruan, S.; Huang, Y.; He, M.; Gao, H. Advanced Biomaterials for Cell-Specific Modulation and Restore of Cancer Immunotherapy. Adv. Sci. 2022, 9, 2200027. [Google Scholar] [CrossRef] [PubMed]
- Md Moshikur, R.; Shimul, I.M.; Uddin, S.; Wakabayashi, R.; Moniruzzaman, M.; Goto, M. Transformation of Hydrophilic Drug into Oil-Miscible Ionic Liquids for Transdermal Drug Delivery. ACS Appl. Mater. Interfaces 2022, 14, 55332–55341. [Google Scholar] [CrossRef] [PubMed]
- Uddin, S. Lipid-Based Ionic Liquid Is a Novel Biocompatible Carrier for the Transdermal Peptide Drug Delivery. In Proceedings of the 23rd International Conference and Exhibition on Pharmaceutics & Novel Drug Delivery Systems, London, UK, 21–22 February 2022. [Google Scholar]
- Uddin, S. Synthesis of Widely-Soluble Biocompatible Ionic Liquids Aiming to Enhance Transdermal Drug Delivery System. In Proceedings of the 22nd World Congress on Pharmaceutical Sciences and Innovations in Pharma Industry, Berlin, Germany, 24–25 June 2022. [Google Scholar]
- Hmingthansanga, V.; Singh, N.; Banerjee, S.; Manickam, S.; Velayutham, R.; Natesan, S. Improved Topical Drug Delivery: Role of Permeation Enhancers and Advanced Approaches. Pharmaceutics 2022, 14, 2818. [Google Scholar] [CrossRef] [PubMed]
- Ghasemiyeh, P.; Mohammadi-Samani, S. Potential of Nanoparticles as Permeation Enhancers and Targeted Delivery Options for Skin: Advantages and Disadvantages. Drug Des. Dev. Ther. 2020, 14, 3271–3289. [Google Scholar] [CrossRef]
- Yu, Y.Q.; Yang, X.; Wu, X.F.; Fan, Y. Bin Enhancing Permeation of Drug Molecules Across the Skin via Delivery in Nanocarriers: Novel Strategies for Effective Transdermal Applications. Front. Bioeng. Biotechnol. 2021, 9, 646554. [Google Scholar] [CrossRef]
- Anik, M.I.; Mahmud, N.; Al Masud, A.; Khan, M.I.; Islam, M.N.; Uddin, S.; Hossain, M.K. Role of Reactive Oxygen Species in Aging and Age-Related Diseases: A Review. ACS Appl. Bio Mater. 2022, 5, 4028–4054. [Google Scholar] [CrossRef]
- Dib, N.; Lépori, C.M.O.; Correa, N.M.; Silber, J.J.; Falcone, R.D.; García-Río, L. Biocompatible Solvents and Ionic Liquid-Based Surfactants as Sustainable Components to Formulate Environmentally Friendly Organized Systems. Polymers 2021, 13, 1378. [Google Scholar] [CrossRef]
- Bajpai, D.; Tyagi, V.K. Nonionic Surfactants: An Overview. Tenside Surfactants Deterg. 2010, 47, 190–196. [Google Scholar] [CrossRef]
- Miyazawa, T.; Itaya, M.; Burdeos, G.C.; Nakagawa, K.; Miyazawa, T. A Critical Review of the Use of Surfactant-Coated Nanoparticles in Nanomedicine and Food Nanotechnology. Int. J. Nanomed. 2021, 16, 3937–3999. [Google Scholar] [CrossRef]
- Souto, E.B.; Cano, A.; Martins-Gomes, C.; Coutinho, T.E.; Zielińska, A.; Silva, A.M. Microemulsions and Nanoemulsions in Skin Drug Delivery. Bioengineering 2022, 9, 158. [Google Scholar] [CrossRef]
- Drugs, N.; Evaluation, D. Good Review Practice: Clinical Review of Investigational New Drug Applications. FDA 2013, 6, 527–542. [Google Scholar] [CrossRef]
- Muhammad, S.; Janakiraman, A.K.; Khan, A.; Naeem, A. Syed Faisal Badshah Surfactants and Their Role in Pharmaceutical Product Development: An Overview. J. Pharm. Pharm. 2019, 6, 72–82. [Google Scholar]
- Cheng, K.C.; Khoo, Z.S.; Lo, N.W.; Tan, W.J.; Chemmangattuvalappil, N.G. Design and Performance Optimisation of Detergent Product Containing Binary Mixture of Anionic-Nonionic Surfactants. Heliyon 2020, 6, e03861. [Google Scholar] [CrossRef]
- Ameta, R.K.; Soni, K.B.A. Recent Advances in Improving the Bioavailability of Hydrophobic/Lipophilic Drugs and Their Delivery via Self-Emulsifying Formulations. Colloids Interfaces 2023, 7, 16. [Google Scholar] [CrossRef]
- Som, I.; Bhatia, K.; Yasir, M. Status of Surfactants as Penetration Enhancers in Transdermal Drug Delivery. J. Pharm. Bioalied Sci. 2012, 4, 2–9. [Google Scholar] [CrossRef]
- Islam, M.R.; Uddin, S.; Chowdhury, M.R.; Wakabayashi, R.; Moniruzzaman, M.; Goto, M. Insulin Transdermal Delivery System for Diabetes Treatment Using a Biocompatible Ionic Liquid-Based Microemulsion. ACS Appl. Mater. Interfaces 2021, 13, 42461–42472. [Google Scholar] [CrossRef] [PubMed]
- Directions, F. Controlled Drug Delivery Systems: Current Status and Future Directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef]
- Kdimati, S.; Mullins, C.S.; Linnebacher, M. Cancer-Cell-Derived Igg and Its Potential Role in Tumor Development. Int. J. Mol. Sci. 2021, 22, 11597. [Google Scholar] [CrossRef]
- Van der Leun, A.M.; Thommen, D.S.; Schumacher, T.N. CD8+ T Cell States in Human Cancer: Insights from Single-Cell Analysis. Nat. Rev. Cancer 2020, 20, 218–232. [Google Scholar] [CrossRef]
- Liang, F.; Nilsson, L.M.; Byvald, F.; Rezapour, A.; Taflin, H.; Nilsson, J.A.; Yrlid, U. A Fraction of CD8+ T Cells from Colorectal Liver Metastases Preferentially Repopulate Autologous Patient-Derived Xenograft Tumors as Tissue-Resident Memory T Cells. Cancer 2022, 14, 2882. [Google Scholar] [CrossRef]
- Gupta, M.; Wahi, A.; Sharma, P.; Nagpal, R.; Raina, N.; Kaurav, M.; Bhattacharya, J.; Rodrigues Oliveira, S.M.; Dolma, K.G.; Paul, A.K.; et al. Recent Advances in Cancer Vaccines: Challenges, Achievements, and Futuristic Prospects. Vaccines 2022, 10, 2011. [Google Scholar] [CrossRef]
- Karki, R.; Sharma, B.R.; Tuladhar, S.; Williams, E.P.; Zalduondo, L.; Samir, P.; Zheng, M.; Sundaram, B.; Banoth, B.; Malireddi, R.K.S.; et al. Synergism of TNF-α and IFN-γ Triggers Inflammatory Cell Death, Tissue Damage, and Mortality in SARS-CoV-2 Infection and Cytokine Shock Syndromes. Cell 2021, 184, 149–168. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.R.; Chowdhury, M.R.; Wakabayashi, R.; Tahara, Y.; Kamiya, N.; Moniruzzaman, M.; Goto, M. Choline and Amino Acid Based Biocompatible Ionic Liquid Mediated Transdermal Delivery of the Sparingly Soluble Drug Acyclovir. Int. J. Pharm. 2020, 582, 119335. [Google Scholar] [CrossRef]
- Hu, H.; Li, Y.; Zhou, Q.; Ao, Y.; Yu, C.; Wan, Y.; Xu, H.; Li, Z.; Yang, X. Redox-Sensitive Hydroxyethyl Starch-Doxorubicin Conjugate for Tumor Targeted Drug Delivery. ACS Appl. Mater. Interfaces 2016, 8, 30833–30844. [Google Scholar] [CrossRef]
- Hossain, M.A.; Sutradhar, L.; Sarker, T.R.; Saha, S.; Iqbal, M.M. Toxic Effects of Chlorpyrifos on the Growth, Hematology, and Different Organs Histopathology of Nile Tilapia, Oreochromis Niloticus. Saudi J. Biol. Sci. 2022, 29, 103316. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.R.; Chowdhury, M.R.; Wakabayashi, R.; Kamiya, N.; Moniruzzaman, M.; Goto, M. Ionic Liquid-in-Oil Microemulsions Prepared with Biocompatible Choline Carboxylic Acids for Improving the Transdermal Delivery of a Sparingly Soluble Drug. Pharmaceutics 2020, 12, 392. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Formulations | Composition | Drug (mg/mL) | Particle Size (nm) | PDI | ||||
|---|---|---|---|---|---|---|---|---|
| Name | Symbol * | Surfactant (2.5 wt.%) | Co-Surfactant (2.5 wt.%) | Base-Liquids (1 mL) | OVA (mg) | IMQ (mg) | ||
| Cationic cosurfactants-based formulations | ||||||||
| IL-BKC-NDF | F-1 | [EDMPC][Lin] | BKC | IPM | 2 | - | 396 | 0.398 |
| IL-DA-NDF | F-2 | [EDMPC][Lin] | DA | IPM | 2 | - | 841 | 0.562 |
| IL-DTAB-NDF | F-3 | [EDMPC][Lin] | DTAB | IPM | 2 | - | 663 | 0.466 |
| Anionic cosurfactants-based formulations | ||||||||
| IL-SDS-NDF | F-4 | [EDMPC][Lin] | SDS | IPM | 2 | - | 543 | 0.335 |
| IL-MBS-NDF | F-5 | [EDMPC][Lin] | MBS | IPM | 2 | - | 712 | 0.621 |
| IL-SS-NDF | F-6 | [EDMPC][Lin] | SS | IPM | 2 | - | 476 | 0.425 |
| Nonionic or Neutral cosurfactants-based formulations | ||||||||
| IL-S-20-NDF | F-7 | [EDMPC][Lin] | Span-20 | IPM | 2 | - | 260 | 0.254 |
| IL-S-80-NDF | F-8 | [EDMPC][Lin] | Span-80 | IPM | 2 | - | 429 | 0.301 |
| IL-T-20-NDF | F-9 | [EDMPC][Lin] | Tween-20 | IPM | 2 | - | 174 | 0.263 |
| IL-T-80-NDF | F-10 | [EDMPC][Lin] | Tween-80 | IPM | 2 | - | 216 | 0.212 |
| IL-Brij-NDF | F-11 | [EDMPC][Lin] | Brij-35 | IPM | 2 | - | 531 | 0.462 |
| IL-Sq-NDF | F-12 | [EDMPC][Lin] | Squalene | IPM | 2 | - | 458 | 0.312 |
| IL-PEG-NDF | F-13 | [EDMPC][Lin] | PEG | IPM | 2 | - | 824 | 0.391 |
| Control group | ||||||||
| Aqueous NDF | F-14 | - | - | PBS | 2 | - | - | - |
| Oil NDF | F-15 | - | - | IPM | 2 | - | - | 0.325 |
| Formulations for nanovaccine study | ||||||||
| Control group | Control | - | - | PBS | 2 | 1 | - | - |
| IL/OVA+IMQ | IL/NP (+)_Inj. | - | - | PBS | 2 | 1 | - | - |
| IL/OVA+IMQ | IL/NP (+)_TP | [EDMPC][Lin] | Span-20 | IPM | 2 | 1 | 338 | 0.266 |
| IL/OVA | IL/NP (−) | [EDMPC][Lin] | Span-20 | IPM | 2 | - | 269 | 0.309 |
| Formulation Symbol | Transdermal Flux | Lag Time | Permeation Coefficient | Diffusion Coefficient | Skin Partition Coefficient |
|---|---|---|---|---|---|
| J (µg/cm2/h) | tL (h) | Kp (cm/h) | D (×10−3 cm2/h) | Kskin | |
| Cationic cosurfactants-based formulations | |||||
| F-1 (BKC) | 1.3 ± 0.2 a | 4.2 ± 0.5 NS | 0.03 ± 0.01 | 0.68 ± 0.02 | 0.08 ± 0.05 |
| F-2 (DA) | 2.1 ± 0.3 a | 3.7 ± 0.4 NS | 0.09 ± 0.05 | 0.72 ± 0.03 | 0.19 ± 0.07 |
| F-3 (DTAB) | 1.8 ± 0.5 a | 3.9 ± 0.6 NS | 0.06 ± 0.03 | 0.71 ± 0.02 | 0.15 ± 0.04 |
| Anionic-cosurfactants-based formulations | |||||
| F-4 (SDS) | 3.9 ± 0.8 b | 3.3 ± 0.6 a | 0.12 ± 0.04 | 0.63 ± 0.03 | 0.36 ± 0.02 |
| F-5 (MBS) | 1.4 ± 0.1 a | 3.8 ± 0.7 NS | 0.07 ± 0.03 | 0.06 ± 0.02 | 0.08 ± 0.02 |
| F-6 (SS) | 2.8 ± 0.4 a | 3.1 ± 0.3 a | 0.09 ± 0.02 | 0.46 ± 0.01 | 0.21 ± 0.05 |
| Nonionic or neutral-cosurfactants-based formulations | |||||
| F-7 (Span-20) | 6.6 ± 0.7 d | 2.8 ± 0.4 c | 0.15 ± 0.07 | 1.12 ± 0.09 | 0.68 ± 0.12 |
| F-8 (Span-80) | 5.1 ± 0.8 b | 2.8 ± 0.6 c | 0.14 ± 0.08 | 1.12 ± 0.11 | 0.52 ± 0.09 |
| F-9 (Tween-20) | 6.1 ± 0.5 c | 2.9 ± 0.5 b | 0.14 ± 0.05 | 1.11 ± 0.07 | 0.61 ± 0.13 |
| F-10 (Tween-80) | 5.4 ± 0.8 c | 2.9 ± 0.3 b | 0.12 ± 0.05 | 1.08 ± 0.05 | 0.49 ± 0.16 |
| F-11 (Brij-35) | 1.2 ± 0.3 a | 4.4 ± 0.8 NS | 0.04 ± 0.07 | 0.10 ± 0.02 | 0.07 ± 0.03 |
| F-12 (Squalene) | 4.8 ± 0.9 b | 3.2 ± 0.6 b | 0.11 ± 0.04 | 0.70 ± 0.05 | 0.39 ± 0.15 |
| F-13 (PEG) | 5.6 ± 0.7 c | 2.9 ± 0.5 b | 0.13 ± 0.09 | 0.98 ± 0.08 | 0.62 ± 0.22 |
| Control group or without surfactant/cosurfactants-based formulations | |||||
| F-14 (PBS) | 0.3 ± 0.1 | 4.5 ± 0.5 | 0.01 ± 0.01 | 0.04 ± 0.01 | 0.05 ± 0.02 |
| Formulations for nanovaccine study | |||||
| Control | 0.3 ± 0.1 | 4.5 ± 0.5 | 0.01 ± 0.01 | 0.02 ± 0.01 | 0.06 ± 0.01 |
| IL/NP (+) | 6.0 ± 0.6 c | 3.1 ± 0.3 a | 0.12 ± 0.05 | 1.10 ± 0.1 | 0.61 ± 0.09 |
| IL/NP (-) | 6.6 ± 0.7 d | 2.8 ± 0.4 c | 0.15 ± 0.07 | 1.12 ± 0.09 | 0.68 ± 0.12 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uddin, S.; Islam, M.R.; Moshikur, R.M.; Wakabayashi, R.; Moniruzzaman, M.; Goto, M. Modification with Conventional Surfactants to Improve a Lipid-Based Ionic-Liquid-Associated Transcutaneous Anticancer Vaccine. Molecules 2023, 28, 2969. https://doi.org/10.3390/molecules28072969
Uddin S, Islam MR, Moshikur RM, Wakabayashi R, Moniruzzaman M, Goto M. Modification with Conventional Surfactants to Improve a Lipid-Based Ionic-Liquid-Associated Transcutaneous Anticancer Vaccine. Molecules. 2023; 28(7):2969. https://doi.org/10.3390/molecules28072969
Chicago/Turabian StyleUddin, Shihab, Md. Rafiqul Islam, Rahman Md. Moshikur, Rie Wakabayashi, Muhammad Moniruzzaman, and Masahiro Goto. 2023. "Modification with Conventional Surfactants to Improve a Lipid-Based Ionic-Liquid-Associated Transcutaneous Anticancer Vaccine" Molecules 28, no. 7: 2969. https://doi.org/10.3390/molecules28072969