
Expression of Somatostatin Receptor Subtypes (SSTR-1–SSTR-5) in Pediatric Hematological and Oncological Disorders

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Results
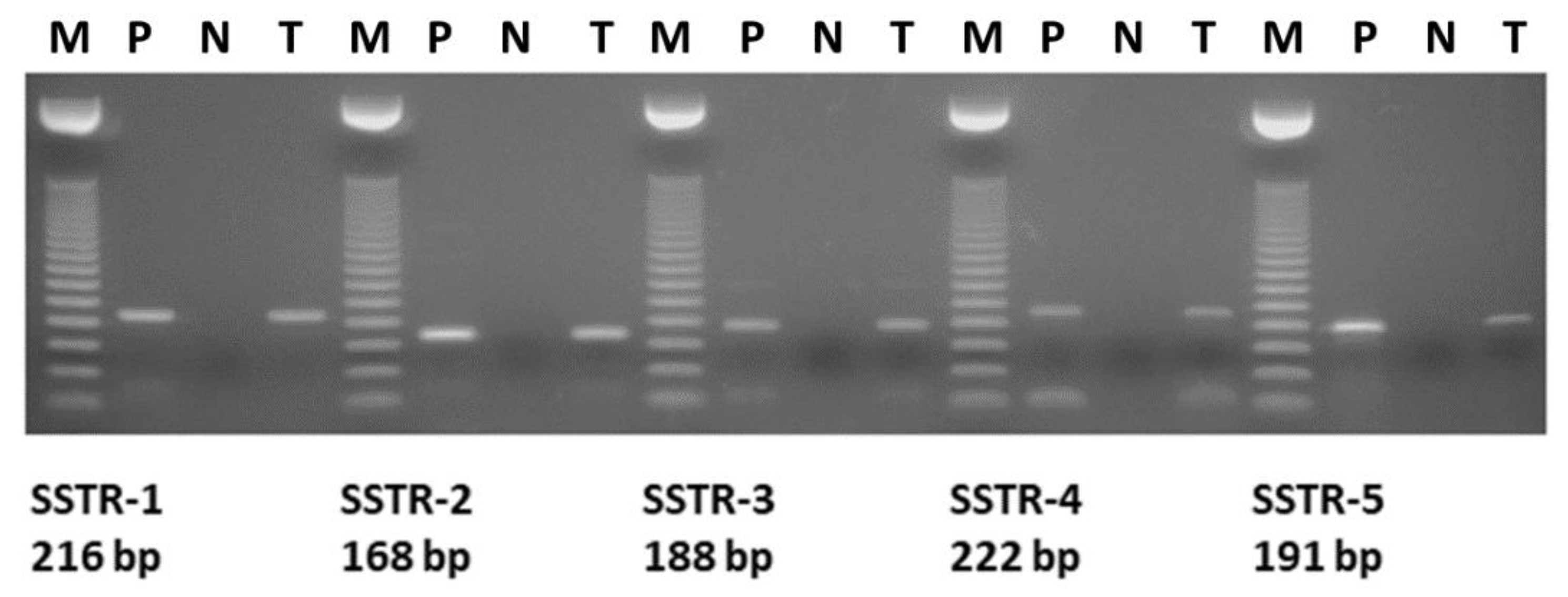
2.1. Expression of SSTRs in Human Pediatric Solid Tumors and Hematological Diseases
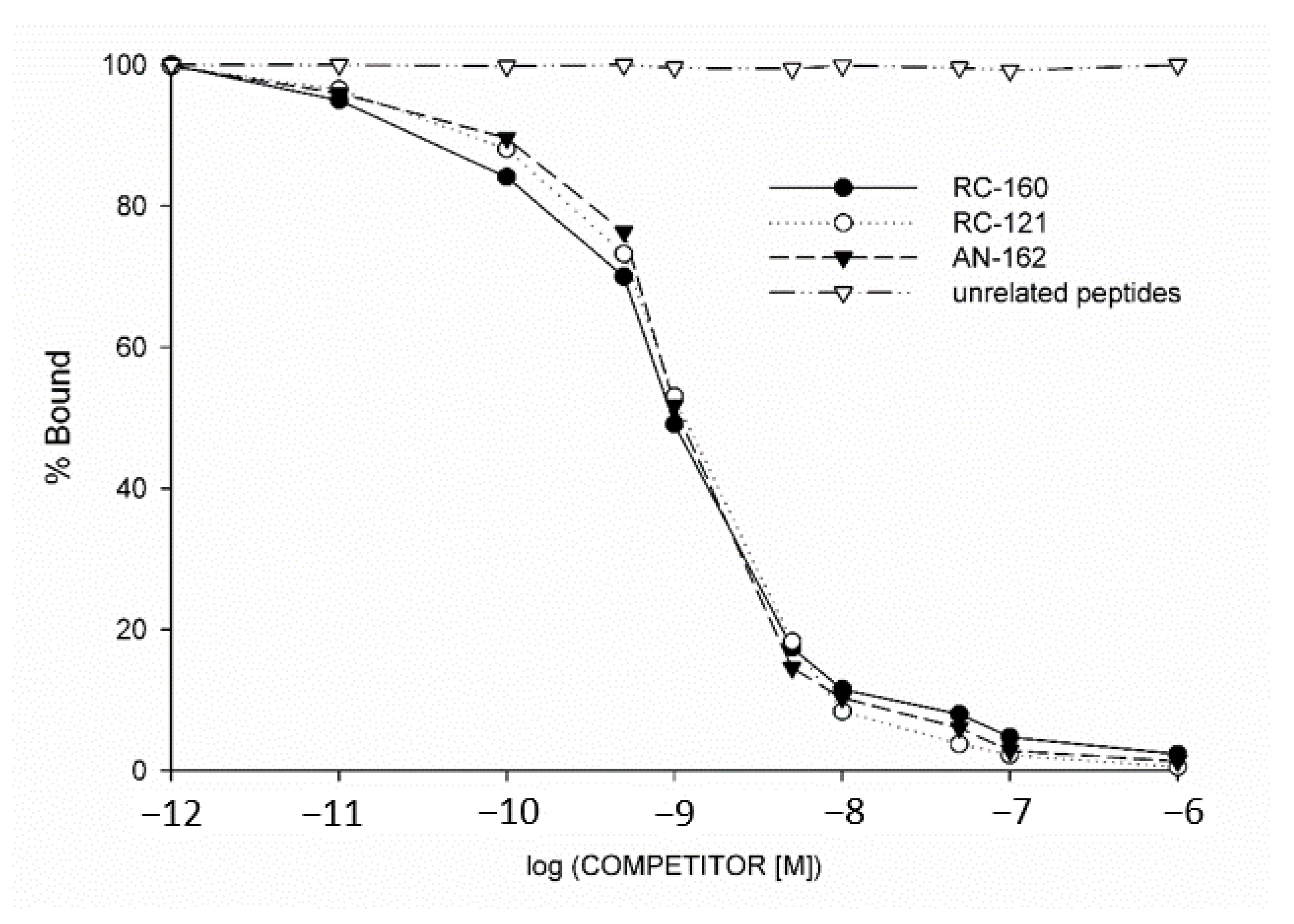
2.2. Radioligand Binding Studies
2.3. Patient Follow-Up
3. Discussion
4. Materials and Methods
4.1. Human Samples
4.2. Histology
4.3. RNA Isolation
4.4. RT-PCR Analysis of Total RNA Samples
4.5. Radioligand Binding Studies
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Drastikova, M.; Beranek, M.; Gabalec, F.; Netuka, D.; Masopust, V.; Cesak, T.; Marek, J.; Palicka, V.; Cap, J. Expression profiles of somatostatin, dopamine, and estrogen receptors in pituitary adenomas determined by means of synthetic multilocus calibrators. Biomed. Pap. 2016, 160, 238–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reubi, J.C.; Laissue, J.; Krenning, E.; Lamberts, S.W. Somatostatin receptors in human cancer: Incidence, characteristics, functional correlates and clinical implications. J. Steroid Biochem. Mol. Biol. 1992, 43, 27–35. [Google Scholar] [CrossRef]
- Cakir, M.; Dworakowska, D.; Grossman, A. Somatostatin receptor biology in neuroendocrine and pituitary tumours: Part 2—Clinical implications. J. Cell. Mol. Med. 2010, 14, 2585–2591. [Google Scholar] [CrossRef] [PubMed]
- Schally, A.V.; Halmos, G. Targeting to peptide receptors. In Drug Delivery in Oncology; Wiley-VCH Verlag GmbH & Co. KGaA: Weinheim, Germany, 2012; pp. 1219–1261. [Google Scholar]
- Harda, K.; Szabo, Z.; Szabo, E.; Olah, G.; Fodor, K.; Szasz, C.; Mehes, G.; Schally, A.V.; Halmos, G. Somatostatin receptors as molecular targets in human uveal melanoma. Molecules 2018, 23, 1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halmos, G.; Schally, A.V.; Sun, B.; Davis, R.; Bostwick, D.G.; Plonowski, A. High expression of somatostatin receptors and messenger ribonucleic acid for its receptor subtypes in organ-confined and locally advanced human prostate cancers. J. Clin. Endocrinol. Metab. 2000, 85, 2564–2571. [Google Scholar] [PubMed] [Green Version]
- Schally, A.V.; Comaru-Schally, A.M.; Nagy, A.; Kovacs, M.; Szepeshazi, K.; Plonowski, A.; Varga, J.L.; Halmos, G. Hypothalamic hormones and cancer. Front. Neuroendocr. 2001, 22, 248–291. [Google Scholar] [CrossRef]
- Halmos, G.; Sun, B.; Schally, A.V.; Hebert, F.; Nagy, A. Human ovarian cancers express somatostatin receptors. J. Clin. Endocrinol. Metab. 2000, 85, 3509–3512. [Google Scholar] [CrossRef]
- Reubi, J.C.; Schaer, J.C.; Laissue, J.A.; Waser, B. Somatostatin receptors and their subtypes in human tumors and in peritumoral vessels. Metabolism 1996, 45, 39–41. [Google Scholar] [CrossRef]
- Patel, Y.C.; Greenwood, M.T.; Panetta, R.; Demchyshyn, L.; Niznik, H.; Srikant, C.B. The somatostatin receptor family. Life Sci. 1995, 57, 1249–1265. [Google Scholar] [CrossRef]
- Reisine, T.; Bell, G.I. Molecular biology of somatostatin receptors. Endocr. Rev. 1995, 16, 427–442. [Google Scholar]
- Patel, Y.C.; Srikant, C.B. Somatostatin Receptors. Trends Endocrinol. Metab. 1997, 8, 398–405. [Google Scholar] [CrossRef]
- Susini, C.; Buscail, L. Rationale for the use of somatostatin analogs as antitumor agents. Ann. Oncol. 2006, 17, 1733–1742. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.C.; Srikant, C.B. Subtype selectivity of peptide analogs for all five cloned human somatostatin receptors (hsstr 1–5). Endocrinology 1994, 135, 2814–2817. [Google Scholar] [CrossRef] [PubMed]
- Patel, Y.C. Molecular pharmacology of somatostatin receptor subtypes. J. Endocrinol. Investig. 1997, 20, 348–367. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Porras, M.; Cárdenas-Salas, J.; Álvarez-Escolá, C. Somatostatin Analogs in Clinical Practice: A Review. Int. J. Mol. Sci. 2020, 21, 1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreff, M.; Schulz, S.; Handel, M.; Keilhoff, G.; Braun, H.; Pereira, G.; Klutzny, M.; Schmidt, H.; Wolf, G.; Hollt, V. Distribution, targeting, and internalization of the sst4 somatostatin receptor in rat brain. J. Neurosci. 2000, 20, 3785–3797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, W.; Chen, J.; Cao, X.; Yang, M.; Zhu, J.; Zhao, G. Solitary infantile myofibromatosis in the bones of the upper extremities: Two rare cases and a review of the literature. Oncol. Lett. 2013, 6, 1406–1408. [Google Scholar] [CrossRef] [Green Version]
- Mashiah, J.; Hadj-Rabia, S.; Dompmartin, A.; Harroche, A.; Laloum-Grynberg, E.; Wolter, M.; Amoric, J.C.; Hamel-Teillac, D.; Guero, S.; Fraitag, S.; et al. Infantile myofibromatosis: A series of 28 cases. J. Am. Acad. Dermatol. 2014, 71, 264–270. [Google Scholar] [CrossRef]
- Larralde, M.; Ferrari, B.; Martinez, J.P.; Barbieri, M.A.F.; Mendez, J.H.; Casas, J. Infantile myofibromatosis. An. Bras. Dermatol. 2017, 92, 854–857. [Google Scholar] [CrossRef]
- Letelier, C.; Gunther, M.; Alarcon, A.; Vera, P.; Kakarieka, E.; Pantoja, R. Agressive pediatric myofibromatosis in a two-year-old child. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 216–219. [Google Scholar] [CrossRef]
- Coppit, G.L., III; Perkins, J.A.; Manning, S.C. Nasopharyngeal teratomas and dermoids: A review of the literature and case series. Int. J. Pediatric Otorhinolaryngol. 2000, 52, 219–227. [Google Scholar] [CrossRef]
- Woodward, P.J.; Sohaey, R.; Kennedy, A.; Koeller, K.K. From the archives of the afip: A comprehensive review of fetal tumors with pathologic correlation. Radiographics 2005, 25, 215–242. [Google Scholar] [CrossRef] [PubMed]
- Ognjanovic, S.; Linabery, A.M.; Charbonneau, B.; Ross, J.A. Trends in childhood rhabdomyosarcoma incidence and survival in the united states, 1975–2005. Cancer 2009, 115, 4218–4226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esparza, S.D.; Sakamoto, K.M. Topics in pediatric leukemia—Acute lymphoblastic leukemia. Medscape Gen. Med. 2005, 7, 23. [Google Scholar]
- Bernt, K.M.; Hunger, S.P. Current concepts in pediatric philadelphia chromosome-positive acute lymphoblastic leukemia. Front. Oncol. 2014, 4, 54. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA A Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Brown, P.; Inaba, H.; Annesley, C.; Beck, J.; Colace, S.; Dallas, M.; DeSantes, K.; Kelly, K.; Kitko, C.; Lacayo, N.; et al. Pediatric acute lymphoblastic leukemia, version 2.2020, nccn clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 81–112. [Google Scholar] [CrossRef] [Green Version]
- James, R.M.; Kinsey, S.E. The investigation and management of chronic neutropenia in children. Arch. Dis. Child. 2006, 91, 852–858. [Google Scholar] [CrossRef] [Green Version]
- Dale, D.C. How I manage children with neutropenia. Br. J. Haematol. 2017, 178, 351–363. [Google Scholar] [CrossRef] [Green Version]
- Gresh, R. Overview of pediatric cancer. In MSD Manual; Nemours/Alfred I. duPont Hospital for Children: Wilmington, NC, USA, 2019. [Google Scholar]
- Minard-Colin, V.; Auperin, A.; Pillon, M.; Burke, G.A.A.; Barkauskas, D.A.; Wheatley, K.; Delgado, R.F.; Alexander, S.; Uyttebroeck, A.; Bollard, C.M.; et al. Rituximab for high-risk, mature b-cell non-hodgkin’s lymphoma in children. N. Engl. J. Med. 2020, 382, 2207–2219. [Google Scholar] [CrossRef]
- Vegi, N.M.; Chakrabortty, S.; Zegota, M.M.; Kuan, S.L.; Stumper, A.; Rawat, V.P.S.; Sieste, S.; Buske, C.; Rau, S.; Weil, T.; et al. Somatostatin receptor mediated targeting of acute myeloid leukemia by photodynamic metal complexes for light induced apoptosis. Sci. Rep. 2020, 10, 371. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; de Reuver, P.R.; Gill, P.; Andrici, J.; D’Urso, L.; Mittal, A.; Pavlakis, N.; Clarke, S.; Samra, J.S.; Gill, A.J. Somatostatin Receptor SSTR-2a Expression Is a Stronger Predictor for Survival Than Ki-67 in Pancreatic Neuroendocrine Tumors. Medicine 2015, 94, e1281. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, S.; Reubi, J.C.; Kalkner, K.M.; Laissue, J.A.; Horisberger, U.; Olerud, C.; Westlin, J.E. Metastatic hormone-refractory prostatic adenocarcinoma expresses somatostatin receptors and is visualized in vivo by [111in]-labeled dtpa-d-[phe1]-octreotide scintigraphy. Cancer Res. 1995, 55, 5805–5810. [Google Scholar]
- Kaemmerer, D.; Trager, T.; Hoffmeister, M.; Sipos, B.; Hommann, M.; Sanger, J.; Schulz, S.; Lupp, A. Inverse expression of somatostatin and cxcr4 chemokine receptors in gastroenteropancreatic neuroendocrine neoplasms of different malignancy. Oncotarget 2015, 6, 27566–27579. [Google Scholar] [CrossRef] [PubMed]
- Kumar, U.; Grant, M. Somatostatin and somatostatin receptors. Results Probl. Cell Differ. 2010, 50, 137–184. [Google Scholar] [CrossRef] [PubMed]
- Albers, A.R.; O’Dorisio, M.S. Clinical use of somatostatin analogues in paediatric oncology. Digestion 1996, 57, 38–41. [Google Scholar] [CrossRef]
- Dishop, M.K.; Kuruvilla, S. Primary and metastatic lung tumors in the pediatric population: A review and 25-year experience at a large children’s hospital. Arch. Pathol. Lab. Med. 2008, 132, 1079–1103. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Sample Type | SSTR-1 | SSTR-2 | SSTR-3 | SSTR-4 | SSTR-5 | SSTR | |
|---|---|---|---|---|---|---|---|---|
| Kd (nM) | Bmax (fmol/mg Protein) | |||||||
| 1 | Teratoma | - | + | - | + | - | 5.76 | 274.0 |
| 2 | Myofibromatosis | - | + | - | - | - | 6.85 | 273.3 |
| 3 | Fibrous dysplasia | - | + | - | - | - | 4.94 | 255.1 |
| 4 | Hodgkin lymphoma | + | + | + | + | + | 8.01 | 760.8 |
| 5 | Rhabdomyosarcoma | + | + | - | + | + | 8.12 | 505.1 |
| 6 | Rhabdomyosarcoma | + | + | + | + | - | 4.31 | 371.4 |
| 7 | Hamartoma | + | + | - | + | - | 4.02 | 297.9 |
| 8 | Acute lymphoblastic leukemia | + | + | + | - | - | N/A | |
| 9 | Acute lymphoblastic leukemia | + | + | - | - | - | N/A | |
| 10 | Acute lymphoblastic leukemia | + | + | - | - | - | N/A | |
| 11 | Acute lymphoblastic leukemia | - | + | - | + | - | N/A | |
| 12 | Acute lymphoblastic leukemia | - | + | - | + | - | N/A | |
| 13 | Immune thrombocytopenia | - | + | - | - | - | N/A | |
| 14 | Hereditary spherocytosis | + | + | + | + | - | N/A | |
| 15 | Chronic benign neutropenia | + | + | - | + | - | N/A | |
| Compound | IC50 Values (nM) | |
|---|---|---|
| Hodgkin Lymphoma (Patient No.4) | Rhabdomyosarcoma (Patient No.5) | |
| RC-160 (Vapreotide®) | 0.86 | 0.73 |
| RC-121 | 1.04 | 0.92 |
| AN-162 | 1.53 | 1.19 |
| Sample | Histological Type | Gender | Sample Type | Age at Sample Collection | 5-Year Survival |
|---|---|---|---|---|---|
| 1 | Teratoma/adenocarcinoma component | Male | Mediastinal tumor tissue | 14.5 year | died |
| 2 | Juvenile myofibromatosis | Male | Right hip bone tumor tissue | 2 year | alive |
| 3 | Fibrous dysplasia | Female | Bone tumor tissue | 10.5 year | alive |
| 4 | Hodgkin lymphoma | Female | Lymph node | 15 year | alive |
| 5 | Rhabdomyosarcoma | Male | Pelvic tumor tissue | 12.5 year | died |
| 6 | Rhabdomyosarcoma | Female | Neck mass biopsy | 8 year | died |
| 7 | Benign mesenchymal hamartoma | Male | Mediastinal mass | 4 year | alive |
| 8 | Acute lymphoblastic leukemia | Female | Bone marrow | 5 year | alive |
| 9 | Acute lymphoblastic leukemia | Male | Bone marrow | 13 year | alive |
| 10 | Acute lymphoblastic leukemia | Male | Bone marrow | 9.5 year | died |
| 11 | Acute lymphoblastic leukemia | Male | Bone marrow | 6.5 year | alive |
| 12 | Acute lymphoblastic leukemia | Male | Peripheral blood | 15 year | died |
| 13 | Immune thrombocytopenia | Male | Bone marrow | 10 month | alive |
| 14 | Hereditary spherocytosis | Female | Bone marrow | 9 month | alive |
| 15 | Chronic benign neutropenia | Male | Bone marrow | 12.5 month | alive |
| SSTR-1 sense | 5′-TAT CTG CCT GTG CTA CGT GC-3’(1 exon) |
| SSTR-1 antisense | 5’-GAT GAC CGA CAG CTG ACT CA-3′(1 exon) |
| SSTR-2 sense | 5′-CGG AGT GAC AGT AAG CAG GA-3′(1 exon) |
| SSTR-2 antisense | 5′-CGA AGC CAG TGT GGG TAGG-3′(1 exon) |
| SSTR-3 sense | 5’-TGA GTC ACC AAC GTC TAC ATCC-3’(1 exon) |
| SSTR-3 antisense | 5’-ACG CTC ATG ACA GTC AGG C-3’(1 exon) |
| SSTR-4 sense | 5′-CGC TAC GCC AAG ATG AAG A-3′(1 exon) |
| SSTR-4 antisense | 5′-AGA CAG AAG ACG CTG GTG AA-3′(1 exon) |
| SSTR-5 sense | 5’-CGT CTT CAT CAT CTA CAC GG-3’(1 exon) |
| SSTR-5 antisense | 5’-GGC CAG GTT GAC GAT GTT GA-3’(1 exon) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harda, K.; Szabo, Z.; Juhasz, E.; Dezso, B.; Kiss, C.; Schally, A.V.; Halmos, G. Expression of Somatostatin Receptor Subtypes (SSTR-1–SSTR-5) in Pediatric Hematological and Oncological Disorders. Molecules 2020, 25, 5775. https://doi.org/10.3390/molecules25235775
Harda K, Szabo Z, Juhasz E, Dezso B, Kiss C, Schally AV, Halmos G. Expression of Somatostatin Receptor Subtypes (SSTR-1–SSTR-5) in Pediatric Hematological and Oncological Disorders. Molecules. 2020; 25(23):5775. https://doi.org/10.3390/molecules25235775
Chicago/Turabian StyleHarda, Kristof, Zsuzsanna Szabo, Eva Juhasz, Balazs Dezso, Csongor Kiss, Andrew V. Schally, and Gabor Halmos. 2020. "Expression of Somatostatin Receptor Subtypes (SSTR-1–SSTR-5) in Pediatric Hematological and Oncological Disorders" Molecules 25, no. 23: 5775. https://doi.org/10.3390/molecules25235775