
Traditional Chinese Medicine Rhodiola Sachalinensis Borissova from Baekdu Mountain (RsBBM) for Rheumatoid Arthritis: Therapeutic Effect and Underlying Molecular Mechanisms

Abstract
:1. Introduction
2. Results
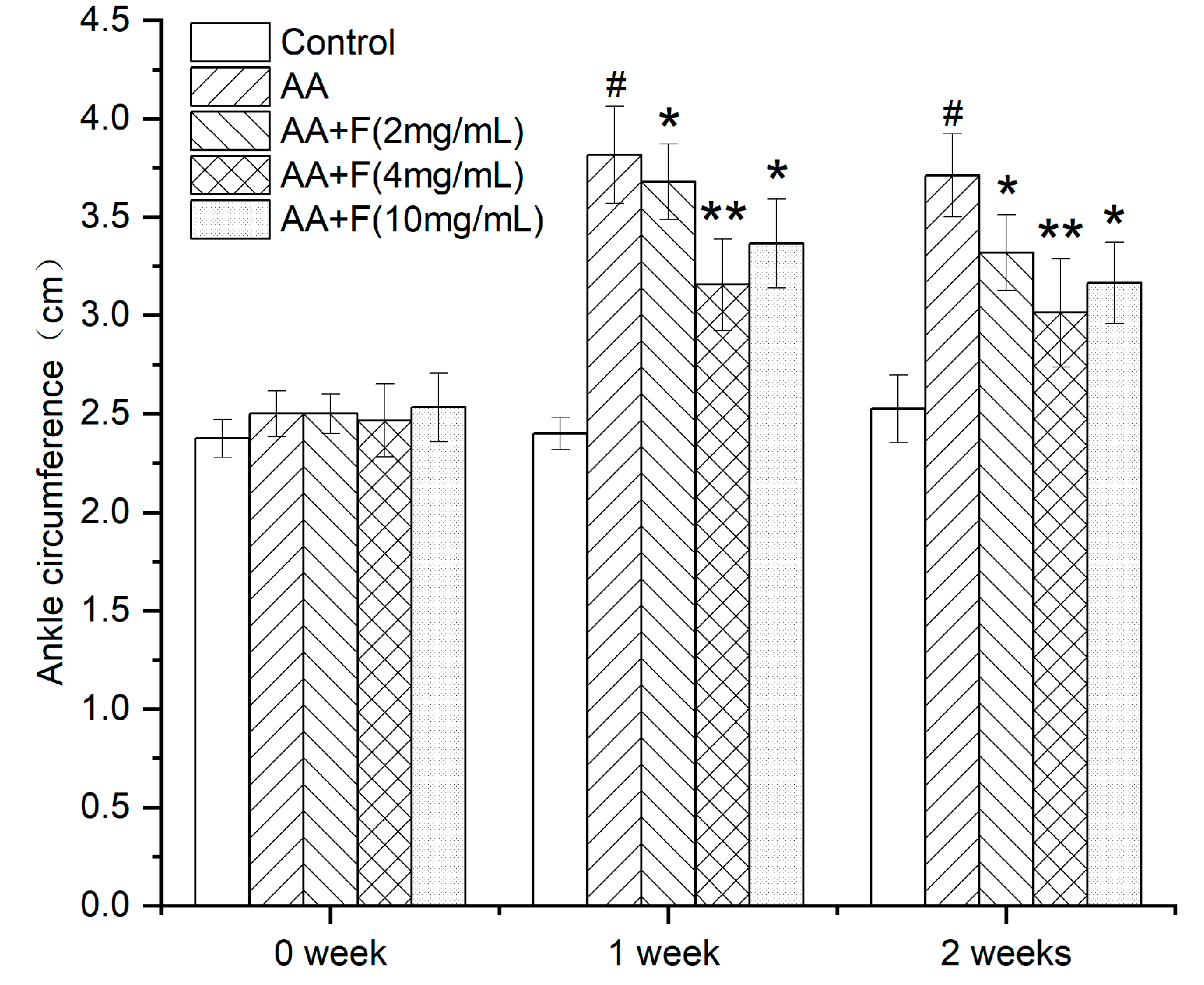
2.1. Effect of the 50% Ethanol Extract of RsBBM on Rat Ankle Joint Swelling
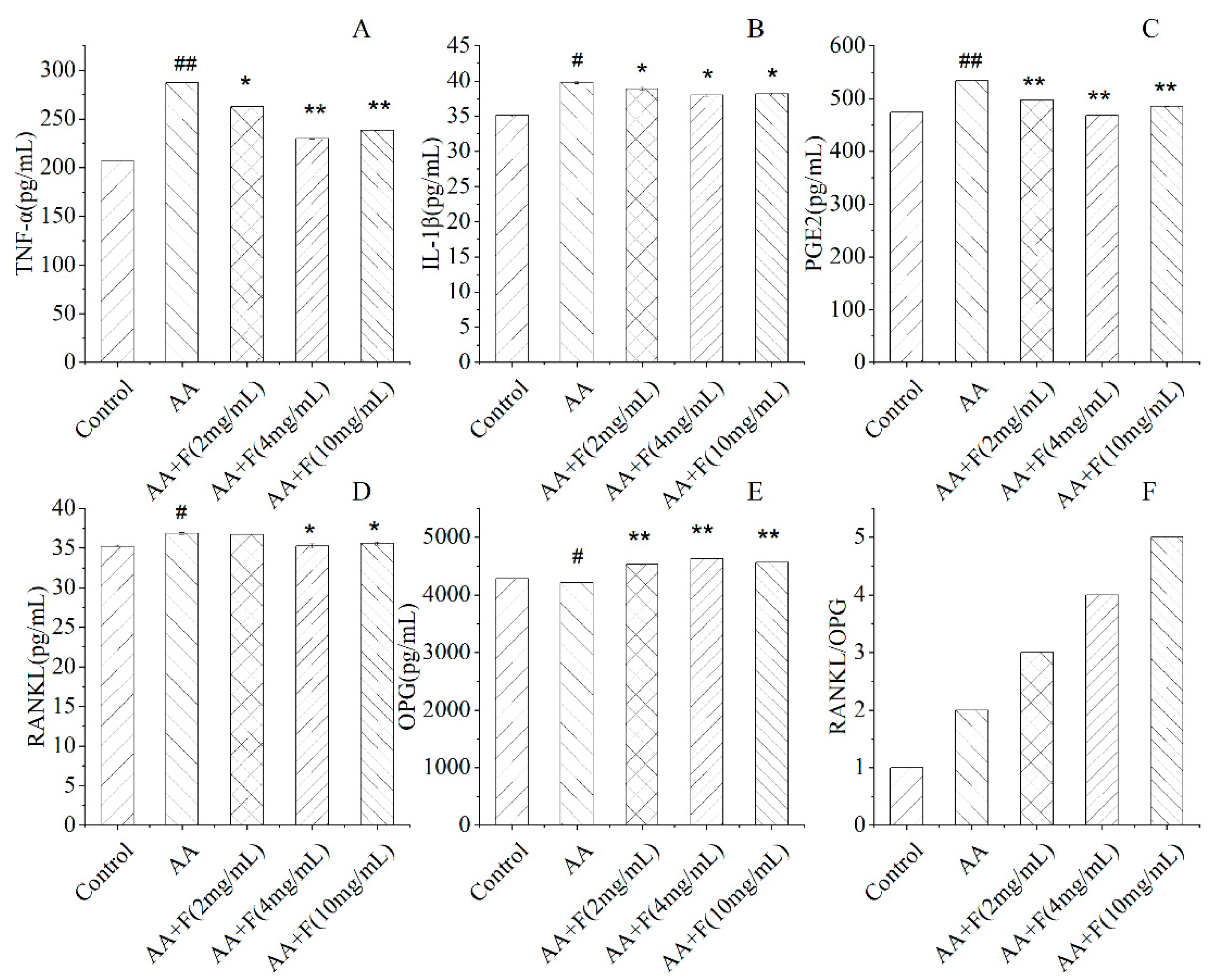
2.2. Effects of the 50% Ethanol Extract of RsBBM on Serum Cytokine Levels
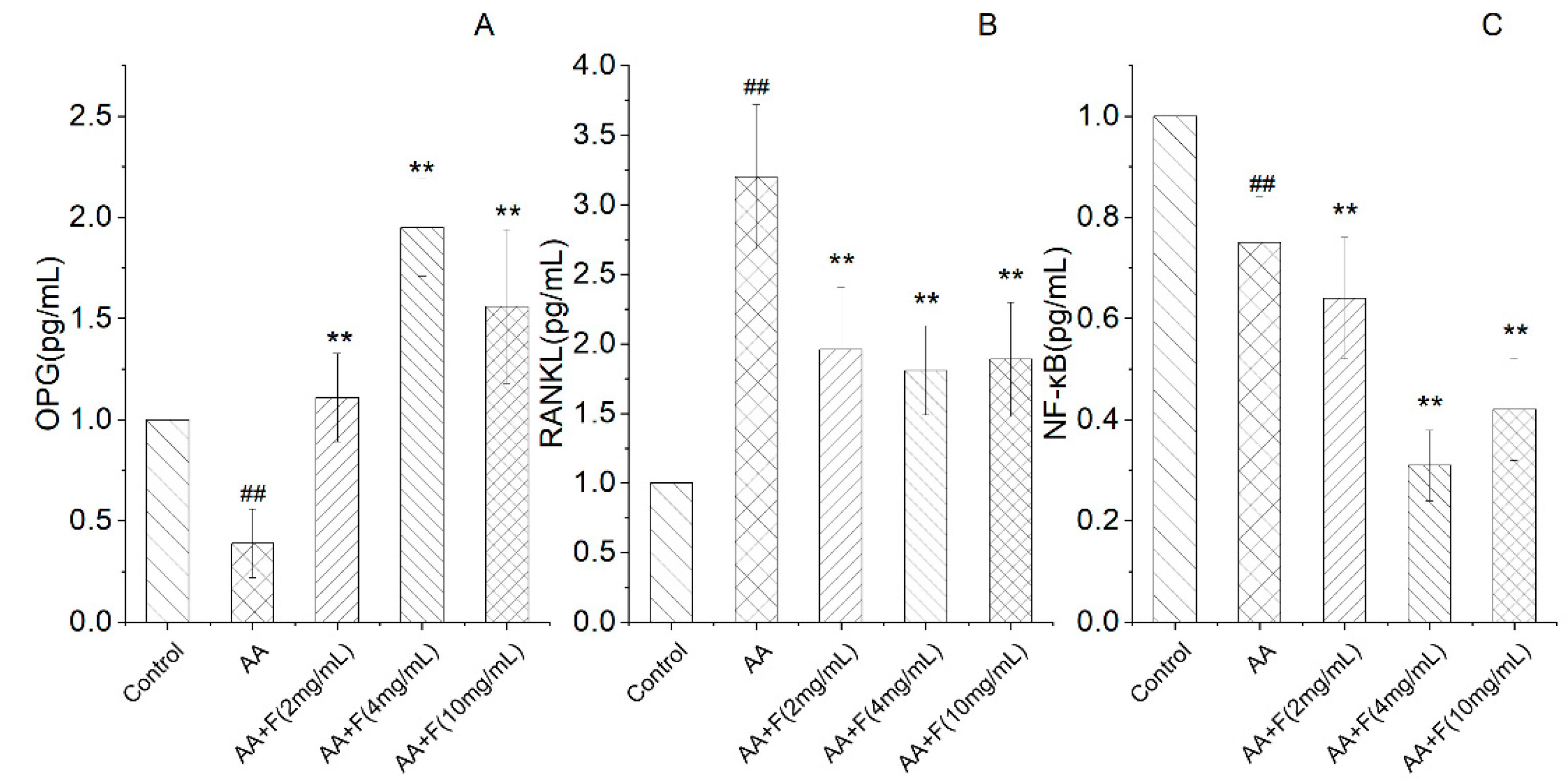
2.3. Effects of the 50% Ethanol Extract of RsBBM on mRNA-Level Expression of Arthritis-Associated Genes
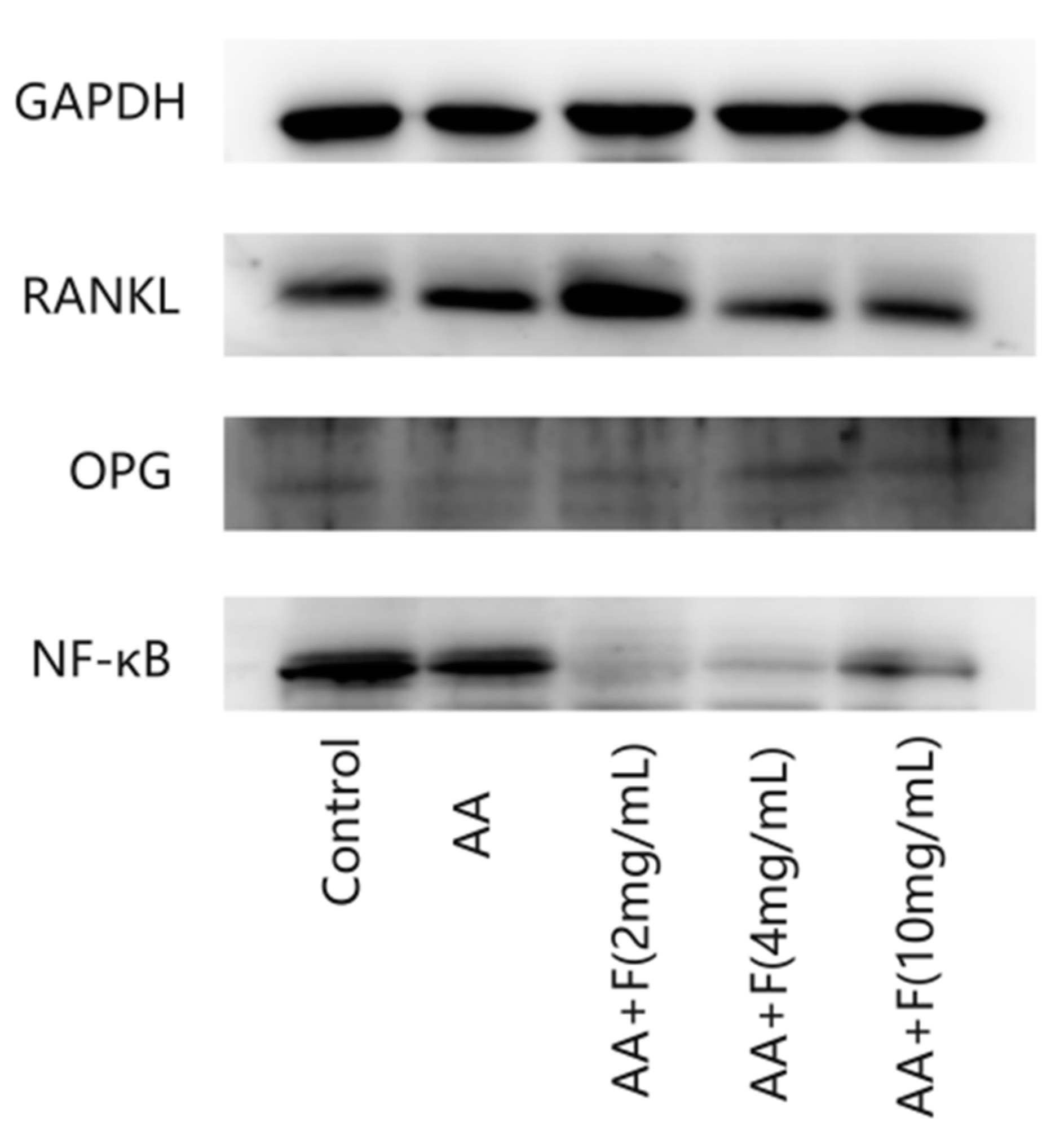
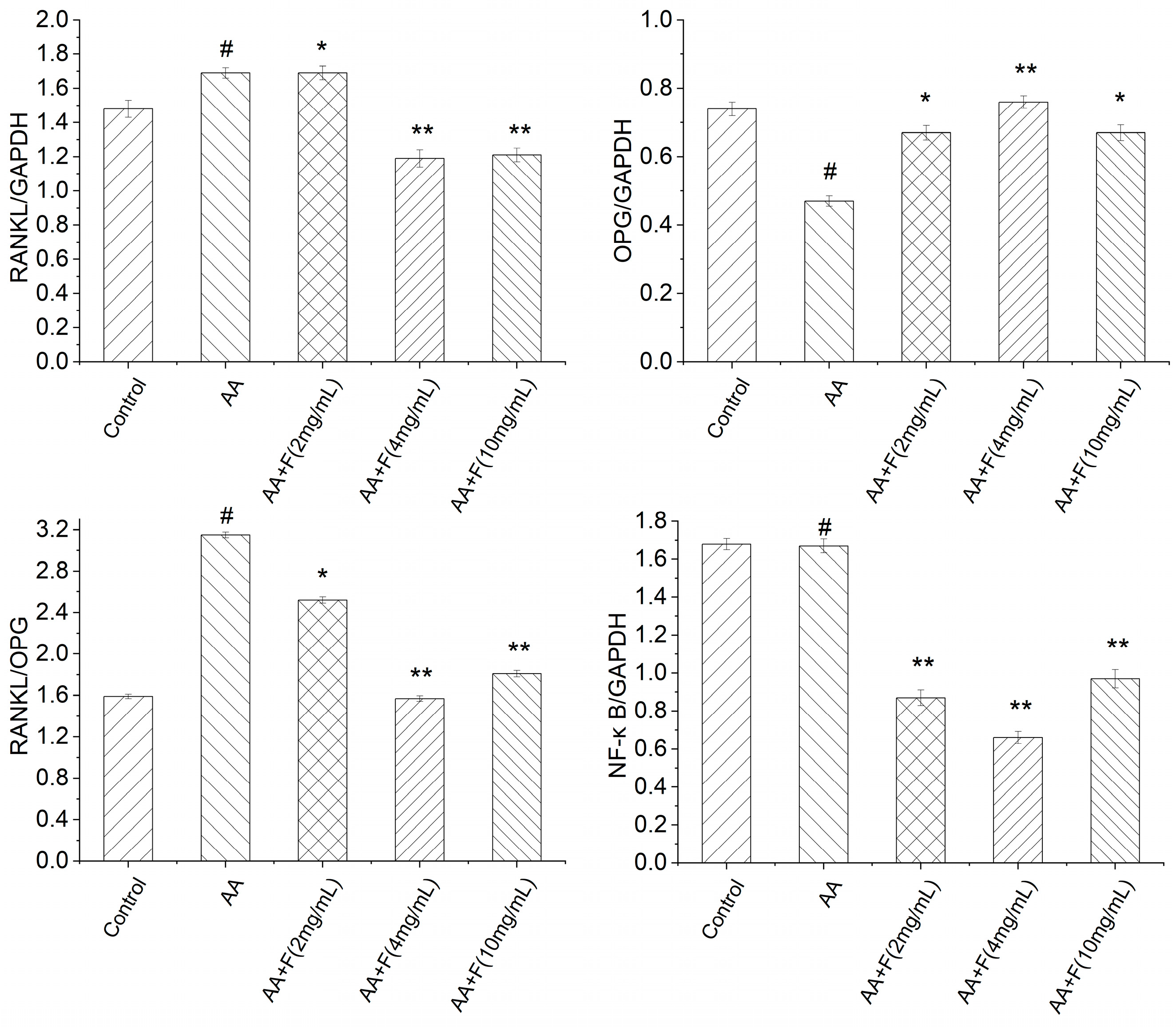
2.4. Effects of the 50% Ethanol Extract of RsBBM on Expression of Arthritis-Associated Proteins
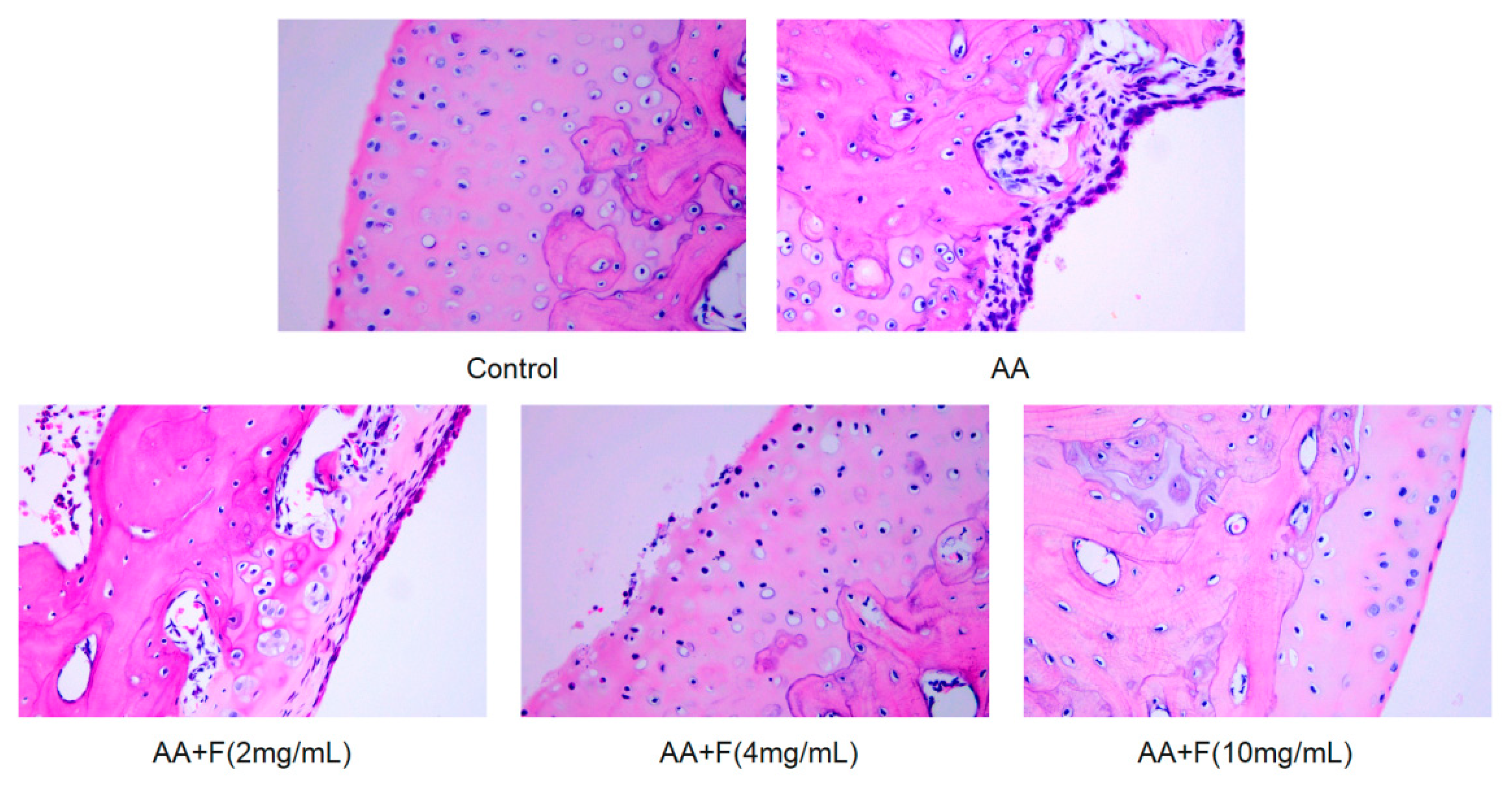
2.5. Histopathological Examination
3. Discussion
4. Materials and Methods
4.1. Chinese Herbal Extract
4.2. Chemicals and Reagents
4.3. Therapeutic Administrative Protocol
4.4. Serum Cytokines Measurements
4.5. RNA Extraction, cDNA Reverse Transcription, and Quantitavive Real-Time PCR
4.6. Western Blot-Based Detection of Protein Expression Levels
4.7. Histological Study of Rat Joint Tissues
4.8. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Sample Availability
References
- Oğul, Y.; Gür, F.; Cengiz, M.; Gür, B.; Sarı, R.A.; Kızıltunç, A. Evaluation of oxidant and intracellular anti-oxidant activity in rheumatoid arthritis patients: In Vivo and in silico studies. Int. Immunopharmacol. 2021, 97, 107654. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Lin, Q. Genomics, Transcriptomics and proteomics to elucidate the pathogenesis of rheumatoid arthritis. Rheumatol. Int. 2017, 37, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Firestein, G.S.; McInnes, I.B. Immunopathogenesis of Rheumatoid Arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef] [PubMed]
- Tateiwa, D.; Yoshikawa, H.; Kaito, T. Cartilage and Bone Destruction in Arthritis: Pathogenesis and Treatment Strategy: A Literature Review. Cells 2019, 8, 818. [Google Scholar] [CrossRef]
- Corvo, M.L. Liposomal Nanosystems in Rheumatoid Arthritis. Pharmaceutics 2021, 13, 454–478. [Google Scholar]
- Khan, Z.A.; Tripathi, R.; Mishra, B. Methotrexate: A detailed review on drug delivery and clinical aspects. Expert Opin. Drug Deliv. 2012, 9, 151–169. [Google Scholar] [CrossRef]
- Crofford, L.J. Use of NSAIDs in treating patients with arthritis. Arthritis Res. Ther. 2013, 15 (Suppl. S3), S2. [Google Scholar] [CrossRef]
- Solomon, D.H.; Husni, M.E.; Libby, P.A.; Yeomans, N.D.; Lincoff, A.M.; Lüscher, T.F.; Menon, V.; Brennan, D.M.; Wisniewski, L.M.; Nissen, S.E.; et al. The Risk of Major NSAID Toxicity with Celecoxib, Ibuprofen, or Naproxen: A Secondary Analysis of the PRECISION Trial. Am. J. Med. 2017, 130, 1415–1422. [Google Scholar] [CrossRef]
- Zampeli, E.; Vlachoyiannopoulos, P.G.; Tzioufas, A.G. Treatment of rheumatoid arthritis: Unraveling the conundrum. J. Autoimmun. 2015, 65, 1–18. [Google Scholar] [CrossRef]
- George, G.; Shyni, G.L.; Raghu, K.G. Current and novel therapeutic targets in the treatment of rheumatoid arthritis. Inflammopharmacology 2020, 28, 1457–1476. [Google Scholar] [CrossRef]
- Loyola-Sanchez, A.; Hazlewood, G.; Crowshoe, L.; Linkert, T.; Hull, P.M.; Marshall, D.; Barnabe, C. Qualitative Study of Treatment Preferences for Rheumatoid Arthritis and Pharmacotherapy Acceptance: Indigenous Patient Perspectives. Arthritis Care Res. 2020, 72, 544–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Zhang, Y.; Zhu, W.; Ma, C.; Ruan, J.; Long, H.; Wang, Y. Sinomenine Inhibits the Progression of Rheumatoid Arthritis by Regulating the Secretion of Inflammatory Cytokines and Monocyte/Macrophage Subsets. Front. Immunol. 2018, 9, 2228. [Google Scholar] [CrossRef] [PubMed]
- Pu, W.L.; Zhang, M.Y.; Bai, R.Y.; Sun, L.K.; Li, W.H.; Yu, Y.L.; Zhang, Y.; Song, L.; Wang, Z.X.; Peng, Y.F.; et al. Anti-inflammatory effects of Rhodiola rosea L.: A review. Biomed. Pharmacother. 2020, 21, 109552. [Google Scholar] [CrossRef] [PubMed]
- Panossian, A.; Wikman, G.; Sarris, J. Rosenroot (Rhodiola rosea): Traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine 2010, 17, 481–493. [Google Scholar] [CrossRef]
- Wang, H.M.; Wang, M. Nanometer preparation of traditional Chinese medicine for rheumatoid arthritis. Zhongguo Zhong Yao Za Zhi 2019, 44, 3908–3916. [Google Scholar]
- Kong, X.Y.; Wen, C.P. On Research Progress of Western and Chinese Medicine Treatment on Pre-Rheumatoid Arthritis. Chin. J. Integr. Med. 2019, 25, 643–647. [Google Scholar] [CrossRef]
- Silva, I.; Branco, J.C. Rank/Rankl/opg: Literature review. Acta Reumatol. Port. 2011, 36, 209–218. [Google Scholar]
- Zhao, Y.; Wang, H.L.; Li, T.T.; Yang, F.; Tzeng, C.M. Baicalin Ameliorates Dexamethasone-Induced Osteoporosis by Regulation of the RANK/RANKL/OPG Signaling Pathway. Drug Des. Dev. Ther. 2020, 14, 195–206. [Google Scholar] [CrossRef]
- Xue, P.P.; Yuan, J.D.; Yao, Q.; Zhao, Y.Z.; Xu, H.L. Bioactive Factors-imprinted Scaffold Vehicles for Promoting Bone Healing: The Potential Strategies and the Confronted Challenges for Clinical Production. BIO Integr. 2020, 1, 37–54. [Google Scholar] [CrossRef]
- Qin, S.; Liu, D.; Zhou, Z.; Chen, S. The Roles of Long Non-coding RNAs in Osteogenic Differentiation and Bone Diseases. BIO Integr. 2022, 3, 21–31. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L. Biology of RANK, RANKL, and osteoprotegerin. Arthritis Res. Ther. 2007, 9 (Suppl. S1), S1. [Google Scholar] [CrossRef] [PubMed]
- Boyce, B.F.; Xing, L. Functions of RANKL/RANK/OPG in bone modeling and remodeling. Arch. Biochem. Biophys. 2008, 473, 139–146. [Google Scholar] [CrossRef]
- Pérez-Sayáns, M.; Somoza-Martín, J.M.; Barros-Angueira, F.; Rey, J.M.; García-García, A. RANK/RANKL/OPG role in distraction osteogenesis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2010, 109, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Roman-Blas, J.A.; Jimenez, S.A. NF-kappaB as a potential therapeutic target in osteoarthritis and rheumatoid arthritis. Osteoarthr. Cartil. 2006, 14, 839–848. [Google Scholar] [CrossRef]
- Jiang, Q.; Yi, M.; Guo, Q.; Wang, C.; Wang, H.; Meng, S.; Liu, C.; Fu, Y.; Ji, H.; Chen, T. Protective effects of polydatin on lipopolysaccharide-induced acute lung injury through TLR4-MyD88-NF-kappaB pathway. Int. Immunopharmacol. 2015, 29, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Mou, Y.; Tan, J.; Wei, L.; Qiao, Y.; Wei, T.; Xiang, P.; Peng, S.; Zhang, Y.; Huang, Z.; et al. The protective effect of CDDO-Me on lipopolysaccharide-induced acute lung injury in mice. Int. Immunopharmacol. 2015, 25, 55–64. [Google Scholar] [CrossRef]
- Wang, G.; Xie, X.; Yuan, L.; Qiu, J.; Duan, W.; Xu, B.; Chen, X. Resveratrol ameliorates rheumatoid arthritis via activation of SIRT1-Nrf2 signaling pathway. Biofactors 2020, 46, 441–453. [Google Scholar] [CrossRef]
- Chen, L.; Li, J.; Ke, X.; Qu, W.; Zhang, J.; Feng, F.; Liu, W. The therapeutic effects of Periploca forrestii Schltr. Stem extracts on collagen-induced arthritis by inhibiting the activation of Src/NF-κB signaling pathway in rats. J. Ethnopharmacol. 2017, 202, 12–19. [Google Scholar] [CrossRef]
- Kim, H.Y.; Park, E.J.; Joe, E.H.; Jou, I. Curcumin suppresses Janus kinase-STAT inflammatory signaling through activation of Src homology 2 domain-containing tyrosine phosphatase 2 in brain microglia. J. Immunol. 2003, 171, 6072–6079. [Google Scholar] [CrossRef]
- Leuenroth, S.J.; Crews, C.M. Studies on calcium dependence reveal multiple modes of action for triptolide. Chem. Biol. 2005, 12, 1259–1268. [Google Scholar] [CrossRef]
- Zeng, J.Z.; Ma, L.F.; Meng, H.; Yu, H.M.; Zhang, Y.K.; Guo, A. (5R)-5-hydroxytriptolide (LLDT-8) prevents collagen-induced arthritis through OPG/RANK/RANKL signaling in a rat model of rheumatoid arthritis. Exp. Ther. Med. 2016, 12, 3101–3106. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Cai, L.; Zhang, L.; Wang, G.; Xie, R.; Jiang, Y.; Yuan, Y.; Nie, H. Paeoniflorin ameliorates collagen-induced arthritis via suppressing nuclear factor-kappaB signalling pathway in osteoclast differentiation. Immunology 2018, 12, 58. [Google Scholar]
- Zuo, S.; Zou, W.; Wu, R.M.; Yang, J.; Fan, J.N.; Zhao, X.K.; Li, H.Y. Icariin alleviates IL-1beta-induced matrix degradation by activating the Nrf2/ARE pathway in human chondrocytes. Drug Des. Dev. Ther. 2019, 13, 3949–3961. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.J.; Wu, J.Y.; Leung, W.C.; Liu, Y.X.; Fu, X.Q.; Zhu, J.Q.; Wu, Y.; Chou, J.Y.; Yin, C.L.; Wang, Y.P.; et al. An herbal formula inhibits STAT3 signaling and attenuates bone erosion in collagen-induced arthritis rats. Phytomedicine 2020, 76, 153254. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liang, S.; Tan, C.H.; Cao, S.; Xu, X.; Er Saw, P.; Tao, W. Nanocarriers in the Enhancement of Therapeutic Efficacy of Natural Drugs. BIO Integr. 2021, 2, 40–49. [Google Scholar] [CrossRef]
- Xu, D.; Hu, M.J.; Wang, Y.Q.; Cui, Y.L. Antioxidant Activities of Quercetin and Its Complexes for Medicinal Application. Molecules 2019, 24, 1123. [Google Scholar] [CrossRef]
- Reyes-Farias, M.; Carrasco-Pozo, C. The Anti-Cancer Effect of Quercetin: Molecular Implications in Cancer Metabolism. Int. J. Mol. Sci. 2019, 20, 3177. [Google Scholar] [CrossRef]
- Devi, K.P.; Malar, D.S.; Nabavi, S.F.; Sureda, A.; Xiao, J.; Nabavi, S.M.; Daglia, M. Kaempferol and inflammation: From chemistry to medicine. Pharmacol. Res. 2015, 99, 1–10. [Google Scholar] [CrossRef]
- Alam, W.; Khan, H.; Shah, M.A.; Cauli, O.; Saso, L. Kaempferol as a Dietary Anti-Inflammatory Agent: Current Therapeutic Standing. Molecules 2020, 25, 4073. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inflammatory Infiltration | Synovial Hyperplasia | Cartilage Destruction | Bone Erosion | Total Score | |
|---|---|---|---|---|---|
| Control | 0 | 0 | 0 | 0 | 0 |
| AA | 2.8 | 2.4 | 2.1 | 1.8 | 9.1 |
| AA+F (2 mg/mL) | 2.5 | 1.9 | 1.0 | 0.8 | 6.2 |
| AA+F (4 mg/mL) | 1.8 | 1.4 | 0.7 | 1.5 | 5.4 |
| AA+F (10 mg/mL) | 2.7 | 1.7 | 0.8 | 0.7 | 5.9 |
| Gene | Primer Sequence (5′-3′) | Product (bp) |
|---|---|---|
| GAPDH-Rat-F | GGTGGACCTCATGGCCTACAT | 21 |
| GAPDH-Rat-R | CTCTCTTGCTCTCAGTATCCTTGCT | 25 |
| OPG-Rat-F | ACTTGGCCTCCTGCTAATTC | 20 |
| OPG-Rat-R | CGCACAGGGTGACATCTATT | 20 |
| RANKL-Rat-F | CATCGCTCTGTTCCTGTACTT | 21 |
| RANKL-Rat-R | CGAGTCCTGCAAACCTGTAT | 20 |
| NF-κB-Rat-F | GGTTACGGGAGATGTGAAGATG | 22 |
| NF-κB-Rat-R | GTGGATGATGGCTAAGTGTAGG | 22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, Y.; Zhang, J.; Yu, H.; Zhang, Y.; Zhang, H.; Hao, C.; Zuo, L.; Shi, N.; Li, W. Traditional Chinese Medicine Rhodiola Sachalinensis Borissova from Baekdu Mountain (RsBBM) for Rheumatoid Arthritis: Therapeutic Effect and Underlying Molecular Mechanisms. Molecules 2022, 27, 6058. https://doi.org/10.3390/molecules27186058
Ma Y, Zhang J, Yu H, Zhang Y, Zhang H, Hao C, Zuo L, Shi N, Li W. Traditional Chinese Medicine Rhodiola Sachalinensis Borissova from Baekdu Mountain (RsBBM) for Rheumatoid Arthritis: Therapeutic Effect and Underlying Molecular Mechanisms. Molecules. 2022; 27(18):6058. https://doi.org/10.3390/molecules27186058
Chicago/Turabian StyleMa, Yinghui, Jinbei Zhang, Huan Yu, Yanfei Zhang, Huifeng Zhang, Chengyi Hao, Lili Zuo, Nianqiu Shi, and Wenliang Li. 2022. "Traditional Chinese Medicine Rhodiola Sachalinensis Borissova from Baekdu Mountain (RsBBM) for Rheumatoid Arthritis: Therapeutic Effect and Underlying Molecular Mechanisms" Molecules 27, no. 18: 6058. https://doi.org/10.3390/molecules27186058