
ECG Signal Classification Using Deep Learning Techniques Based on the PTB-XL Dataset


Abstract
:1. Introduction
2. Materials and Methods
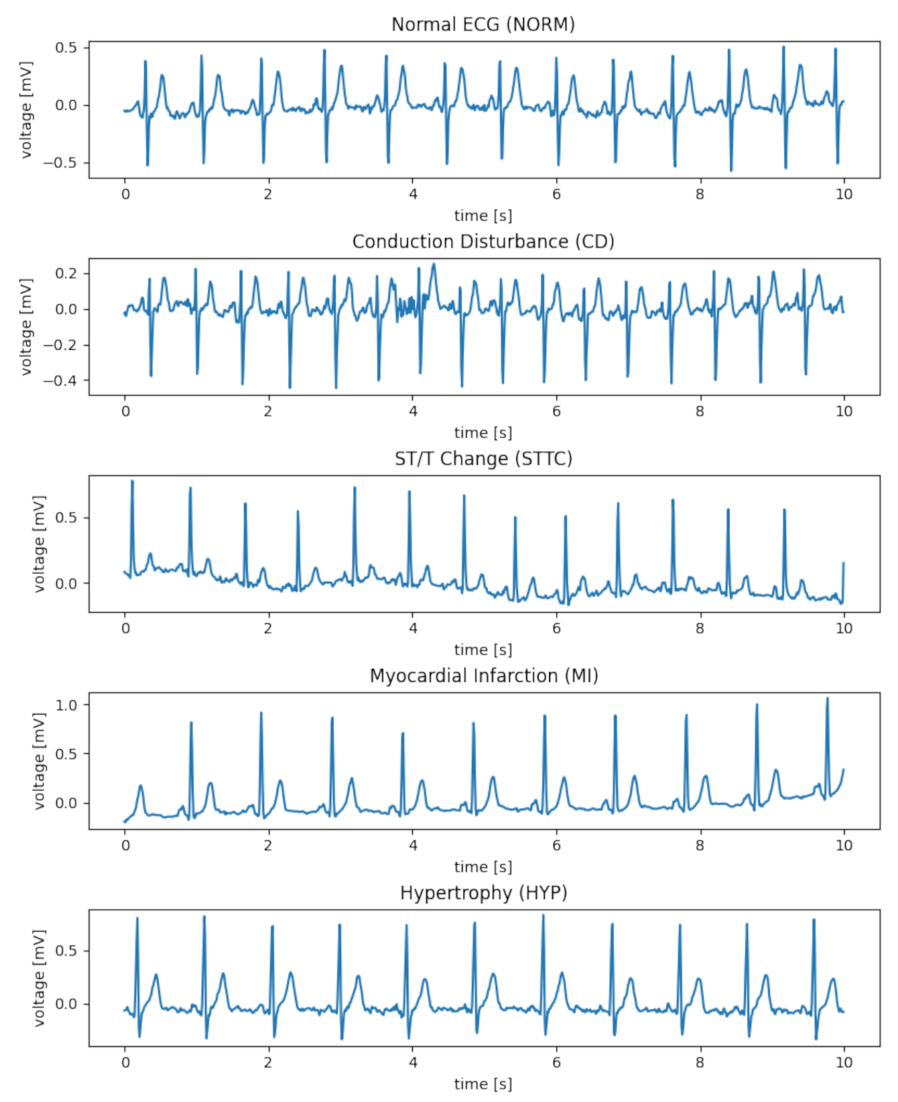
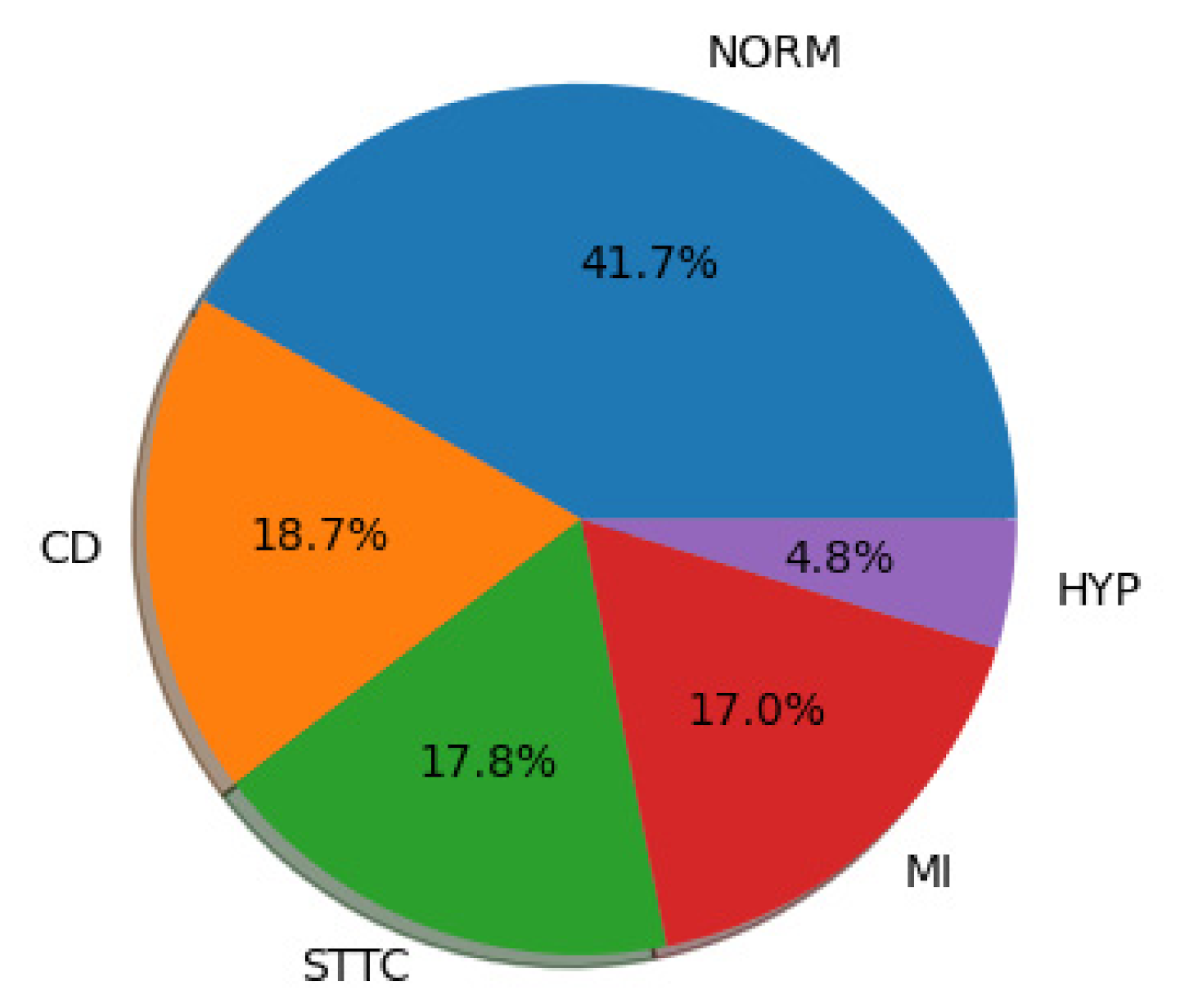
2.1. PTB-XL Dataset
2.2. Designed Network Architectures
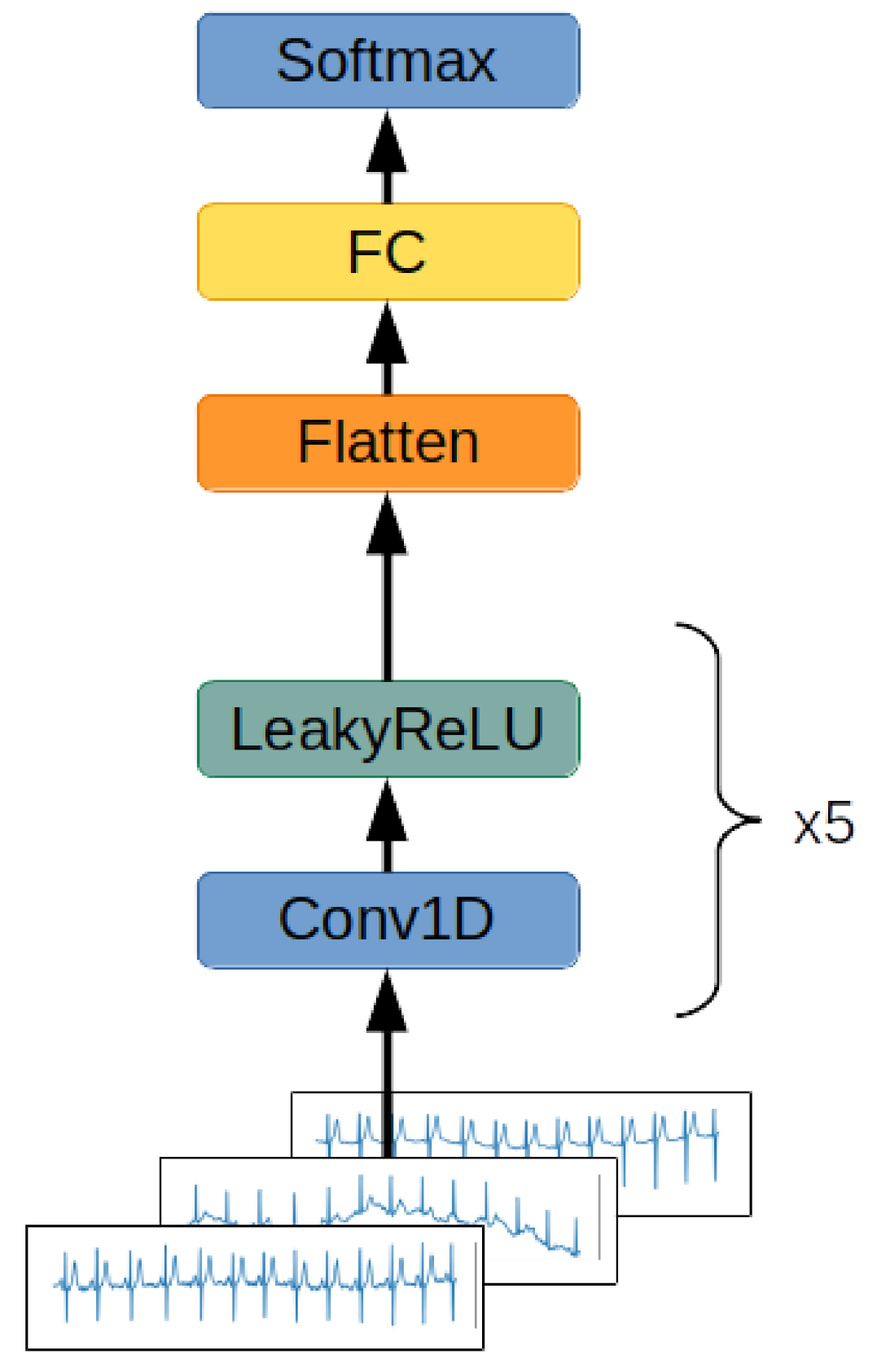
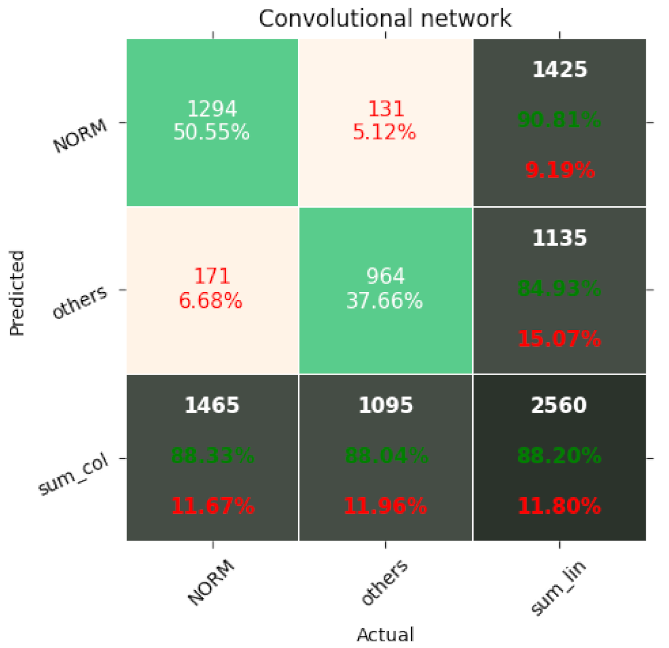
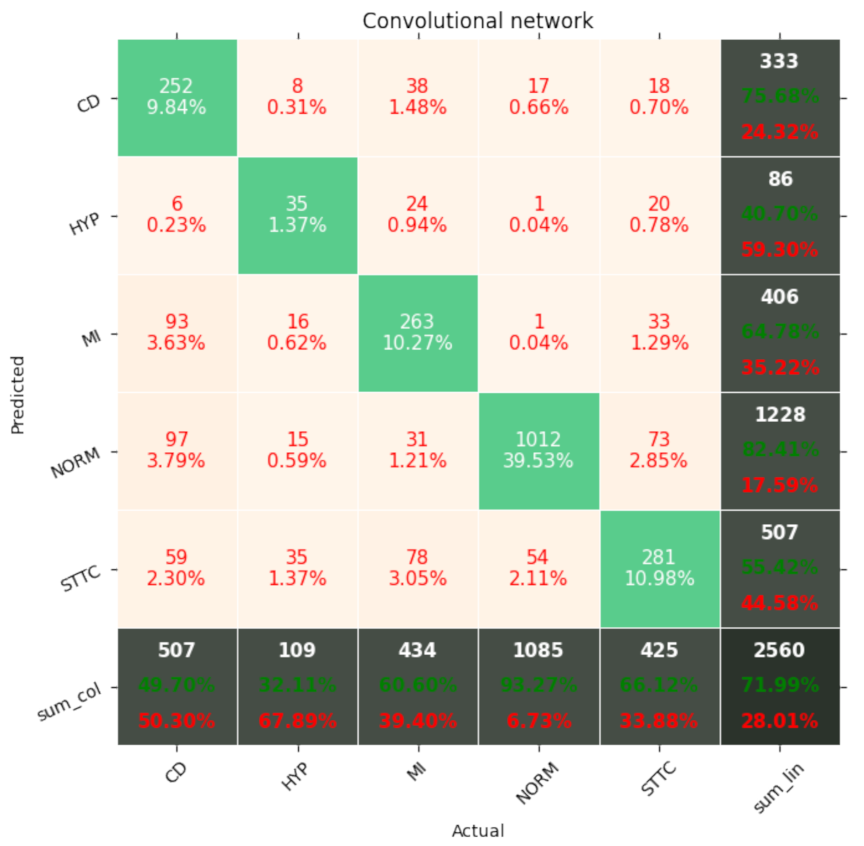
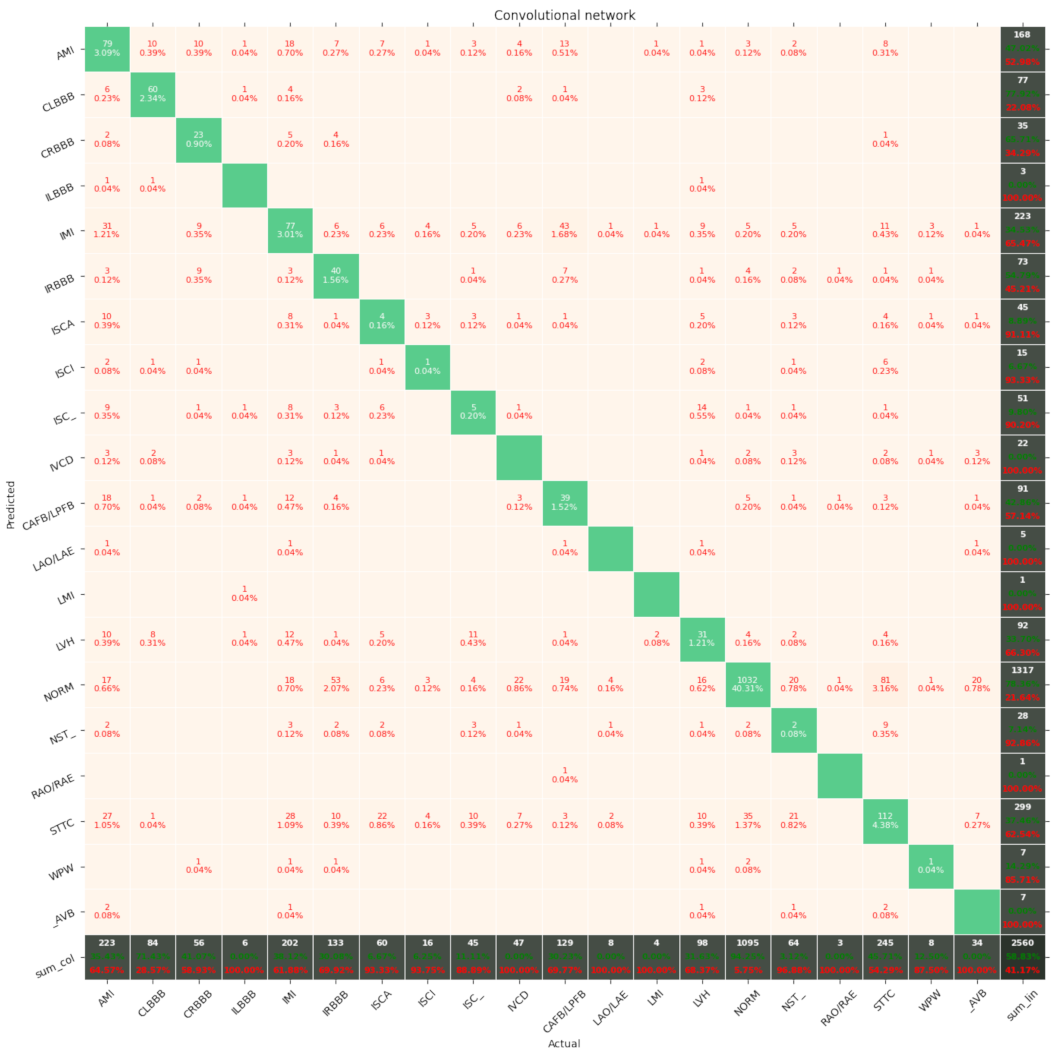
2.2.1. Convolutional Network
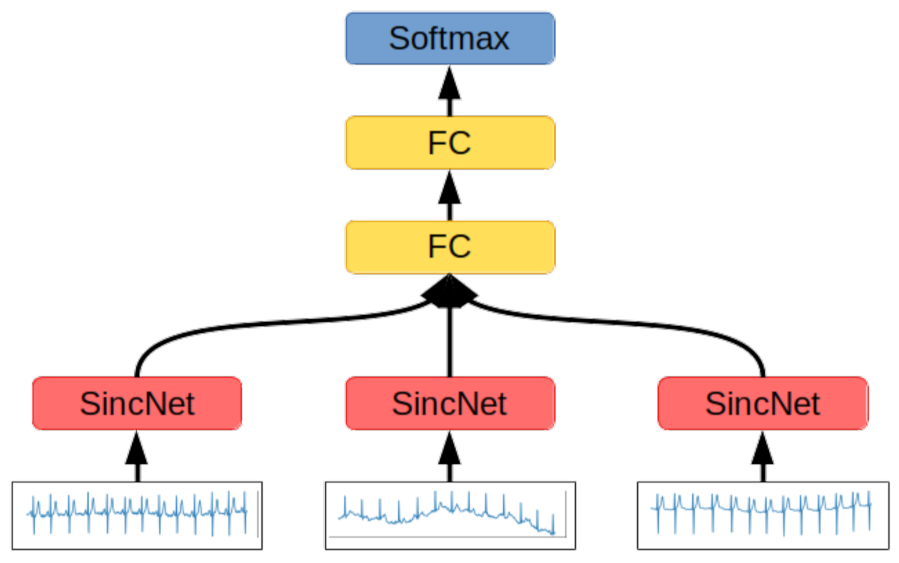
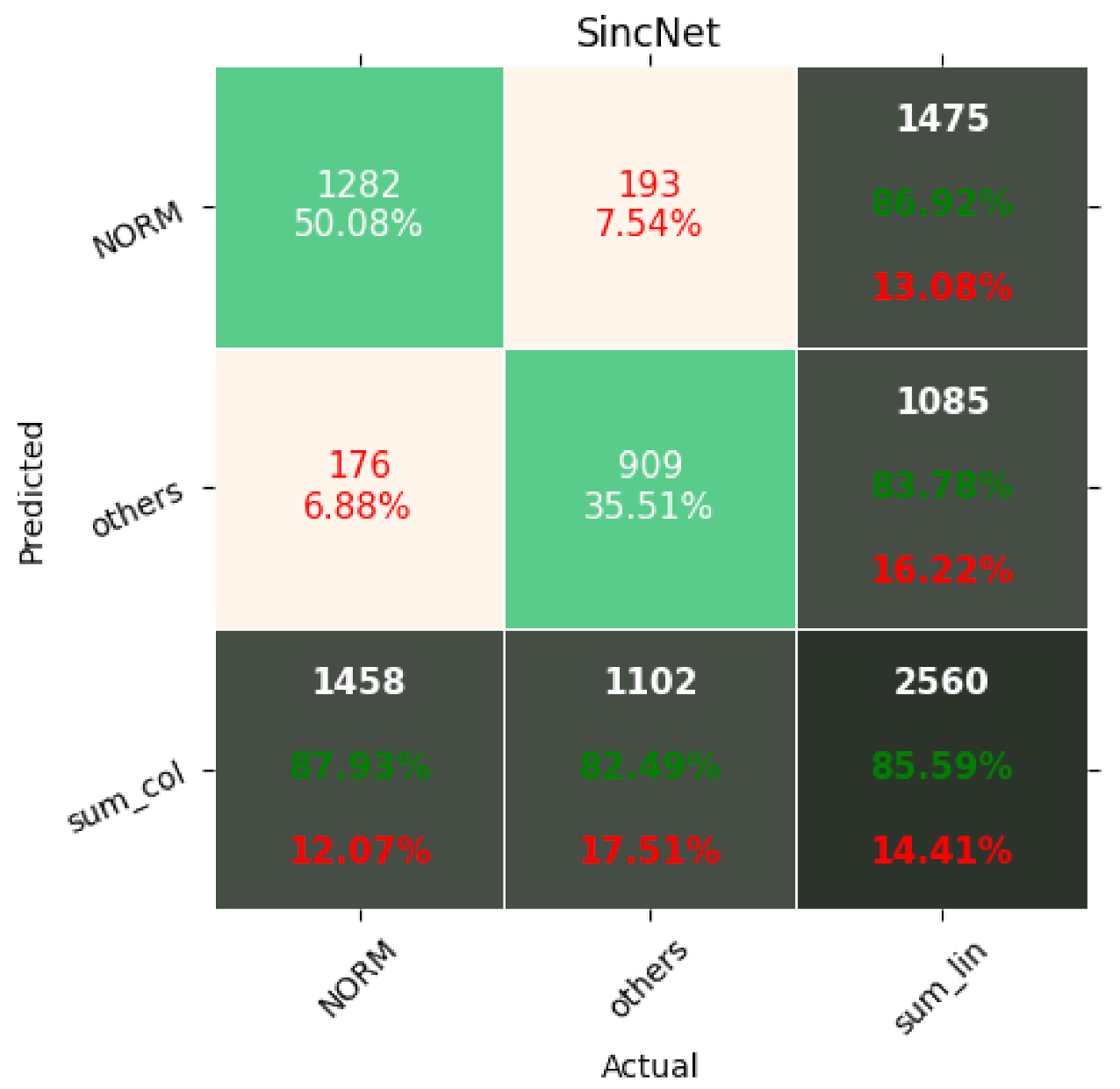
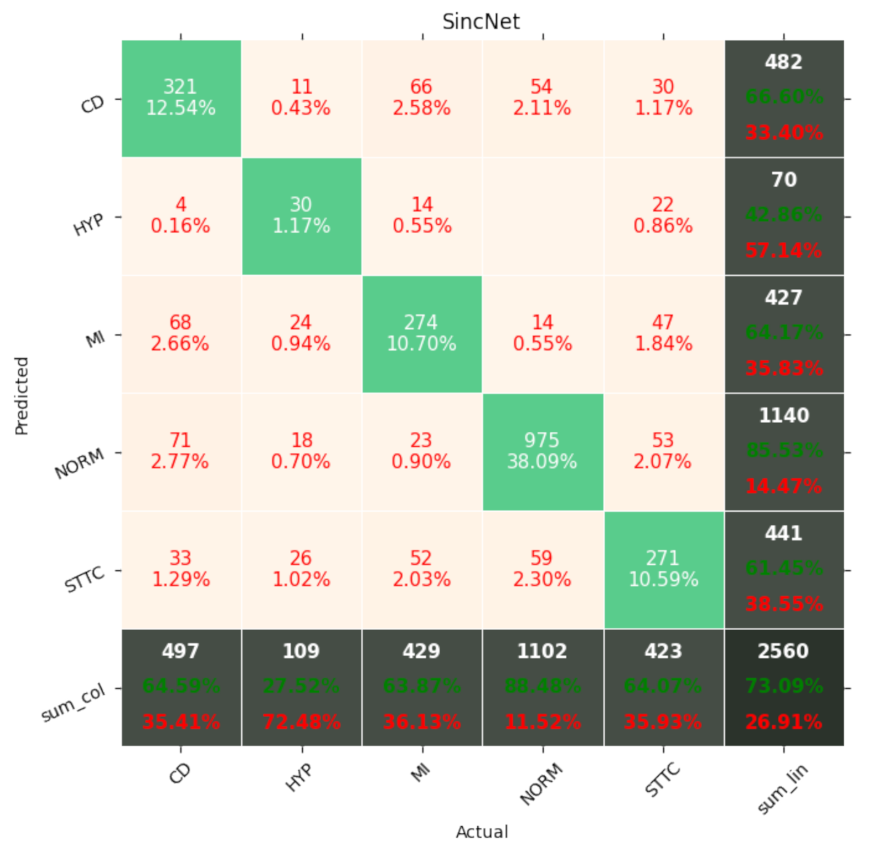
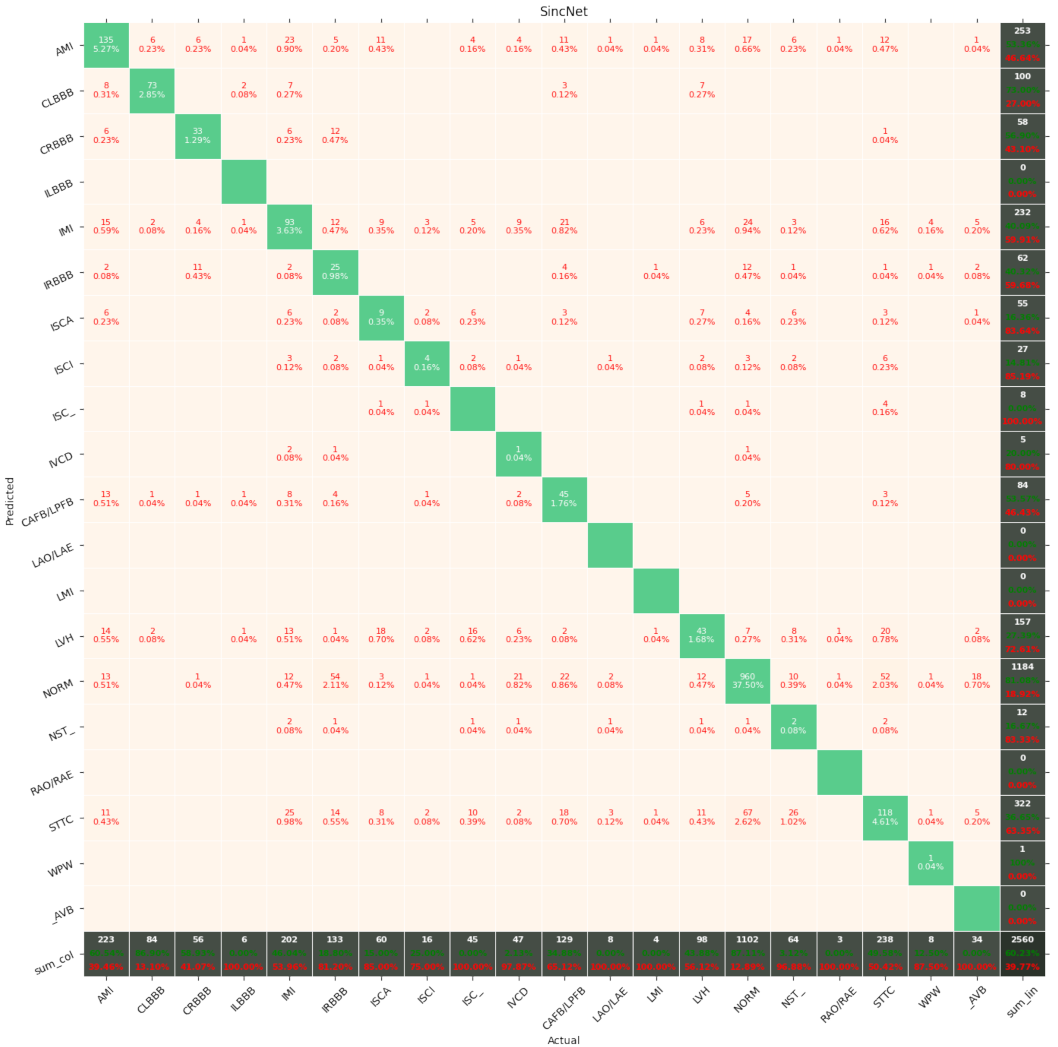
2.2.2. SincNet
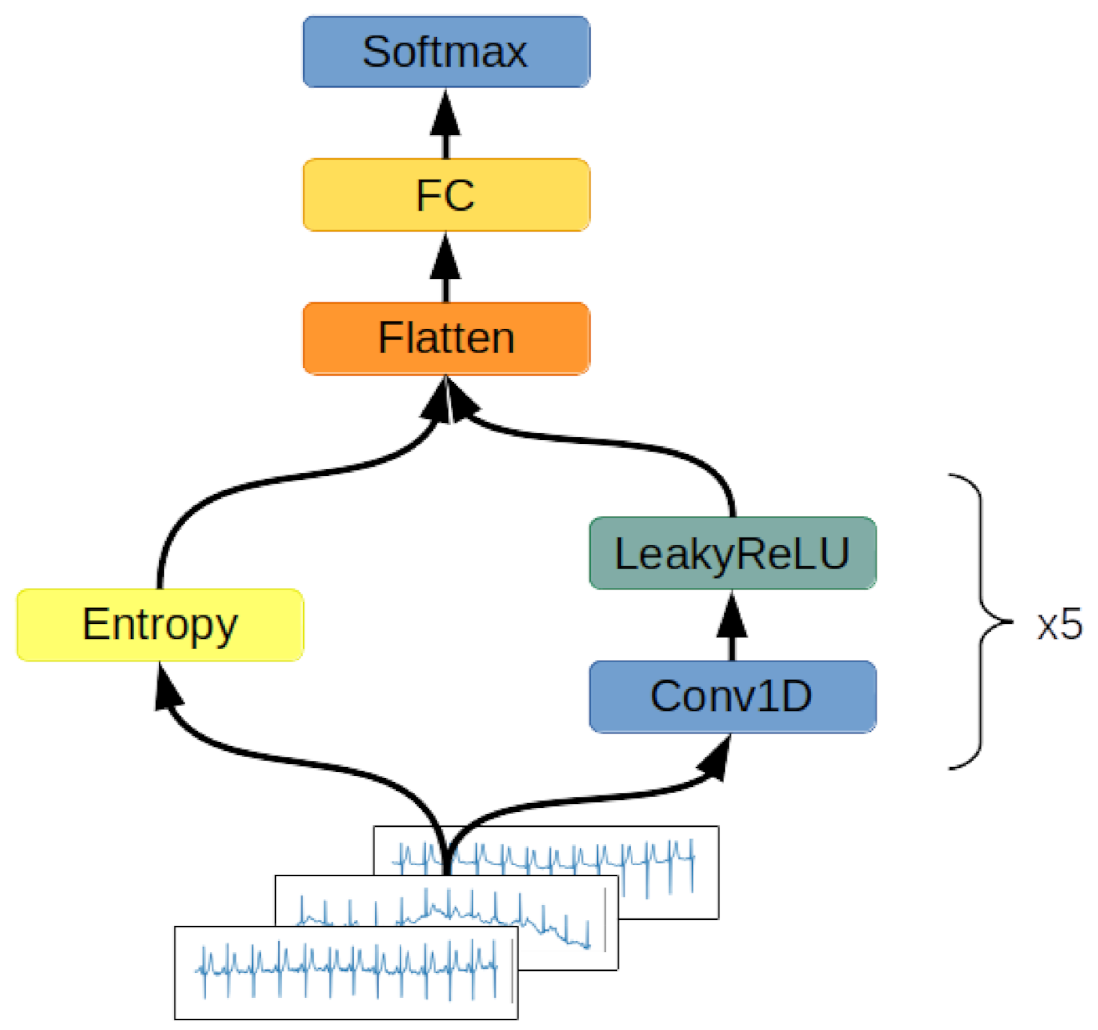
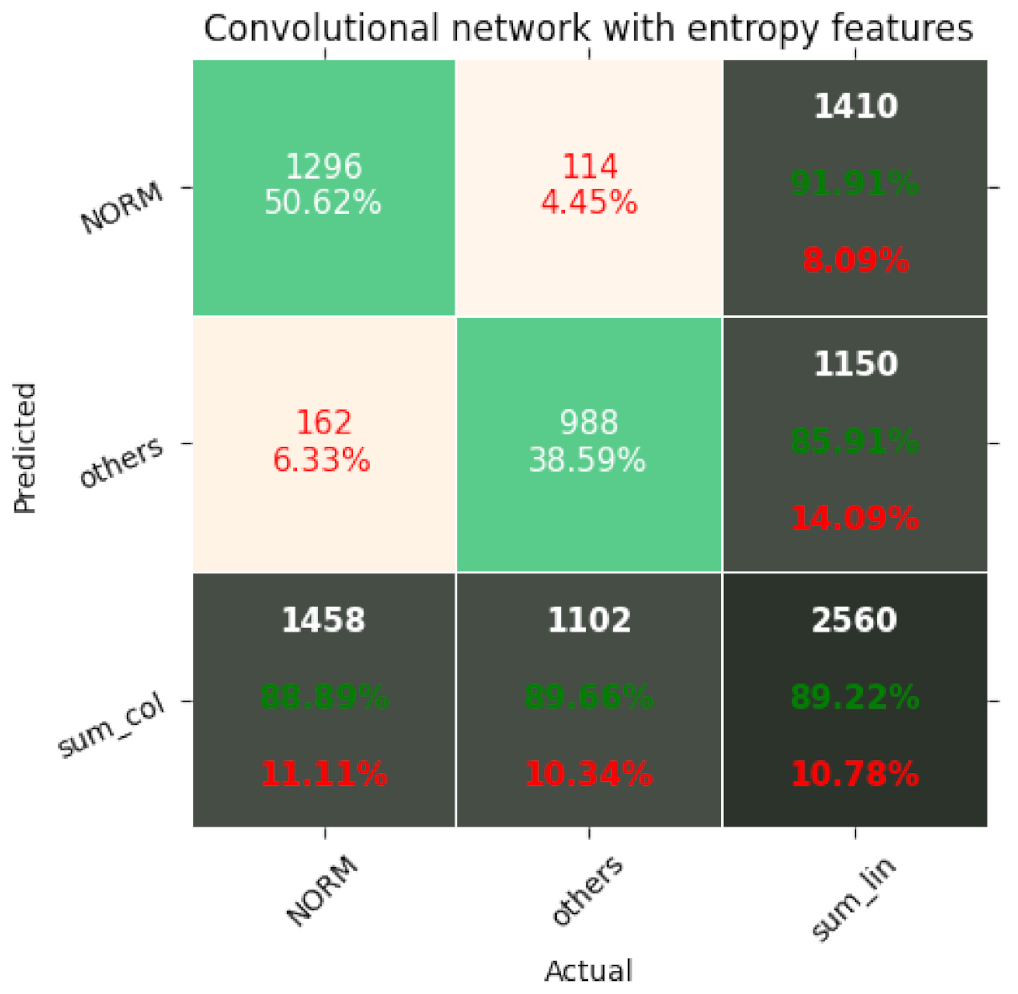
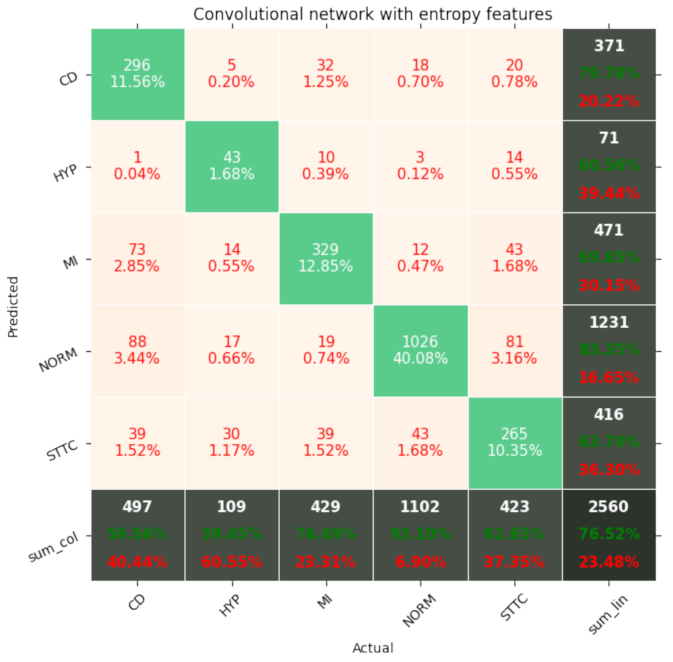
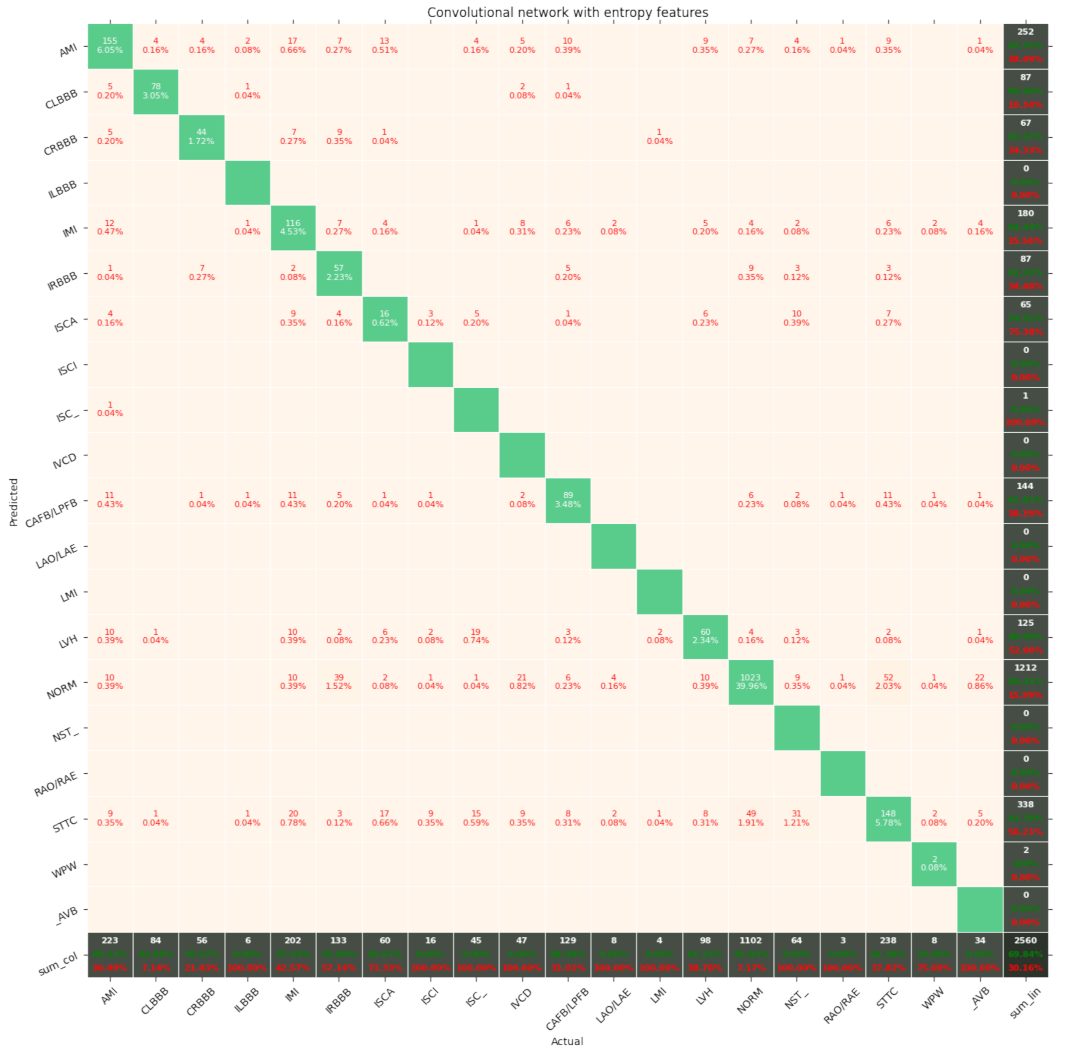
2.2.3. Convolutional Network with Entropy Features
- Shannon entropy—the summation of the informativeness of every possible state in the signal by measuring its probability. As a result, Shannon entropy is the measurement of the spread of the data [27];
- Approximate entropy—the measurement of series regularity. It provides information on how much the ECG fluctuates and its predictability [28];
- Sample entropy—an improvement on approximate entropy due to the lack of the signal length’s impact on the entropy computations [28];
- Permutation entropy—the measurement of the order relations between ECG samples. This quantifies how regular and deterministic the signal is [29];
- Spectral entropy—the quantification of the energy spread uniformness across the frequency spectrum [30];
- SVD entropy—the measurement of how possible the dimensionality reduction of time series matrix is through factorization using the eigenvector approach;
- Rényi entropy—the generalization of the Shannon entropy by introducing the fractal order of the subsequent informativeness of each signal’s state [31];
- Tsallis entropy—the generalization of the Boltzmann–Gibbs entropy, able to detect long-term memory effects on the signal [32];
- Extropy—the measurement of the amount of uncertainty represented by the distribution of the values in the observed ECG signal [33].
2.3. Metrics
- Accuracy: Acc = (TP + TN)/(TP + FP + TN + FN);
- Precision = TP/(TP + FP);
- Recall = TP/(TP + FN);
- F1 = 2 * precision * recall/(precision + recall);
- AUC—area under the curve, ROC—area under the receiver operating characteristic curve. The ROC is a curve determined by calculating TFP = true positive rate = TP/(TP + FN) and FPR = false positive rate = FP/(TN + FP). The false positive rate describes the x-axis and the true positive rate the y-axis of a coordinate system. By changing the threshold value responsible for the classification of an example as belonging to either the positive or negative class, pairs of TFP-FPR are generated, resulting in the creation of the ROC curve. The AUC is a measurement of the area below the ROC curve;
- Total Params—number of neurons in the network. The smaller this number, the better, as less computation is required in order to perform classification.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics—2018 update: A report from the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Bajpai, B.; Dhiman, G.; Soni, M.; Gomathi, S.; Mane, D. Review of ECG arrhythmia classification using deep neural network. Mater. Today Proc. 2021. In Press. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Noncommunicable Diseases; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Bogun, F.; Anh, D.; Kalahasty, G.; Wissner, E.; Serhal, C.B.; Bazzi, R.; Weaver, W.D.; Schuger, C. Misdiagnosis of atrial fibrillation and its clinical consequences. Am. J. Med. 2004, 117, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Schläpfer, J.; Wellens, H.J. Computer-interpreted electrocardiograms: Benefits and limitations. J. Am. Coll. Cardiol. 2017, 70, 1183–1192. [Google Scholar] [CrossRef]
- Houssein, E.H.; Kilany, M.; Hassanien, A.E. ECG signals classification: A review. Int. J. Intell. Eng. Informatics 2017, 5, 376–396. [Google Scholar] [CrossRef]
- Jambukia, S.H.; Vipul, K.D.; Harshadkumar, B.P. Classification of ECG signals using machine learning techniques: A survey. In Proceedings of the 2015 International Conference on Advances in Computer Engineering and Applications, Ghaziabad, India, 19–20 March 2015. [Google Scholar]
- Macfarlane, P.W.; Devine, B.; Clark, E. The university of Glasgow (Uni-G) ECG analysis program. In Proceedings of the Computers in Cardiology, Lyon, France, 25–28 September 2005. [Google Scholar]
- Wang, J.; Qiao, X.; Liu, C.; Wang, X.; Liu, Y.; Yao, L.; Zhang, H. Automated ECG classification using a non-local convolutional block attention module. Comput. Methods Programs Biomed. 2021, 203, 106006. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E.; et al. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [Green Version]
- Wagner, P.; Strodthoff, N.; Bousseljot, R.; Samek, W.; Schaeffter, T. PTB-XL, a large publicly available electrocardiography dataset (version 1.0.1). Sci. Data 2020, 7, 1–5. [Google Scholar] [CrossRef]
- Jia, W.; Xu, X.; Xu, X.; Sun, Y.; Liu, X. Automatic Detection and Classification of 12-lead ECGs Using a Deep Neural Network. In Proceedings of the Computing in Cardiology, Rimini, Italy, 13–16 September 2020; pp. 1–4. [Google Scholar]
- Zhu, Z.; Lan, X.; Zhao, T.; Guo, Y.; Kojodjojo, P.; Xu, Z.; Liu, Z.; Liu, S.; Wang, H.; Sun, X.; et al. Identification of 27 abnormalities from multi-lead ECG signals: An ensembled SE_ResNet framework with sign loss function. Physiol. Meas. 2021, 42, 065008. [Google Scholar] [CrossRef]
- Strodthoff, N.; Wagner, P.; Schaeffter, T.; Samek, W. Deep learning for ECG analysis: Benchmarks and insights from PTB-XL. arXiv 2020, arXiv:2004.13701. [Google Scholar] [CrossRef]
- Smisek, R.; Nemcova, A.; Marsanova, L.; Smital, L.; Vitek, M.; Kozumplik, J. Cardiac Pathologies Detection and Classification in 12-lead ECG. In Proceedings of the Computing in Cardiology, Rimini, Italy, 13–16 September 2020; pp. 1–4. [Google Scholar]
- Zhang, D.; Yang, S.; Yuan, X.; Zhang, P. Interpretable deep learning for automatic diagnosis of 12-lead electrocardiogram. Iscience 2021, 4, 102373. [Google Scholar] [CrossRef]
- Warrick, P.A.; Lostanlen, V.; Eickenberg, M.; Andén, J.; Homsi, M.N. Arrhythmia Classification of 12-lead Electrocardiograms by Hybrid Scattering-LSTM Networks. In Proceedings of the Computing in Cardiology, Rimini, Italy, 13–16 September 2020; pp. 1–4. [Google Scholar]
- Acharya, U.R.; Fujita, H.; Adam, M.; Lih, O.S.; Hong, T.J.; Sudarshan, V.K.; Koh, J.E. Automated characterization of arrhythmias using nonlinear features from tachycardia ECG beats. In Proceedings of the 2016 IEEE International Conference on Systems, Man, and Cybernetics (SMC), Budapest, Hungary, 9–12 October 2016. [Google Scholar]
- Jo, Y.Y.; Cho, Y.; Lee, S.Y.; Kwon, J.M.; Kim, K.H.; Jeon, K.H.; Cho, S.; Park, J.; Oh, B.H. Explainable artificial intelligence to detect atrial fibrillation using electrocardiogram. Int. J. Cardiol. 2021, 328, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Lepek, M.; Pater, A.; Muter, K.; Wiszniewski, P.; Kokosińska, D.; Salamon, J.; Puzio, Z. 12-lead ECG Arrythmia Classification Using Convolutional Neural Network for Mutually Non-Exclusive Classes. In Proceedings of the Computing in Cardiology, Rimini, Italy, 13–16 September 2020; pp. 1–4. [Google Scholar]
- Ramaraj, E.; Virgeniya, S.C. A Novel Deep Learning based Gated Recurrent Unit with Extreme Learning Machine for Electrocardiogram (ECG) Signal Recognition. Biomed. Signal Process. Control 2021, 68, 102779. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Caruana, R.; Lawrence, S.; Giles, L. Overfitting in neural nets: Backpropagation, conjugate gradient, and early stopping. In Proceedings of the 14th Annual Neural Information Processing Systems Conference, Denver, CO, USA, 27 November–2 December 2020; pp. 402–408. [Google Scholar]
- Ravanelli, M.; Yoshua, B. Speaker recognition from raw waveform with sincnet. In Proceedings of the 2018 IEEE Spoken Language Technology Workshop (SLT), Athens, Greece, 18–21 December 2018. [Google Scholar]
- Molau, S.; Pitz, M.; Schluter, R.; Ney, H. Computing Mel-frequency cepstral coefficients on the power spectrum. In Proceedings of the 2001 IEEE International Conference on Acoustics, Speech, and Signal Processing, Salt Lake City, UT, USA, 7–11 May 2001. [Google Scholar]
- Shannon, C. A mathematical theory of communication. Bell Syst. Tech. J. 1948, 27, 379–423. [Google Scholar] [CrossRef] [Green Version]
- Richman, J.S.; Moorman, J.R. Physiological time-series analysis using approximate entropy and sample entropy. Am. J. Physiol.-Heart Circ. Physiol. 2000, 278, H2039–H2049. [Google Scholar] [CrossRef] [Green Version]
- Bandt, C.H.; Bernd, P. Permutation entropy: A natural complexity measure for time series. Phys. Rev. Lett. 2002, 88, 174102. [Google Scholar] [CrossRef]
- Inouye, T.; Shinosaki, K.; Sakamoto, H.; Toi, S.; Ukai, S.; Iyama, A.; Katsuda, Y.; Hirano, M. Quantification of EEG irregularity by use of the entropy of the power spectrum. Electroencephalogr. Clin. Neurophysiol. 1991, 79, 204–210. [Google Scholar] [CrossRef]
- Renyi, A. On measures of entropy and information. In Proceedings of the Fourth Berkeley Symposium on Mathematical Statistics and Probability, Volume 1: Contributions to the Theory of Statistics; University of California Press: Oakland, CA, USA, 1961; pp. 547–561. [Google Scholar]
- Bezerianos, A.; Tong, S.; Thakor, N. Time dependent entropy of EEG rhythm changes following brain ischemia. Ann. Biomed. Eng. 2003, 31, 221–232. [Google Scholar] [CrossRef]
- Lad, F.; Sanfilippo, G.; Agrò, G. Extropy: A complementary dual of entropy. arXiv 2011, arXiv:1109.6440. [Google Scholar] [CrossRef]
- Granero-Belinchón, C.; Roux, S.G.; Garnier, N.B. Information Theory for Non-Stationary Processes with Stationary Increments. Entropy 2019, 21, 1223. [Google Scholar] [CrossRef] [Green Version]
















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Records | Class | Description |
|---|---|---|
| 7185 | NORM | Normal ECG |
| 3232 | CD | Myocardial Infarction |
| 3064 | STTC | ST/T Change |
| 2936 | MI | Conduction Disturbance |
| 815 | HYP | Hypertrophy |
| Number of Records | Subclass | Class | Description |
|---|---|---|---|
| 7185 | NORM | NORM | Normal ECG |
| 1713 | STTC | STTC | Non-diagnostic T abnormalities, suggests digitalis effect, long QT interval, ST-T changes compatible with ventricular aneurysm, compatible with electrolyte abnormalities |
| 1636 | AMI | MI | Anterior myocardial infarction, anterolateral myocardial infarction, in anteroseptal leads, in anterolateral leads, in lateral leads |
| 1272 | IMI | MI | Inferior myocardial infarction, inferolateral myocardial infarction, inferoposterolateral myocardial infarction, inferoposterior myocardial infarction, in inferior leads, in inferolateral leads |
| 881 | LAFB/LPFB | CD | Left anterior fascicular block, left posterior fascicular block |
| 798 | IRBBB | CD | Incomplete right bundle branch block |
| 733 | LVH | HYP | Left ventricular hypertrophy |
| 527 | CLBBB | CD | (Complete) left bundle branch block |
| 478 | NST_ | STTC | Nonspecific ST changes |
| 429 | ISCA | STTC | In anterolateral leads, in anteroseptal leads, in lateral leads, in anterior leads |
| 385 | CRBBB | CD | (Complete) right bundle branch block |
| 326 | IVCD | CD | Nonspecific intraventricular conduction disturbance |
| 297 | ISC_ | STTC | Ischemic ST-T changes |
| 204 | _AVB | CD | First-degree AV block, second-degree AV block, third-degree AV block |
| 147 | ISCI | STTC | In inferior leads, in inferolateral leads |
| 67 | WPW | CD | Wolff–Parkinson–White syndrome |
| 49 | LAO/LAE | HYP | Left atrial overload/enlargement |
| 44 | ILBBB | CD | Incomplete left bundle branch block |
| 33 | RAO/RAE | HYP | Right atrial overload/enlargement |
| 28 | LMI | MI | Lateral myocardial infarction |
| Number of Classes | Acc | Avg Precision | Avg Recall | Avg F1 | Avg AUC | Total Params |
|---|---|---|---|---|---|---|
| 2 | 0.882 | 0.879 | 0.882 | 0.88 | 0.953 | 8882 |
| 5 | 0.72 | 0.636 | 0.602 | 0.611 | 0.877 | 11,957 |
| 20 | 0.589 | 0.259 | 0.228 | 0.238 | 0.856 | 27,332 |
| Number of Classes | Acc | Avg Precision | Avg Recall | Avg F1 | Avg AUC | Total Params |
|---|---|---|---|---|---|---|
| 2 | 0.858 | 0.855 | 0.854 | 0.855 | 0.93 | 6,109,922 |
| 5 | 0.73 | 0.666 | 0.589 | 0.6 | 0.884 | 6,109,922 |
| 20 | 0.593 | 0.287 | 0.269 | 0.262 | 0.807 | 6,269,204 |
| Number of Classes | Acc | Avg Precision | Avg Recall | Avg F1 | Avg AUC | Total Params |
|---|---|---|---|---|---|---|
| 2 | 0.892 | 0.889 | 0.893 | 0.891 | 0.96 | 58,178 |
| 5 | 0.765 | 0.714 | 0.662 | 0.68 | 0.910 | 58,259 |
| 20 | 0.698 | 0.355 | 0.339 | 0.332 | 0.815 | 58,664 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Śmigiel, S.; Pałczyński, K.; Ledziński, D. ECG Signal Classification Using Deep Learning Techniques Based on the PTB-XL Dataset. Entropy 2021, 23, 1121. https://doi.org/10.3390/e23091121
Śmigiel S, Pałczyński K, Ledziński D. ECG Signal Classification Using Deep Learning Techniques Based on the PTB-XL Dataset. Entropy. 2021; 23(9):1121. https://doi.org/10.3390/e23091121
Chicago/Turabian StyleŚmigiel, Sandra, Krzysztof Pałczyński, and Damian Ledziński. 2021. "ECG Signal Classification Using Deep Learning Techniques Based on the PTB-XL Dataset" Entropy 23, no. 9: 1121. https://doi.org/10.3390/e23091121