
Vitamin B12 in Foods, Food Supplements, and Medicines—A Review of Its Role and Properties with a Focus on Its Stability

Abstract
:1. Introduction
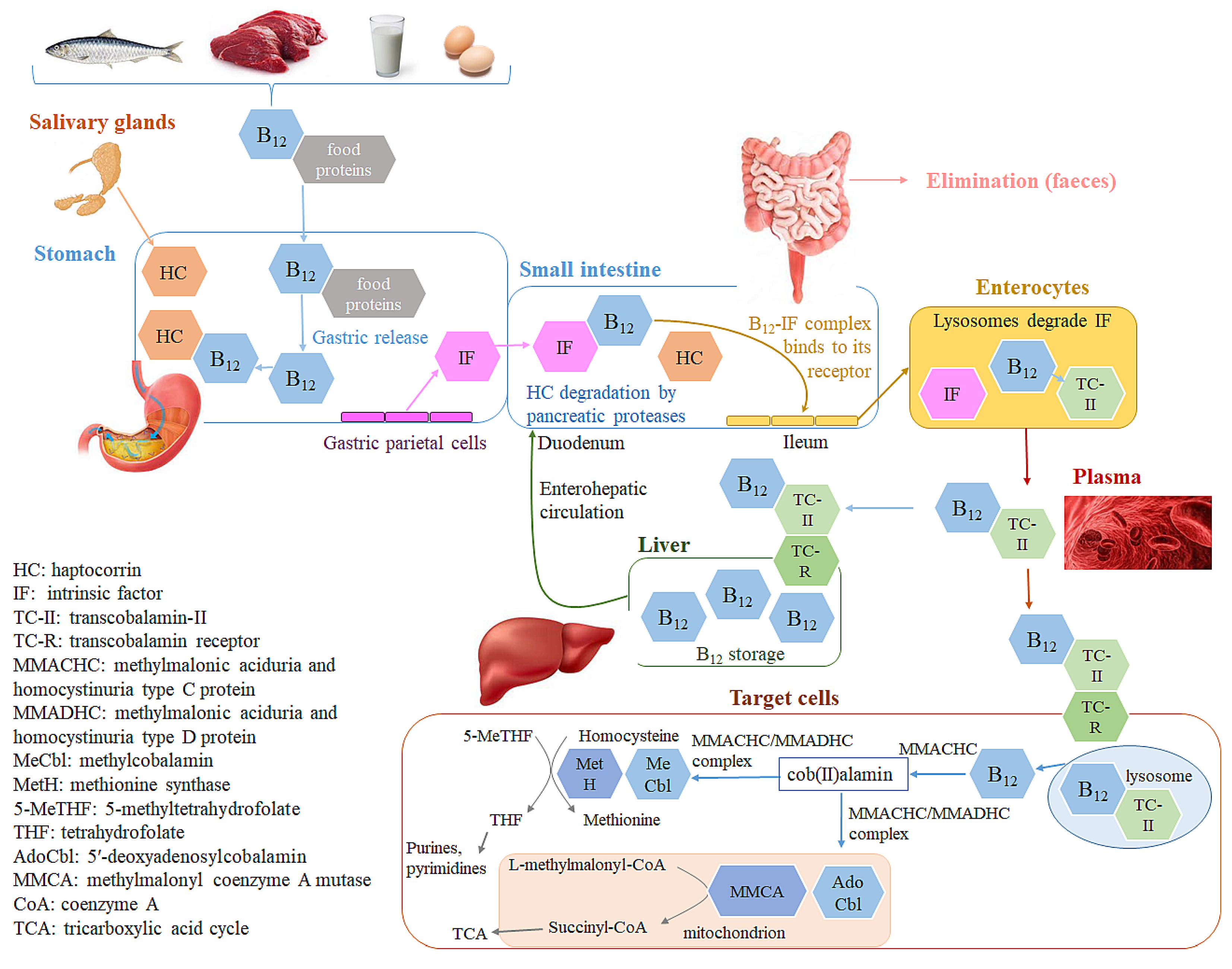
2. Vitamin B12 ADME Properties, Activation, and Stability in the Human Body
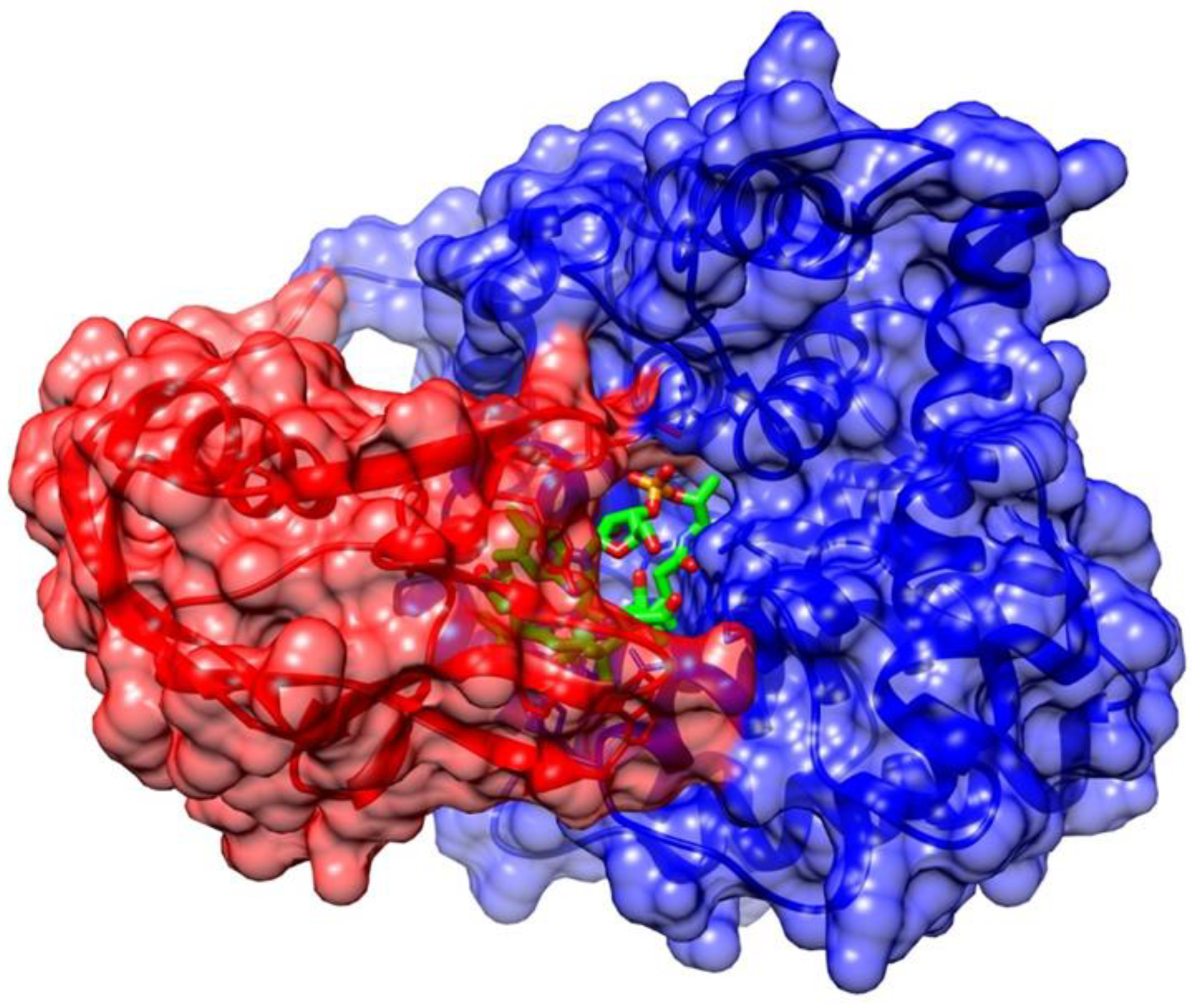
Vitamin B12 Stability in the Complex with Transport Proteins in the Human Body
3. Mechanism of Action of Vitamin B12 in the Human Body
4. Vitamin B12 Deficiency
5. Treatment and Prevention of Vitamin B12 Deficiency
5.1. Different Routes of Vitamin B12 Application
5.2. Different Vitamin B12 Forms
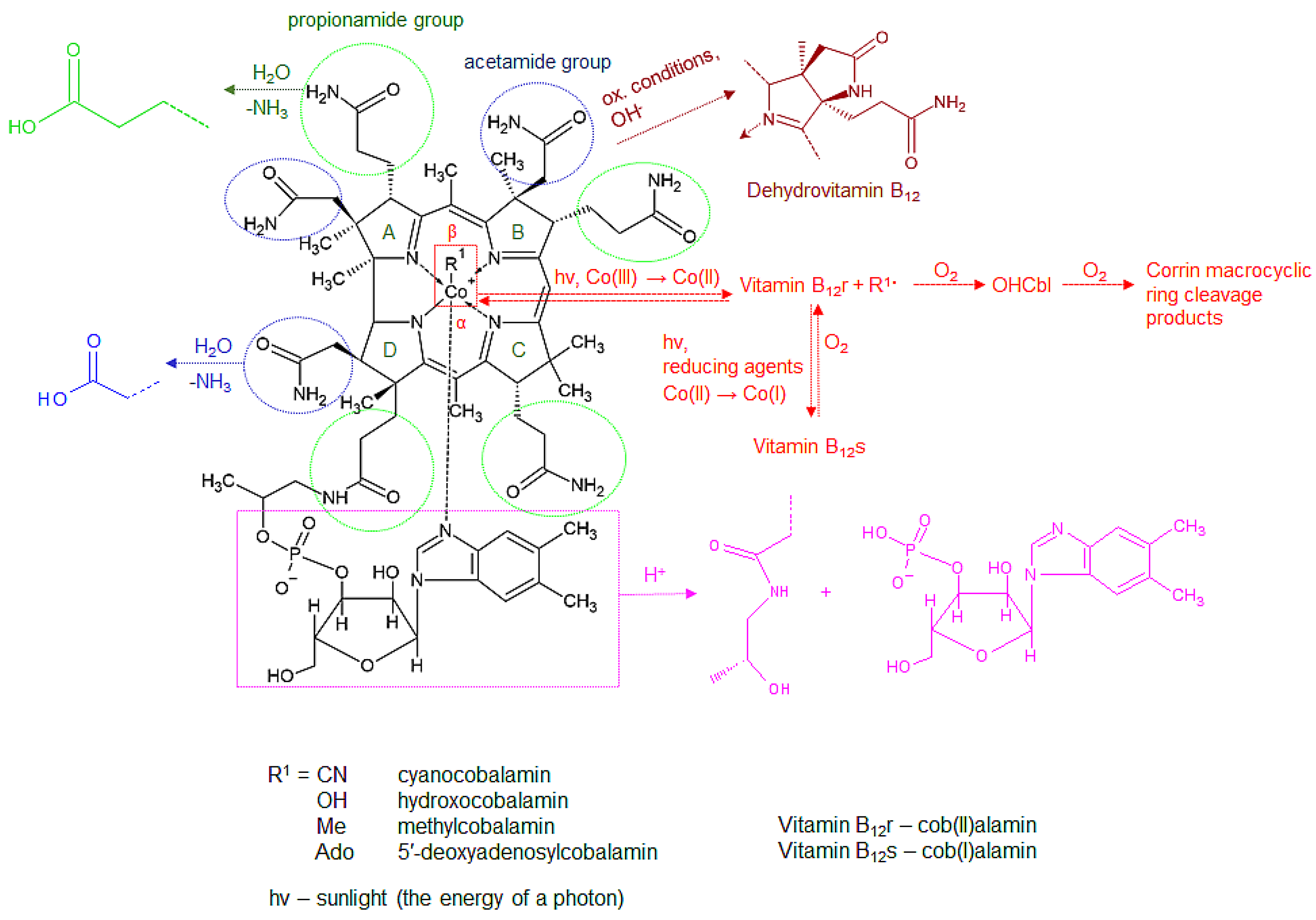
6. Chemistry and Reactivity of Vitamin B12
- Hydrolytic deamidation of the side chains
- Lactam formation
- Phosphate bond hydrolysis in the nucleotide moiety
- Reduction in the cobalt atom
- Cleavage the of β-ligand Co-C bond
7. Vitamin B12 Stability
7.1. Factors Affecting the Stability of Different Vitamin B12 Forms
7.1.1. Temperature
7.1.2. PH of the Solution
7.1.3. Exposure to Light
7.1.4. Presence of Oxidizing and Reducing Agents
7.2. Characteristic Interactions in Vitamin B12 Products
7.2.1. Vitamin B12—Reducing Sugars (Dextrose and Sucrose)
7.2.2. Vitamin B12—Riboflavin
7.2.3. Vitamin B12—Thiamine
7.2.4. Vitamin B12—Nicotinamide
7.2.5. Vitamin B12—Mixtures of Water-Soluble Vitamins
8. Vitamin B12 in Foods, Food Supplements, and Medicines
8.1. Vitamin B12 Stability in Foods
8.2. Vitamin B12 Stability in Food Supplements and Medicines
8.2.1. Vitamin B12 Stability in Liquid Dosage Forms
8.2.2. Vitamin B12 Stability in Solid Dosage Forms
8.3. Vitamin B12 Content in Fortified Foods, Food Supplements, and Medicines and Their Regulation
9. Strategies for Vitamin B12 Stabilization
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA) Scientific Opinion on Dietary Reference Values for Cobalamin (Vitamin B12). EFSA J. 2015, 13, 4150. [CrossRef] [Green Version]
- Kumar, N. Chapter 60-Neurologic Aspects of Cobalamin (B12) Deficiency. In Handbook of Clinical Neurology; Neurologic Aspects of Systemic Disease Part II; Biller, J., Ferro, J.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2014; Volume 120, pp. 915–926. [Google Scholar]
- Jägerstad, M.; Arkbåge, K. Cobalamins | Properties and Determination. In Encyclopedia of Food Sciences and Nutrition, 2nd ed.; Caballero, B., Ed.; Academic Press: Oxford, UK, 2003; pp. 1419–1427. ISBN 978-0-12-227055-0. [Google Scholar]
- Anes, J.M.; Beck, R.A.; Brink, J.J.; Goldberg, R.J. Nitritocobalamin and Nitrosocobalamin May Be Confused with Sulfitocobalamin Using Cation-Exchange Chromatography. J. Chromatogr. B Biomed. Appl. 1994, 660, 180–185. [Google Scholar] [CrossRef]
- Wiley, T.E.; Miller, N.A.; Miller, W.R.; Sofferman, D.L.; Lodowski, P.; Toda, M.J.; Jaworska, M.; Kozlowski, P.M.; Sension, R.J. Off to the Races: Comparison of Excited State Dynamics in Vitamin B12 Derivatives Hydroxocobalamin and Aquocobalamin. J. Phys. Chem. A 2018, 122, 6693–6703. [Google Scholar] [CrossRef]
- Watanabe, F. Vitamin B12 Sources and Bioavailability. Exp. Biol. Med. 2007, 232, 1266–1274. [Google Scholar] [CrossRef]
- Watanabe, F.; Bito, T. Vitamin B12 Sources and Microbial Interaction. Exp. Biol. Med. 2018, 243, 148–158. [Google Scholar] [CrossRef]
- Watanabe, F.; Yabuta, Y.; Bito, T.; Teng, F. Vitamin B₁₂-Containing Plant Food Sources for Vegetarians. Nutrients 2014, 6, 1861–1873. [Google Scholar] [CrossRef] [Green Version]
- Langan, R.C.; Goodbred, A.J. Vitamin B12 Deficiency: Recognition and Management. AFP 2017, 96, 384–389. [Google Scholar]
- Ryan-Harshman, M.; Aldoori, W. Vitamin B12 and Health. Can. Fam. Physician 2008, 54, 536–541. [Google Scholar]
- Schnellbaecher, A.; Binder, D.; Bellmaine, S.; Zimmer, A. Vitamins in Cell Culture Media: Stability and Stabilization Strategies. Biotechnol. Bioeng. 2019, 116, 1537–1555. [Google Scholar] [CrossRef] [Green Version]
- Commission Regulation (EC) No 1170/2009 of 30 November 2009 Amending Directive 2002/46/EC of the European Parliament and of Council and Regulation (EC) No 1925/2006 of the European Parliament and of the Council as Regards the Lists of Vitamin and Minerals and Their Forms That Can Be Added to Foods, Including Food Supplements (Text with EEA Relevance). Available online: https://www.legislation.gov.uk/eur/2009/1170/contents (accessed on 18 January 2022).
- Shipton, M.J.; Thachil, J. Vitamin B12 Deficiency—A 21st Century Perspective. Clin. Med. 2015, 15, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Romain, M.; Sviri, S.; Linton, D.M.; Stav, I.; van Heerden, P.V. The Role of Vitamin B12 in the Critically Ill—A Review. Anaesth. Intensive Care 2016, 44, 447–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, A.; Habeych, E.; Silva-Zolezzi, I.; Galaffu, N.; Allen, L.H. Methods to Assess Vitamin B12 Bioavailability and Technologies to Enhance Its Absorption. Nutr. Rev. 2018, 76, 778–792. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H. Causes of Vitamin B12 and Folate Deficiency. Food Nutr. Bull. 2008, 29, S20–S34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kozyraki, R.; Cases, O. Vitamin B12 Absorption: Mammalian Physiology and Acquired and Inherited Disorders. Biochimie 2013, 95, 1002–1007. [Google Scholar] [CrossRef]
- Randaccio, L.; Geremia, S.; Demitri, N.; Wuerges, J. Vitamin B12: Unique Metalorganic Compounds and the Most Complex Vitamins. Molecules 2010, 15, 3228–3259. [Google Scholar] [CrossRef] [Green Version]
- Schneider, Z.; Stroinski, A. Comprehensive B12: Chemistry, Biochemistry, Nutrition, Ecology, Medicine; Walter de Gruyter: Berlin, Germany; Boston, MA, USA, 2011; ISBN 978-3-11-084479-5. [Google Scholar]
- van Asselt, D.Z.B.; Merkus, F.W.H.M.; Russel, F.G.M.; Hoefnagels, W.H.L. Nasal Absorption of Hydroxocobalamin in Healthy Elderly Adults. Br. J. Clin. Pharmacol. 1998, 45, 83–86. [Google Scholar] [CrossRef] [Green Version]
- Nascobal® Nasal Spray (Cyanocobalamin, USP) 500 Mcg/Spray Pack Insert. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2005/021642lbl.pdf (accessed on 18 January 2022).
- Dave, H.; Agarwal, V.; Maseeh, A.; Patel, K. Novel Methylcobalamin Nasal Spray versus Intramuscular Injection: A Randomized, Crossover Comparative Bioavailability Study. Int. J. Endocrinol. Metabol. Dis. 2021, 7, 1–6. [Google Scholar] [CrossRef]
- Quadros, E.V.; Sequeira, J.M. Cellular Uptake of Cobalamin: Transcobalamin and the TCblR/CD320 Receptor. Biochimie 2013, 95, 1008–1018. [Google Scholar] [CrossRef] [Green Version]
- Mascarenhas, R.; Li, Z.; Gherasim, C.; Ruetz, M.; Banerjee, R. The Human B12 Trafficking Protein CblC Processes Nitrocobalamin. J. Biol. Chem. 2020, 295, 9630–9640. [Google Scholar] [CrossRef]
- Moreno-Garcia, M.A.; Rosenblatt, D.S.; Jerome-Majewska, L.A. Vitamin B12 Metabolism during Pregnancy and in Embryonic Mouse Models. Nutrients 2013, 5, 3531–3550. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Hannibal, L.; Gherasim, C.; Jacobsen, D.W.; Banerjee, R. A Human Vitamin B12 Trafficking Protein Uses Glutathione Transferase Activity for Processing Alkylcobalamins. J. Biol. Chem. 2009, 284, 33418–33424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, K.; Gherasim, C.; Banerjee, R.; Koutmos, M. Structure of Human B12 Trafficking Protein CblD Reveals Molecular Mimicry and Identifies a New Subfamily of Nitro-FMN Reductases. J. Biol. Chem. 2015, 290, 29155–29166. [Google Scholar] [CrossRef] [PubMed]
- Obeid, R.; Fedosov, S.N.; Nexo, E. Cobalamin Coenzyme Forms Are Not Likely to Be Superior to Cyano- and Hydroxyl-Cobalamin in Prevention or Treatment of Cobalamin Deficiency. Mol. Nutr. Food Res. 2015, 59, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Reizenstein, P.; Ek, G.; Matthews, C.M. Vitamin B12 Kinetics in Man. Implications on Total-Body-B12-Determinations, Human Requirements, and Normal and Pathological Cellular B12 Uptake. Phys. Med. Biol. 1966, 11, 295–306. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, F.; Samman, S. Vitamin B12 in Health and Disease. Nutrients 2010, 2, 299–316. [Google Scholar] [CrossRef] [Green Version]
- Wuerges, J.; Geremia, S.; Randaccio, L. Structural Study on Ligand Specificity of Human Vitamin B12 Transporters. Biochem. J. 2007, 403, 431–440. [Google Scholar] [CrossRef] [Green Version]
- Fedosov, S.N.; Grissom, C.B.; Fedosova, N.U.; Moestrup, S.K.; Nexø, E.; Petersen, T.E. Application of a fluorescent cobalamin analogue for analysis of the binding kinetics. A study employing recombinant human transcobalamin and intrinsic factor. FEBS J. 2006, 273, 4742–4753. [Google Scholar] [CrossRef]
- Wuerges, J.; Geremia, S.; Fedosov, S.N.; Randaccio, L. Vitamin B12 Transport Proteins: Crystallographic Analysis of Beta-Axial Ligand Substitutions in Cobalamin Bound to Transcobalamin. IUBMB Life 2007, 59, 722–729. [Google Scholar] [CrossRef] [Green Version]
- Siega, P.; Wuerges, J.; Arena, F.; Gianolio, E.; Fedosov, S.N.; Dreos, R.; Geremia, S.; Aime, S.; Randaccio, L. Release of Toxic Gd3+Ions to Tumour Cells by Vitamin B12 Bioconjugates. Chemistry 2009, 15, 7980–7989. [Google Scholar] [CrossRef] [Green Version]
- Wuerges, J.; Garau, G.; Geremia, S.; Fedosov, S.N.; Petersen, T.E.; Randaccio, L. Structural Basis for Mammalian Vitamin B12 Transport by Transcobalamin. Proc. Natl. Acad. Sci. USA 2006, 103, 4386–4391. [Google Scholar] [CrossRef] [Green Version]
- Lyon, P.; Strippoli, V.; Fang, B.; Cimmino, L. B Vitamins and One-Carbon Metabolism: Implications in Human Health and Disease. Nutrients 2020, 12, 2867. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.; Laganà, A.S.; Rapisarda, A.M.C.; La Ferrera, G.M.G.; Buscema, M.; Rossetti, P.; Nigro, A.; Muscia, V.; Valenti, G.; Sapia, F.; et al. Vitamin B12 among Vegetarians: Status, Assessment and Supplementation. Nutrients 2016, 8, 767. [Google Scholar] [CrossRef] [PubMed]
- Takahashi-Iñiguez, T.; García-Hernandez, E.; Arreguín-Espinosa, R.; Flores, M.E. Role of Vitamin B12 on Methylmalonyl-CoA Mutase Activity. J. Zhejiang. Univ. Sci. B 2012, 13, 423–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, R.C.; Brown, D.L. Vitamin B12 Deficiency. AFP 2003, 67, 979–986. [Google Scholar]
- Herrmann, W.; Obeid, R. Cobalamin Deficiency. Subcell. Biochem. 2012, 56, 301–322. [Google Scholar] [CrossRef]
- Miller, A.; Korem, M.; Almog, R.; Galboiz, Y. Vitamin B12, Demyelination, Remyelination and Repair in Multiple Sclerosis. J. Neurol. Sci. 2005, 233, 93–97. [Google Scholar] [CrossRef]
- Zelder, F. Recent Trends in the Development of Vitamin B12 Derivatives for Medicinal Applications. Chem. Commun. 2015, 51, 14004–14017. [Google Scholar] [CrossRef]
- Froese, D.S.; Fowler, B.; Baumgartner, M.R. Vitamin B12, Folate, and the Methionine Remethylation Cycle—Biochemistry, Pathways, and Regulation. J. Inherit. Metab. Dis. 2019, 42, 673–685. [Google Scholar] [CrossRef] [Green Version]
- Selhub, J. Folate, Vitamin B12 and Vitamin B6 and One Carbon Metabolism. J. Nutr. Health Aging 2002, 6, 39–42. [Google Scholar]
- Azzini, E.; Raguzzini, A.; Polito, A. A Brief Review on Vitamin B12 Deficiency Looking at Some Case Study Reports in Adults. Int. J. Mol. Sci. 2021, 22, 9694. [Google Scholar] [CrossRef]
- Green, R.; Allen, L.H.; Bjørke-Monsen, A.-L.; Brito, A.; Guéant, J.-L.; Miller, J.W.; Molloy, A.M.; Nexo, E.; Stabler, S.; Toh, B.-H.; et al. Vitamin B12 Deficiency. Nat. Rev. Dis. Primers 2017, 3, 17040. [Google Scholar] [CrossRef] [PubMed]
- Nalder, L.; Zheng, B.; Chiandet, G.; Middleton, L.T.; de Jager, C.A. Vitamin B12 and Folate Status in Cognitively Healthy Older Adults and Associations with Cognitive Performance. J. Nutr. Health Aging 2021, 25, 287–294. [Google Scholar] [CrossRef]
- Pawlak, R. Vitamin B12 Status Is a Risk Factor for Bone Fractures among Vegans. Med. Hypotheses 2021, 153, 110625. [Google Scholar] [CrossRef] [PubMed]
- Desmond, M.A.; Sobiecki, J.G.; Jaworski, M.; Płudowski, P.; Antoniewicz, J.; Shirley, M.K.; Eaton, S.; Książyk, J.; Cortina-Borja, M.; De Stavola, B.; et al. Growth, Body Composition, and Cardiovascular and Nutritional Risk of 5- to 10-y-Old Children Consuming Vegetarian, Vegan, or Omnivore Diets. Am. J. Clin. Nutr. 2021, 113, 1565–1577. [Google Scholar] [CrossRef] [PubMed]
- Saravanan, P.; Sukumar, N.; Adaikalakoteswari, A.; Goljan, I.; Venkataraman, H.; Gopinath, A.; Bagias, C.; Yajnik, C.S.; Stallard, N.; Ghebremichael-Weldeselassie, Y.; et al. Association of Maternal Vitamin B12 and Folate Levels in Early Pregnancy with Gestational Diabetes: A Prospective UK Cohort Study (PRiDE Study). Diabetologia 2021, 64, 2170–2182. [Google Scholar] [CrossRef]
- Behere, R.V.; Deshmukh, A.S.; Otiv, S.; Gupte, M.D.; Yajnik, C.S. Maternal Vitamin B12 Status During Pregnancy and Its Association with Outcomes of Pregnancy and Health of the Offspring: A Systematic Review and Implications for Policy in India. Front. Endocrinol. 2021, 12, 619176. [Google Scholar] [CrossRef]
- Rashid, S.; Meier, V.; Patrick, H. Review of Vitamin B12 Deficiency in Pregnancy: A Diagnosis Not to Miss as Veganism and Vegetarianism Become More Prevalent. Eur. J. Haematol. 2021, 106, 450–455. [Google Scholar] [CrossRef]
- Devalia, V.; Hamilton, M.S.; Molloy, A.M. British Committee for Standards in Haematology Guidelines for the Diagnosis and Treatment of Cobalamin and Folate Disorders. Br. J. Haematol. 2014, 166, 496–513. [Google Scholar] [CrossRef]
- Ströhle, A.; Richter, M.; González-Gross, M.; Neuhäuser-Berthold, M.; Wagner, K.-H.; Leschik-Bonnet, E.; Egert, S.; for the German Nutrition Society (DGE). The Revised D-A-CH-Reference Values for the Intake of Vitamin B12: Prevention of Deficiency and Beyond. Mol. Nutr. Food Res. 2019, 63, 1801178. [Google Scholar] [CrossRef] [Green Version]
- de Benoist, B. Conclusions of a WHO Technical Consultation on Folate and Vitamin B12 Deficiencies. Food Nutr. Bull. 2008, 29, S238–S244. [Google Scholar] [CrossRef]
- Pawlak, R.; Lester, S.E.; Babatunde, T. The Prevalence of Cobalamin Deficiency among Vegetarians Assessed by Serum Vitamin B12: A Review of Literature. Eur. J. Clin. Nutr. 2014, 68, 541–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mądry, E.; Lisowska, A.; Grebowiec, P.; Walkowiak, J. The Impact of Vegan Diet on B12 Status in Healthy Omnivores: Five-Year Prospective Study. Acta. Sci. Pol. Technol. Aliment. 2012, 11, 209–212. [Google Scholar] [PubMed]
- Office of Dietary Supplements-Vitamin B12. Available online: https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/ (accessed on 6 October 2022).
- Al Amin, A.S.M.; Gupta, V. Vitamin B12 (Cobalamin). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Bensky, M.J.; Ayalon-Dangur, I.; Ayalon-Dangur, R.; Naamany, E.; Gafter-Gvili, A.; Koren, G.; Shiber, S. Comparison of Sublingual vs. Intramuscular Administration of Vitamin B12 for the Treatment of Patients with Vitamin B12 Deficiency. Drug Deliv. Transl. Res. 2019, 9, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Estourgie-van Burk, G.F.; van der Kuy, P.H.M.; de Meij, T.G.; Benninga, M.A.; Kneepkens, C.M.F. Intranasal Treatment of Vitamin B12 Deficiency in Children. Eur. J. Pediatr. 2020, 179, 349–352. [Google Scholar] [CrossRef]
- Verma, D.; Chandra, J.; Kumar, P.; Shukla, S.; Sengupta, S. Efficacy of Oral Methylcobalamin in Treatment of Vitamin B12 Deficiency Anemia in Children. Pediatr. Blood. Cancer. 2017, 64, e26698. [Google Scholar] [CrossRef]
- Andrès, E.; Zulfiqar, A.-A.; Vogel, T. State of the Art Review: Oral and Nasal Vitamin B12 Therapy in the Elderly. QJM 2020, 113, 5–15. [Google Scholar] [CrossRef]
- Houle, S.K.D.; Kolber, M.R.; Chuck, A.W. Should Vitamin B12 Tablets Be Included in More Canadian Drug Formularies? An Economic Model of the Cost-Saving Potential from Increased Utilisation of Oral versus Intramuscular Vitamin B12 Maintenance Therapy for Alberta Seniors. BMJ Open 2014, 4, e004501. [Google Scholar] [CrossRef] [Green Version]
- Vidal-Alaball, J.; Butler, C.C.; Potter, C.C. Comparing Costs of Intramuscular and Oral Vitamin B12 Administration in Primary Care: A Cost-Minimization Analysis. Eur. J. Gen. Pr. 2006, 12, 169–173. [Google Scholar] [CrossRef]
- Sanz-Cuesta, T.; González-Escobar, P.; Riesgo-Fuertes, R.; Garrido-Elustondo, S.; del Cura-González, I.; Martín-Fernández, J.; Escortell-Mayor, E.; Rodríguez-Salvanés, F.; García-Solano, M.; González-González, R.; et al. Oral versus Intramuscular Administration of Vitamin B12 for the Treatment of Patients with Vitamin B12 Deficiency: A Pragmatic, Randomised, Multicentre, Non-Inferiority Clinical Trial Undertaken in the Primary Healthcare Setting (Project OB12). BMC Public Health 2012, 12, 394. [Google Scholar] [CrossRef] [Green Version]
- Bolaman, Z.; Kadikoylu, G.; Yukselen, V.; Yavasoglu, I.; Barutca, S.; Senturk, T. Oral versus Intramuscular Cobalamin Treatment in Megaloblastic Anemia: A Single-Center, Prospective, Randomized, Open-Label Study. Clin. Ther. 2003, 25, 3124–3134. [Google Scholar] [CrossRef]
- Kuzminski, A.M.; Del Giacco, E.J.; Allen, R.H.; Stabler, S.P.; Lindenbaum, J. Effective Treatment of Cobalamin Deficiency with Oral Cobalamin. Blood 1998, 92, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Castelli, M.C.; Friedman, K.; Sherry, J.; Brazzillo, K.; Genoble, L.; Bhargava, P.; Riley, M.G.I. Comparing the Efficacy and Tolerability of a New Daily Oral Vitamin B12 Formulation and Intermittent Intramuscular Vitamin B12 in Normalizing Low Cobalamin Levels: A Randomized, Open-Label, Parallel-Group Study. Clin. Ther. 2011, 33, 358–371.e2. [Google Scholar] [CrossRef] [PubMed]
- Saraswathy, A.; Dutta, A.; Simon, E.; Chacko, A. Randomized Open Label Trial Comparing Efficacy of Oral versus Intramuscular Vitamin B12 Supplementation for Treatment of Vitamin B12 Deficiency. Gastroenterology 2012, 142, S-216. [Google Scholar] [CrossRef]
- Sanz-Cuesta, T.; Escortell-Mayor, E.; Cura-Gonzalez, I.; Martin-Fernandez, J.; Riesgo-Fuertes, R.; Garrido-Elustondo, S.; Mariño-Suárez, J.E.; Álvarez-Villalba, M.; Gómez-Gascón, T.; González-García, I.; et al. Oral versus Intramuscular Administration of Vitamin B12 for Vitamin B12 Deficiency in Primary Care: A Pragmatic, Randomised, Non-Inferiority Clinical Trial (OB12). BMJ Open 2020, 10, e033687. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, L.; Qin, L.L.; Song, Y.; Vidal-Alaball, J.; Liu, T.H. Oral Vitamin B12 versus Intramuscular Vitamin B12 for Vitamin B12 Deficiency. Cochrane Database Syst. Rev. 2018, 2018, CD004655. [Google Scholar] [CrossRef]
- Masucci, L.; Goeree, R. Vitamin B12 Intramuscular Injections Versus Oral Supplements. Ont. Health Technol. Assess. Ser. 2013, 13, 1–24. [Google Scholar]
- van Walraven, C.; Austin, P.; Naylor, C.D. Vitamin B12 Injections versus Oral Supplements. How Much Money Could Be Saved by Switching from Injections to Pills? Can. Fam. Physician 2001, 47, 79–86. [Google Scholar]
- Vidal-Alaball, J.; Butler, C.C.; Cannings-John, R.; Goringe, A.; Hood, K.; McCaddon, A.; McDowell, I.; Papaioannou, A. Oral Vitamin B12 versus Intramuscular Vitamin B12 for Vitamin B12 Deficiency. Cochrane Database Syst. Rev. 2005, 23, CD004655. [Google Scholar] [CrossRef] [Green Version]
- Tugba-Kartal, A.; Cagla-Mutlu, Z. Comparison of Sublingual and Intramuscular Administration of Vitamin B12 for the Treatment of Vitamin B12 Deficiency in Children. RIC 2021, 72, 4648. [Google Scholar] [CrossRef]
- Orhan Kiliç, B.; Kiliç, S.; Şahin Eroğlu, E.; Gül, E.; Belen Apak, F.B. Sublingual Methylcobalamin Treatment Is as Effective as Intramuscular and Peroral Cyanocobalamin in Children Age 0–3 Years. Hematology 2021, 26, 1013–1017. [Google Scholar] [CrossRef]
- Varkal, M.A.; Karabocuoglu, M. Efficiency of the Sublingual Route in Treating B12 Deficiency in Infants. Int. J. Vitam. Nutr. Res. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sharabi, A.; Cohen, E.; Sulkes, J.; Garty, M. Replacement Therapy for Vitamin B12 Deficiency: Comparison between the Sublingual and Oral Route. Br. J. Clin. Pharmacol. 2003, 56, 635–638. [Google Scholar] [CrossRef] [PubMed]
- Parry-Strong, A.; Langdana, F.; Haeusler, S.; Weatherall, M.; Krebs, J. Sublingual Vitamin B12 Compared to Intramuscular Injection in Patients with Type 2 Diabetes Treated with Metformin: A Randomised Trial. N. Z. Med. J. 2016, 129, 67–75. [Google Scholar] [PubMed]
- Del Bo’, C.; Riso, P.; Gardana, C.; Brusamolino, A.; Battezzati, A.; Ciappellano, S. Effect of Two Different Sublingual Dosages of Vitamin B12 on Cobalamin Nutritional Status in Vegans and Vegetarians with a Marginal Deficiency: A Randomized Controlled Trial. Clin. Nutr. 2019, 38, 575–583. [Google Scholar] [CrossRef] [Green Version]
- van Campen, C.L.M.; Riepma, K.; Visser, F.C. Open Trial of Vitamin B12 Nasal Drops in Adults with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Comparison of Responders and Non-Responders. Front. Pharmacol. 2019, 10, 1102. [Google Scholar] [CrossRef] [Green Version]
- Tillemans, M.P.H.; Donders, E.M.V.J.; Verweij, S.L.; Van der Hoeven, R.T.M.; Kalisvaart, K.J. Effect of Administration Route on the Pharmacokinetics of Cobalamin in Elderly Patients: A Randomized Controlled Trial. Curr. Ther. Res. Clin. Exp. 2014, 76, 21–25. [Google Scholar] [CrossRef]
- Randaccio, L.; Geremia, S.; Wuerges, J. Crystallography of Vitamin B12 Proteins. J. Organomet. Chem. 2007, 692, 1198–1215. [Google Scholar] [CrossRef]
- Paul, C.; Brady, D.M. Comparative Bioavailability and Utilization of Particular Forms of B12 Supplements with Potential to Mitigate B12-Related Genetic Polymorphisms. Integr. Med. 2017, 16, 42–49. [Google Scholar]
- European Food Safety Authority (EFSA). 5′-Deoxyadenosylcobalamin and Methylcobalamin as Sources for Vitamin B12 Added as a Nutritional Substance in Food Supplements-Scientific Opinion of the Scientific Panel on Food Additives and Nutrient Sources Added to Food. EFSA J. 2008, 6, 815. [Google Scholar] [CrossRef]
- Gräsbeck, R. Hooked to Vitamin B12 since 1955: A Historical Perspective. Biochimie 2013, 95, 970–975. [Google Scholar] [CrossRef]
- Yazaki, Y.; Chow, G.; Mattie, M. A Single-Center, Double-Blinded, Randomized Controlled Study to Evaluate the Relative Efficacy of Sublingual and Oral Vitamin B-Complex Administration in Reducing Total Serum Homocysteine Levels. J. Altern. Complement. Med. 2006, 12, 881–885. [Google Scholar] [CrossRef] [Green Version]
- Stabler, S.P. Clinical Practice. Vitamin B12 Deficiency. N. Engl. J. Med. 2013, 368, 149–160. [Google Scholar] [CrossRef]
- Seetharam, B.; Yammani, R.R. Cobalamin Transport Proteins and Their Cell-Surface Receptors. Expert Rev. Mol. Med. 2003, 5, 1–18. [Google Scholar] [CrossRef]
- Fedosov, S.N.; Berglund, L.; Fedosova, N.U.; Nexø, E.; Petersen, T.E. Comparative Analysis of Cobalamin Binding Kinetics and Ligand Protection for Intrinsic Factor, Transcobalamin, and Haptocorrin. J. Biol. Chem. 2002, 277, 9989–9996. [Google Scholar] [CrossRef] [Green Version]
- Hippe, E. Changes in Stokes Radius on Binding of Vitamin B12 to Human Intrinsic Factor and Transcobalamins. Biochim. BioPhys. Acta 1970, 208, 337–339. [Google Scholar] [CrossRef]
- Gruber, K.; Puffer, B.; Kräutler, B. Vitamin B12-Derivatives—Enzyme Cofactors and Ligands of Proteins and Nucleic Acids. Chem. Soc. Rev. 2011, 40, 4346–4363. [Google Scholar] [CrossRef]
- Gailus, S.; Höhne, W.; Gasnier, B.; Nürnberg, P.; Fowler, B.; Rutsch, F. Insights into Lysosomal Cobalamin Trafficking: Lessons Learned from CblF Disease. J. Mol. Med. 2010, 88, 459–466. [Google Scholar] [CrossRef]
- Rutsch, F.; Gailus, S.; Miousse, I.R.; Suormala, T.; Sagné, C.; Toliat, M.R.; Nürnberg, G.; Wittkampf, T.; Buers, I.; Sharifi, A.; et al. Identification of a Putative Lysosomal Cobalamin Exporter Altered in the CblF Defect of Vitamin B12 Metabolism. Nat. Genet. 2009, 41, 234–239. [Google Scholar] [CrossRef]
- Oladipo, O.; Rosenblatt, D.S.; Watkins, D.; Miousse, I.R.; Sprietsma, L.; Dietzen, D.J.; Shinawi, M. Cobalamin F Disease Detected by Newborn Screening and Follow-up on a 14-Year-Old Patient. Pediatrics 2011, 128, e1636–e1640. [Google Scholar] [CrossRef]
- Waggoner, D.J.; Ueda, K.; Mantia, C.; Dowton, S.B. Methylmalonic Aciduria (CblF): Case Report and Response to Therapy. Am. J. Med. Genet. 1998, 79, 373–375. [Google Scholar] [CrossRef]
- Chu, R.C.; Begley, J.A.; Colligan, P.D.; Hall, C.A. The Methylcobalamin Metabolism of Cultured Human Fibroblasts. Metabolism 1993, 42, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Gherasim, C.; Lofgren, M.; Banerjee, R. Navigating the B12 Road: Assimilation, Delivery, and Disorders of Cobalamin. J. Biol. Chem. 2013, 288, 13186–13193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quadros, E.V.; Jackson, B.; Hoffbrand, A.V.; Linnell, J.C. Interconversion of Cobalamins in Human Lymphocytes in Vitro and the Influence of Nitrous Oxide on Synthesis of Cobalamin Coenzymes. In Interconversion of Cobalamins in Human Lymphocytes In Vitro and the Influence of Nitrous Oxide on Synthesis of Cobalamin Coenzymes; De Gruyter: Berlin, Germany, 2019; pp. 1045–1054. ISBN 978-3-11-151082-8. [Google Scholar]
- Banerjee, R. B12 Trafficking in Mammals: A for Coenzyme Escort Service. ACS Chem. Biol. 2006, 1, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Quadros, E.V. Advances in the Understanding of Cobalamin Assimilation and Metabolism. Br. J. Haematol. 2010, 148, 195–204. [Google Scholar] [CrossRef] [Green Version]
- Kacpura, A.; Frigeni, M.; Gunther, K.; Farach, L. Clinical and Biochemical Outcomes in Cobalamin C Deficiency with Use of High-Dose Hydroxocobalamin in the Early Neonatal Period. Am. J. Med. Genet. A 2022, 188, 1831–1835. [Google Scholar] [CrossRef]
- Andersson, H.C.; Shapira, E. Biochemical and Clinical Response to Hydroxocobalamin versus Cyanocobalamin Treatment in Patients with Methylmalonic Acidemia and Homocystinuria (CblC). J. Pediatr. 1998, 132, 121–124. [Google Scholar] [CrossRef]
- Higashimoto, T.; Kim, A.Y.; Ogawa, J.T.; Sloan, J.L.; Almuqbil, M.A.; Carlson, J.M.; Manoli, I.; Venditti, C.P.; Gunay-Aygun, M.; Wang, T. High-dose Hydroxocobalamin Achieves Biochemical Correction and Improvement of Neuropsychiatric Deficits in Adults with Late Onset Cobalamin C Deficiency. JIMD Rep. 2019, 51, 17–24. [Google Scholar] [CrossRef]
- Carrillo-Carrasco, N.; Chandler, R.J.; Venditti, C.P. Combined Methylmalonic Acidemia and Homocystinuria, CblC Type. I. Clinical Presentations, Diagnosis and Management. J. Inherit. Metab. Dis. 2012, 35, 91–102. [Google Scholar] [CrossRef] [Green Version]
- Carrillo-Carrasco, N.; Sloan, J.; Valle, D.; Hamosh, A.; Venditti, C.P. Hydroxocobalamin Dose Escalation Improves Metabolic Control in CblC. J. Inherit. Metab. Dis. 2009, 32, 728–731. [Google Scholar] [CrossRef] [Green Version]
- Carrillo-Carrasco, N.; Venditti, C.P. Combined Methylmalonic Acidemia and Homocystinuria, CblC Type. II. Complications, Pathophysiology, and Outcomes. J. Inherit. Metab. Dis. 2012, 35, 103–114. [Google Scholar] [CrossRef] [Green Version]
- Froese, D.S.; Zhang, J.; Healy, S.; Gravel, R.A. Mechanism of Vitamin B12-Responsiveness in CblC Methylmalonic Aciduria with Homocystinuria. Mol. Genet. Metab. 2009, 98, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.N.; Shinton, N.K. Comparison of Hydroxocobalamin and Cyanocobalamin in the Treatment of Pernicious Anaemia. Lancet 1965, 2, 1305–1308. [Google Scholar] [CrossRef]
- Okuda, K.; Yashima, K.; Kitazaki, T.; Takara, I. Intestinal Absorption and Concurrent Chemical Changes of Methylcobalamin. J. Lab. Clin. Med. 1973, 81, 557–567. [Google Scholar] [PubMed]
- Freeman, A.G. Hydroxocobalamin versus Cyanocobalamin. J. R. Soc. Med. 1996, 89, 659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foulds, W.S.; Freeman, A.G.; Phillips, C.I.; Wilson, J. Cyanocobalamin: A Case for Withdrawal. Lancet 1970, 1, 35. [Google Scholar] [CrossRef]
- Carmel, R. Efficacy and Safety of Fortification and Supplementation with Vitamin B12: Biochemical and Physiological Effects. Food Nutr. Bull. 2008, 29, S177–S187. [Google Scholar] [CrossRef] [Green Version]
- Green, R. Cobalamins. In Encyclopedia of Human Nutrition, 2nd ed.; Caballero, B., Ed.; Elsevier: Oxford, UK, 2005; pp. 401–407. ISBN 978-0-12-226694-2. [Google Scholar]
- Kräutler, B. Biochemistry of B12-Cofactors in Human Metabolism. In Water Soluble Vitamins: Clinical Research and Future Application; Stanger, O., Ed.; Subcellular Biochemistry; Springer: Dordrecht, The Netherlands, 2012; pp. 323–346. ISBN 978-94-007-2199-9. [Google Scholar]
- Rucker, R.B.; Zempleni, J.; Suttie, J.W.; McCormick, D.B. Handbook of Vitamins, 4th ed.; Taylor & Francis: Oxford, UK, 2007; ISBN 978-0-8493-4022-2. [Google Scholar]
- Bonnett, R. The Chemistry of the Vitamin B12 Group. Chem. Rev. 1963, 63, 573–605. [Google Scholar] [CrossRef]
- ó Proinsias, K.; Giedyk, M.; Gryko, D. Vitamin B12: Chemical Modifications. Chem. Soc. Rev. 2013, 42, 6605–6619. [Google Scholar] [CrossRef]
- Giedyk, M.; Goliszewska, K.; Gryko, D. Vitamin B12 Catalysed Reactions. Chem. Soc. Rev. 2015, 44, 3391–3404. [Google Scholar] [CrossRef] [Green Version]
- Hogenkamp, H.P.C.; Barker, H.A.; Mason, H.S. An Electron-Spin Resonance Study of Coenzyme B12. Arch. Biochem. BioPhys. 1963, 100, 353–359. [Google Scholar] [CrossRef]
- Ahmad, I.; Qadeer, K.; Zahid, S.; Sheraz, M.A.; Ismail, T.; Hussain, W.; Ansari, I.A. Effect of Ascorbic Acid on the Degradation of Cyanocobalamin and Hydroxocobalamin in Aqueous Solution: A Kinetic Study. AAPS PharmSciTech 2014, 15, 1324–1333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banerjee, R. The Yin-Yang of Cobalamin Biochemistry. Chem. Biol. 1997, 4, 175–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamun, A.A.; Toda, M.J.; Lodowski, P.; Kozlowski, P.M. Photolytic Cleavage of Co–C Bond in Coenzyme B12-Dependent Glutamate Mutase. J. Phys. Chem. B 2019, 123, 2585–2598. [Google Scholar] [CrossRef] [PubMed]
- Jensen, K.P.; Ryde, U. How the Co−C Bond Is Cleaved in Coenzyme B12 Enzymes: A Theoretical Study. J. Am. Chem. Soc. 2005, 127, 9117–9128. [Google Scholar] [CrossRef]
- Trenner, N.R.; Buhs, R.P.; Bacher, F.A.; Gakenheimer, W.C. A Note Concerning the Incompatibility of Vitamin B12 and Ascorbic Acid. J. Am. Pharm. Assoc. 1950, 39, 361. [Google Scholar] [CrossRef]
- Bartilucci, A.J.; Digirolamo, R.; Eisen, H. Cyanocobalamin (Vitamin B12). II. Further Studies of the Effect of Ascorbic Acid Degradation Products on Cyanocobalamin. J. Am. Pharm. Assoc. 1958, 47, 42–43. [Google Scholar] [CrossRef]
- Rosenberg, A.J. The Copper-Promoted Decomposition of Vitamin B12 in Solutions of Ascorbic Acid. J. Biol. Chem. 1956, 219, 951–956. [Google Scholar] [CrossRef]
- Gakenheimer, W.C.; Feller, B.A. A Note on a Preliminary Observation of the Incompatibility of Vitamin B12 and Ascorbic Acid. J. Am. Pharm. Assoc. 1949, 38, 660. [Google Scholar] [CrossRef]
- Bartilucci, A.; Foss, N.E. Cyanocobalamin (Vitamin B12). I. A Study of the Stability of Cyanocobalamin and Ascorbic Acid in Liquid Formulations. J. Am. Pharm. Assoc. 1954, 43, 159–162. [Google Scholar] [CrossRef]
- Vitamin B12: A Review of Analytical Methods for Use in Food. Available online: https://www.gov.uk/government/publications/vitamin-b12-a-review-of-analytical-methods-for-use-in-food (accessed on 25 April 2022).
- Zironi, E.; Gazzotti, T.; Barbarossa, A.; Devicienti, C.; Scardilli, M.; Pagliuca, G. Technical Note: Development and Validation of a Method Using Ultra Performance Liquid Chromatography Coupled with Tandem Mass Spectrometry for Determination of Vitamin B12 Concentrations in Milk and Dairy Products. J. Dairy Sci. 2013, 96, 2832–2836. [Google Scholar] [CrossRef] [Green Version]
- Qiu, X.; Zhang, H.; Yin, Y.; Brandes, H.; Marsala, T.; Stenerson, K.; Cramer, H.; You, H. Determination of Active Vitamin B12 (Cobalamin) in Dietary Supplements and Ingredients by Reversed-Phase Liquid Chromatography: Single-Laboratory Validation. Food Chem. 2019, 298, 125010. [Google Scholar] [CrossRef]
- Kamath, A.; Pemminati, S. Methylcobalamin in Vitamin B12 Deficiency: To Give or Not to Give? J. Pharmacol. Pharmacother. 2017, 8, 33–34. [Google Scholar] [CrossRef] [Green Version]
- Cyanocobalamin Safety Data Sheet; Product No.: PHR1234; CAS-No.: 68-19-9; Merck Ife Science S.r.l.: Milano, Italy, 2021.
- Coenzyme B12 Safety Data Sheet; Product No.: C0884; CAS-No.: 13870-90-1; Merck Life Science S.r.l.: Milano, Italy, 2022.
- Hydroxocobalamin Acetate Safety Data Sheet; Product No.: H8017; CAS-No.: 22465-48-1; Merck Life Science S.r.l.: Milano, Italy, 2022.
- Methylcobalamin Safety Data Sheet; Product No.: M9756; CAS-No.: 13422-55-4; Merck Life Science S.r.l.: Milano, Italy, 2022.
- Cyanocobalamin Certified Reference Material Certificate of Analysis; Catalog No.: PHR1234; LOT No.: P500234; Fluca Analytical, Sigma-Aldrich RTC, Inc.: Laramie, WY, USA, 2022.
- Council of Europe. European Pharmacopoeia, 10th ed.; Council of Europe: Strasbourg, France, 2020. [Google Scholar]
- Temova Rakuša, Ž.; Grobin, A.; Roškar, R. A Comprehensive Approach for the Simultaneous Analysis of All Main Water-Soluble Vitamins in Multivitamin Preparations by a Stability-Indicating HPLC-DAD Method. Food Chem. 2021, 337, 127768. [Google Scholar] [CrossRef]
- Bajaj, S.R.; Singhal, R.S. Degradation Kinetics of Vitamin B12 in Model Systems of Different PH and Extrapolation to Carrot and Lime Juices. J. Food Eng. 2020, 272, 109800. [Google Scholar] [CrossRef]
- CYANOKIT® (Hydroxocobalamin for Injection) for Intravenous Infusion. Highlights of Prescribing Information; Merck Santé s.a.s.: Semoy, France, 2018.
- Mander, L.; Liu, H.W. Comprehensive Natural Products II: Chemistry and Biology, Volumes 1−10. J. Am. Chem. Soc. 2010, 132, 9929. [Google Scholar] [CrossRef]
- Hadinata Lie, A.; Chandra-Hioe, M.V.; Arcot, J. Sorbitol Enhances the Physicochemical Stability of B12 Vitamers. Int. J. Vitam. Nutr. Res. 2020, 90, 439–447. [Google Scholar] [CrossRef]
- Brown, K.L. Chemistry and Enzymology of Vitamin B12. Chem. Rev. 2005, 105, 2075–2150. [Google Scholar] [CrossRef]
- Brown, K.L.; Zou, X. Thermolysis of Coenzymes B12 at Physiological Temperatures: Activation Parameters for Cobalt-Carbon Bond Homolysis and a Quantitative Analysis of the Perturbation of the Homolysis Equilibrium by the Ribonucleoside Triphosphate Reductase from Lactobacillus Leichmannii. J. Inorg. Biochem. 1999, 77, 185–195. [Google Scholar] [CrossRef]
- Combs, G.F. Poglavje 1: Chemical and Physiological Properties of Vitamins. V. In The Vitamins: Fundamental Aspects in Nutrition and Health, 3rd ed.; Elsevier Academic Press: Amsterdam, The Netherlands, 2008; pp. 503–514. [Google Scholar]
- Yessaad, M.; Bernard, L.; Bourdeaux, D.; Chennell, P.; Sautou, V. Development of a Stability Indicating Method for Simultaneous Analysis of Five Water-Soluble Vitamins by Liquid Chromatography. Pharm. Technol. Hosp. Pharm. 2018, 3, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Monajjemzadeh, F.; Ebrahimi, F.; Zakeri-Milani, P.; Valizadeh, H. Effects of Formulation Variables and Storage Conditions on Light Protected Vitamin B12 Mixed Parenteral Formulations. Adv. Pharm. Bull. 2014, 4, 329–338. [Google Scholar] [CrossRef]
- Ahmad, I.; Hussain, W. Stability of Cyanocobalamin in Parenteral Preparations. Pak. J. Pharm. Sci. 1993, 6, 53–59. [Google Scholar] [PubMed]
- British Pharmacopoeia Commission Office: Medicines and Healthcare products Regulatory Agency. British Pharmacopoeia 2020; Crown Copyright 2019: London, UK, 2020. [Google Scholar]
- Convention, U.S.P. The United States Pharmacopeia: USP 44-NF 39; United States Pharmacopeial Convention Inc.: Washington, DC, USA, 2021; ISBN 978-1-889788-39-5. [Google Scholar]
- Randaccio, L.; Geremia, S.; Nardin, G.; Wuerges, J. X-Ray Structural Chemistry of Cobalamins. Coord. Chem. Rev. 2006, 11–12, 1332–1350. [Google Scholar] [CrossRef]
- Demerre, L.J.; Wilson, C. Photolysis of Vitamin B12. J. Am. Pharm. Assoc. 1956, 45, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Andruniów, T.; Lodowski, P.; Garabato, B.D.; Jaworska, M.; Kozlowski, P.M. The Role of Spin-Orbit Coupling in the Photolysis of Methylcobalamin. J. Chem. Phys. 2016, 144, 124305. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, A.P.; Lodowski, P.; Kozlowski, P.M. Aerobic Photolysis of Methylcobalamin: Unraveling the Photoreaction Mechanism. Phys. Chem. Chem. Phys. 2022, 24, 6093–6106. [Google Scholar] [CrossRef] [PubMed]
- Kozlowski, P.M.; Garabato, B.D.; Lodowski, P.; Jaworska, M. Photolytic Properties of Cobalamins: A Theoretical Perspective. Dalton Trans. 2016, 45, 4457–4470. [Google Scholar] [CrossRef]
- Hogenkamp, H.P.C. The Photolysis of Methylcobalamin. Biochemistry 1966, 5, 417–422. [Google Scholar] [CrossRef]
- Yamada, R.; Shimizu, S.; Fukui, S. Formation of Vitamin B12s by Anaerobic Photolysis of Cobalt-Alkylcobalamins. Biochim. BioPhys. Acta 1966, 124, 197–200. [Google Scholar] [CrossRef]
- Ahmad, I.; Hussain, W.; Fareedi, A.A. Photolysis of Cyanocobalamin in Aqueous Solution. J. Pharm. Biomed. Anal. 1992, 10, 9–15. [Google Scholar] [CrossRef]
- Lodowski, P.; Jaworska, M.; Garabato, B.D.; Kozlowski, P.M. Mechanism of Co-C Bond Photolysis in Methylcobalamin: Influence of Axial Base. J. Phys. Chem. A 2015, 119, 3913–3928. [Google Scholar] [CrossRef]
- Qadeer, K.; Arsalan, A.; Ahmad, I.; Fatima, K.; Anwar, Z.; Ahmed, S.; Khattak, S.u.R.; Mahmud, S. Photochemical Interaction of Cyanocobalamin and Hydroxocobalamin with Cysteine. J. Mol. Struct. 2021, 1228, 129441. [Google Scholar] [CrossRef]
- Juzeniene, A.; Nizauskaite, Z. Photodegradation of Cobalamins in Aqueous Solutions and in Human Blood. J. Photochem. PhotoBiol. B Biol. 2013, 122, 7–14. [Google Scholar] [CrossRef]
- Vaid, F.H.M.; Zahid, S.; Faiyaz, A.; Qadeer, K.; Gul, W.; Anwar, Z.; Ahmad, I. Photolysis of Methylcobalamin in Aqueous Solution: A Kinetic Study. J. Photochem. PhotoBiol. A Chem. 2018, 362, 40–48. [Google Scholar] [CrossRef]
- Jones, A.R. The Photochemistry and Photobiology of Vitamin B12. Photochem. PhotoBiol. Sci. 2017, 16, 820–834. [Google Scholar] [CrossRef]
- Ahmed, L.M.; Saaed, S.I.; Marhoon, A.A. Effect of Oxidation Agents on Photo-Decolorization of Vitamin B12 in the Presence of ZnO/UV-A System. Indones. J. Chem. 2018, 18, 272–278. [Google Scholar] [CrossRef]
- Hunt, A.P. Kinetic and Mechanistic Studies on the Reaction of the Reduced Vitamin B12 Complex Cob(II)Alamin with Hydrogen Peroxide. Undergraduate Thesis, Kent State University, Kent, OH, USA, 2013. OhioLINK Electronic Theses and Dissertations Center. Available online: https://rave.ohiolink.edu/etdc/view?acc_num=ksuhonors1367864401 (accessed on 6 June 2022). OhioLINK Electronic Theses and Dissertations Center.
- Dubnoff, J.W. A Cobalamin Glutathione Complex. Biochem. BioPhys. Res. Commun. 1964, 16, 484–488. [Google Scholar] [CrossRef]
- Jacobsen, D.W.; Troxell, L.S.; Brown, K.L. Catalysis of Thiol Oxidation by Cobalamins and Cobinamides: Reaction Products and Kinetics. Biochemistry 1984, 23, 2017–2025. [Google Scholar] [CrossRef]
- Chiu, P.-C.; Reinhard, M. Transformation of Carbon Tetrachloride by Reduced Vitamin B12 in Aqueous Cysteine Solution. Environ. Sci. Technol. 1996, 30, 1882–1889. [Google Scholar] [CrossRef]
- Rodgers, Z.L.; Shell, T.A.; Brugh, A.M.; Nowotarski, H.L.; Forbes, M.D.E.; Lawrence, D.S. Fluorophore Assisted Photolysis of Thiolato-Cob(III)Alamins. Inorg. Chem. 2016, 55, 1962–1969. [Google Scholar] [CrossRef] [Green Version]
- Cavallini, D.; Scandurra, R.; Barboni, E.; Marcucci, M. The Inability of Thiols to Reduce Cobalamins in the Absence of a Metalion. FEBS Lett. 1968, 1, 272–274. [Google Scholar] [CrossRef] [Green Version]
- Randaccio, L.; Geremia, S.; Nardin, G.; Šlouf, M.; Srnova, I. Crystal Chemistry of Cobalamins. Structural Characterization of the Co−S Bond in Cobalamins. Inorg. Chem. 1999, 38, 4087–4092. [Google Scholar] [CrossRef]
- Hogenkamp, H.P.; Bratt, G.T.; Kotchevar, A.T. Reaction of Alkylcobalamins with Thiols. Biochemistry 1987, 26, 4723–4727. [Google Scholar] [CrossRef]
- Hogenkamp, H.P.C. The Interaction between Vitamin B12 and Vitamin C. Am. J. Clin. Nutr. 1980, 33, 1–3. [Google Scholar] [CrossRef]
- Macek, T.J. Stability Problems with Some Vitamins in Pharmaceuticals. Am. J. Pharm. Sci. Support. Public Health 1960, 132, 433–455. [Google Scholar]
- Nazhat, N.B.; Golding, B.T.; Johnson, G.R.A.; Jones, P. Destruction of Vitamin B12 by Reaction with Ascorbate: The Role of Hydrogen Peroxide and the Oxidation State of Cobalt. J. Inorg. Biochem. 1989, 36, 75–81. [Google Scholar] [CrossRef]
- Ahmad, I.; Qadeer, K.; Hafeez, A.; Zahid, S.; Sheraz, M.A.; ur Rehman Khattak, S. Effect of Ascorbic Acid on the Photolysis of Cyanocobalamin and Aquocobalamin/Hydroxocobalamin in Aqueous Solution: A Kinetic Study. J. Photochem. PhotoBiol. A Chem. 2017, 332, 92–100. [Google Scholar] [CrossRef]
- Hutchins, H.H.; Cravioto, P.J.; Macek, T.J. A Comparison of the Stability of Cyanocobalamin and Its Analogs in Ascorbate Solution. J. Am. Pharm. Assoc. 1956, 45, 806–808. [Google Scholar] [CrossRef]
- Lee, W.; Lee, Y.-B.; Huh, M.H.; Choi, J.K. Determination of the Chemical Stability of Cyanocobalamin in Medical Food by a Validated Immunoaffinity Column-Linked HPLC Method. J. Food. Qual. 2022, 2022, e1619936. [Google Scholar] [CrossRef]
- van der Merwe, J.; Steenekamp, J.; Steyn, D.; Hamman, J. The Role of Functional Excipients in Solid Oral Dosage Forms to Overcome Poor Drug Dissolution and Bioavailability. Pharmaceutics 2020, 12, 393. [Google Scholar] [CrossRef]
- Akers, M.J. Excipient-Drug Interactions in Parenteral Formulations. J. Pharm. Sci. 2002, 91, 2283–2300. [Google Scholar] [CrossRef]
- Barr, M.; Robert Kohn, S.; Tice, L.F. The Effect of Various Sugars and Polyols on the Stability of Vitamin B12. J. Am. Pharm. Assoc. 1957, 46, 650–652. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, D.R.; Libardi, S.H.; Skibsted, L.H. Riboflavin as a Photosensitizer. Effects on Human Health and Food Quality. Food Funct. 2012, 3, 487–502. [Google Scholar] [CrossRef] [PubMed]
- Ansari, I.A.; Vaid, F.H.M.; Ahmad, I. Spectral Study of Photolysis of Aqueous Cyanocobalamin Solutions in Presence of Vitamins B and C. Pak. J. Pharm. Sci. 2004, 17, 93–99. [Google Scholar] [PubMed]
- Ahmad, I.; Hussain, W. Multicomponent Spectrophotometric Assay of Cyanocobalamin, Hydroxocobalamin and Riboflavin. Pak. J. Pharm. Sci. 1992, 5, 121–127. [Google Scholar]
- Ahmad, I.; Hafeez, A.; Akhter, N.; HM Vaid, F.; Qadeer, K. Effect of Riboflavin on the Photolysis of Cyanocobolamin in Aqueous Solution. Open Anal. Chem. J. 2012, 6, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Feller, B.A.; Macek, T.J. Effect of Thiamine Hydrochloride on the Stability of Solutions of Crystalline Vitamin B12. J. Am. Pharm. Assoc. 1955, 44, 662–665. [Google Scholar] [CrossRef]
- Mukherjee, S.L.; Sen, S.P. Stability of Vitamin B12. Part II. Protection by an Iron Salt Against Destruction by Aneurine and Nicotinamide. J. Pharm. Pharmacol. 1959, 11, 26–31. [Google Scholar] [CrossRef]
- Doerge, R.F.; Ravin, L.J.; Caldwell, H.C. Effect of the Thiazole Moiety of Thiamine Hydrochloride and Selected Model Compounds on Cyanocobalamin Stability. J. Pharm. Sci. 1965, 54, 1038–1040. [Google Scholar] [CrossRef]
- Blitz, M.; Eigen, E.; Gunsberg, E. Vitamin B12 Studies-The Instability of Vitamin B12 in the Presence of Thiamine and Niacinamide. J. Am. Pharm. Assoc. 1954, 43, 651–653. [Google Scholar] [CrossRef]
- Gambier, A.S.; Rahn, E.P.G. Vitamin B12 in the Presence of Vitamin B1 and Niacinamide in Aqueous Combinations. J. Am. Pharm. Assoc. 1958, 47, 356–359. [Google Scholar] [CrossRef]
- Ahmad, I.; Ansari, I.A.; Ismail, T. Effect of Nicotinamide on the Photolysis of Cyanocobalamin in Aqueous Solution. J. Pharm. Biomed. Anal. 2003, 31, 369–374. [Google Scholar] [CrossRef]
- Chawla, J.; Kvarnberg, D. Hydrosoluble Vitamins. Handb. Clin. Neurol. 2014, 120, 891–914. [Google Scholar] [CrossRef]
- Russell, R.M.; Baik, H.; Kehayias, J.J. Older Men and Women Efficiently Absorb Vitamin B12 from Milk and Fortified Bread. J. Nutr. 2001, 131, 291–293. [Google Scholar] [CrossRef] [Green Version]
- Zeuschner, C.L.; Hokin, B.D.; Marsh, K.A.; Saunders, A.V.; Reid, M.A.; Ramsay, M.R. Vitamin B12 and Vegetarian Diets. Med. J. Aust. 2013, 199, S27-32. [Google Scholar] [CrossRef]
- Ottaway, P.B. Stability of Vitamins in Food. In The Technology of Vitamins in Food; Ottaway, P.B., Ed.; Springer: Boston, MA, USA, 1993; pp. 90–113. ISBN 978-1-4615-2131-0. [Google Scholar]
- Edelmann, M.; Chamlagain, B.; Santin, M.; Kariluoto, S.; Piironen, V. Stability of Added and in Situ-Produced Vitamin B12 in Breadmaking. Food Chem. 2016, 204, 21–28. [Google Scholar] [CrossRef] [Green Version]
- Riaz, M.N.; Asif, M.; Ali, R. Stability of Vitamins during Extrusion. Crit. Rev. Food Sci. Nutr. 2009, 49, 361–368. [Google Scholar] [CrossRef]
- Killeit, U. Vitamin Retention in Extrusion Cooking. Food Chem. 1994, 49, 149–155. [Google Scholar] [CrossRef]
- Bajaj, S.R.; Singhal, R.S. Effect of Extrusion Processing and Hydrocolloids on the Stability of Added Vitamin B12 and Physico-Functional Properties of the Fortified Puffed Extrudates. LWT 2019, 101, 32–39. [Google Scholar] [CrossRef]
- Hemery, Y.M.; Fontan, L.; Laillou, A.; Jallier, V.; Moench-Pfanner, R.; Avallone, S.; Berger, J. Influence of Storage Conditions and Packaging of Fortified Wheat Flour on Microbial Load and Stability of Folate and Vitamin B12. Food Chem. X 2020, 5, 100076. [Google Scholar] [CrossRef]
- Devi, R. Food Processing and Impact on Nutrition. Sch. J. Agric. Vet. Sci. 2015, 2, 304–311. [Google Scholar]
- Watanabe, F.; Abe, K.; Fujita, T.; Goto, M.; Hiemori, M.; Nakano, Y. Effects of Microwave Heating on the Loss of Vitamin B12 in Foods. J. Agric. Food Chem. 1998, 46, 206–210. [Google Scholar] [CrossRef]
- Czerwonka, M.; Szterk, A.; Waszkiewicz-Robak, B. Vitamin B12 Content in Raw and Cooked Beef. Meat Sci. 2014, 96, 1371–1375. [Google Scholar] [CrossRef]
- Bennink, M.R.; Ono, K. Vitamin B12, E and D Content of Raw and Cooked Beef. J. Food Sci. 1982, 47, 1786–1792. [Google Scholar] [CrossRef]
- Nishioka, M.; Kanosue, F.; Yabuta, Y.; Watanabe, F. Loss of Vitamin B12 in Fish (Round Herring) Meats during Various Cooking Treatments. J. Nutr. Sci. Vitaminol. 2011, 57, 432–436. [Google Scholar] [CrossRef] [Green Version]
- Johns, P.W.; Das, A.; Kuil, E.M.; Jacobs, W.A.; Schimpf, K.J.; Schmitz, D.J. Cocoa Polyphenols Accelerate Vitamin B12 Degradation in Heated Chocolate Milk. Int. J. Food Sci. Technol. 2015, 50, 421–430. [Google Scholar] [CrossRef]
- Rosenblum, C.; Woodbury, D.T. The Determination of the Stability of Vitamin B12 in Multivitamin Mixture by a Radioactive Indicator Method. J. Am. Pharm. Assoc. 1952, 41, 368–371. [Google Scholar] [CrossRef]
- Blitz, M.; Eigen, E.; Gunsberg, E. Studies Relating to The Stability of Vitamin B12 in B-Complex Injectable Solutions. J. Am. Pharm. Assoc. 1956, 45, 803–806. [Google Scholar] [CrossRef]
- Chamle, A.H.; Shane, N.L.J.; Pai, A.; Muddukrishna, B.S. Photodegradation of Methylcobalamin and Its Determination in a Commercial Formulation. Indian J. Pharm. Sci. 2019, 81, 57–62. [Google Scholar] [CrossRef]
- Ip, K.; Banov, D.; Bassani, G.; Morgan, L. Physicochemical Stability of Extemporaneously Prepared Methylcobalamin Injections in the Presence and Absence of Preservative and the Impact of Light Exposure. Int. J. Pharm. Compd. 2019, 23, 167–175. [Google Scholar]
- Kusadome, C.; Shibayama, Y.; Nishi, Y.; Takeda, Y.; Yamada, K. Stability of High-Dose Methylcobalamin Injection. J. Appl. Ther. Res. 2008, 6, 15–18. [Google Scholar]
- Jacob, J.T.; Nessel, R.J.; Blodinger, J. Stability of Cyanocobalamin in Film-Coated Multivitamin Tablets. J Pharm. Sci. 1968, 57, 1854–1857. [Google Scholar] [CrossRef] [PubMed]
- Ohmori, S.; Kataoka, M.; Koyama, H. Stability of Cyanocobalamin in Sugar-Coated Tablets. Int. J. Pharm. 2007, 337, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Saeki, T.; Katagiri, Y.; Hirano, H.; Naora, K. Photostability of Mecobalamin in Tablet and Capsule at the Dispensing Level. Shimane J. Med. Sci. 1984, 8, 1–8. [Google Scholar]
- LeDoux, M.A.; Appelhans, K.R.; Braun, L.A.; Dziedziczak, D.; Jennings, S.; Liu, L.; Osiecki, H.; Wyszumiala, E.; Griffiths, J.C. A Quality Dietary Supplement: Before You Start and after It’s Marketed—A Conference Report. Eur. J. Nutr. 2015, 54, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temova Rakuša, Ž.; Srečnik, E.; Roškar, R. Novel HPLC-UV Method for Simultaneous Determination of Fat-Soluble Vitamins and Coenzyme Q10 in Medicines and Supplements. Acta Chim. Slov. 2017, 64, 523–529. [Google Scholar] [CrossRef] [Green Version]
- Flynn, A.; Kehoe, L.; Hennessy, Á.; Walton, J. Estimating Safe Maximum Levels of Vitamins and Minerals in Fortified Foods and Food Supplements. Eur. J. Nutr. 2017, 56, 2529–2539. [Google Scholar] [CrossRef] [Green Version]
- Andrews, K.W.; Roseland, J.M.; Gusev, P.A.; Palachuvattil, J.; Dang, P.T.; Savarala, S.; Han, F.; Pehrsson, P.R.; Douglass, L.W.; Dwyer, J.T.; et al. Analytical Ingredient Content and Variability of Adult Multivitamin/Mineral Products: National Estimates for the Dietary Supplement Ingredient Database12. Am. J. Clin. Nutr. 2017, 105, 526–539. [Google Scholar] [CrossRef] [Green Version]
- Yoo, S.J.; Walfish, S.L.; Atwater, J.B.; Giancaspro, G.; Sarma, N. Factors to Consider in Setting Adequate Overages of Vitamins and Minerals in Dietary Supplements. Pharm. Forum 2016, 42, 111–114. [Google Scholar]
- European Commission (2012) Guidance Document for Competent Authorities for the Control of Compliance with EU Legislation with Regard to the Setting of Tolerances for Nutrient Values Declared on a Label. 2012. Available online: https://www.fsai.ie/uploadedfiles/guidance_tolerances_december_2012.pdf (accessed on 19 May 2022).
- Center for Food Safety and Applied Nutrition (CFSAN). Guidance for Industry: Guide for Developing and Using Data Bases for Nutrition Labeling. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/guidance-industry-guide-developing-and-using-data-bases-nutrition-labeling (accessed on 19 June 2022).
- Chopra, A.S.; Lordan, R.; Horbańczuk, O.K.; Atanasov, A.G.; Chopra, I.; Horbańczuk, J.O.; Jóźwik, A.; Huang, L.; Pirgozliev, V.; Banach, M.; et al. The Current Use and Evolving Landscape of Nutraceuticals. Pharmacol. Res. 2022, 175, 106001. [Google Scholar] [CrossRef]
- Droz, N.; Marques-Vidal, P. Multivitamins/Multiminerals in Switzerland: Not as Good as It Seems. Nutr. J. 2014, 13, 24. [Google Scholar] [CrossRef] [Green Version]
- Dwyer, J.T.; Coates, P.M.; Smith, M.J. Dietary Supplements: Regulatory Challenges and Research Resources. Nutrients 2018, 10, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute of Medicine (US) Standing Committee on the Scientific Evaluation of Dietary Reference Intakes and its Panel on Folate, Other B Vitamins, and Choline. Dietary Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academies Press (US): Washington, DC, USA, 1998; ISBN 978-0-309-06411-8. [Google Scholar]
- Klejdus, B.; Petrlová, J.; Potěšil, D.; Adam, V.; Mikelová, R.; Vacek, J.; Kizek, R.; Kubáň, V. Simultaneous Determination of Water- and Fat-Soluble Vitamins in Pharmaceutical Preparations by High-Performance Liquid Chromatography Coupled with Diode Array Detection. Anal. Chim. Acta 2004, 520, 57–67. [Google Scholar] [CrossRef]
- Fan, D.; Zhang, Y.; Wu, H. Development of a Simple and Sensitive HPLC-DAD Method for Quantification of Vitamin B12 Fortified in Infant Food. Anal. Methods 2021, 13, 4920–4925. [Google Scholar] [CrossRef]
- Luo, X.; Chen, B.; Ding, L.; Tang, F.; Yao, S. HPLC-ESI-MS Analysis of Vitamin B12 in Food Products and in Multivitamins-Multimineral Tablets. Anal. Chim. Acta 2006, 562, 185–189. [Google Scholar] [CrossRef]
- Raju, C.S.K.; Yu, L.L.; Schiel, J.E.; Long, S.E. A Simple and Sensitive LC-ICP-MS Method for the Accurate Determination of Vitamin B12 in Fortified Breakfast Cereals and Multivitamin Tablets. J. Anal. At. Spectrom. 2013, 28, 901–907. [Google Scholar] [CrossRef]
- Li, H.B.; Chen, F.; Jiang, Y. Determination of Vitamin B12 in Multivitamin Tablets and Fermentation Medium by High-Performance Liquid Chromatography with Fluorescence Detection. J. Chromatogr. A 2000, 891, 243–247. [Google Scholar] [CrossRef]
- Chatzimichalakis, P.F.; Samanidou, V.F.; Verpoorte, R.; Papadoyannis, I.N. Development of a Validated HPLC Method for the Determination of B-Complex Vitamins in Pharmaceuticals and Biological Fluids after Solid Phase Extraction. J. Sep. Sci. 2004, 27, 1181–1188. [Google Scholar] [CrossRef]
- Marszałł, M.L.; Lebiedzińska, A.; Czarnowski, W.; Szefer, P. High-Performance Liquid Chromatography Method for the Simultaneous Determination of Thiamine Hydrochloride, Pyridoxine Hydrochloride and Cyanocobalamin in Pharmaceutical Formulations Using Coulometric Electrochemical and Ultraviolet Detection. J. Chromatogr. A 2005, 1094, 91–98. [Google Scholar] [CrossRef]
- Chen, P.; Wolf, W.R.; Castanheira, I.; Sanches-Silva, A. A LC/UV/Vis Method for Determination of Cyanocobalamin (VB12) in Multivitamin Dietary Supplements with on-Line Sample Clean-Up. Anal. Methods 2010, 2, 1171–1175. [Google Scholar] [CrossRef] [Green Version]
- Li, H.B.; Chen, F. Determination of Vitamin B12 in Pharmaceutical Preparations by a Highly Sensitive Fluorimetric Method. Fresenius. J. Anal. Chem. 2000, 368, 836–838. [Google Scholar] [CrossRef]
- Patil, S.S.; Srivastava, A.K. Development and Validation of a Liquid Chromatography Method for the Simultaneous Determination of Eight Water-Soluble Vitamins in Multivitamin Formulations and Human Urine. J. AOAC Int. 2013, 96, 1273–1280. [Google Scholar] [CrossRef] [PubMed]
- D’Ulivo, L.; Yang, L.; Ding, J.; Pagliano, E.; Leek, D.M.; Thibeault, M.-P.; Mester, Z. Determination of Cyanocobalamin by Isotope Dilution LC-MS/MS. Anal. Chim. Acta 2017, 990, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, X.; Schnute, W. Simultaneous Analysis of Water-Soluble Vitamins in Vitamin-Enriched Beverages and Multivitamin Dietary Supplements by UHPLC-MS/MS; Application Note 294; Thermo Scientific: Waltham, MA, USA, 2016. [Google Scholar]
- Moreno, P.; Salvadó, V. Determination of Eight Water- and Fat-Soluble Vitamins in Multi-Vitamin Pharmaceutical Formulations by High-Performance Liquid Chromatography. J. Chromatogr. A 2000, 870, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, M.; Ide, N.; Shiraishi, S.; Ono, K. Effect of Various Halide Salts on the Incompatibility of Cyanocobalamin and Ascorbic Acid in Aqueous Solution. Chem. Pharm. Bull. 2005, 53, 688–690. [Google Scholar] [CrossRef]
- Wang, H.; Shou, Y.; Zhu, X.; Xu, Y.; Shi, L.; Xiang, S.; Feng, X.; Han, J. Stability of Vitamin B12 with the Protection of Whey Proteins and Their Effects on the Gut Microbiome. Food Chem. 2019, 276, 298–306. [Google Scholar] [CrossRef]
- Uchida, T.; Suguri, T.; Harjinder, S. Folic Acid and/or Vitamin B12-Lactoferrin Complex. U.S. Patent US6500472B2, 31 December 2002. [Google Scholar]
- Grissom, C.B.; Chagovetz, A.M.; Wang, Z. Use of Viscosigens to Stabilize Vitamin B12 Solutions against Photolysis. J. Pharm. Sci. 1993, 82, 641–643. [Google Scholar] [CrossRef]
- Bajaj, S.R.; Singhal, R.S. Enhancement of Stability of Vitamin B12 by Co-Crystallization: A Convenient and Palatable Form of Fortification. J. Food Eng. 2021, 291, 110231. [Google Scholar] [CrossRef]
- Rajakumari, R.; Oluwafemi, O.S.; Thomas, S.; Kalarikkal, N. Dietary Supplements Containing Vitamins and Minerals: Formulation, Optimization and Evaluation. Powder Technol. 2018, 336, 481–492. [Google Scholar] [CrossRef]
- Wang, J.-R.; Zhou, C.; Yu, X.; Mei, X. Stabilizing Vitamin D3 by Conformationally Selective Co-Crystallization. Chem. Commun. 2014, 50, 855–858. [Google Scholar] [CrossRef]
- Zhu, B.; Wang, J.-R.; Zhang, Q.; Mei, X. Improving Dissolution and Photostability of Vitamin K3 via Cocrystallization with Naphthoic Acids and Sulfamerazine. Cryst. Growth Des. 2016, 16, 483–492. [Google Scholar] [CrossRef]
- Choudhury, N.; Meghwal, M.; Das, K. Microencapsulation: An Overview on Concepts, Methods, Properties and Applications in Foods. Food Front. 2021, 2, 426–442. [Google Scholar] [CrossRef]
- Singh, M.N.; Hemant, K.S.Y.; Ram, M.; Shivakumar, H.G. Microencapsulation: A Promising Technique for Controlled Drug Delivery. Res. Pharm. Sci. 2010, 5, 65–77. [Google Scholar] [PubMed]
- Carlan, I.C.; Estevinho, B.N.; Rocha, F. Study of Different Encapsulating Agents for the Microencapsulation of Vitamin B12. Environ. Eng. Manag. J. 2018, 17, 855–864. [Google Scholar] [CrossRef]
- Carlan, I.C.; Estevinho, B.N.; Rocha, F. Study of Microencapsulation and Controlled Release of Modified Chitosan Microparticles Containing Vitamin B12. Powder Technol. 2017, 318, 162–169. [Google Scholar] [CrossRef]
- Chalella Mazzocato, M.; Thomazini, M.; Favaro-Trindade, C.S. Improving Stability of Vitamin B12 (Cyanocobalamin) Using Microencapsulation by Spray Chilling Technique. Food Res. Int. 2019, 126, 108663. [Google Scholar] [CrossRef]
- Gupta, R.G.; Rao, B.C. Microencapsulation of Vitamin B12 by Emulsion Technique. Drug Dev. Ind. Pharm. 1985, 11, 41–53. [Google Scholar] [CrossRef]
- Oh, S.; Cave, G.; Lu, C. Vitamin B12 (Cobalamin) and Micronutrient Fortification in Food Crops Using Nanoparticle Technology. Front. Plant Sci. 2021, 12, 668819. [Google Scholar] [CrossRef]
- de Britto, D.; Pinola, F.G.; Mattoso, L.H.C.; Assis, O.B.G. Analysis of Thermal and Aqueous Suspension Stabilities of Chitosan Based Nanoencapsulated Vitamins. Química Nova 2016, 39, 1126–1130. [Google Scholar] [CrossRef]
- Maiorova, L.A.; Erokhina, S.I.; Pisani, M.; Barucca, G.; Marcaccio, M.; Koifman, O.I.; Salnikov, D.S.; Gromova, O.A.; Astolfi, P.; Ricci, V.; et al. Encapsulation of Vitamin B12 into Nanoengineered Capsules and Soft Matter Nanosystems for Targeted Delivery. Colloids Surf. B Biointerfaces 2019, 182, 110366. [Google Scholar] [CrossRef]
- Arsalan, A.; Ahmad, I.; Ali, S.A.; Qadeer, K.; Mahmud, S.; Humayun, F.; Beg, A.E. The Kinetics of Photostabilization of Cyanocobalamin in Liposomal Preparations. Int. J. Chem. Kinet. 2020, 52, 207–217. [Google Scholar] [CrossRef]
- Gorantla, S.; Wadhwa, G.; Jain, S.; Sankar, S.; Nuwal, K.; Mahmood, A.; Dubey, S.K.; Taliyan, R.; Kesharwani, P.; Singhvi, G. Recent Advances in Nanocarriers for Nutrient Delivery. Drug Deliv. Transl. Res. 2021, 12, 2359–2384. [Google Scholar] [CrossRef]
- Lee, J.; Yang, J.H.; Kim, K.S.; Park, G.D. Effect of Liposome Storage of Cyanocobalamin on Its Degradation by Ascorbic Acid. Food Suppl. Biomater. Health 2021, 1, e7. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Vitamin B12 Content | Fortified Foods | Food Supplements | Medicines |
|---|---|---|---|
| AV (Min–Max) (%) | 131.4 (85.4–242.5) | 115.6 (56.0–281.8) | 85.9 (5.0–178.0) |
 |  |  | |
| No. | 13 | 46 | 22 |
| References | [229,230,231,232] | [133,141,232,233,234,235,236,237,238,239,240] | [141,150,151,211, 235,237,241] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Temova Rakuša, Ž.; Roškar, R.; Hickey, N.; Geremia, S. Vitamin B12 in Foods, Food Supplements, and Medicines—A Review of Its Role and Properties with a Focus on Its Stability. Molecules 2023, 28, 240. https://doi.org/10.3390/molecules28010240
Temova Rakuša Ž, Roškar R, Hickey N, Geremia S. Vitamin B12 in Foods, Food Supplements, and Medicines—A Review of Its Role and Properties with a Focus on Its Stability. Molecules. 2023; 28(1):240. https://doi.org/10.3390/molecules28010240
Chicago/Turabian StyleTemova Rakuša, Žane, Robert Roškar, Neal Hickey, and Silvano Geremia. 2023. "Vitamin B12 in Foods, Food Supplements, and Medicines—A Review of Its Role and Properties with a Focus on Its Stability" Molecules 28, no. 1: 240. https://doi.org/10.3390/molecules28010240