
Phytoecdysteroids from Serratula coronata L. for Psoriatic Skincare

 , and
, and
Abstract
:1. Introduction
2. Results
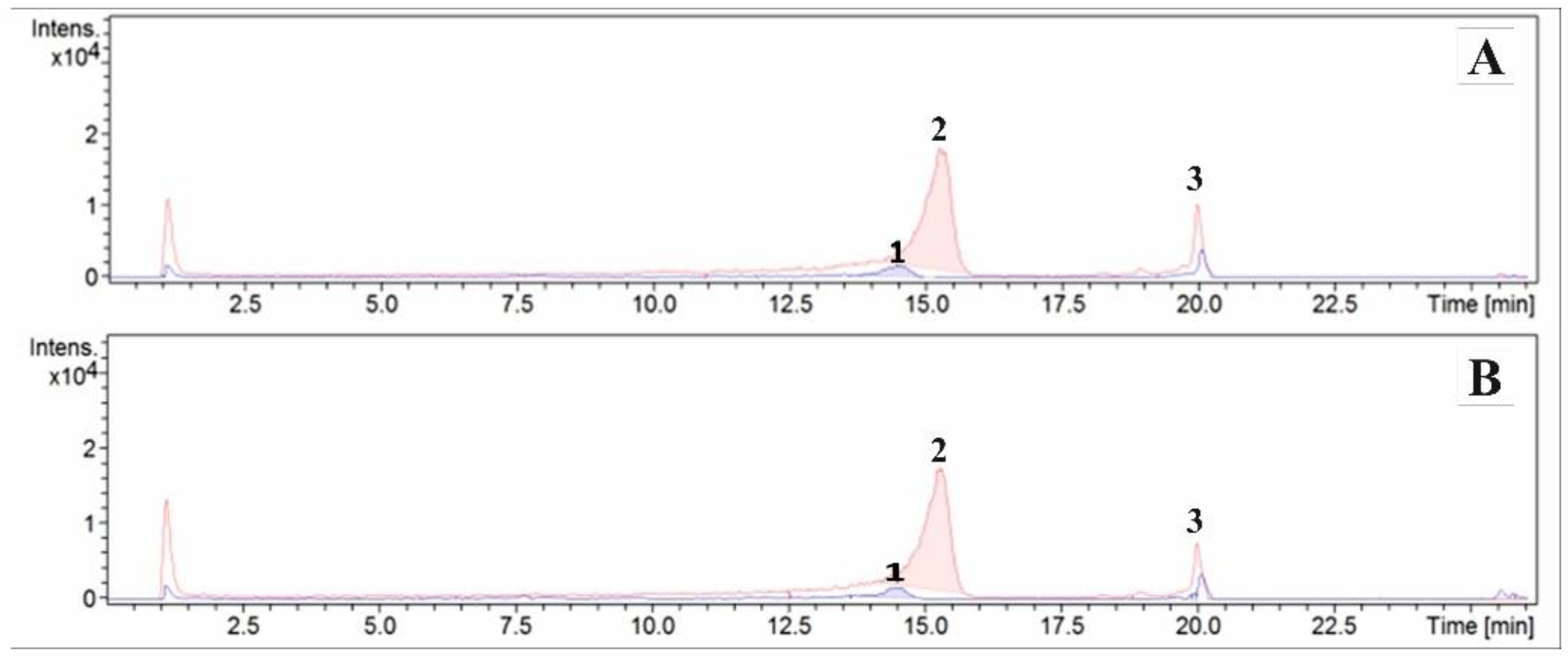
2.1. Determination of Dominant Ecdysteroids in Formulations Using the ESI/HPLC-MS Method
2.2. Patch Tests
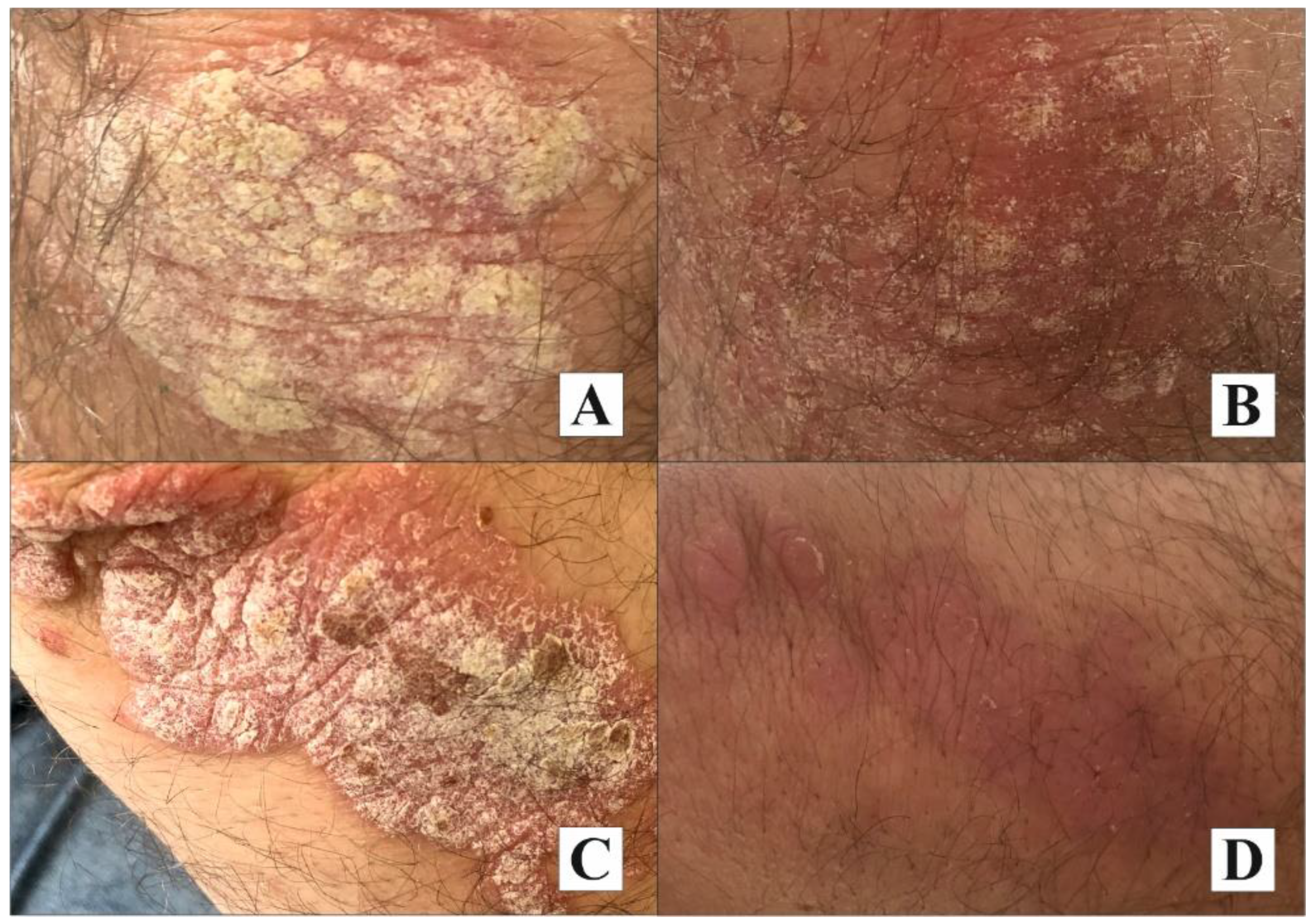
2.3. Results of the Clinical Assessment of Psoriatic Lesions
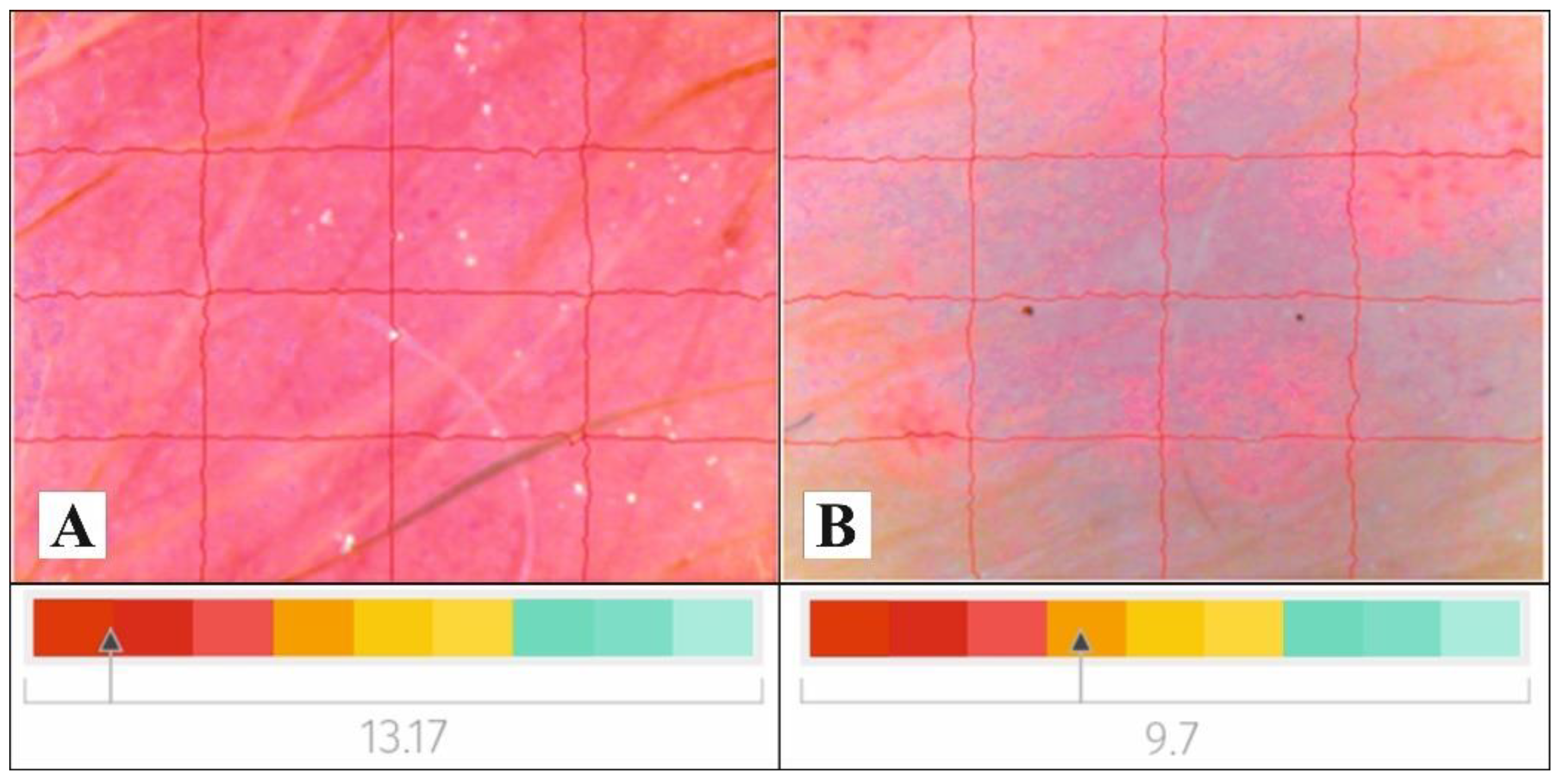
2.4. Measurements of Skin Biophysical Parameters
3. Discussion
4. Materials and Methods
4.1. Material
4.2. Study Group
4.3. Methods
4.3.1. Determination of Dominant Ecdysteroids in Creams Using the ESI/HPLC-MS Method
4.3.2. Clinical Assessment
4.3.3. Patch Tests
4.3.4. Measurement of Skin Biophysical Parameters
4.3.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Sample Availability
References
- Bélanger, A.; de Oliveira, C.P.; Maheux, M.; Pouliot, R. Plaque Psoriasis: Understanding Risk, Factors of This Inflammatory Skin Pathology. J. Cosmet. Dermatol. Sci. Appl. 2016, 6, 67–80. [Google Scholar] [CrossRef] [Green Version]
- Parisi, R.; Iskandar, I.Y.K.; Kontopantelis, E.; Augustin, M.; Griffiths, C.E.M.; Ashcroft, D.M. National, regional, and worldwide epidemiology of psoriasis: Systematic analysis and modeling study. Br. Med. J. 2020, 28, 369. [Google Scholar]
- Branisteanu, D.E.; Cojocaru, C.; Diaconu, R.; Porumb, E.A.; Alexa, A.I.; Nicolescu, A.C.; Brihan, I.; Bogdanici, C.M.; Branisteanu, G.; Dimitriu, A.; et al. Update on the etiopathogenesis of psoriasis (Review). Exp. Ther. Med. 2022, 23, 201. [Google Scholar] [CrossRef]
- Staubach, P.; Zimmer, S. Psoriasis vulgaris-mehr als eine Hauterkrankung Management der Psoriasis im 21. Jahrhundert [Plaque psoriasis-more than a skin disorder]. Med. Monatsschr. Pharm. 2017, 40, 231–233. [Google Scholar]
- Fredriksson, T.; Peterson, U. Severe psoriasis-oral therapy with a new retinoid. Dermatologica 1978, 157, 238–244. [Google Scholar] [CrossRef]
- Langley, R.G.; Ellis, C.N. Evaluating psoriasis with Psoriasis Area and Severity Index, Psoriasis Global Assessment and Lattice System Physician’s Global Assessment. J. Am. Acad. Dermatol. 2004, 51, 563–569. [Google Scholar] [CrossRef]
- Schmitt, J.; Wozel, G. The Psoriasis Area and Severity Index is the adequate criterion to define severity in chronic plaque -type psoriasis. Dermatology 2005, 210, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Tokuyama, M.; Mabuchi, T. New treatment addressing the pathogenesis of psoriasis. Int. J. Mol. Sci. 2020, 21, 7488. [Google Scholar] [CrossRef]
- Torsekar, R.; Gautam, M.M. Topical Therapies in Psoriasis. Indian Dermatol. Online J. 2017, 8, 235–245. [Google Scholar] [CrossRef]
- Alhammad, I.M.; Aseri, A.M.; Alqahtani, S.A.M.; Alshaebi, M.F.; Alqahtani, S.A.; Alzahrani, R.A.; Alhaji, A.A.; Alamoudi, M.K.; Bafarat, A.Y.; Jad, A.Y.; et al. A review on updates in management and treatment of psoriasis. Arch Pharma Pract. 2021, 12, 74–78. [Google Scholar] [CrossRef]
- Young, M.; Aldredge, L.; Parker, P. Psoriasis for the primary care practitioner. J. Am. Assoc. Nurse Pract. 2017, 29, 157–178. [Google Scholar] [CrossRef] [PubMed]
- Luger, T.; Seite, S.; Humbert, P.; Krutmann, J.; Triller, R.; Dréno, B. Recommendations for adjunctive basic skin care in patients with psoriasis. Eur. J. Dermatol. 2014, 24, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Cannavo, S.P.; Guarneri, F.; Giuffrida, R.; Aragona, E.; Guarneri, C. Evaluation of cutaneous surface parameters in psoriatic patients. Skin. Res. Technol. 2017, 23, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Onselen, J.V. An overview of psoriasis and the role of emollient therapy. Br. J. Community Nurs. 2013, 18, 174–179. [Google Scholar] [CrossRef]
- Hekmatpou, D.; Mehrabi, F.; Rahzani, K.; Aminiyan, A. The effect of Aloe Vera clinical trials on prevention and healing of skin wound: A systematic review. Iran. J. Med. Sci. 2019, 44, 1. [Google Scholar]
- Singh, K.K.; Tripathy, S. Natural treatment alternative for psoriasis: A review on herbal resources. J. Appl. Pharm. Sci. 2014, 4, 114–121. [Google Scholar]
- Hoffmann, J.; Gendrisch, F.; Schempp, C.M.; Wölfle, U. New herbal biomedicines for the topical treatment of dermatological disorders. Biomedicines 2020, 8, 27. [Google Scholar] [CrossRef] [Green Version]
- Loizzo, M.R.; Provenzano, E.; Menichini, F.; Tundis, R. Anti-psoriasis agents from natural plant sources. Cur. Med. Chem. 2016, 23, 1250–1267. [Google Scholar]
- Lin, Y.K.; See, L.C.; Huang, Y.H.; Chi, C.C.; Hui, R.C.Y. Comparison of indirubin concentrations in indigo naturalis ointment for psoriasis treatment: A randomized, double-blind, dosage-controlled trial. Br. J. Dermatol. 2018, 178, 124–131. [Google Scholar] [CrossRef]
- Frasheri, L.; Schielein, M.C.; Tizek, L.; Mikschl, P.; Biedermann, T.; Zink, A. Great green tea ingredient? A narrative literature review on epigallocatechin gallate and its biophysical properties for topical use in dermatology. Phytother. Res. 2020, 34, 2170–2179. [Google Scholar] [CrossRef]
- Pazyar, N.; Yaghoobi, R. Soybean: A potential antipsoriasis agent. Jundishapur. J. Nat. Pharm. Prod. 2015, 10, e20924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.J.; Wu, N.L.; Lee, G.A.; Hung, C.F. The therapeutic potential and molecular mechanism of isoflavone extract against psoriasis. Sci. Rep. 2018, 8, 6335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odinokov, V.N.; Galyautdinov, I.V.; Nedopekin, D.V.; Khalilov, L.M.; Shashkov, A.S.; Kachala, V.V.; Dinan, L.; Lafont, R. Phytoecdysteroids from the juice of Serratula coronata L. (Asteraceae). Insect. Biochem. Mol. Biol. 2002, 32, 161–165. [Google Scholar] [CrossRef]
- Nsimba, R.Y.; Kikuzaki Konisi, Y. Ecdysteroids act as inhibitors of calf skin collagenase and oxidative stress. J. Biochem. Mol. Toxicol. 2008, 22, 240–250. [Google Scholar] [CrossRef]
- Das, N.; Mishra, S.K.; Bishayee, A.; Ali, E.S.; Bishayee, A. The phytochemical, biological, and medicinal attributes of phytoecdysteroids: An updated review. Acta Pharm. Sin. B 2021, 11, 1740–1766. [Google Scholar] [CrossRef]
- Abraham, A.; Roga, G. Topical Steroid-Damaged Skin. Indian J. Dermatol. 2014, 59, 456–459. [Google Scholar] [CrossRef]
- Shawahna, R.; Jaradat, N.A. Ethnopharmacological survey of medicinal plants used by patients with psoriasis in the West Bank of Palestine. BMC Complemen. Altern. Med. 2017, 17, 4. [Google Scholar] [CrossRef] [Green Version]
- Kaur, A.; Kumar, S. Plants and plant products with potential antipsoriatic activity-a review. Pharm. Biol. 2012, 50, 1573–1591. [Google Scholar] [CrossRef] [Green Version]
- El-Gammal, A.; Di Nardo, V.; Daaboul, F.; Tchernev, G.; Wollina, U.; Lotti, J.; Lotti, T. Is There a Place for Local Natural Treatment of Psoriasis? Open. Access Maced. J. Med. Sci. 2018, 6, 839–842. [Google Scholar] [CrossRef] [Green Version]
- Akhdar, M.; Abedini, R.; Tavakolpour, S.; Gholibeigian, Z.; Azizpour, A. A randomized, double-blind, placebo-controlled trial of a commercial Aloe vera gel for mitigation of phototherapy side-effects in vitiligo patients. J. Herb. Med. 2021, 28, 100442. [Google Scholar] [CrossRef]
- Bylka, W.; Znajdek-Awiżeń, P.; Studzińska-Sroka, E.; Brzezińska, M. Centella asiatica in cosmetology. Adv. Dermatol. Allergol. 2013, 1, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Sampson, J.H.; Raman, A.; Karlsen, G.; Navsaria, H.; Leigh, I.M. In vitro keratinocyte antiproliferative effect of Centella asiatica extract and triterpenoid saponins. Phytomedicine 2001, 8, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Lorz, L.R.; Kim, M.-Y.; Cho, J.Y. Medicinal potential of Panax ginseng and its ginsenosides in atopic dermatitis treatment. J. Ginsen. Resg. 2020, 44, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.P.; PrakashDadhich, O.; Deepa. A review study of medicinal uses of manjishtha (Rubia Cordifolia). Int. J. Adv. Res. 2017, 5, 1394–1401. [Google Scholar] [CrossRef] [Green Version]
- Miraj, S. Pharmacological effects of Saccharum officinarum L. Pharm. Lett. 2016, 8, 223–225. [Google Scholar]
- Laekeman, G.; Vlietinck, A. Phytoecdysteroids: Phytochemistry and Pharmacological Activity. In Natural Products: Phytochemistry, Botany and Metabolism of Alkaloids, Phenolics and Terpenes; Ramawat, K.G., Mérillon, J.M., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 3827–3849. [Google Scholar]
- Dinan, L.; Balducci, C.; Guibout, L.; Lafont, R. Small-scale analysis of phytoecdysteroids in seeds by HPLC-DAD-MS for the identification and quantification of specific analogues, dereplication and chemotaxonomy. Phytochem. Anal. 2020, 31, 643–661. [Google Scholar] [CrossRef]
- Napierała, M.; Nawrot, J.; Gornowicz-Porowska, J.; Florek, E.; Moroch, A.; Adamski, Z.; Kroma, A.; Miechowicz, I.; Nowak, G. Separation and HPLC Characterization of Active Natural Steroids in a Standardized Extract from the S. coronata Herb with Antiseborrheic Dermatitis Activity. Int. J. Environ. Res. Public Health 2020, 17, 6453. [Google Scholar] [CrossRef]
- Goossens, A. Cosmetic Contact Allergens. Cosmetics 2016, 3, 5. [Google Scholar] [CrossRef] [Green Version]
- Denisow-Pietrzyk, M.; Pietrzyk, Ł.; Denisow, B. Asteraceae species as potential environmental factors of allergy. Environ. Sci. Pollut. Res. Int. 2019, 26, 6290–6300. [Google Scholar] [CrossRef] [Green Version]
- Rozas-Muñoz, E.; Lepoittevin, J.P.; Pujol, R.M.; Giménez-Arnau, A. Allergic Contact Dermatitis to Plants: Understanding the Chemistry will Help our Diagnostic Approach. Actas Dermo-Sifiliogr. 2012, 103, 456–477. [Google Scholar] [CrossRef]
- Kim, B.; Cho, H.-E.; Moon, S.H.; Ahn, H.-J.; Bae, S.; Cho, H.-D.; An, S. Transdermal delivery systems in cosmetics. Biomed. Dermatol. 2020, 4, 10. [Google Scholar] [CrossRef]
- Essendoubi, M.; Gobinet, C.; Reynaud, R.; Angiboust, J.F.; Manfait, M.; Piot, O. Human skin penetration of hyaluronic acid of different molecular weights as probed by Raman spectroscopy. Skin. Res. Technol. 2015, 22, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Fluhr, J.W.; Cavallotti, C.; Berardesca, E. Emollients, moisturizers and keratolytic agents in psoriasis. Clin. Dermatol. 2008, 26, 380–386. [Google Scholar] [CrossRef] [PubMed]
- Proksch, E. pH in nature, humans and skin. J. Dermatol. 2018, 45, 1044–1052. [Google Scholar] [CrossRef]
- Chan, A.; Mauro, T. Acidification in the epidermis and the role of secretory phospholipases. Dermatoendocrinology 2011, 3, 84–90. [Google Scholar] [CrossRef] [Green Version]
- Couteau, C.; Coiffard, L. Overview of skin whitening agents: Drugs and cosmetic products. Cosmetics 2016, 3, 27. [Google Scholar] [CrossRef]
- Bargo, P.R.; Kollias, N. Measurement of skin texture through polarization imaging. Br. J. Dermatol. 2009, 162, 724–731. [Google Scholar] [CrossRef]
- Rhodes, J.; Clay, C.; Phillips, M. The surface area of the hand and the palm for estimating percentage of total body surface area: Results of a meta-analysis. Br. J. Dermatol. 2013, 169, 76–84. [Google Scholar] [CrossRef]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clin. Exp. Dermatol. 1994, 19, 210–216. [Google Scholar] [CrossRef]
- Szepietowski, J.; Salomon, J.; Finlay, A.Y.; Klepacki, A.; Chodynicka, B.; Marionneau, N.; Taibc, C.; Myon, E. Wskaźnik wpływu dolegliwości skórnych na jakość życia-Dermatology Life Quality Index (DLQI): Polska wersja językowa. Dermatol. Klin. 2004, 6, 63–70. [Google Scholar]
- Long, C.C.; Finlay, A.Y. The finger-tip unit-a new practical measure. Clin. Exp. Dermatol. 1991, 16, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.D.; Aalto-Korte, K.; Agner, T.; Andersen, K.E.; Bircher, A.; Bruze, M.; Cannavó, A.; Giménez-Arnau, A.; Gonçalo, M.; Goossens, A.; et al. European Society of Contact Dermatitis guideline for diagnostic patch testing-recommendations on best practice. Contact Dermat. 2015, 73, 195–221. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics of Psoriatic Lesions | Cream 0 (n = 17) | Cream 1 (n = 20) | Cream 2 (n = 18) | Cream 3 (n = 15) | |
|---|---|---|---|---|---|
| Area (cm2) | Baseline mean ± SD | 14.8 ± 21.2 | 17.4 ± 22.7 | 20.1 ± 33.1 | 14.1 ± 14.2 |
| follow-up mean ± SD | 14.6 ± 20.8 | 14.6 ± 20.1 | 19.0 ± 32.8 | 12.4 ± 12.8 | |
| p value | 0.0679 | 0.0015 * | 0.0176 * | 0.0179 * | |
| Erythema (points) | Baseline M(range) | 2 (1–4) | 2 (1–3) | 2 (1–4) | 2 (1–4) |
| follow-up M (range) | 1 (1–4) | 1 (1–3) | 1 (0–4) | 1 (0–3) | |
| p value | 0.0175 * | <0.0001 * | 0.0032 * | <0.0001 * | |
| Infiltration (points) | Baseline M (range) | 1 (0–3) | 2 (0–4) | 1 (0–3) | 2 (1–4) |
| follow-up M (range) | 0 (0–3) | 0.5 (0–2) | 0 (0–1) | 0 (0–2) | |
| p value | 0.0336 | <0.0001 * | 0.0022 | <0.0001 * | |
| Scaling (points) | Baseline M (range) | 1 (0–2) | 2 (0–3) | 1 (0–3) | 2 (0–3) |
| follow-up M (range) | 1 (0–2) | 1 (0–2) | 0.5 (0–2) | 1 (0–3) | |
| p value | >0.05 | <0.0001 * | <0.0001 * | <0.0001 * | |
| Parameter | Cream 0 (n = 17) | Cream 1 (n = 20) | Cream 2 (n = 18) | Cream 3 (n = 15) | Comparison between Creams (p) | |
|---|---|---|---|---|---|---|
| Melanin Index (AU) | Baseline Mean ± SD | 148.5 ± 79.9 | 164.5 ± 79.8 | 150.0 ± 37.8 | 199.8 ± 88.8 | 0.1576 |
| follow-up Mean ± SD | 141.1 ± 57.8 | 150.9 ± 65.9 | 127.2 ± 28.0 | 150.8 ± 67.9 | 0.6286 | |
| p value | 0.9811 | 0.1259 | 0.0057 * | 0.0007 * | ||
| Erythema Index (AU) | Baseline Mean ± SD | 409.9 ±113.2 | 407.8 ± 108.6 | 402.4 ± 89.1 | 409.4 ± 105.3 | 0.9870 |
| follow-up Mean ± SD | 435.2 ± 74.7 | 437.3 ± 89.0 | 433.2 ± 76.3 | 456.4 ± 106.2 | 0.6611 | |
| p value | 0.0684 | 0.4115 | 0.0854 | 0.1118 | ||
| pH | Baseline Mean ± SD | 5.54 ± 0.52 | 5.79 ± 0.81 | 5.77 ± 0.49 | 5.9 ± 0.9 | 0.6953 |
| follow-up Mean ± SD | 5.56 ± 0.51 | 5.72 ± 0.78 | 5.54 ± 0.81 | 5.25 ± 0.47 | 0.1184 | |
| p value | 0.5862 | 0.5862 | 0.0166 * | 0.0066 * | ||
| Hydration (AU) | Baseline Mean ± SD | 12.5 ± 7.8 | 10.2 ± 7.6 | 13.1 ± 11.6 | 12.1 ± 6.9 | 0.7626 |
| follow-up Mean ± SD | 17.6 ± 8.5 | 19.6 ± 8.6 | 15.9 ± 8.5 | 18.5 ± 8.2 | 0.2016 | |
| p value | 0.0003 * | 0.0001 * | 0.0936 | 0.0076 * | ||
| TEWL (g/h/m2) | Baseline Mean ± SD | 23.1 ± 9.8 | 21.4 ± 12.1 | 21.4 ± 8.8 | 21.7 ± 9.6 | 0.8672 |
| follow-up Mean ± SD | 16.9 ± 8.8 | 14.4 ± 6.6 | 17.8 ± 6.2 | 16.4 ± 9.3 | 0.3453 | |
| p value | 0.0003 * | 0.0001 * | 0.0582 | 0.0108 * | ||
| Creams | Composition | Ingredient Content (g) |
|---|---|---|
| 0 | Lekobaza® (placebo) | 30 |
| 1 | Lekobaza®/S. coronata extract | 27/3 |
| 2 | Lekobaza®/salicylic acid | 25/5 |
| 3 | Lekobaza®/S. coronata extract/salicylic acid | 22/3/5 |
| Parameter (Mean ± SD) | All (n = 70) | Female (n = 36) | Male (n = 34) |
|---|---|---|---|
| Age [years] | 41.1 ± 13.1 | 41.1 ± 13.2 | 41.1 ± 13.2 |
| PASI [points] | 4.2 ± 2.9 | 3.0 ± 1.8 | 5.4 ± 3.4 |
| BSA [%] | 2.7 ± 0.5 | 2.8 ± 0.4 | 2.7 ± 0.4 |
| DLQI [points] | 5.2 ± 3.2 | 5.2 ± 3.3 | 5.2 ± 3.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kroma, A.; Pawlaczyk, M.; Feliczak-Guzik, A.; Urbańska, M.; Jenerowicz, D.; Seraszek-Jaros, A.; Kikowska, M.; Gornowicz-Porowska, J. Phytoecdysteroids from Serratula coronata L. for Psoriatic Skincare. Molecules 2022, 27, 3471. https://doi.org/10.3390/molecules27113471
Kroma A, Pawlaczyk M, Feliczak-Guzik A, Urbańska M, Jenerowicz D, Seraszek-Jaros A, Kikowska M, Gornowicz-Porowska J. Phytoecdysteroids from Serratula coronata L. for Psoriatic Skincare. Molecules. 2022; 27(11):3471. https://doi.org/10.3390/molecules27113471
Chicago/Turabian StyleKroma, Anna, Mariola Pawlaczyk, Agnieszka Feliczak-Guzik, Maria Urbańska, Dorota Jenerowicz, Agnieszka Seraszek-Jaros, Małgorzata Kikowska, and Justyna Gornowicz-Porowska. 2022. "Phytoecdysteroids from Serratula coronata L. for Psoriatic Skincare" Molecules 27, no. 11: 3471. https://doi.org/10.3390/molecules27113471